
Abstract
A 49-year-old man with hypertension for 2 years, was incidentally found to have right intrarenal aneurysms during a routine abdominal ultrasound examination. He reported fluctuating blood pressure readings over the past 18 months. Laboratory parameters were within normal limits, with a serum creatinine level of 1.05 mg/dL. An abdominal CT angiogram revealed a large lobulated intrarenal aneurysm in the lower pole, which communicated with another smaller cortical aneurysm. Additional features suggested the presence of an arteriovenous (AV) fistula. Upon further questioning, the patient disclosed a history of blunt abdominal trauma following a motor vehicle accident 3 years ago. This trauma likely explains the CT findings and the development of hypertension secondary to renovascular disease in this patient. Angiography confirmed the presence of 2 renal artery pseudoaneurysms in the midpolar region, for which selective coil embolization was performed. The patient was stable and asymptomatic at his 2-week follow-up. His blood pressure reading was 110/80 mmHg, showing improvement compared to his pre-procedure recordings. There are very few reported cases of renal pseudoaneurysms causing secondary hypertension. Additionally, this case highlights that successful embolization can result in a substantial improvement in hypertension in these patients.
Introduction
Renovascular disease (RVD) is a major cause of potentially reversible hypertension. It accounts for 1% to 5% of all hypertension cases in the general population and 5.4% of secondary hypertension cases in young adults. The most common type of RVD is atherosclerotic renal artery stenosis, followed by fibromuscular dysplasia. 1 The incidence of renal artery pseudoaneurysms causing secondary hypertension is extremely rare. We describe a case of pseudoaneurysms of the renal artery branches detected incidentally in a 49-year-old man with hypertension, with successful management of the condition.
Case Presentation
A 49-year-old man with a history of hypertension for 2 years was incidentally found to have a right intrarenal aneurysm during a routine abdominal ultrasound examination. Over the past 18 months, he had experienced fluctuating blood pressure, with the highest recorded reading of 160/90 mmHg, and was on Telmisartan 20 mg daily. There was no history of gross haematuria, flank pain or urinary tract infections. On examination, a bruit was audible in the right upper abdominal region and his blood pressure was 140/80 mmHg.
His serum creatinine level was 1.05 mg/dL. Other laboratory parameters, including complete blood count, blood sugar levels and lipid profile were within normal limits. Urine analysis did not indicate proteinuria or haematuria.
An abdominal computed tomography angiography (CTA) revealed a dilated right renal artery measuring 8 mm, with a lobulated intrarenal aneurysm measuring 4.3 x 2.3 cm in the lower pole, communicating with another cortical aneurysm measuring 1.3 x 1.3 cm under a scar in the interpolar region. Additionally, the renal veins in this area were dilated and draining into a dilated right renal vein measuring 20 mm, suggesting the presence of an arteriovenous (AV) fistula.
Upon further questioning, the patient disclosed a history of blunt abdominal trauma from a motor vehicle accident 3 years ago, which likely resulted in the formation of renal aneurysms and the ensuing hypertension.
Angiography performed by interventional radiologists confirmed the presence of 2 renal artery pseudoaneurysms in the midpolar region with early draining veins. Selective coil embolization was performed to treat the pseudoaneurysms.
Procedure Details
The right common femoral artery was punctured using the Seldinger technique, and a 5 French (Fr) sheath was introduced. A 5Fr Simmons-1 catheter was used to cannulate the right renal artery. Angiography revealed 2 renal pseudoaneurysms arising from the midpolar region with early draining veins. Super-selective cannulation of the right renal artery branches was performed using a microcatheter. Detachable coils (6 mm, 7 mm, and 4 mm) and micronester coils were used for embolization. A check angiogram showed no residual pseudoaneurysm, and an abdominal ultrasound confirmed complete thrombosis of the right renal artery pseudoaneurysm. The sheath was removed, and haemostasis was achieved by manual compression.
Outcome and Follow-Up
The procedure was successful, resulting in the complete occlusion of the pseudoaneurysms. The patient did not develop any post-procedure complications and was stable and asymptomatic at his 2-week follow-up. His blood pressure improved to 110/80 mmHg compared to pre-procedure readings, and laboratory parameters, including serum creatinine (0.88 mg/dL), were within normal limits. Due to continued improvement in blood pressure, his antihypertensive medication was discontinued at 3 months follow-up. At 5 months post-procedure, his blood pressure has remained within the normal range, even after stopping medication. He has been scheduled for a follow-up CT angiogram in 6 months, with ongoing monitoring of renal function.
Discussion
A true aneurysm is a circumscribed dilation of an artery that is degenerative in nature involving all 3 layers of the blood vessel that is, the intima, media and adventitia. A pseudoaneurysm, by contrast, forms because of an injury to 1 or more layers of the arterial wall. In renal pseudoaneurysm, the kidney tissue surrounding the site of injury usually exerts enough compressive force to slow the bleeding, and thus a hematoma forms around the arteriotomy. Subsequently, reactive fibrosis occurs and encapsulates the haemorrhage, forming a structure that resembles an aneurysmal sac. 2
Renal artery pseudoaneurysm occurs most frequently as a complication of certain renal interventional procedures such as kidney biopsy, percutaneous nephrostomy, open or endoscopic surgeries on the kidney or because of penetrating trauma. Occurrences following blunt abdominal trauma are rare. 3
The exact mechanism of pseudoaneurysm formation after blunt trauma is less well understood than that of penetrating trauma but is likely to involve shear injury secondary to deceleration forces. 4 It is a potentially life-threatening condition necessitating early diagnosis and intervention. 5 In cases of blunt trauma, presentation can be delayed from days to years after the injury, with the longest reported delay being 15 years. 6 In patients with trauma-associated pseudoaneurysm, pain and haematuria are common findings, although the lesion may be asymptomatic, presenting only with anemia and hypertension. 2
Renal artery stenosis resulting in reduced blood flow is a known cause of renin mediated renovascular hypertension. Disrupted blood flow from stable or enlarging pseudoaneurysms would produce similar downstream turbulence and result in renin mediated hypertension. 5
Some evidence suggests that these injuries may regress without intervention, although isolated observation is not recommended as a management strategy in most patients due to the high risk of rupture. 2
Ultrasonography and computed tomography are particularly useful when renal vascular and parenchymal injuries are suspected. 7 Colour doppler revealed a characteristic sign of two-directional flow at the pseudoaneurysm neck and a “yin-yang” pattern inside the lesion, thus revealing the direction of blood flow entering and leaving the pseudoaneurysm. 8 However, the ability to confirm the presence and anatomical location of renal artery pseudoaneurysms and perform therapeutic procedures makes angiography the gold standard test of choice. 7
Endovascular catheter angioembolization with thrombogenic agents or occlusive coils has evolved into a highly effective and safe procedure that can obviate the need for invasive surgery and is unlikely to result in long-term renal impairment. Thus, it is the currently accepted first-line therapy. 2
Coil embolization is the preferred treatment for intraparenchymal aneurysms arising from medium to small segmental arteries. Embolization of small and distal arteries results in minimal loss of renal parenchyma. Cases with concurrent AV fistulas, as in our patient, are at risk of developing pulmonary embolism when thrombotic agents are used for embolization. 9 Therefore, detachable coils were used for embolization in our patient.
Incomplete embolization leads to ischemic renal tissue that may continue to secrete renin for some time, resulting in sustained arterial hypertension. Patients may suffer postembolization syndrome (characterized by pain, nausea, vomiting, and fever) if a significant amount of renal tissue is infarcted. 9
After successful treatment with angioembolization, patients must be closely monitored as recurrent bleeding has been reported. 2 There are no established protocols for post-treatment follow-up of patients who have undergone selective angioembolization. A repeat CT scan of the abdomen, annual monitoring of blood pressure and renal function is advised. Long-term complications after the procedure are rare. 2
Conclusion
This case report adds to the limited literature on trauma-induced renal pseudoaneurysms resulting in secondary hypertension. Successful coil embolization not only addressed the aneurysms with a significant improvement in the patient’s blood pressure but also avoided major invasive surgery. This demonstrates the effectiveness of minimally invasive intervention in managing hypertension secondary to renovascular disease (Figures 1–3). Abdominal computed tomography angiography (CTA) revealing a dilated right renal artery measuring 8 mm, with a lobulated intrarenal aneurysm measuring 4.3 x 2.3 cm in the lower pole, the renal veins in this area are dilated and draining into a dilated right renal vein measuring 20 mm, suggesting the presence of an arteriovenous (AV) fistula. Angiography showing the presence of two renal artery pseudoaneurysms in the midpolar region with early draining veins. Angiogram showing micronester coils used for embolization with no residual pseudoaneurysm.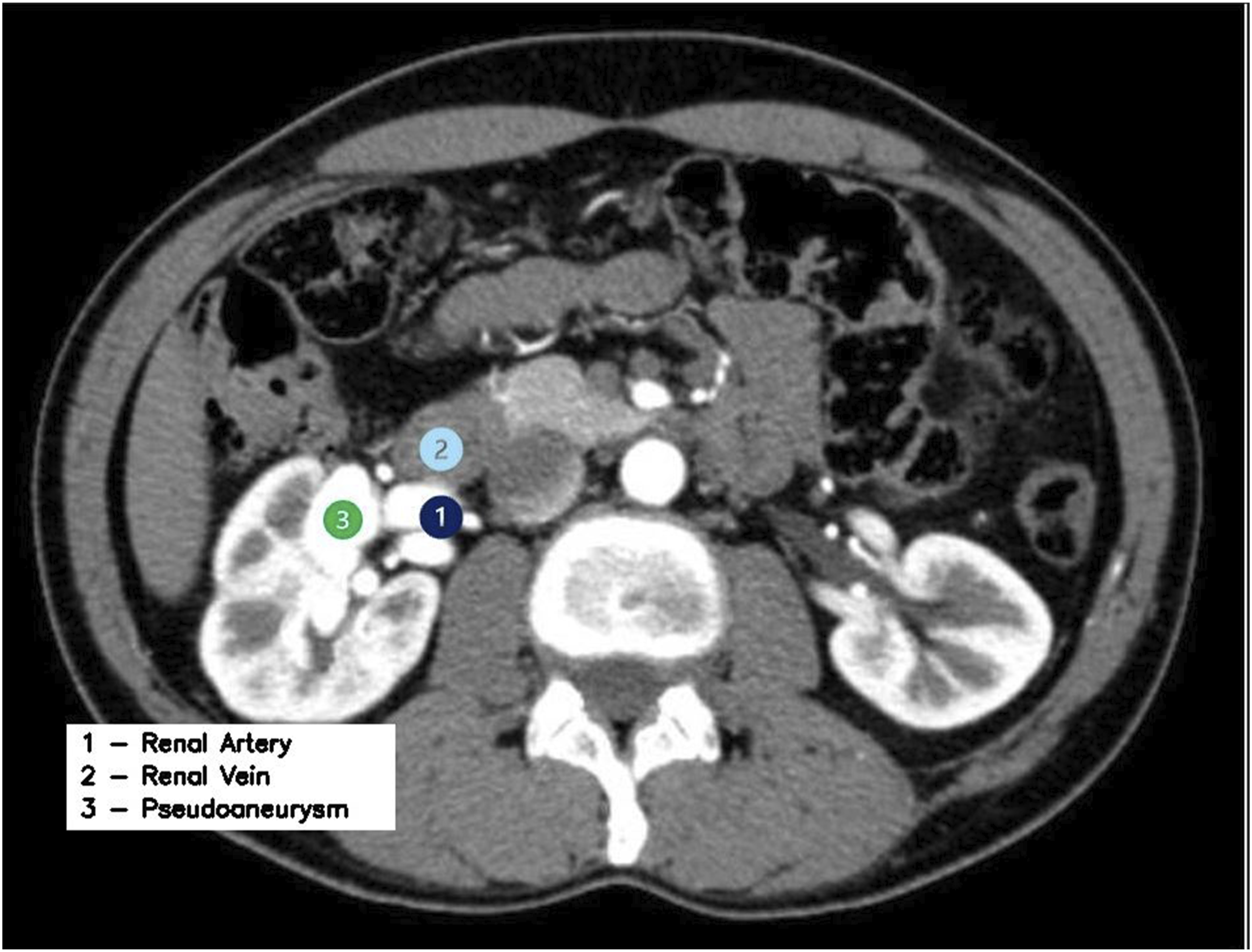


Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.