
Abstract
Introduction
There is no consensus on the optimal secondary stroke prevention regimen for patients with atrial fibrillation undergoing carotid artery stenting (CAS). Our objective is to compare the long-term efficacy and safety of different medical regimens after CAS.
Methods
This retrospective observational study included patients with pre-existing atrial fibrillation who underwent CAS from 2011 to 2024. Patients were divided into three treatment groups: dual antiplatelet therapy (DAPT), single antiplatelet therapy plus oral anticoagulation (AA), and triple therapy (dual antiplatelet therapy plus oral anticoagulation, TT). The primary outcome was the incidence of major bleeding. Secondary outcomes included the incidence of clinically relevant minor bleeding, recurrent stroke, and stent thrombosis.
Results
Of the 1047 patients who underwent CAS, 129 met the inclusion criteria: 31 in the DAPT group, 46 in the AA group, and 52 in the TT group. At 3 months, major bleeding events occurred in 3.2% (1/31) of patients in the DAPT group, 6.5% (3/46) in the AA group, and 7.7% (4/52) in the TT group (P = 0.71). Ischemic stroke after stent placement occurred in 6.4% (2/31) of cases in the DAPT group, compared to 4.3% (2/46) in the AA group and 1.9% (1/52) in the TT group (P = 0.57). Stent thrombosis occurred in 3.2% (1/31) of patients in the DAPT group, 6.5% (3/46) in the AA group, and 1.9% (1/52) in the TT group (P = 0.32).
Conclusion
Our findings suggest no significant differences in bleeding events or ischemic outcomes among the different antiplatelet and anticoagulation regimens in patients with atrial fibrillation who underwent CAS.
Introduction
Carotid endarterectomy and carotid stenting (CAS) are used in the treatment of symptomatic carotid stenosis, with patients typically undergoing intervention in their 7th and 8th decades.1-5 Atrial fibrillation is a common comorbidity in this patient population, with some studies suggesting an incidence ranging from 9.3% to 18.3%. 6 Anticoagulation is the mainstay for stroke prevention in atrial fibrillation, especially in patients with higher CHA2DS2-VASc scores.7-9 Patients undergoing carotid stent placement typically require a 3-month course of dual antiplatelet therapy to prevent stent occlusion and thromboembolism followed by a single antiplatelet medication indefinitely.10-12
Patients with both carotid stenosis and atrial fibrillation pose unique challenges for secondary stroke prevention. The ideal strategy that balances robust antiplatelet therapy and anticoagulation to prevent cardioembolic strokes, while minimizing hemorrhagic risk, remains unclear. Evidence suggests that dual antiplatelet therapy plus an oral anticoagulant may offer the strongest protection against stent occlusion and thromboembolism, albeit with an increased risk of bleeding.13,14 Conversely, dual antiplatelet therapy alone, or a single antiplatelet agent combined with an oral anticoagulant, may not provide sufficient protection against stent thrombosis or thromboembolism.
This study aims to compare the long-term efficacy and safety of three secondary prevention regimens in patients who have undergone CAS and have concurrent non-valvular atrial fibrillation: dual antiplatelet therapy (DAPT), single antiplatelet therapy plus oral anticoagulation (AA), and triple therapy (dual antiplatelet therapy plus oral anticoagulation, TT).
Methods
Study Design
This single-center retrospective observational study included patients with pre-existing atrial fibrillation who underwent CAS from 2011 to June 2024. The institutional review board approved the study and waived the requirement for consent due to its retrospective design. Patients were included if they met the following criteria: previous, persistent, permanent, or paroxysmal non-valvular atrial fibrillation; and either symptomatic atherosclerotic carotid stenosis or asymptomatic atherosclerotic carotid stenosis that fulfilled revascularization criteria per American Heart Association guidelines.10,15 Patient demographics were also obtained. The risk of cardioembolic stroke was evaluated using CHA2DS2-VASc scores. The CHA2DS2-VASc score is a clinical tool used to assess the risk of stroke in patients with atrial fibrillation. It incorporates common risk factors, including congestive heart failure, hypertension, age (with higher points for ≥75), diabetes, prior stroke or thromboembolism, vascular disease, and female sex. Each factor contributes a weighted point value to a maximum score of 9. The higher the score, the greater the patient’s annual stroke risk, guiding clinicians on whether anticoagulation therapy is recommended to reduce this risk. HAS-BLED scores were used to stratify the risk of hemorrhage between groups. 16 The HAS-BLED score considers factors such as hypertension, abnormal renal or liver function, prior stroke, bleeding history, labile international normalized ratios (INR), age over 65, and the use of drugs or alcohol. With a maximum score of 9, a higher score indicates an increased bleeding risk, prompting closer monitoring and risk factor modification rather than automatic avoidance of anticoagulation.
Three treatment groups were established based on the antithrombotic regimens used at our institution: (1) DAPT group; (2) Single antiplatelet and an anticoagulant (AA group); and (3) DAPT and an anticoagulant (TT group). Antiplatelet medications included aspirin (81 mg or 325 mg daily), clopidogrel (75 mg daily), and ticagrelor (90 mg twice daily). Anticoagulants included warfarin (dosed to a therapeutic INR of 2-3) or a direct oral anticoagulant (DOAC)—either apixaban (5 mg twice daily) or rivaroxaban (20 mg daily). The choice of antithrombotic regimen is made by the provider in discussion with the patient, without institutional preference or specific recommendations.
Neurologic evaluations and modified Rankin scores were recorded before the procedure and at the 90-day follow-up, while follow-up imaging was performed using carotid ultrasonography or computed tomography angiography (CTA). Patients were excluded if they had valvular atrial fibrillation, contraindications to antiplatelet or anticoagulant therapy, a history of intracranial hemorrhage, active bleeding disorders, severe hepatic impairment, end-stage renal disease (creatinine clearance <15 mL/min), were lost to follow-up, or were pregnant.
Outcome Measures
The primary outcome was incidence of major bleeding as defined by the international Society of Thrombosis and Haemostasis. This includes fatal bleeding, bleeding into a critical organ, bleeding causing a decrease in hemoglobin by 2 g/dL, or bleeding that requires two or more transfusions of whole blood or packed red blood cells. 17 Secondary outcomes included incidence of clinically relevant minor bleeding, recurrent stroke, and stent thrombosis. Non-major clinically relevant hemorrhage was defined as significant enough to warrant medical attention but does not cause hemodynamic instability, require transfusion of ≥2 units of blood, or involve a critical site such as intracranial, intraspinal, intraocular, pericardial, intra-articular, or retroperitoneal locations. These minor bleedings were recorded from each patient last clinical and imaging follow-up. A subgroup analysis was additionally conducted across the three groups. Stent thrombosis was defined by an increased degree of in-stent stenosis on follow-up imaging. For carotid ultrasonography, these included peak systolic velocity ≥200 cm/s for ≥50% stenosis and ≥300 cm/s, end-diastolic velocity ≥140 cm/s, and internal carotid artery/common carotid artery ratio ≥3.8 for ≥70% stenosis.18,19 NASCET criteria was used for determining stent thrombosis on CTA. 20
Statistical Analysis
The values for continuous variables are presented as means and two-sample t tests were used for analysis. The Mann-Whitney test, medians, and interquartile ranges were used for non-normal distributions. Categorical variables were analyzed using the x2 test or the Fisher exact test for non-normal distributions. Univariate and multivariate linear regression analyses were conducted for each outcome, with therapy as the predictor and adjusted for clinical variables. The DAPT therapy patients were used as the reference group for the entire analysis. Odds ratio (OR) and 95% confidence interval (CI) were provided. Sample size was estimated using a chi-square test for proportions across the three groups based on expected bleeding events of 4 (TT), and 0 (DAPT and AA) reported by Pardo-Galiana et al. 13 The estimated minimal sample size required to detect a statistically significant difference with 80% power at α = 0.05 was 25 patients. All data were analyzed using R, version 4.3.3. A P-value of less than 0.05 was considered statistically significant.
Results
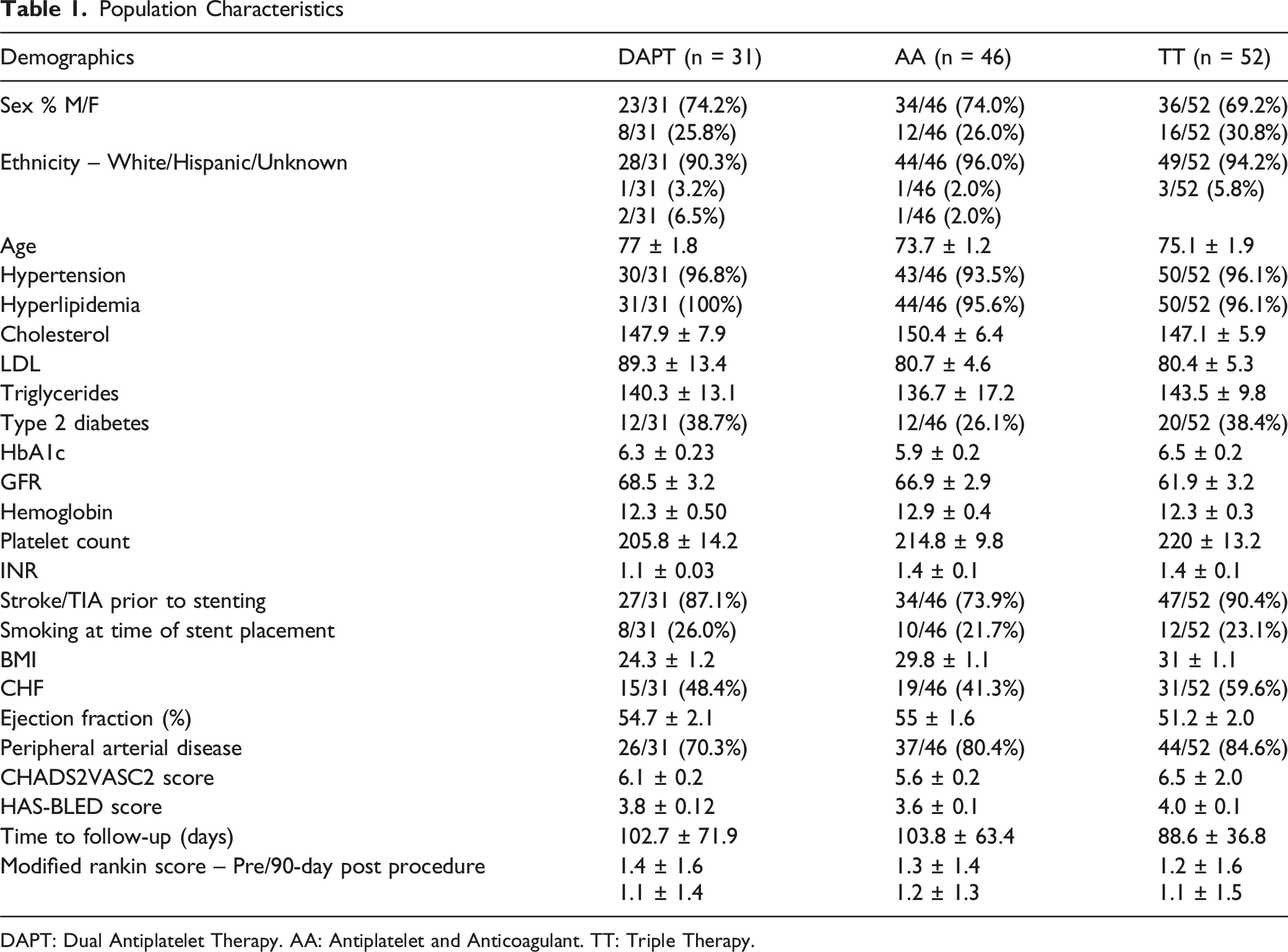
Of the 1047 patients who underwent CAS within the specified timeframe, 213 had atrial fibrillation. Of those, 129 patients met inclusion criteria, 31 patients in the DAPT group; 46 patients in the AA group; and 52 patients in the TT group (Figure 1, Table 1). The CHADS2VA2Sc scores were: 6.1 ± 0.2 for the DAPT group; 5.6 ± 0.2 for the AA group; and 6.5 ± 2.0 for the TT group. The HAS-BLED scores were: 3.8 ± 0.1 for the DAPT group; 3.6 ± 0.1 for the AA group; and 3.8 ± 0.1 for the TT group. Across all groups, the mean clinical and imaging follow-up time ranged from approximately 89 to 104 days. Ultrasound was the predominant imaging method used for follow-up, accounting for 59%–73% of cases. Flowchart of Patient Selection Population Characteristics DAPT: Dual Antiplatelet Therapy. AA: Antiplatelet and Anticoagulant. TT: Triple Therapy.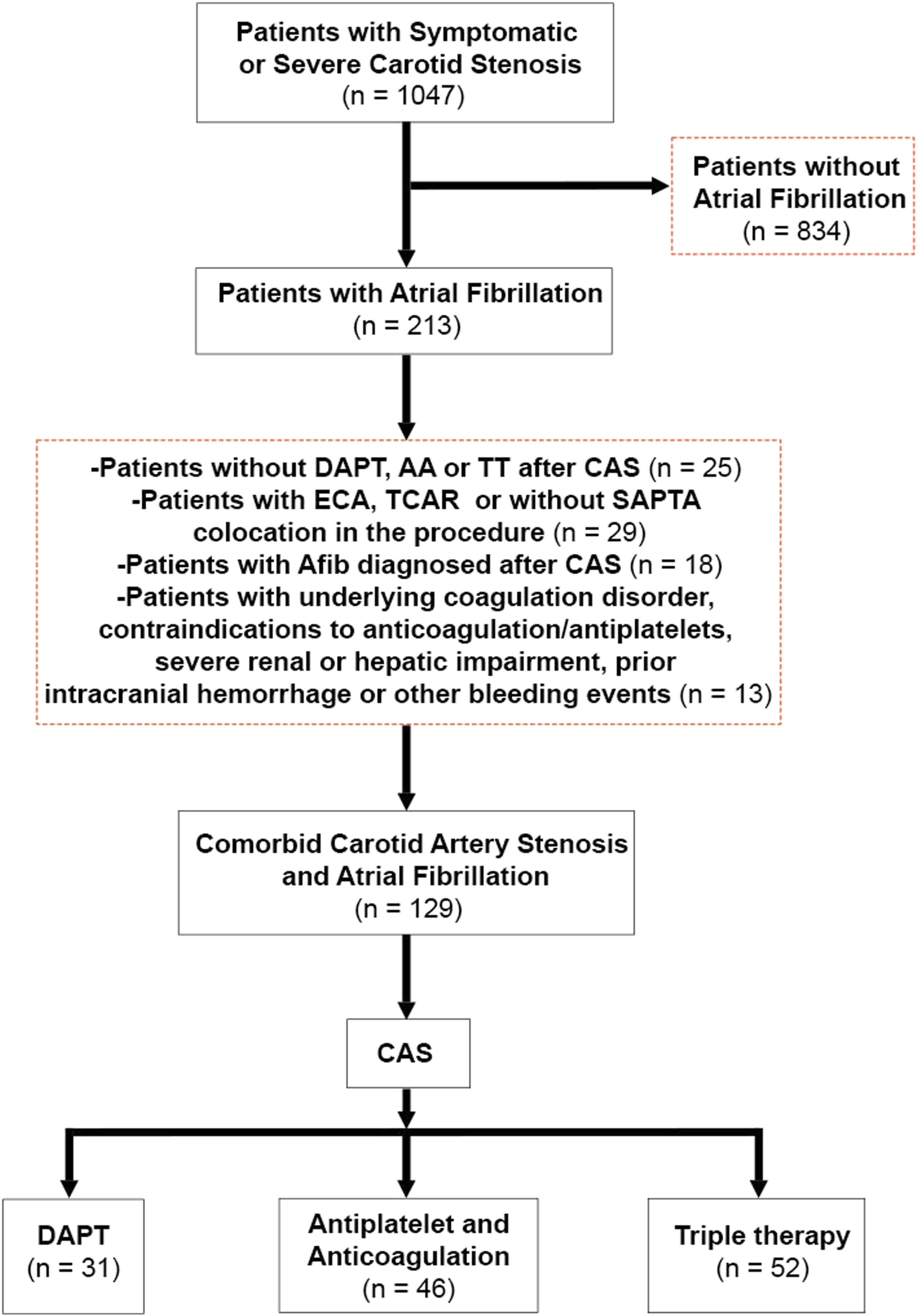
Clinical Outcomes Summary

DAPT: Dual Antiplatelet Therapy. AA: Antiplatelet and Anticoagulant. TT: Triple Therapy.
Thrombotic Outcomes Post CAS
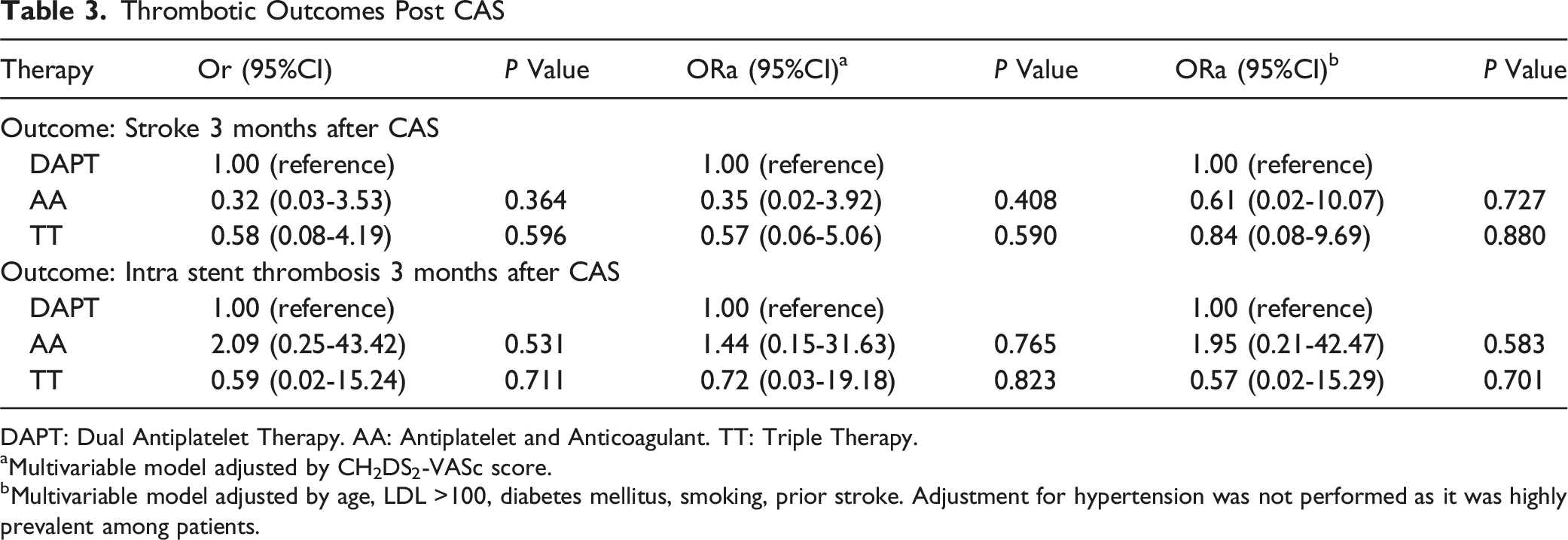
DAPT: Dual Antiplatelet Therapy. AA: Antiplatelet and Anticoagulant. TT: Triple Therapy.
aMultivariable model adjusted by CH2DS2-VASc score.
bMultivariable model adjusted by age, LDL >100, diabetes mellitus, smoking, prior stroke. Adjustment for hypertension was not performed as it was highly prevalent among patients.
Hemorrhagic Outcomes Post CAS
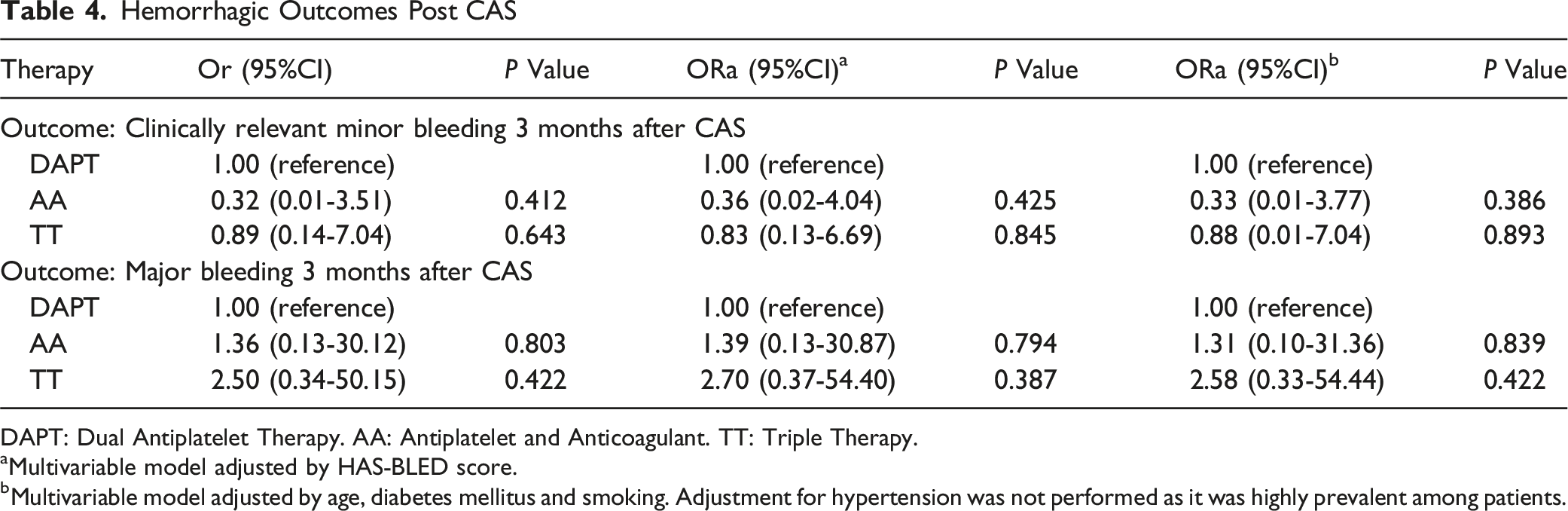
DAPT: Dual Antiplatelet Therapy. AA: Antiplatelet and Anticoagulant. TT: Triple Therapy.
aMultivariable model adjusted by HAS-BLED score.
bMultivariable model adjusted by age, diabetes mellitus and smoking. Adjustment for hypertension was not performed as it was highly prevalent among patients.
Outcome Measures Across Different Medications Regimen
On subgroup analysis, in the DAPT group including 31 patients, 27/31 (87.1%) were on Aspirin + Clopidogrel and 4/31 (12.9%) on Aspirin + Ticagrelor. Likewise, in the 46 patients of the AA cohort, 18/46 (39.1%) were on Apixaban + Aspirin, 8/46 (17.4%) on Apixaban + Clopidogrel, 7/46 (15.2%) on Dabigatran + Aspirin, 1/46 (2.2%) on Dabigatran + Clopidogrel, 7/46 (15.2%) on Warfarin + Aspirin and 5/46 (10.9%) on Warfarin + Clopidogrel. In the TT group including 51 patients, 33/51 (64.7%) were on Apixaban + Aspirin + Clopidogrel while 18/51 (35.3%) were on Warfarin + Aspirin + Clopidogrel. The rates of hemorrhagic and thrombotic events were similar among patients on different medication regimen. (Supplemental Table 1).
Discussion
This study compared the safety and efficacy of three antithrombotic regimens in patients with atrial fibrillation undergoing CAS. Our findings suggest no statistically significant differences in bleeding events or ischemic outcomes among different antiplatelet and anticoagulation regimens.
Patients on TT showed a trend towards lower ischemic events (1.9%) for both ischemic stroke and stent thrombosis, but slightly higher major bleeding (7.7%), while the AA group had a higher rate of stent thrombosis (6.5%). The DAPT group showed the highest rate of ischemic stroke (6.4%) but the lowest rate of major bleeding (3.2%), likely due to the absence of anticoagulation for cardioembolic protection. These non-significant trends suggest potential trade-offs between thrombotic protection and bleeding risk. The higher stent thrombosis rate in the AA group may indicate that a single anti-platelet agent combined with anticoagulation might be insufficient to prevent thrombosis of the stent.
Our results are similar to what has been previously reported. Pardo-Galiana et al also compared the efficacy and safety of different antithrombotic regimens in patients with atrial fibrillation undergoing CAS, albeit with a smaller sample size (n = 91) and shorter follow up. 13 Their results showed major hemorrhage in 23.4% of patients on triple therapy, compared to just 4% in the DAPT group and none in the antiplatelet and anticoagulant group. There was one instance of stent thrombosis in their antiplatelet/anticoagulant group and one cardioembolic stroke in the DAPT group. 13 A study by Nii et al. that included 17 patients receiving vitamin K antagonists plus DAPT and 14 patients receiving DOAC plus DAPT, reported one hemorrhagic event and one thromboembolic event in the vitamin K antagonist group, while no in-stent restenosis was observed at 6 months. 21 Variability in technique (eg, adjunctive angioplasty or type or stent used) and antithrombotic protocols, which can differ substantially across centers, may explain discrepancies in bleeding and thrombotic rates across studies. In contrast, in our larger cohort with longer follow-up, ischemic and bleeding event rates were similar across the three treatment groups.
The findings from our current study also align with the broader cardiovascular literature regarding antithrombotic therapy in patients with atrial fibrillation for patients undergoing coronary stent placement. Guidelines from the European Society of Cardiology (ESC) in 2023 recommend individualized approaches based on patient-specific thrombotic and bleeding risks, emphasizing the importance of regular risk assessment and treatment adjustment. 15 Sharma et al conducted a comprehensive analysis and reported comparable bleeding risks across different antithrombotic regimens in patients with atrial fibrillation undergoing percutaneous coronary intervention, with major bleeding rates ranging from 3%–5% across treatment groups. 22 A meta-analysis by Lopes et al showed decreased major bleeding events in patients on DAPT compared to triple therapy, namely a 47% reduction in major bleeding events compared to triple therapy (Hazard Ratio: 0.53, 95% CI: 0.36-0.85). 23 However, unlike previous studies, there was no difference in the incidence of ischemic stroke in the DAPT group or the triple therapy group (HR: 1.09, 95% CI: 0.57-2.08). The AUGUSTUS trial, a multicenter, randomized controlled trial comparing Apixaban with vitamin K antagonists and aspirin with placebo while on a P2Y12 inhibitor in patients whom underwent coronary stenting, provided valuable insights into treatment strategies. 24 It demonstrated that Apixaban and a P2Y12 inhibitor might offer a favorable balance between efficacy and safety in this patient population. Conversely, major or clinically relevant non-major bleeding occurred in 16.1% of patients receiving apixaban, a P2Y12 inhibitor, and aspirin (triple therapy) vs 9.0% receiving apixaban, a P2Y12 inhibitor and placebo (antiplatelet and anticoagulation) (HR 1.89; 95% CI, 1.59-2.24; P < 0.001). Although studies specifically evaluating triple therapy in acute carotid stenting are limited, evidence from antiplatelet regimens in related settings, such as tandem occlusions, may provide insights. For example, Diana et al performed a systematic review and meta-analysis of antithrombotic regimens in emergent carotid stenting for acute ischemic stroke due to tandem occlusions, including 34 studies with 1658 patients. They found no significant differences in the rates of symptomatic intracranial hemorrhage or in-stent thrombosis among patients receiving no antiplatelet therapy, single antiplatelet therapy, DAPT or glycoprotein IIb/IIIa inhibitors. 25 However, the impact of concomitant anticoagulation (ie, triple therapy) was not assessed. Therefore, further studies evaluating clinical outcomes in patients treated with triple therapy are warranted.
This study has significant limitations. First, this is a single-center retrospective study, and the relatively small sample size may have limited our ability to detect differences between groups. Furthermore, the generalizability of our findings to other populations or healthcare settings may be restricted. The retrospective design also introduces potential biases related to patient selection and data collection. In addition, our 3-month follow-up period may not have been adequate to capture long-term outcomes. However, thrombotic and hemorrhagic events do not commonly occur beyond 90 days.26,27 Consequently, we encourage further prospective multicentric studies analyzing this subset of patients. Finally, the heterogeneity in the types and dosages of antiplatelet and anticoagulant therapies across different providers could have influenced the observed results. However, this reflects a common real-world scenario in which physicians individualize medication regimens to optimize care for diverse patient populations.
Conclusion
In conclusion, our study suggests that DAPT, antiplatelet and anticoagulation therapy, and DAPT and anticoagulation, have similar safety and efficacy profiles in patients with atrial fibrillation undergoing CAS. These findings underscore the need for a personalized approach at the time of deciding the best regimen for patients who have atrial fibrillation and undergo CAS.
Supplemental Material
Supplemental Material - Secondary Prevention after Carotid Stenting in Patients With Atrial Fibrillation
Supplemental Material for Secondary Prevention after Carotid Stenting in Patients With Atrial Fibrillation Alex D Hanson, Diedo J Ojeda, Arshaq Saleem, Elena Sagues, Andres Gudino, Randall Krug, Edgar A Samaniego in Vascular and Endovascular Surgery.
Footnotes
Ethical Approval
The institutional review board at the University of Iowa approved the study.
Informed Consent
Waived the requirement for consent due to its retrospective design.
Author Contributions
Alex Hanson: Conceptualization, Methodology, Data Curation, Writing-Original draft preparation. Diego Ojeda: Data Curation. Arshaq Saleem: Data Curation. Elena Sagues: Methodology, Formal Analysis and Writing-Review and Editing. Andres Gudino: Data Curation. Randall Krug: Writing-Review and Editing. Edgar A Samaniego: Conceptualization, Methodology, Writing-Review,Editing and Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The patient data for this study is not online, but can be made available upon request, if appropriate.
Submission Declaration
This work has not been published before and it is not under consideration for publication elsewhere. The article is approved by all authors. If accepted, the article will not be published elsewhere in the same form, in English or in any other language, including electronically, without the written consent of the copyright-holder.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.