
Abstract
Objective
This study aimed to compare 30-day postoperative outcomes of carotid body tumor (CBT) resections performed by vascular surgeons vs otolaryngologists, examining complication rates, operation time, and hospital stay duration.
Methods
A retrospective cohort analysis was conducted using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database from 2006 to 2020. Patients undergoing CBT resection were identified using CPT code 60605. Only cases performed by vascular surgeons or otolaryngologists were included. The primary outcome was any major postoperative complication, with secondary outcomes including operation time and hospital length of stay. Multivariable logistic and linear regression models adjusted for confounders including age, sex, modified Charlson Comorbidity Index (mCCI), race, surgical setting, and emergency status.
Results
A total of 718 patients (545 vascular surgery, 173 otolaryngology) were included. Patients operated on by vascular surgeons were older (58 vs 51 years, p < .001), had a significantly higher incidence of hypertension (51% vs 36%; p < .001) and mCCI (1.78 ± 1.47 vs 1.25 ± 1.36; p < .001). Otolaryngology surgeries had significantly longer mean operative times (203 vs 145 min, p < .001) and a higher, though not statistically significant, rate of major complications (5.3% vs 2.3%, p = .07). Adjusted multivariable analysis showed otolaryngology specialty was independently associated with increased odds of severe adverse events (aOR: 2.99; 95% CI: 1.15-7.56; p = .021) and longer operation time (aβ: 61; 95% CI: 46-75; p < .001), but not with reoperation rates.
Conclusion
While both specialties achieved generally safe outcomes, CBT resections performed by otolaryngologists were associated with longer operative times and higher odds of major complications. These differences may reflect variations in case complexity, patient selection, or surgical expertise, warranting further prospective research into multidisciplinary and specialty-specific outcomes for CBT surgery.
Introduction
Carotid body tumors (CBTs) are rare neoplasms of neuroectodermal tissue with an incidence of 1:30 000-100,000. 1 Despite low incidence, these tumors represent 65% of head and neck paragangliomas and are primarily benign with only 5% of them being malignant.2,3 CBTs are mostly asymptomatic with the presence of a neck mass being the most common initial presentation. 4 Three types of CBTs include the familial, sporadic, and hyperplastic forms. 5 Familial CBTs mainly present in younger patients, are more likely to be malignant and are associated with succinate dehydrogenase (SDH) mutations. 6
Surgical resection is the preferred treatment method by both vascular surgeons and otolaryngologists, with radiotherapy reserved for patients who cannot undergo operations due to comorbidities. Additionally, radiotherapy should be considered for treatment of residual tumor, unresectable large tumors, and malignant lesions with lymph node metastases. 7 With surgical resection as the preferred treatment method, preoperative imaging with ultrasound, CT or MR angiography of the neck is crucial to evaluate the size of the lesion, carotid artery involvement, tumor vascularity, proximity to cranial nerves and the extension to the skull base. 4 Common complications of CBT resection include stroke and transient ischemic attack (3.6% and 3.6%, respectively), hypoglossal and superior laryngeal nerve injury (10.7% and 1.8%, respectively), and hematoma (1.8%). 1 However, the incidence of these complications may vary due to the diverse group of surgical specialists performing these operations, each with varying levels of experience in treating these rare tumors. This group includes vascular surgeons, otolaryngologists, general surgeons, and surgical oncologists.2,8-10 Therefore, the aim of this study was to compare the outcomes of CBT resection performed by vascular surgeons vs otolaryngologists as primary surgical teams.
Methods
Data Source
In this cohort study, we conducted an analysis using de-identified data sourced from the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) Participant Use Files spanning from January 1, 2006, to December 31, 2020. This database encompasses cases from over 700 participating hospitals in the United States and includes more than 300 variables collected prospectively, covering patient characteristics, procedure-related information, and 30-day outcomes. To ensure transparency and adherence to guidelines, we followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. 11 Importantly, this study was exempt from review and informed consent requirements by the Yale Institutional Review Board due to the utilization of deidentified data.
Patient Population, Primary Exposure and Outcome
All patients who received carotid body tumor resection surgery between the years 2006-2020 were considered. We used Current Procedural Terminology
(CPT) code 60605 to find these cases. Cases with otolaryngology or vascular surgery as their primary surgical team were compared to each other. The primary outcome of our study was any postoperative major complications. Based on prior literature, major complications were defined as mortality, use of a ventilator for more than 48 h, unplanned intubation, stroke/cerebrovascular accident, pulmonary embolism, deep vein thrombosis, cardiac arrest, myocardial infarction, acute renal failure, progressive renal insufficiency, sepsis, or septic shock. The secondary outcomes of our study were operation time and hospital length of stay. To isolate the effect of surgical specialty, we excluded cases in which multiple surgical specialties were involved. Only cases performed by a single primary surgical team—either vascular surgery or otolaryngology—were included in the analysis.
Covariates
The following baseline demographic data were used in this study: age, race, ethnicity, sex, body mass index (BMI), and comorbidities including smoking and the modified Charlson Comorbidity Index (mCCI). Modified Charlson Comorbidity index was calculated based on congestive heart failure, chronic obstructive pulmonary disease, diabetes mellitus, end-stage renal disease, ascites, and disseminated cancer. The values were summed for a total number, to which one point was added for each decade greater than 40 years of age. The mCCI is a well-validated scoring system for surgical patients. An adapted version for NSQIP has been shown to be sensitive in stratifying mortality. 12 Perioperative variables included inpatient/outpatient status and emergency status of the surgery.
Statistical Analysis
We conducted data analysis using R, Version 2023.06.2 + 561. Patients with missing data were included in the analysis if they had complete data for the primary exposure and primary outcome components and if covariates had less than 10% missing values. No imputation analysis was performed. Descriptive statistics were presented as means along with their corresponding standard deviations for continuous variables and as percentages for categorical variables. To compare patients based on the surgical specialty that operated on them, global univariate analyses were conducted. Categorical variables were assessed using the Pearson χ2 test, and the Fisher exact test was used where appropriate. For continuous and ordinal variables, the Wilcoxon rank-sum test was employed. To assess the independent association of the surgical specialty with severe adverse outcomes, we conducted multivariable logistic regression, controlling for pre-defined confounding variables including race, sex, mCCI, setting, and the emergency status of the surgery. Odds ratios (ORs) along with their corresponding 95% confidence intervals (CIs) were reported for the results of the multivariable regression models. Statistical significance was determined at a threshold of p < .05, and all reported p values are two-tailed.
Results
Overall Findings
During the 14-year study period, 718 tumor resections were performed, of which 545 (76%) were conducted by vascular surgeons and 173 (24%) by otolaryngologists. The mean [SD] age was 59 [45, 68]) years; 64% were women; mean [SD] mCCI was 1.65 [0.2, 3.1]). Patients were 83% white, 14% black, 2.7% Asian, 0.3% American Indian or Alaska Native, 0.3% Native Hawaiian or Pacific Islander. For the entire population, the percentage of major complications within 30 days was (3.1%), including rates of 0.3% mortality, 1.1% being ventilator dependent for more than 48 h or reintubated, 1.1% cerebrovascular event, 0.7% deep vein thrombosis (DVT) or pulmonary embolism (PE), 0.1% cardiac arrest or myocardial infarction, 0.3% sepsis or septic shock, 3.1% return to the operating room and 0.7% surgical site infection.
Demographics and Operative Details by Specialty
Patient Characteristics by Surgical Specialty.
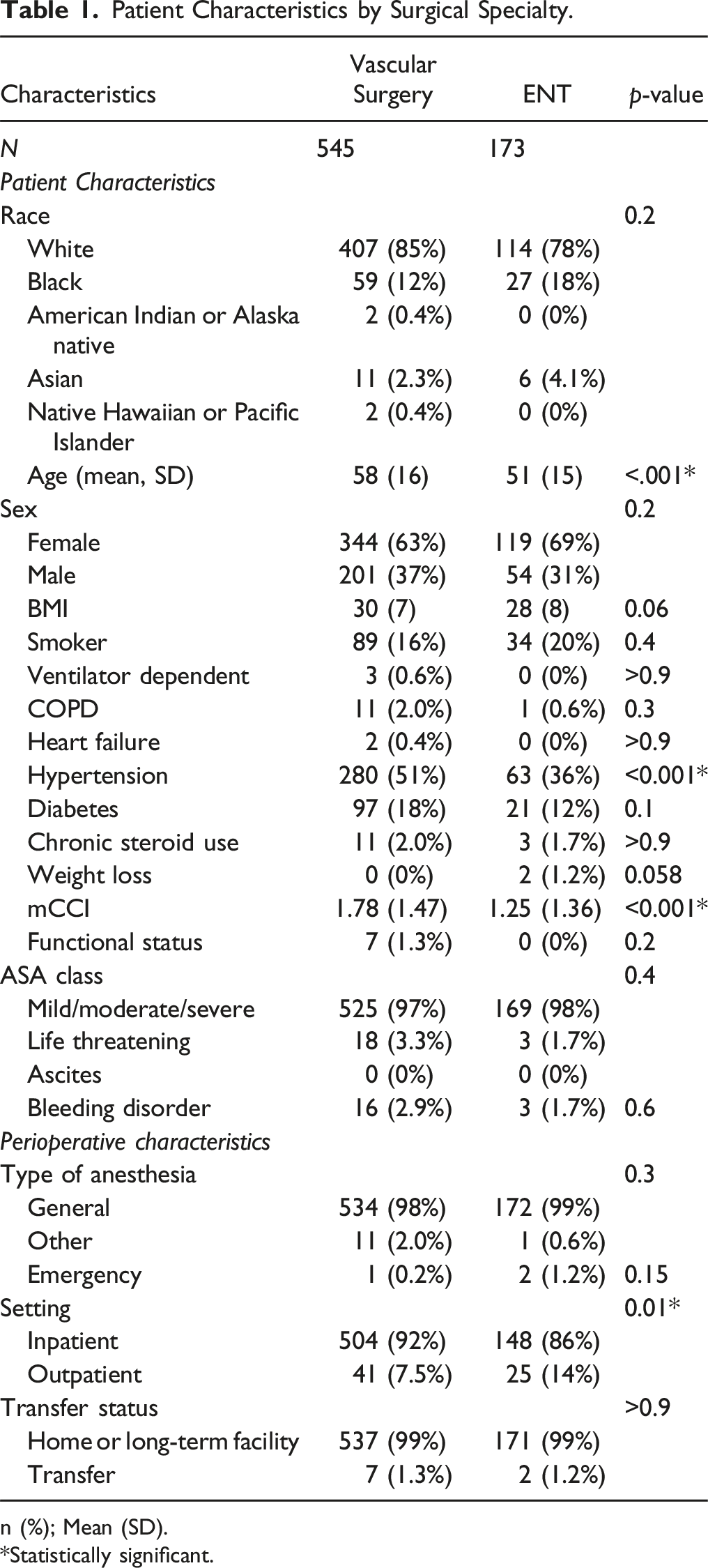
n (%); Mean (SD).
*Statistically significant.
Surgical Outcomes by Specialty
Surgical Outcomes by Surgical Specialty.
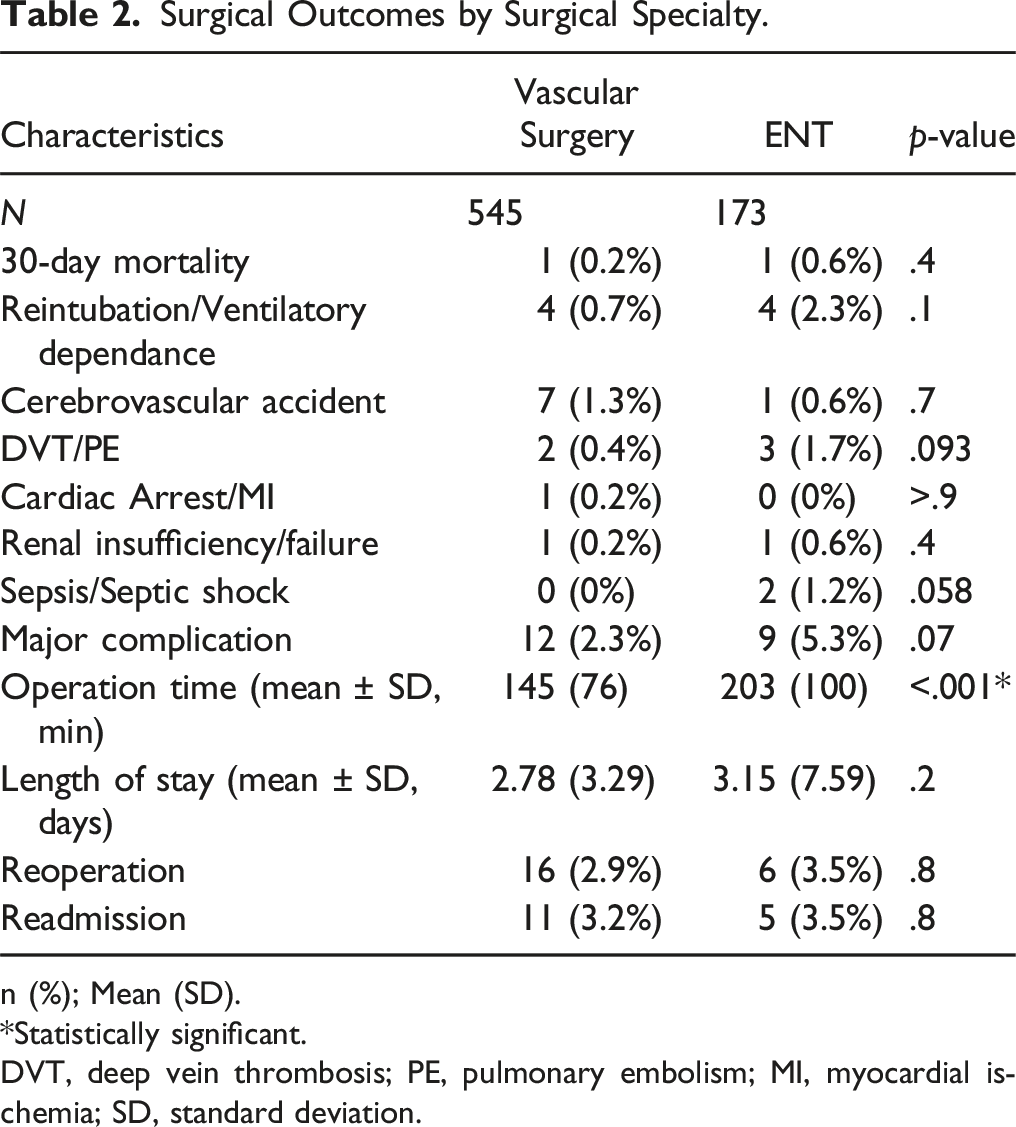
n (%); Mean (SD).
*Statistically significant.
DVT, deep vein thrombosis; PE, pulmonary embolism; MI, myocardial ischemia; SD, standard deviation.
Multivariable Analysis by Specialty
Factors Associated With Operation Time.
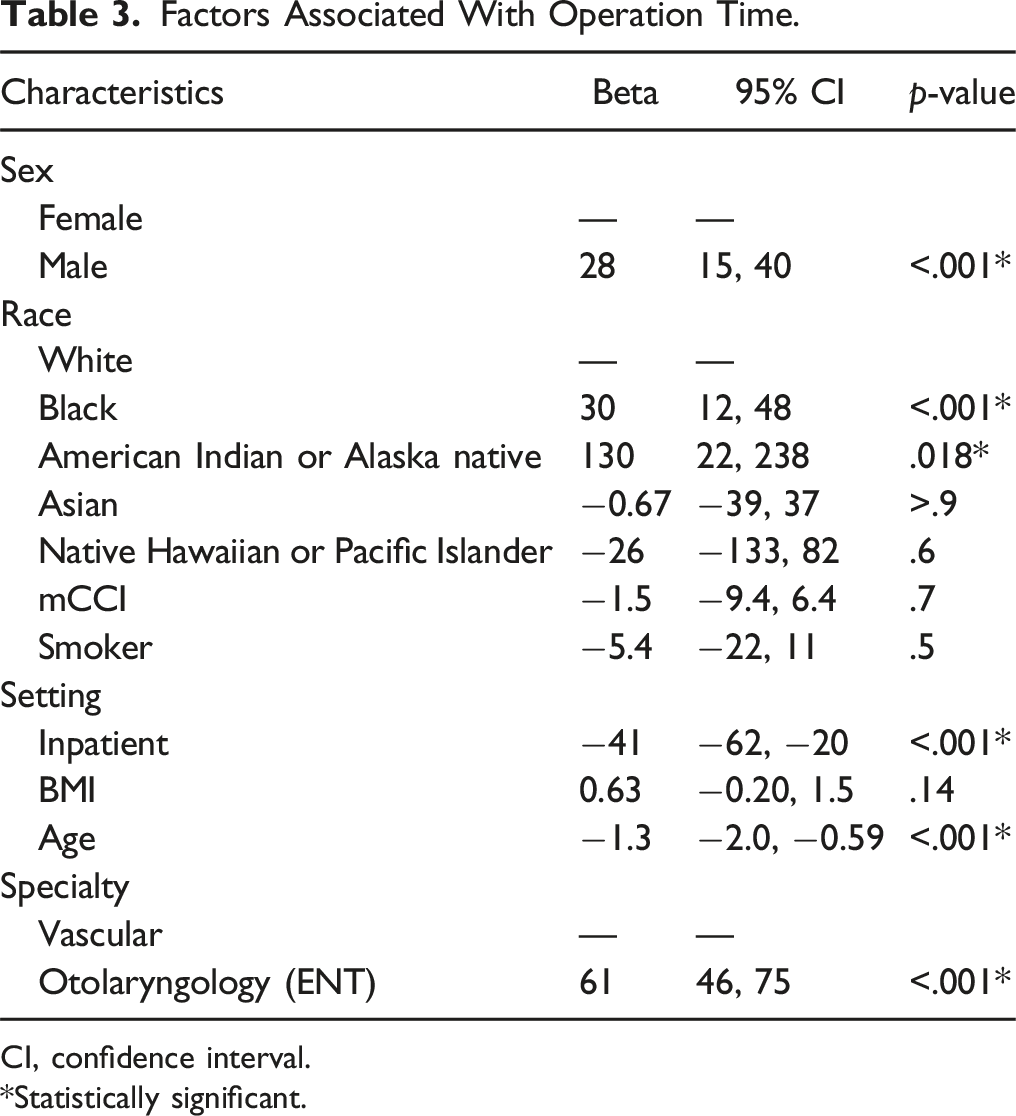
CI, confidence interval.
*Statistically significant.
Factors Associated With Serious Adverse Event.
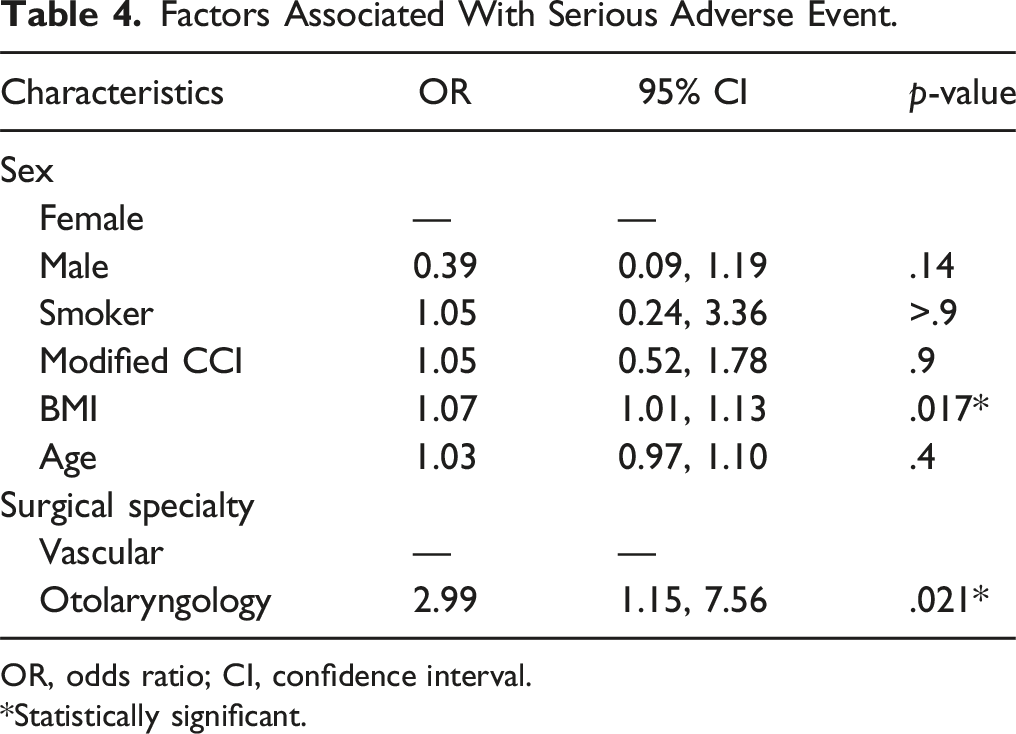
OR, odds ratio; CI, confidence interval.
*Statistically significant.
Factors Associated With Reoperation.
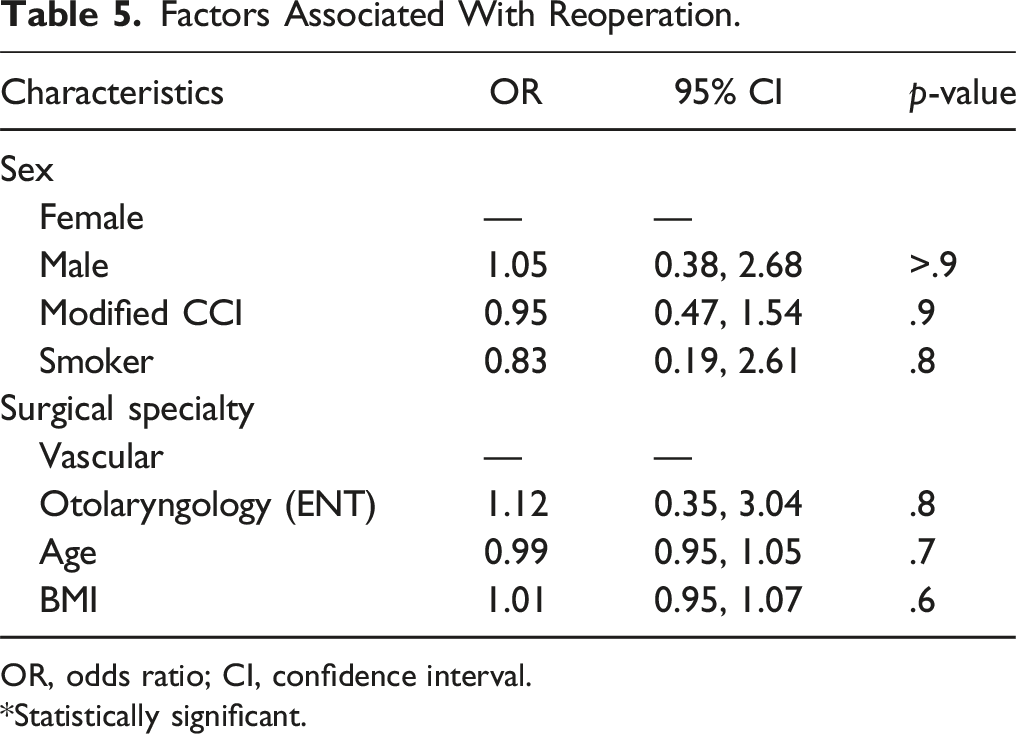
OR, odds ratio; CI, confidence interval.
*Statistically significant.
Discussion
This study compared the demographics and outcomes of patients undergoing CBT resection by vascular surgeons and otolaryngologists. The results indicated that patients treated by vascular surgeons tended to be older and more likely to have hypertension, whereas the cohort treated by ENT teams experienced longer operative times and a higher incidence of severe adverse outcomes. Interestingly, a larger proportion of CBT resections performed by ENT teams were done in the outpatient setting as compared to those performed by vascular surgeons. Furthermore, since inpatient settings were associated with shorter operative times, it can be perhaps concluded that the shorter operative times seen in surgeries performed by vascular teams may be due to the inpatient setting. Alternatively, the longer operative times and higher incidence of adverse outcomes in the ENT group may be attributed to the resection of tumors with higher Shamblin classifications or malignant features. However, due to the lack of granular data in the NSQIP database (eg, tumor extent, radiologic features, etc), these associations cannot be clearly defined, which could serve as a focus for future research.
Additionally, besides the outpatient procedure setting, male gender and Black or American Indian/Alaska Native races were significantly associated with longer operative times. One possible explanation is that males might have a higher rate of CBT with malignant features, necessitating more extensive resections. However, a study examining factors associated with malignancy in CBT found no such association between male gender and malignant features in a multivariate logistic regression. 13 Therefore, future research should explore the relationship between gender and the need for longer CBT resections. Interestingly, the association between race and longer operative times has not been previously reported. However, in a study on the epidemiology and survival of patients with malignant carotid body tumors using the Surveillance, Epidemiology, and End Results (SEER) database, race was not found to be associated with either overall or disease-specific survival. 14 This new finding warrants further investigation in future studies. Finally, our data revealed no association between the primary operative team specialty and CBT reoperation rates.
While many studies have explored the use of a multidisciplinary approach for CBT resection, there is limited literature directly comparing outcomes between vascular surgeons and otolaryngologists. One such study, conducted at a single center between 2000 and 2019, examined the outcomes of CBT resections performed by multidisciplinary teams and included a sub-analysis comparing the results of vascular surgeon and otolaryngologist interventions. 15 Similar to the current study, this comparison of patient demographics and surgical outcomes revealed distinct patterns between the two specialties. For example, vascular surgeons resected tumors in older patients with cardiovascular disease and were more likely to use preoperative embolization, while otolaryngologists tended to operate on earlier-stage tumors and those with malignant features. 15 Notably, all Shamblin I tumors were resected by otolaryngologists, while vascular surgeons more commonly handled Shamblin II tumors. Shamblin III tumors, typically more complex, were usually addressed by a combined surgical team. A sub-analysis directly comparing outcomes between vascular (14 tumors) and ENT (38 tumors) teams found no statistically significant differences in carotid artery injury, blood loss, cranial nerve injury, surgical duration, post-operative hypertension, length of stay, or readmission rates. 15 However, the authors noted that surgeries performed by multidisciplinary teams—typically reserved for advanced-stage tumors—were associated with higher rates of carotid artery injury, residual tumor, and longer hospitalizations. Additionally, the current analysis does not account for differences in imaging findings, Shamblin classification, or cranial nerve injury, as this information is not available in the NSQIP database. Addressing these factors will be an important area for future research.
A different study did not directly compare the outcomes between vascular and ENT teams but instead evaluated whether a multidisciplinary approach improved outcomes after CBT resection. 16 The multidisciplinary team included endocrinologists, geneticists, vascular surgeons, otolaryngologists, radiologists, thoracic surgeons, physiatrists, and speech therapists. This comprehensive evaluation encompassed genetic counseling, preoperative SDH gene mutation analysis, preoperative adjunctive endovascular procedures (PAEPs), and postoperative rehabilitation. PAEPs included external carotid artery stenting, percutaneous transfemoral embolization, or direct percutaneous puncture of the tumor with simultaneous embolization. The study involved 57 consecutive CBT resections performed at a single institution between 1995 and 2019. 16 Patients were divided into two groups: those treated by vascular surgeons and those treated by multidisciplinary teams. Of note, this study did not include a sub-analysis of outcomes for patients whose tumors were resected by both vascular and ENT surgeons together. 16 The incidence of SDH mutations, patient characteristics, and tumor size were similar between the two groups. However, when comparing outcomes, patients treated by a multidisciplinary team had significantly shorter operative times and lower blood loss compared to those treated solely by vascular surgeons. Additionally, blood loss was significantly reduced in patients who underwent PAEPs compared to those who had direct surgery. Importantly, PAEPs were performed only in patients with CBT lesions exceeding 45 mm, all of whom were in the group treated by multidisciplinary teams. Since PAEPs provided better surgical control of the carotid bifurcation, the shorter procedure times and lower blood loss in this group could be attributed to the use of PAEPs. No significant differences were observed between the groups regarding transient or persistent cranial nerve injuries. These findings suggest that the comprehensive multidisciplinary care provided to these patients offers significant benefits. Unfortunately, the retrospective nature of the current study, which utilized data from a national database, limits the ability to assess whether other specialties were involved in the comprehensive evaluation, treatment, and postoperative care for the patients in the study.
This study has several limitations that should be considered when interpreting the results. One major limitation is the retrospective nature of the data analysis, which may lead to recall or selection bias. Additionally, limited data accuracy can arise from inconsistencies in data entry, especially when diagnostic or procedural codes failed to represent true clinical picture. Furthermore, the NSQIP database does not capture procedure-specific complications such as cranial nerve injury, which is one of the most clinically relevant morbidities in CBT surgery. This absence limits the ability to fully characterize differences in complication profiles between specialties. Similarly, key anatomic tumor descriptors such as Shamblin classification are not available, precluding adjustment for case complexity. As a result, the observed differences in operative time and morbidity may, in part, reflect underlying differences in tumor stage or technical difficulty that could not be accounted for in this dataset. Additionally, treatment protocols in large datasets often lack detailed descriptions, making it difficult to account for variations in surgical techniques, preoperative management, the use of pre-embolization procedures, the type of preoperative imaging used for treatment planning, and postoperative care. Similarly, long-term follow-up is often limited or unavailable in database studies, restricting the ability to assess long-term complications or recurrence rates. Additionally, the overall low frequency of major adverse events, coupled with the smaller number of cases in the otolaryngology group, may limit the statistical power and precision of some outcome comparisons. As such, some findings—particularly those related to complications—should be interpreted with caution. Taken together, these limitations underscore the need for caution when drawing conclusions from the study and highlight the importance of complementary prospective studies to validate the findings and address these gaps in data.
Conclusion
While both specialties achieved generally safe outcomes, carotid body tumor resections performed by otolaryngologists were associated with longer operative times and higher odds of major complications. These differences may reflect variations in case complexity, patient selection, or surgical expertise, warranting further prospective research into multidisciplinary and specialty-specific outcomes for carotid body tumor surgery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Cardiovascular Imaging T32; T32 EB009035.
Ethical Statement
Data Availability Statement
The data for this study can be made available based on request.