
Abstract
Background
Chronic mesenteric ischemia (CMI) can result from progressive atherosclerotic disease with symptoms arising in severe cases. Endovascular revascularization with a balloon-expandable covered stent is the preferred first-line treatment for CMI, but balloon deployment may be complicated by severe calcification in the mesenteric arteries. Techniques used to address severe calcification, such as open surgery revascularization and high-pressure, non-compliant balloon dilations, are associated with higher complication rates and calcium fracturing. Intravascular lithotripsy (IVL) is a novel technique to treat arterial calcifications in situ, having previously been used to target atherosclerotic lesions in the coronary and peripheral arterial beds.
Case Presentation
We present a 93-year old woman with a one year history of severe postprandial abdominal pain with an acute worsening of her mid-epigastric pain for two days. CTA showed severe calcifications at the origin of the superior mesenteric artery (SMA), which was confirmed and localized by an aortogram. Intravascular lithotripsy (IVL) was used to break down the calcification and prepare the SMA for stenting. Following IVL treatment, two overlapping covered stents were deployed and a final aortogram demonstrated patency of the SMA ostia with distal flow in the ileocecal branch.
Conclusion
IVL could be considered an adjunct to stenting in the setting of severe atherosclerotic disease in the visceral arteries when endovascular revascularization with stenting or balloon angioplasty is insufficient. Although IVL has been investigated in the treatment of calcifications in the coronary and peripheral arteries, it is necessary to explore IVL as a potential treatment for atherosclerotic lesions in the mesenteric arteries in a larger patient population.
Keywords
Background
Mesenteric ischemia can result from a chronic or acute occlusion of mesenteric vessels. Embolic occlusion is the most common culprit of acute mesenteric ischemia, while more than 90% of chronic mesenteric ischemia (CMI) is the result of progressive atherosclerotic disease. 1 In particular, CMI is estimated to be prevalent in 17.5% of elderly patients. 2 Patients may experience symptoms associated with severe atherosclerosis such as postprandial abdominal pain, weight loss, nausea or vomiting, early satiety, diarrhea or constipation, and bowel infarction. 1 First-line therapy for CMI typically involves endovascular revascularization with a balloon-expandable covered stent targeting the superior mesenteric artery (SMA) to rapidly reverse symptoms, restore nutritional status, and prevent acute-on-chronic mesenteric ischemia.3,4
However, calcification poses a barrier to stenting. Open surgery revascularization is an alternative, but it is associated with delayed return of bowel function and higher perioperative complications compared to endovascular approaches. 5 While there are techniques such as high-pressure non-compliant balloon dilation and specialty balloons to assist in revascularizing vessels with severe calcifications, such methods may lead to fracturing of the calcium or dissection. 6 There is also a lack of robust data establishing the safety and superiority of using specialty balloons that are scored, cut, or under high pressure.7,8
Intravascular lithotripsy (IVL) is a novel technique adapted from extracorporeal shock wave lithotripsy, used for the treatment of renal calculi, which delivers sonic pressure waves directly to the calculi, fracturing the calcium deposits. In the same vein, IVL generates spherical sonic pressure waves to disintegrate arterial calcifications in situ. 6 IVL has been studied and used in the treatment of extensive calcifications in coronary and peripheral arterial beds to fracture atherosclerotic lesions and prepare vessels for stenting.9-12 The DISRUPT CAD I - IV trials demonstrate the feasibility, safety, and efficacy of IVL to assist in treating severe coronary artery calcifications with a post-IVL luminal gain of 0.83 ± 0.47 mm and residual stenosis falling to 7.8 ± 7.1% post-IVL and stent placement.6,13 Similarly, the DISRUPT PAD III trial reported a luminal gain of 2.0 ± 0.7 mm with a residual stenosis <50% at the end of the procedure along with residual stenosis reduced to 23.3 ± 12.5%. 14 In theory, the use of IVL in peripheral and coronary arteries may be extended to the mesenteric arteries, where atherosclerotic lesions develop in a similar fashion. This is corroborated by the Clinical Practice Guidelines from the Society for Vascular Surgery which recommend approaching device selection and technical challenges to endovascular revascularization for CMI in the same way as other vascular beds. 15
IVL has not been extensively tested and used in visceral arteries, with few case reports of IVL use in the superior and inferior mesenteric artery.16-20 This case presentation demonstrates technical success and revascularization using IVL as an adjunct to stenting in the setting of severe SMA calcifications.
Case Presentation
A 93-year old woman presented with a one year history of severe postprandial abdominal pain with an acute worsening of her mid-epigastric pain for two days. She had a past medical history of hypertension, hyperlipidemia, coronary artery disease, peripheral vascular disease, and celiac/superior mesenteric stenosis. The patient was previously hospitalized a month prior to her presentation due to abdominal pain from enterocolitis, but a severely stenotic SMA and celiac trunk were incidentally discovered on computed tomography angiography (CTA). After her discharge, she continued to have postprandial pain with associated nausea and vomiting prompting another admission. After returning to the emergency department for abdominal pain, a repeat CTA demonstrated the severely stenotic SMA and excluded other causes of abdominal pain for this admission (Figure 1). Due to the patient’s advanced age and comorbidities, she was deemed high-risk for surgery and was subsequently referred for an SMA stent placement. Written consent was obtained from the patient before the procedure. CTA showing severe calcification at the origin of the superior mesenteric artery and celiac trunk.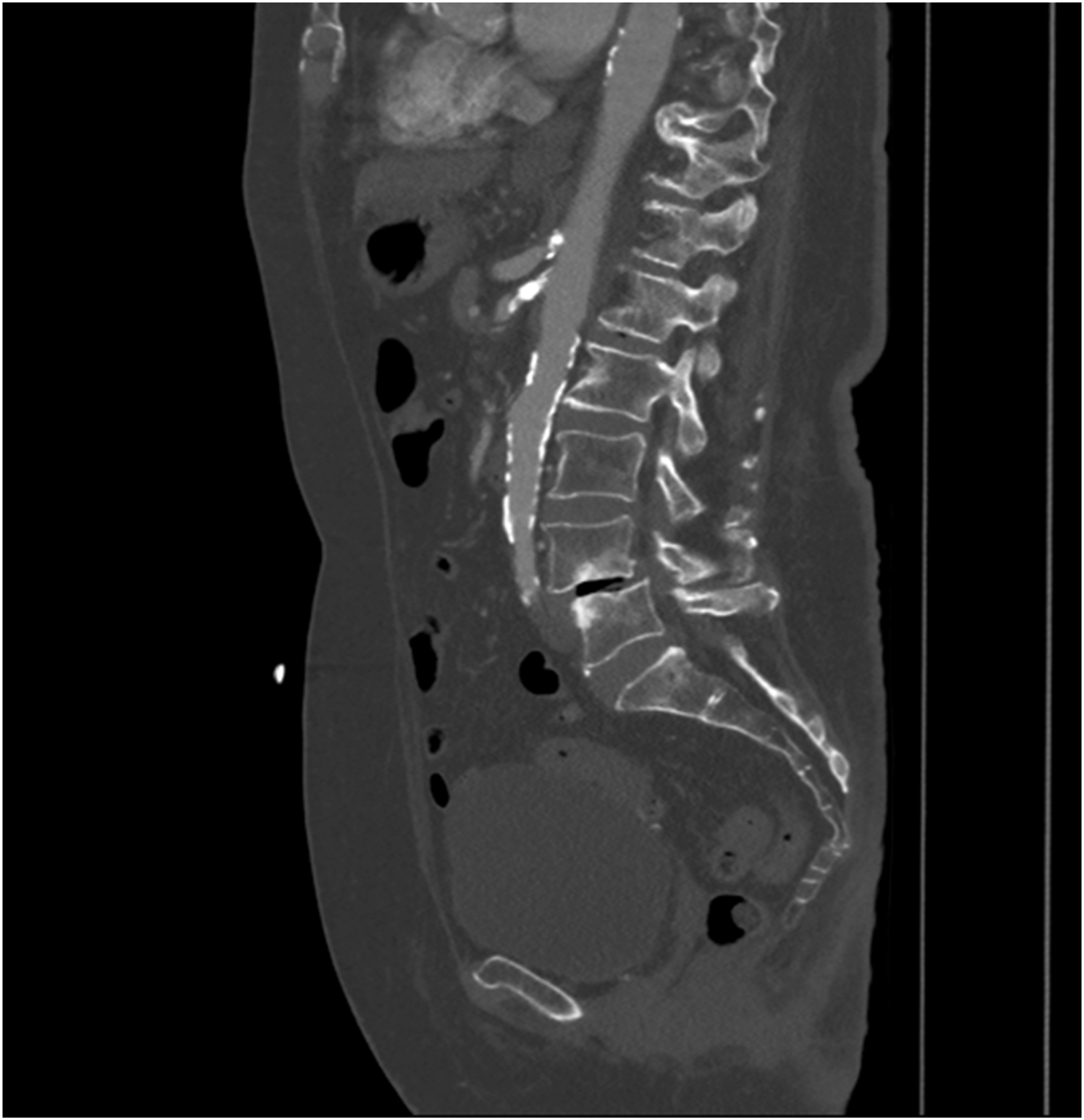
Since the right common femoral artery demonstrated heavy calcification, vascular access was established in the left common femoral artery under ultrasound guidance. An 8 Fr x 45 cm vascular sheath was placed over a 0.035 inch Bentson wire (Cook Medical, Bloomington, IN) into the common femoral artery. A 5-Fr Omniflush catheter (Angiodynamics, Latham, NY) was advanced over the 0.035 inch wire into the abdominal aorta. An aortogram was performed, demonstrating known critical stenosis of the celiac artery with poststenotic dilatation and a complete total occlusion of the SMA ostium due to critical ostial stenosis with distal opacification, likely due to retrograde filling from collateral vessels in the abdomen (Figure 2). An aortogram was performed to localize the stenosis of the superior mesenteric artery.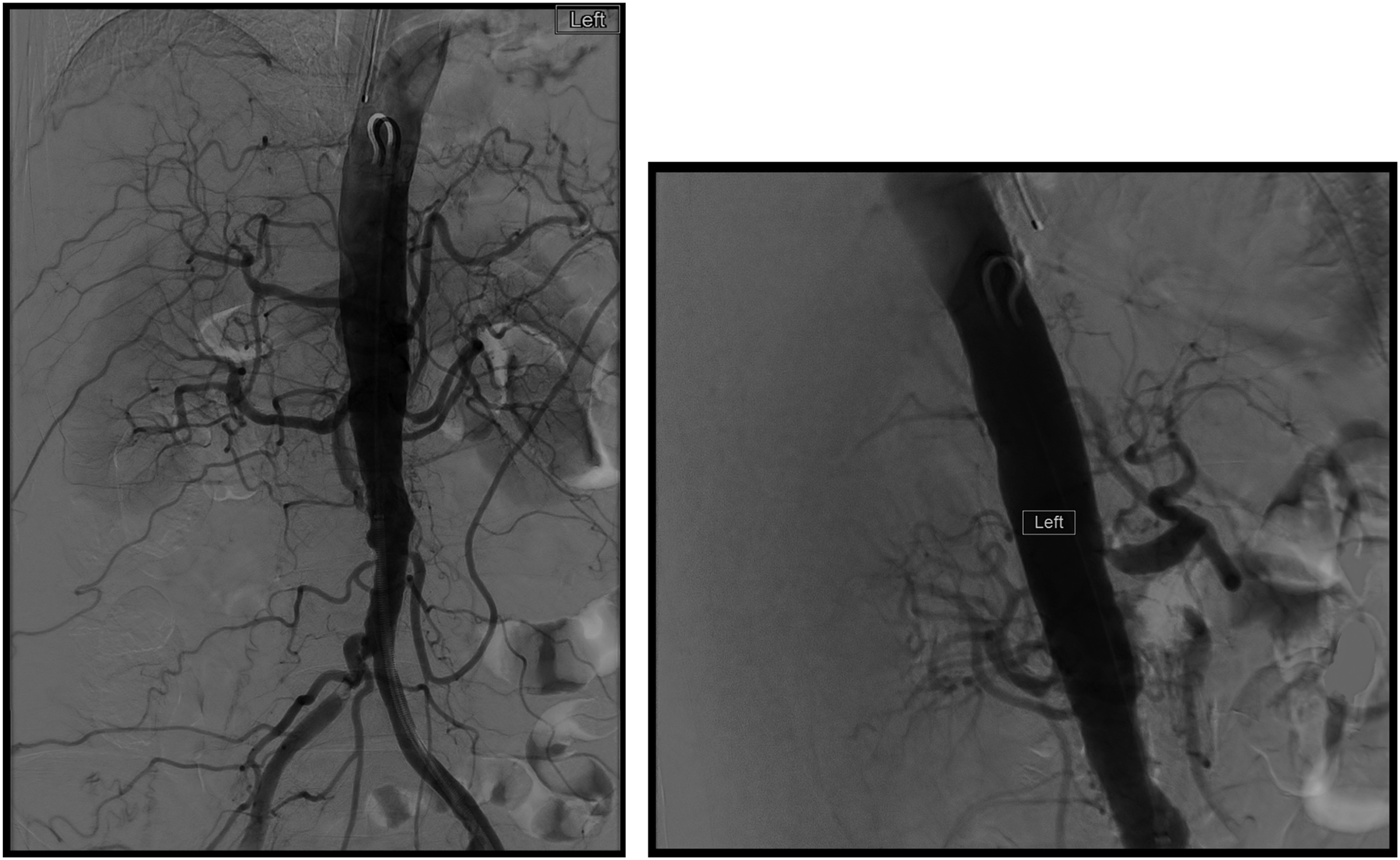
The Omniflush catheter (Angiodynamics, Latham, NY) was then removed, and the SOS2 catheter (Angiodynamics, Latham, NY) was used to engage the superior mesenteric artery with a Glidewire. The SOS2 catheter (Angiodynamics, Latham, NY) was then exchanged for a straight 0.035 × 135 cm Navicross catheter (Terumo, Tokyo, Japan), which was used to catheterize the distal ileocolic artery with a hydrophilic wire. This wire was then exchanged for a 260 cm Rosen wire (Cook, Bloomington, IN), and the sheath was advanced to the level of the SMA. A 4 × 40 cm Mustang balloon (Boston Scientific, Malborough, MA) was advanced over a wire to the SMA ostium and dilated to nominal pressure. Imaging after the dilation demonstrated elastic recoil of the stenosis. The 0.014 × 300 cm Spartacore (Abbott, Abbott Park, IL) was then inserted into the Mustang balloon. The Mustang and Rosen wire were then removed. Then, a 6 mm × 8 cm Shockwave™ Intravascular Lithotripsy Balloon (Shockwave Medical Inc., Santa Clara, CA) was advanced over the wire to the SMA ostium. Intravascular lithotripsy with Shockwave™ IVL balloon was performed (Figure 3). A Shockwave Lithotripsy Balloon (6 mm × 8 cm) was advanced to the SMA ostium. 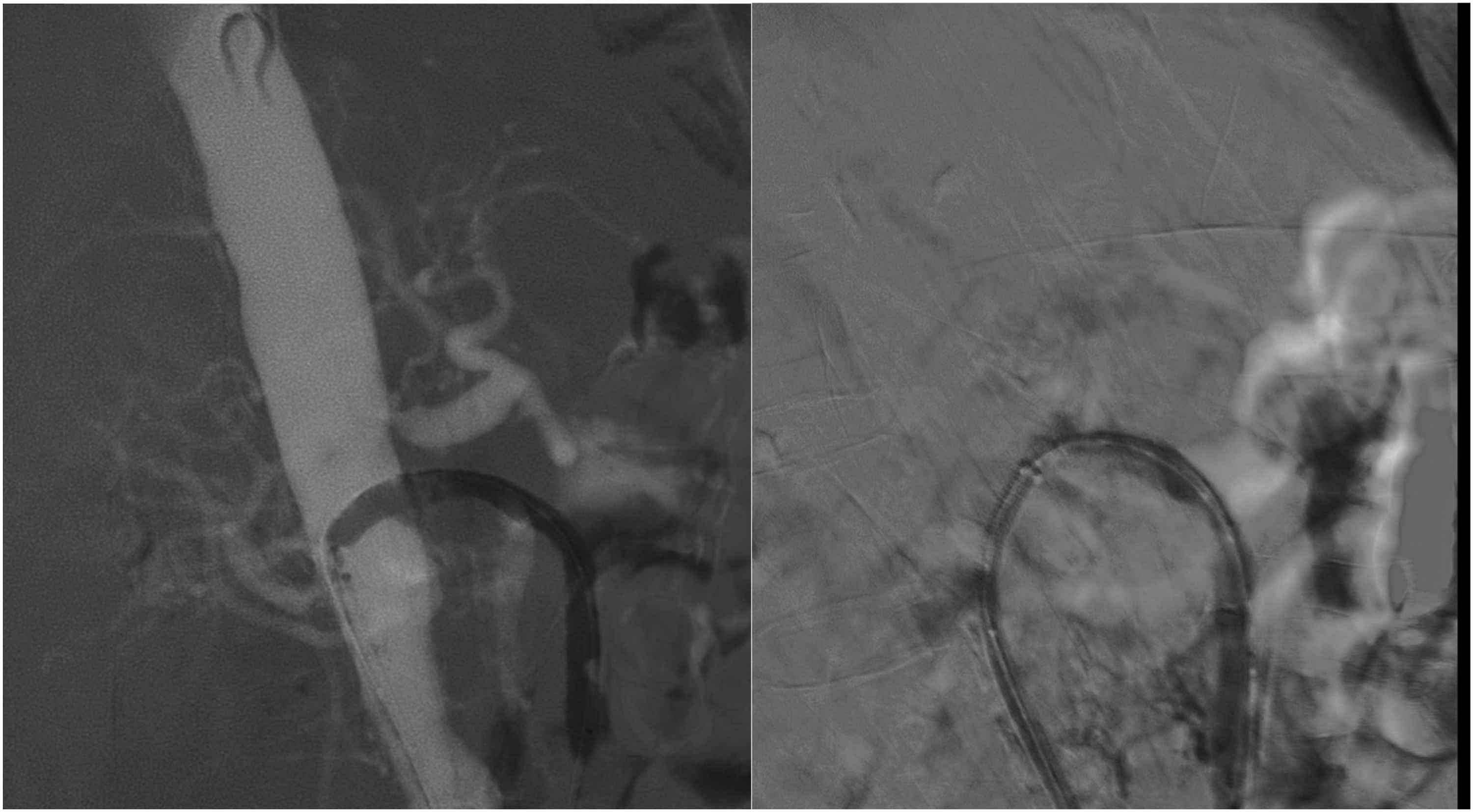
Post lithotripsy angiography through the sheath showed flow within the proximal SMA and collateral vessels. The sheath was advanced across the residual SMA ostial stenosis. A 7 mm × 39 cm ViabahnVBX stent (Gore, Newark, DE) was advanced over a Rosen wire, unsheathed, and deployed. Then, an overlapping 7 mm × 29 cm Viabahn VBX stent (Gore, Newark, DE) was advanced over the wire, unsheathed with the proximal portion just proximal to the SMA origin and deployed (Figure 4). Angiograms were performed, showing flow within the proximal SMA through the newly placed stent. (Left) Deployment of a 7 mm × 39 cm ViabahnVBX stent. (Right) Deployment of an overlapping 7 mm × 29 cm Viabahn VBX stent. 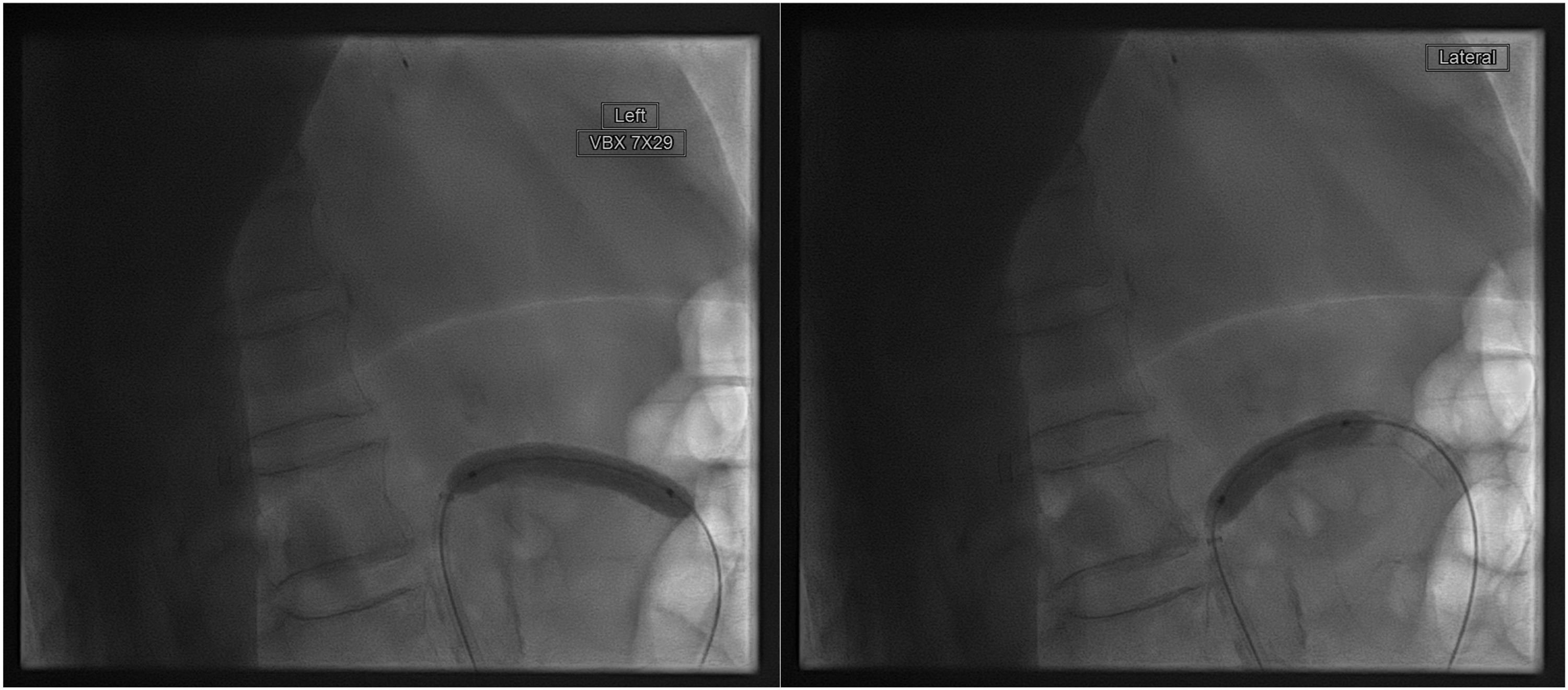
Post-angiography was performed via the sheath, demonstrating improvement of flow within the distal SMA ileocolic branch and patency of the SMA ostia (Figure 5). The patient’s postprandial pain resolved immediately following the procedure. She was able to eat dinner the night after the procedure without pain. She also had no pain the following morning and was subsequently discharged the next day. Her postprandial pain remained absent on two month outpatient follow-up. An arteriogram after the IVL and stent treatment showed patency of the SMA ostia with flow in the distal SMA ileocolic branch. 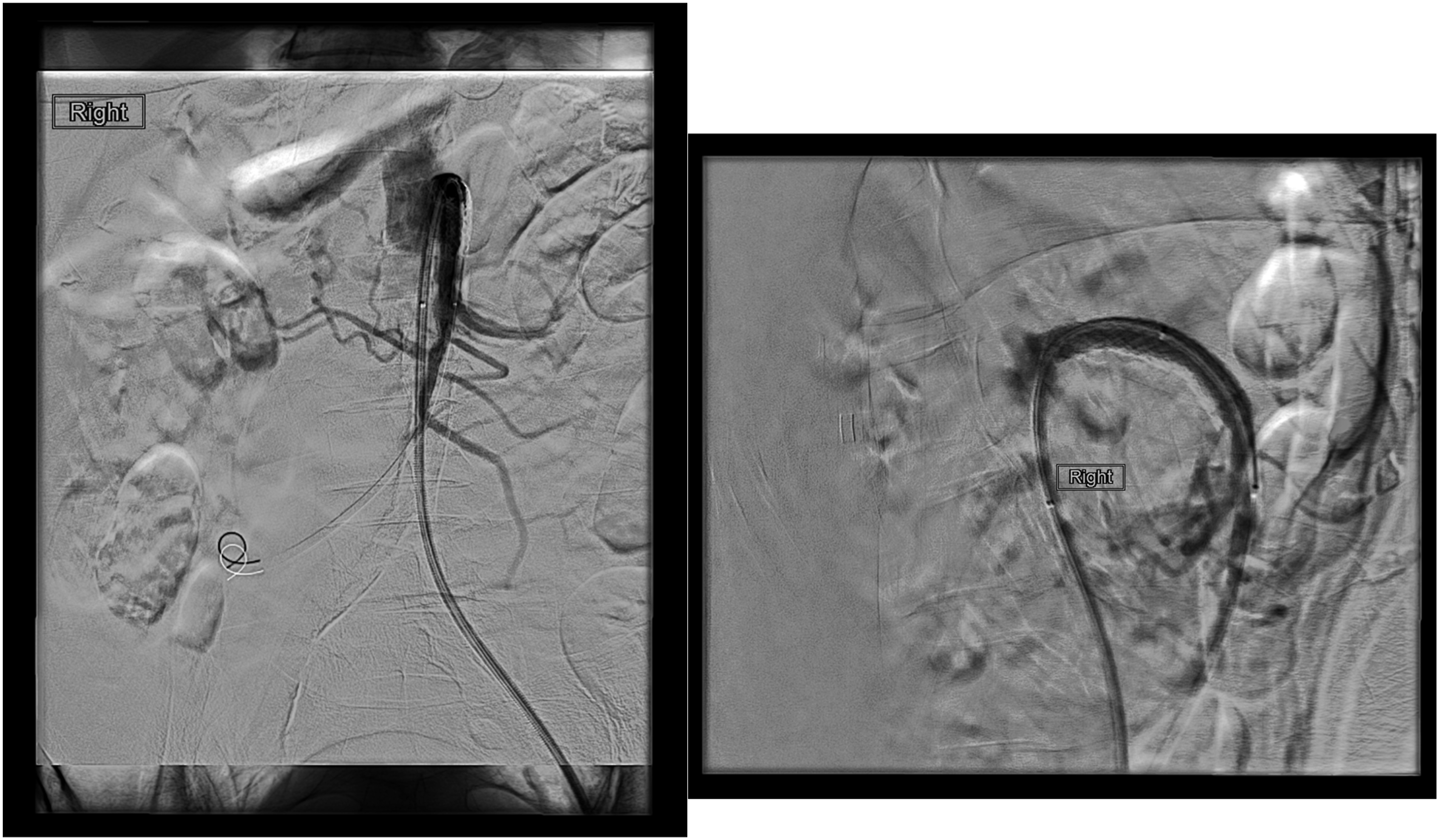
Discussion
To date, there are only a few documented cases of IVL being used for mesenteric ischemia due to atherosclerotic disease.16-20 There are even fewer reported cases in which IVL is used prior to stenting in the visceral arteries. In a single center, use of IVL prior to stenting achieved a primary patency rate of 95% at six months and one year, suggesting that IVL may be safely and effectively used prior to stenting the mesenteric arteries. 21
This case supplements the body of documented cases in which intravascular lithotripsy has been safely used in the visceral arteries—particularly the SMA—and corroborates findings that IVL can be used as an adjunct to prepare for stent placement. IVL prepares the vessel for stenting by fracturing the calcification in a stenotic vessel in a setting where traditional angioplasty is limited by excessive atherosclerotic disease. Previous studies have shown that severely calcified stenoses cause external compression and inadequate expansion of stents which may result in stent recoiling and restenosis.22,23 Elastic recoil of the stenosis was confirmed on imaging following a preliminary dilation of the Mustang balloon. In this particular patient, significant calcifications in the SMA would have prevented the expansion of the stent and IVL was used to restore the vessel lumen.
Additionally, a VBX covered stent was selected due to relatively higher primary patency rates, higher long term patency, and lower rates of restenosis when compared to bare metal stents.24,25 Cost is often cited as a benefit of bare metal stents: covered stents can cost three to five times more than bare metal stents. 26 While bare metal stents may be less costly in the short term, the reduction of reinterventions and hospitalizations associated with covered stents may be more cost effective in the long term. Fewer repeated procedures would translate to a lower cumulative cost of healthcare expenses. In using IVL together with VBX covered stents, technical success and stent patency was achieved with resolution of the symptoms immediately after the procedure and on two month follow-up.
The high cost of the shockwave lithotripsy catheter should also be considered when using this device for mesenteric interventions. While device cost to a particular hospital system is negotiated with the manufacturer and is therefore confidential, a 2020 study reported a retail price of $3450. 27 Because of its longer history in coronary and peripheral interventions, additional reimbursement is available for these indications. For coronary lithotripsy, reimbursement is available through add-on Current Procedural Terminology (CPT) codes. For peripheral lithotripsy, reimbursement is available via Category C Healthcare Common Procedure Coding System (HCPCS) codes for outpatients and International Classification of Diseases −10 - Procedural Coding System (ICD-10-PCS) for inpatients. 28 These mechanisms for additional reimbursement for a novel device are not yet available for mesenteric lithotripsy; therefore, typical reimbursement for angioplasty and stenting may not be high enough to cover the cost of this device. Further study of the safety and efficacy of IVL for mesenteric indications will be important in developing such reimbursement mechanisms in the future.
Conclusion
IVL can be considered prior to stenting in instances where endovascular revascularization is suboptimal, particularly when there is evidence that the SMA is severely calcified. Although IVL has been investigated in the treatment of coronary and peripheral arteries, its safety, feasibility, and efficiency has not yet been established in the visceral arteries in a larger patient population. Large, multicenter studies are necessary to further investigate the value of IVL both prior to stenting and as a potential treatment for severe mesenteric artery calcifications to expand reimbursement mechanisms and facilitate methods of mesenteric recanalization. This case presentation underscores the value of IVL as a tool to revascularize and prepare a severely calcified SMA for stenting.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.