
Abstract
Objective
To evaluate outcomes in patients with type 2 endoleak (T2E) and the impact of treatment outside the device instructions for use (IFU).
Methods
This retrospective single-center study included abdominal aortic aneurysms (AAA) patients who underwent EVAR (2011- 2024). Primary outcomes were 30-day and mid-term complications, reintervention, and mortality by T2E status. Propensity score matching was applied and secondary analysis stratified outcomes by IFU compliance, comparing within (inIFU) or outside(outIFU) IFU in each T2E group.
Results
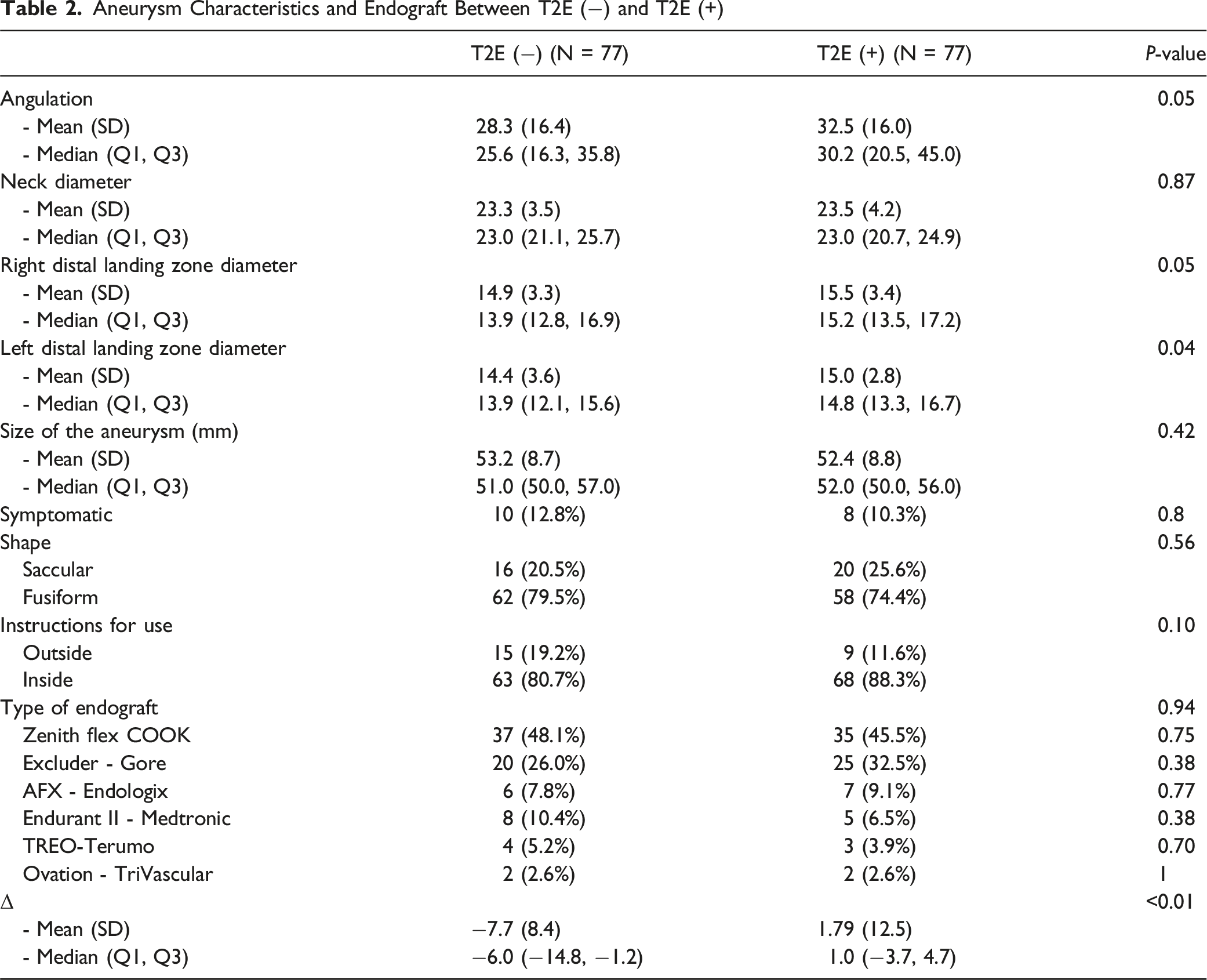
Among 154 EVAR patients (137 men (89.1%) and 17 women (11.0%); mean age 77.5 ± 7.6 years), 77 were T2E(−), and 77 were T2E(+). Baseline characteristics were similar. Thirty-day complications were comparable (T2E(−): 5, 6.4% vs T2E(+): 2, 2.56%, P = 0.72). The mean follow-up duration was 2.7 ± 2.4 years. Sac diameter change (Δ) decreased in the T2E(−) (7.7 ± 8.4 mm) and enlarged in the T2E(+) (1.79 ± 12.5 mm; P < 0.01). Mid-term graft-related complications (T2E(−): 3, 3.8% vs T2E(+): 49, 62.8%, P < 0.01) and reinterventions (T2E(−): 3, 3.8%, vs T2E(+): 20, 25.6% P < 0.01) were higher in the T2E(+) with no difference in mortality (P = 1.00). These findings remained after excluding type 1 endoleaks. Among the T2E(+), those treated outIFU had longer hospital stays (outIFU: 3.0 ± 2.8 days vs inIFU: 1.8 ± 2.0 days, P = 0.03), higher T1E (outIFU: 3, 33.3% vs inIFU: 1, 4.34%, P < 0.01), higher rates of reintervention (outIFU: 9, 100.0% vs inIFU:17; 24.6%, P < 0.01) and higher all-cause mortality than those within IFU criteria (outIFU: 5, 55.0% vs inIFU: 13, 18.8%, P < 0.01). IFU status did not significantly affect outcomes in T2E(−) patients.
Conclusions
T2E is associated with sac growth and increased reinterventions, but not higher mortality. On subgroup analysis, those T2E(+) treated outIFU had longer hospitalizations, higher T1E rates, more reinterventions, and higher all-cause; but not aneurysmal-related mortality.
Keywords
Introduction
Endovascular aortic aneurysm repair (EVAR) has become the treatment of choice for most infrarenal abdominal aortic aneurysms (AAA). However, it has been associated with a greater need for reintervention than an open repair within the first 3 years post-intervention (9% vs 1.7%). 1 The most common indications for reinterventions after EVAR are endoleaks and aneurysmal sac growth. 2 One of the risk factors for these reinterventions is reportedly non-compliance with the instructions for use (IFU) criteria. 3 In recent years, there has been an increase in the number of patients who undergo EVAR outside the IFU, with a prevalence of up to 40%. 4 Complex aortic anatomy and avoidance of the risk of an open operation are reported reasons to perform EVAR outside of IFU. 5 In this setting, we hypothesize that an incomplete seal with a concomitant T2E can sustain sac pressurization, which may lead to sac enlargement and worse outcomes.
Our study aims to evaluate outcomes between patients treated for AAA with EVAR with subsequent type 2 endoleak (T2E). The primary outcome is 30-day and mid-term complications, reintervention rate, and mortality after EVAR with and without T2E. The secondary outcome is to determine whether these outcomes differ based on adherence to IFU.
Methods
Study Design and Patient Cohort
We identified all patients who underwent EVAR for AAA repair within our institution from 2011 to 2024. Data extraction was performed using the electronic medical record. Our institutional review board (IRB) approved this project (IRB# 24-004735). EVARs during this cohort period were performed by 3 board certified vascular surgeons. Although our analytic cohort begins in 2011, EVAR has been established by our institution since 2002. Patient consent was waived due to the study’s retrospective nature and the subjects’ lower-than-minimal risk. All information was collected sequentially in an encrypted database to ensure patient confidentiality of personal information, reducing the risk of information and selection bias by retrieving the data as needed. We excluded patients who underwent open thoracoabdominal, suprarenal, pararenal, juxtarenal, and fenestrated EVAR repair for an objective comparison.
Measures and Definitions
Patient demographic information, comorbidities, aneurysm details, surgical variables, and 30-day and mid-term complications were collected. Comorbidities included for analysis are as listed in the SVS practice guidelines and include hypertension, diabetes mellitus, hyperlipidemia, smoking history, chronic kidney disease, chronic obstructive pulmonary disease, coronary artery disease, atrial fibrillation, and stroke. 6 T2E was defined as an endoleak identified on the final intraoperative angiogram that persisted during follow-up, or as a newly detected T2E on follow-up computed tomography angiography (CTA). To identify a new and/or persistent T2E, all completion angiograms and subsequent follow-up CTAs were reviewed for endoleak presence. On CTA, T2E required arterial and/or delayed-phase sac opacification contiguous with the IMA or lumbar arteries with a visible feeder/collector. In patients who underwent embolization, selective angiography was used to confirm the collateral feeders. Follow-up CTA was performed at 30 days, 6-12 months, and annually thereafter, with earlier imaging if concerns arose, in accordance with SVS surveillance guidelines. 6 The decision to proceed with embolization of the T2E was based on aneurysm sac growth and rate of growth. This decision was made by a multidisciplinary team comprising vascular surgeons and interventional radiologists following current SVS guidelines of aneurysmal sac growth of >5 mm and our own team’s experience. 6 At our institution, prophylactic embolization of the IMA or lumbar arteries is not routinely performed.
The aortic diameter was measured in cross-sectional imaging by a board-certified vascular radiologist and subsequently verified by a board-certified vascular surgeon utilizing centerline measurements. To calculate the change (Δ) of aortic diameter, we compared the pre-operative CTA diameter with all available CTA on follow-up. Sac enlargement was defined as any increase in sac diameter, a positive Δ indicates sac enlargement, while a negative Δ indicates sac reduction/shrinkage. In patients who underwent embolization, sac diameter was recorded before and after the procedure; for the analysis of sac enlargement, the most recent post-embolization CTA measurement was used. To determine patients, who underwent EVAR within (inIFU) or outside IFU (outIFU), we measured the aortic neck length, diameter, angulation, and distal landing zone diameters with 2 separate imaging software (QREADS V.5.15.3, Rochester, MN) and VISAGE V.7.1.18 (San Diego, CA) 7 with centerline capabilities. The IFUs available at the time of implantation for each of the 6 devices were obtained from the respective manufacturers’ websites (Supplemental Figure 1).
Group and Subgroup Identification
Patients were divided into 2 groups: 1) T2E (−) was defined as the absence of T2E or T2E present on completion angiography at the index operation with spontaneous resolution on follow-up CTA, and 2) T2E (+) as the presence of newly diagnosed T2E or persistent T2E previously visualized on completion angiography at the index operation and present subsequently thereafter on CTA. In addition, a parallel analysis excluding patients with concomitant type 1 endoleak (T1E) was performed to assess outcomes of pure T2E. For subgroup analysis, we further stratified them according to adherence to the IFU criteria on their index EVAR. If all aortic measurements met IFU criteria, the patient was categorized as inIFU. If one of the measurements failed to meet the requirements, the patient was classified as outIFU.
Outcomes
The primary outcomes are 30-day and mid-term complications, reintervention, and mortality after EVAR with and without T2E. Secondary outcomes included 30-day and mid-term complications, reinterventions, and mortality stratified by IFU compliance. Thirty-day complications included any surgical event from discharge to 30 days after the procedure. Mid-term complications included any complication related to the index procedure after 30 days. Reintervention was defined as any post-EVAR procedure performed to address endograft-related complications, including embolization, T1E repair, graft explant, or catheter-directed thrombolysis. Reinterventions were analyzed at the event level; patients undergoing multiple procedures contributed one count per event. Cause of death was determined using the National Death Index (NDI) and verified against the institutional electronic medical record when available.
Statistical Analysis
Statistical analysis was performed using R Studio v4.4.1. We assessed normal distribution with the Shapiro-Wilk test. The Mann-Whitney U test was used for continuous variables with non-normal distribution, and the independent T-test was used for normally distributed ones. Pearson’s Chi-squared test was used for categorical variables, and Fisher’s exact test for small sample sizes. We first presented an analysis of the unmatched cohort. The baseline characteristics and anatomic features are summarized by T2E status in Supplemental Tables 4A and 4B, unadjusted outcomes in Supplemental Table 4C. We then performed a propensity-score matching was used to compare patients with and without T2E, controlled for potential confounders identified preliminarily in bivariate analysis of the initial dataset. A 1:1 nearest-neighbor matching algorithm was used, and standardized mean differences (SMDs) were calculated to assess covariate balance before and after matching, with SMD <0.1, as an indicator of acceptable balance. An additional matching process was conducted after excluding patients with concomitant T1E using the same matching methodology to evaluate outcomes in patients with isolated T2E. We also performed a subgroup analysis within T2E(+) comparing outcomes by anticoagulation use at the time of EVAR. Cox proportional hazards regression analysis was performed to estimate hazard ratios (HR) and corresponding 95% confidence intervals (CI) for mid-term graft-related complications, reinterventions, and mortality to further control selected confounders. Multivariate models included variables with P < 0.1 in univariate analysis. Variables included in the univariate and multivariate models for mid-term complications and reintervention included Δ sac, T2E status, and IFU compliance. For mortality, the Charlson Comorbidity Index (CCI) was additionally included to account for baseline comorbidity burden. The concordance index (C-index) was calculated to assess the predictive accuracy of the Cox model. These analyses were conducted for both the full matched cohort and the T1E-excluded group. A Kaplan-Meier survival analysis was used to measure mid-term complications, reinterventions, and mortality, with the log-rank test to compare survival between groups. A P-value of <0.05 was considered statistically significant for all analyses performed.
Results
Patient Demographics
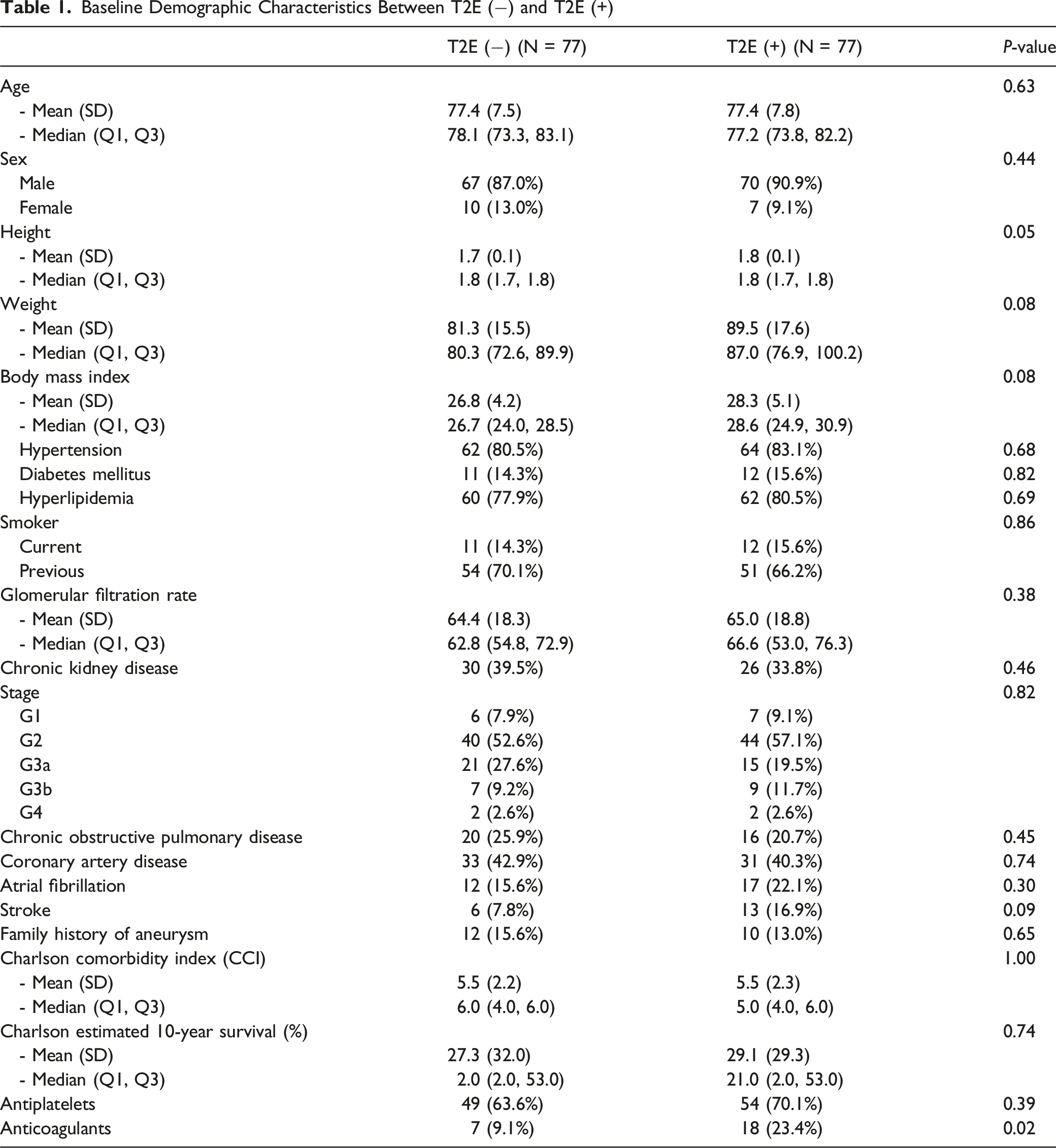
Baseline Demographic Characteristics Between T2E (−) and T2E (+)
Preoperative and Postoperative Aneurysm Characteristics
Aneurysm Characteristics and Endograft Between T2E (−) and T2E (+)
Thirty-Day Complications
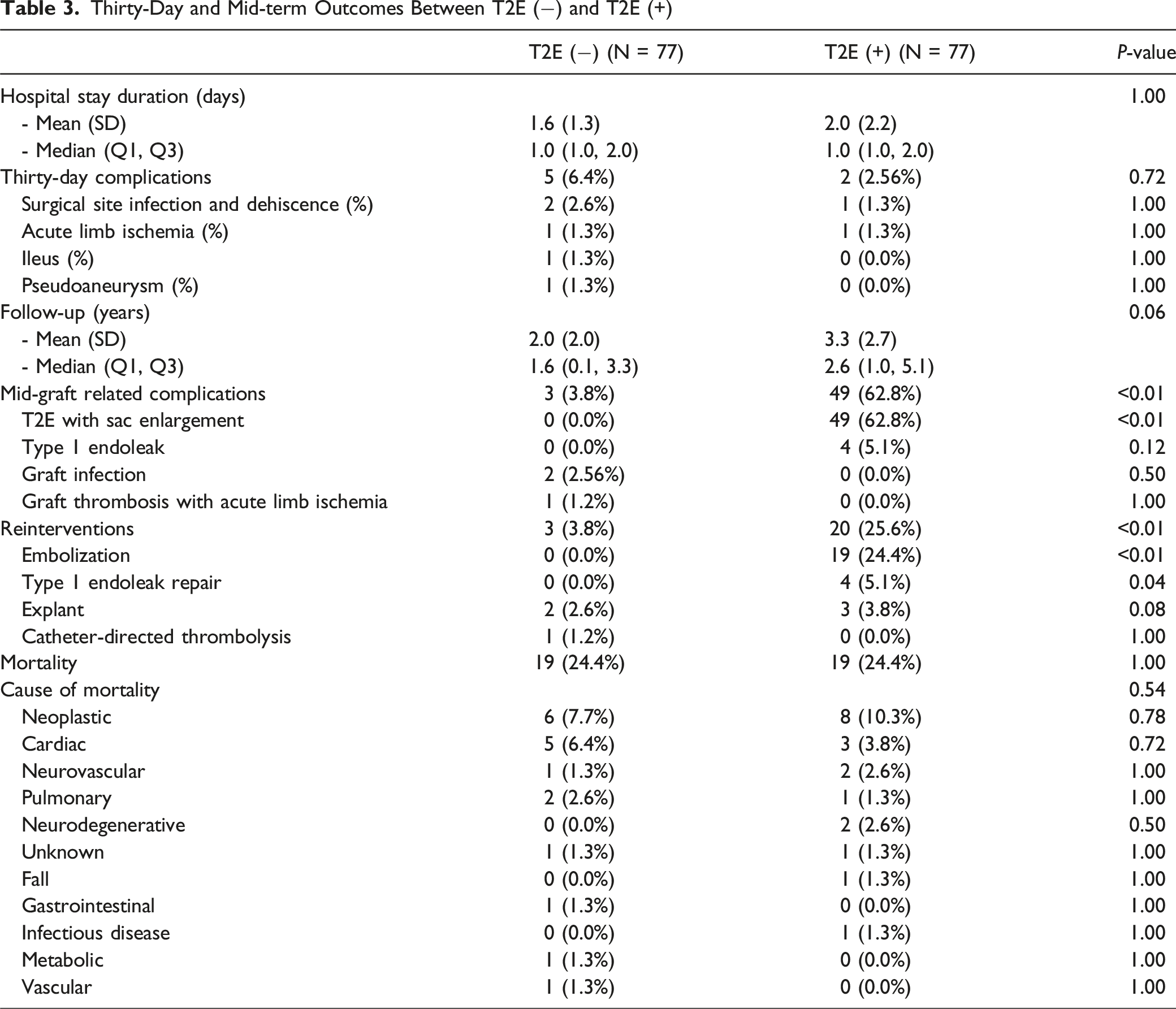
Thirty-Day and Mid-term Outcomes Between T2E (−) and T2E (+)
Mid-term Complications, Reinterventions, and Mortality
The mean follow-up of the entire cohort was 2.7 ± 2.4 years, with a maximum of 10 years. Graft-related complications at follow-up were more common in the T2E (+) group compared to the T2E (−) group (T2E (−): 3, 3.8% vs T2E (+): 49, 62.8%; P < 0.01). T2E with sac enlargement was the most common complication, exclusively found in the T2E group (+) (T2E (−): 0, 0% vs T2E (+): 49, 62.8%; P < 0.01). All other complications are as follows: T1E (T2E (−):0, 0.0% vs T2E (+): 4, 5.1%; P = 0.12), graft infection (T2E (−): 2, 2.56% vs T2E (+): 0, 0.0%; P = 0.5) and graft limb thrombosis with ALI (T2E (−): 1, 1.2% vs T2E (+): 0, 0.0%; P = 1.00).
Graft-related reinterventions were more common in the T2E (+) group compared to the T2E (−) group (T2E (−): 3, 3.8% vs T2E (+): 20, 25.6%; P < 0.01). The most common reintervention was T2E embolization (T2E (−): 0, 0.0% vs T2E (+): 19, 24.4%; P < 0.01) followed by T1E repair (T2E (−): 0, 0.0% vs T2E (+): 4, 5.1%; P = 0.04), graft explant (T2E (−): 2, 2.6% vs T2E (+): 3, 3.8%; P = 0.08), and catheter direct thrombolysis (T2E (−): 1, 1.2% vs T2E (+): 0, 0.0%; P = 1.00), Table 3
Based on the sac diameter Δ, we found that within T2E (+), 63% had sac enlargement, but only 24.7% had more than 5 mm growth. All 4 patients with T1E were in the T2E (+) group, with concomitant T2E. In all cases, the T1Es were diagnosed after the T2E diagnosis, with a mean time of diagnosis of T1E after T2E of 1.74 ± 0.68 years. Three of the 4 T1Es were distal T1E, managed with iliac limb extensions, while the remaining case was a proximal T1E, treated with proximal coil embolization and proximal balloon angioplasty. Three of the 4 cases were initially repaired outside IFU.
Two explants occurred in the T2E (−) group and 3 in the T2E (+) group (P = 0.08). In the T2E (−) group, both explants were due to an infected endograft, one caused by Staphylococcus haemolyticus, and the other was attributed to Staphylococcus aureus. The explants occurred 1.6 ± 1.1 years after the EVAR procedures, both of which were performed inIFU. The patients were treated with axillo-bifemoral artery bypass and aortic ligation. In the T2E (+) group, all explant cases involved patients with concurrent T2E and T1E, where the T1E were diagnosed after the T2E. Among these explants, one patient had a proximal T1E that was treated with coil embolization and balloon angioplasty, which failed to resolve the proximal endoleak. The patient underwent explant 4 years after initial outIFU EVAR. A second patient underwent an explant 2 years after an initial outIFU EVAR due to a failed distal T1E repair, which led to rupture. The third explant was performed at an outside institution 6 years after inIFU EVAR, and it was noted to have lost proximal seal.
Mortality was identical between the groups (T2E (−): 19, 24.4% vs T2E (+): 19, 24.4%; P = 1.00). The most common cause of mortality was cancer-related (T2E (−): 6, 7.7% vs T2E (+): 8, 10.3%; P = 0.78), followed by cardiac causes (T2E (−): 5, 6.4% vs T2E (+): 3, 3.8%; P = 0.72). Only one vascular-related mortality was reported in T2E (−), Table 3.
After excluding patients with T1E, mid-graft related complications remained significantly more common in the T2E (+) group compared to the T2E (−) group (45, 60.8% vs 3, 4.1%, P < 0.01), primarily due to sac enlargement. Reinterventions were also more frequent in the T2E (+) group (17, 23.0% vs 2, 2.7%, P < 0.01). Causes of death did not significantly differ between groups (P = 0.84), Supplemental Table I.
Subgroup Analysis - Type 2 Endoleak Patients and Instructions for Use
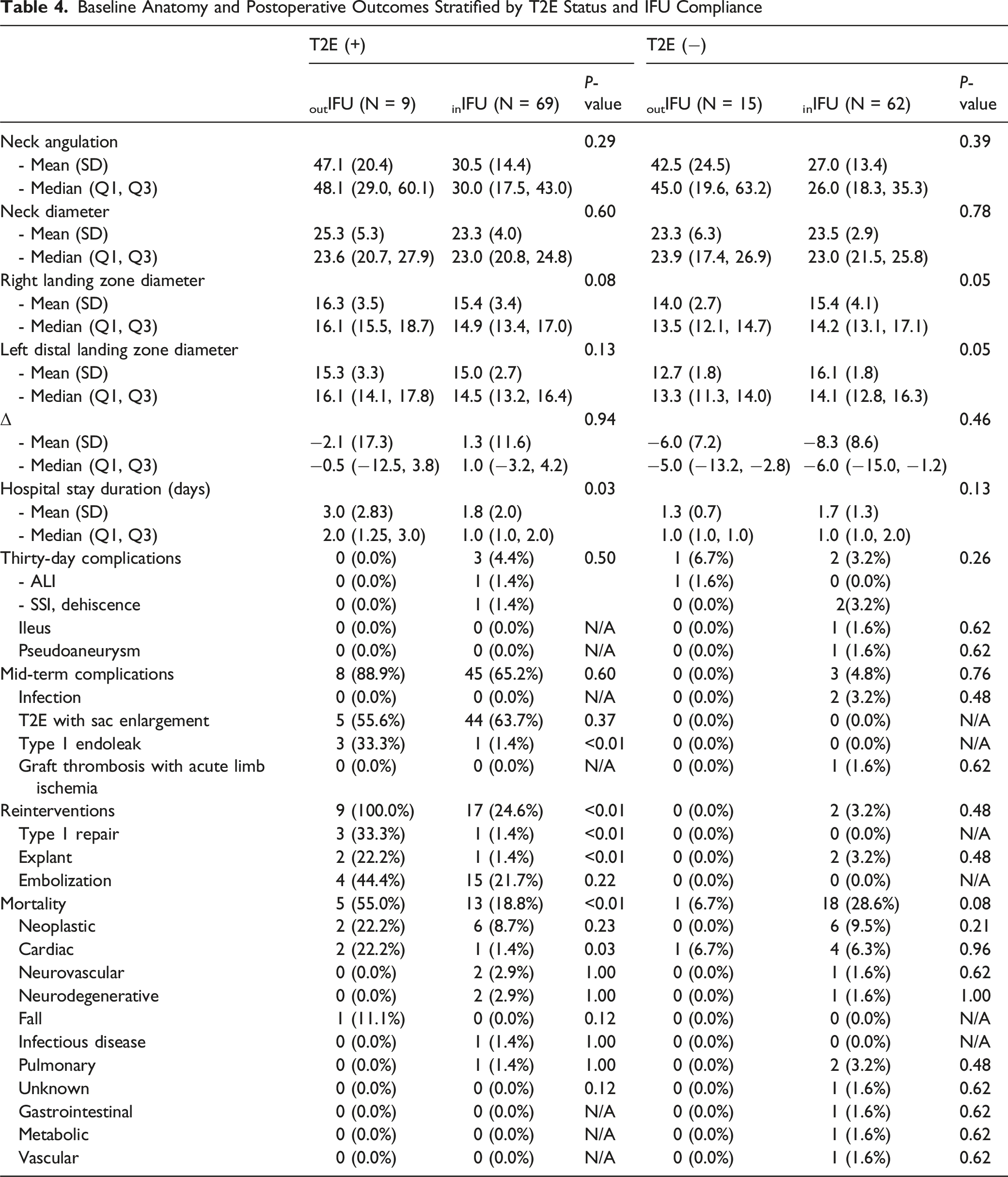
For this sub-analysis, we stratified based on IFU compliance. From the 77 T2E (+) patients, a total of sixty-eight (87.1%) patients were inIFU and 9 (11.6%) were outIFU. The reasons for being outIFU included severe neck angulation in 3 patients, larger neck diameter in 2 patients, insufficient neck length in 2 patients, and inadequate distal landing zone in 2 patients. Observed differences only included mean hospital length of stay (outIFU: 2.8 ± 3.3 days vs inIFU:1.8 ± 2.0 days; P = 0.03).
Regarding the outcomes, no difference was found in the 30-day complication rate between groups (outIFU: 0, 0.0% vs inIFU: 3, 4.4%; P = 0.50). Similarly, mid-term graft-related complications and T2E with sac enlargement rates, occurred at comparable rates (outIFU: 8, 88.9% vs inIFU: 45, 65.2%; P = 0.60), (outIFU: 5, 55.6% vs inIFU: 44, 63.7%; P = 0.37), respectively. However, T1E rates were higher in the outIFU group than in the inIFU group (outIFU: 3, 33.3% vs inIFU: 1, 1.4%; P < 0.01).
Graft-related reintervention was significantly more frequent in the outIFU group (outIFU: 9, 100.0% vs inIFU:17; 24.6%, P < 0.01), with T1E repairs (outIFU: 3, 33.3% vs inIFU:1; 1.4%, P < 0.01), and explants (outIFU: 2, 22.2% vs inIFU:1; 1.4%, P < 0.01) occurring at significantly greater rates. Embolization rates, however, did not differ between groups (outIFU: 4, 44.4% vs inIFU: 15, 22.1%; P = 0.22). All-cause mortality was significantly higher in outIFU (5, 55.0%) compared to inIFU (13, 18.8%, P < 0.01), with a higher cardiac-related mortality (outIFU: 2, 22.2% vs inIFU: 1, 1.4%, P = 0.03). No vascular-related mortality was noted.
Baseline Anatomy and Postoperative Outcomes Stratified by T2E Status and IFU Compliance
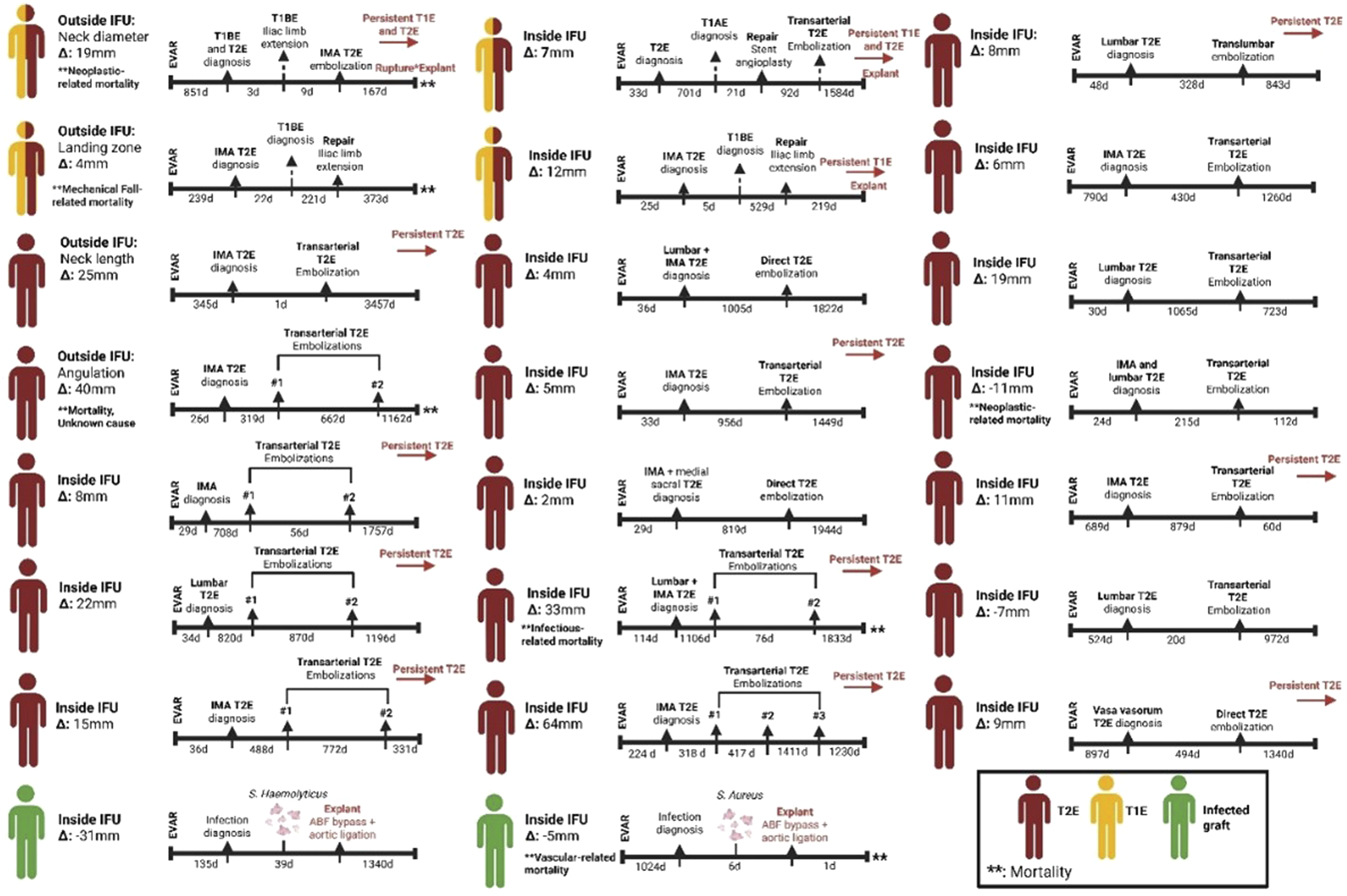
Case-Specific Timeline Overview of Patients With T2E that had Embolization, T1E, and Infected Grafts
Subgroup Analysis - Type 2 Endoleak Patients and Anticoagulation
Among 77 T2E(+) patients, 18 (23%) were on anticoagulation at EVAR and 59 (77%) were not. Sac Δ was similar (mean 0.1 ± 5.3 vs 3.4 ± 12.5; P = 0.59). Thirty-day complications (0.0% vs 3.3%, P = 0.43) and mid-term outcomes were also similar: T1E (16.7% vs 1.7%, P = 0.26), T2E with sac enlargement (55.6% vs 65.0%, P = 0.59). Reinterventions did not differ between groups (50.0% vs 30.0%, P = 0.16), with embolization (16.7% vs 26.7%, P = 0.39), and explant (5.6% vs 0%, P = 0.43) and T1E repair (16.7% vs 1.7%, P = 0.26). All-cause mortality was comparable (16.7% vs 26.7%, P = 0.32), and causes of death showed no clear differences, Supplemental Table V.
Associations with Outcomes after EVAR
Univariate and Multivariate Cox Regression Analyses for Mid-term Complications, Reintervention, and Mortality Outcomes
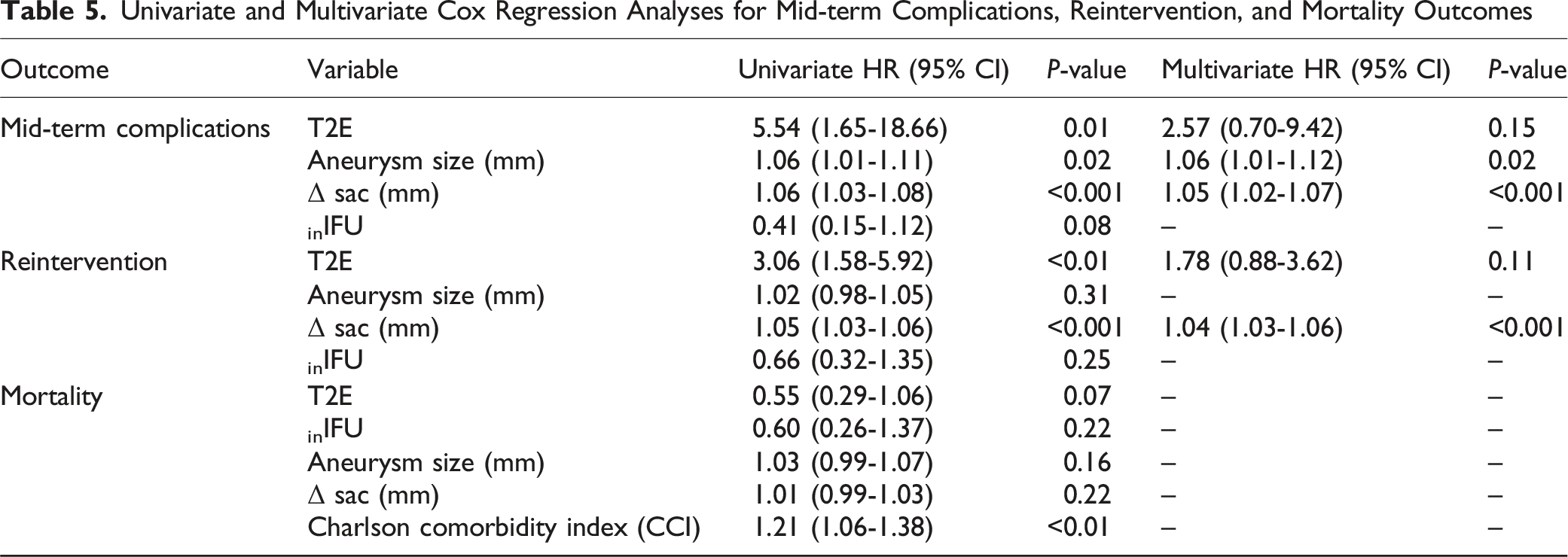
For reintervention, univariate analysis showed that T2E (HR: 3.06; 95% CI: 1.58-5.92; P < 0.01) and Δ sac (HR: 1.05; 95% CI: 1.03-1.06; P < 0.001) were significantly associated with reinterventions. In multivariate analysis, only Δ sac (HR: 1.04; 95% CI: 1.03-1.06; P < 0.001) remained significant. Regarding mortality, only Charlson comorbidity index (CCI) was associated with increased risk for reintervention (HR: 1.21; 95% CI: 1.06-1.38; P < 0.01), Table 5.
After excluding patients with concomitant T1E, univariate Cox analysis demonstrated that the presence of T2E (HR: 3.48; 95% CI: 1.18-10.30; P = 0.02), and the Δ sac (HR: 1.04; 95% CI: 1.02-1.07; P < 0.001) were significantly associated with mid-term graft-related complications. However, on multivariate analysis, only the Δ sac remained independently associated with complications (HR: 1.03; 95% CI: 1.01-1.06; P = 0.008). On univariate analysis, Δ sac was significantly associated with risk for reinterventions (HR: 1.04; 95% CI: 1.02-1.06; P < 0.001) and CCI was significantly associated with mortality (HR: 1.30; 95% CI: 1.13-1.49; P = 0.003), Supplemental Table III.
Kaplan-Meier analysis demonstrated that T2E (+) patients had a significantly higher incidence of mid-term graft-related complications (P < 0.01, Figure 2A) and reinterventions (P = 0.001, Figure 2B) compared to those T2E (−). No statistically significant difference in overall survival was observed between the 2 groups (P = 0.06, Figure 2C). (A) Kaplan-Meier Analysis of Mid-Term Graft-Related Complications Comparing T2E (−) and T2E (+) Patients. (B) Kaplan-Meier Analysis of Reintervention-Free Survival Comparing T2E (−) and T2E (+) Patients. (C) Kaplan-Meier Analysis of Overall Survival Comparing T2E (−) and T2E (+) Patients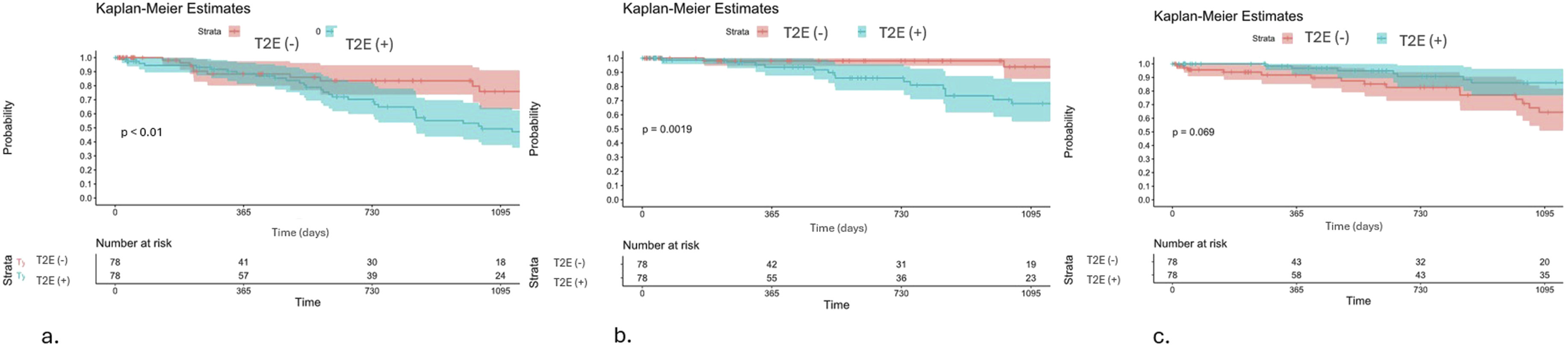
Discussion
T2E prevalence has been reported between 16-50%, with approximately 80-90% resolving spontaneously within the first 6 months after EVAR.8,9 Aneurysm sac growth is the primary parameter for assessing the presence and impact of T2E 10 since retrograde flow can significantly contribute to sac enlargement. 11 In our cohort, we found a rate of 37.6% of T2E on follow-up, with these being diagnosed on a median of 0.7 ± 0.9 years, the higher T2E rate likely reflects our surveillance pattern and the lack of routine pre-operative branch embolization.
The threshold for treatment varies among societies: the Society of Vascular Surgery (SVS) recommends embolization for T2E for more than 5 mm of sac expansion, 6 while the European Society for Vascular Surgery (ESVS) relies on intervention in more than 10 mm.12,13 In our institution, 63% of T2E patients had sac enlargement, but only 24.7% had more than 5 mm growth. In a Japanese study by Seike et al, a 27.4% rate of sac expansion was reported at 4.6 years, 14 while a second study by El Batti et al 15 reported a 40.3% rate of sac expansion at 2 years.
Given the generally benign natural history of T2E, some authors advocate for non-interventional management. 16 A systematic review from 2013 reported a probability of rupture due to T2E of less than 1%. However, a third of the patients whose aneurysm ruptured did not have evidence of sac growth. 17 This phenomenon, known as endotension, can be due to unidentified endoleaks or pressure transmission through intraluminal thrombus. 18
Type 2 Endoleak Outcomes
In our cohort, mid-term graft-related complications and reintervention rate were significantly higher in the T2E (+) group, with a mean sac enlargement of 1.79 ± 12.51 mm. Cox regression analysis confirmed that Δ sac was the only consistent and independent predictor of both mid-term graft-related complications and reinterventions, even after excluding patients with concomitant T1E. Notably, 73% of reinterventions in the T2E (+) patients were embolizations, consistent with the Endurant stent graft natural selection global post-market registry (ENGAGE), where patients with T2E had a significantly higher incidence of aneurysm growth and reinterventions than non-T2E patients (15.4 vs 7.5% at 5 years, P-value <0.001). 16 Despite higher reintervention rates, no significant difference in survival was observed between T2E (+) and T2E (−) patients, consistent with previous studies that emphasize the benign nature of T2E. 19
Our findings suggest that while T2E is associated with sac growth and a higher reintervention rate, this does not translate into worse survival. The majority of reinterventions targeted the endoleak itself without improving outcomes, as the risk of rupture was zero, and survival was unaffected by T2E status. Cox regression demonstrated that Δ sac was the most consistent and independent predictor of both mid-term graft-related complications and reinterventions. These results suggest that routine intervention for T2E may not be justified. Instead, treatment decisions should be individualized, taking into account access to follow-up care, the presence of T1E or type 3 endoleaks, life expectancy, and patient preference. 20
Instructions for Use Compliance and Outcomes
Adherence to IFU anatomical criteria and patient selection can influence sac growth. 21 In our cohort, the main reasons for being outIFU were larger neck angulation and neck diameter, both well-established predictors of AAA sac enlargement. 22 We did not find a significant difference in Δ sac or embolization rates between the outIFU and inIFU groups, likely due to a small sample size. However, the reintervention rate was higher in the outIFU group. Notably, a hostile neck is a well-recognized risk factor for higher reintervention rates due to sac enlargement and a predictor of mortality, mainly due to a poor proximal endograft seal.23,24
Sac enlargement of T2E has more frequently been associated with occult T1E.25,26 In the context of multiple endoleaks, we cannot attribute the sac expansion and rupture to one of them. However, T1E has been a well-recognized risk factor for these complications, 26 with larger neck angulation being consistently associated with T1E in both univariate and multivariate analysis. 27 In our cohort, all patients requiring T1E repair also had concurrent T2E, 3 out of 4 were intervened outIFU, with 3 ultimately requiring an explant. In addition, when we excluded patients with T1E, outcomes remained consistent, reinforcing that sac enlargement, reintervention, and complication rates were driven by T2E.
We observed significantly higher mortality exclusively in patients with T2E in the outIFU group compared to the inIFU group. A 2020 meta-analysis reported greater overall mortality for patients where IFU was not followed (HR, 1.20; 95% CI, 1.02-1.42; P < .03). 27 However, the literature remains divided, with Beckerman et al 28 reporting similar survival rates between outIFU vs inIFU groups, while O’Donnell et al 29 reported lower survival rates outIFU when the main criteria to be outIFU was hostile neck anatomy. Importantly, in our cohort, among patients without T2E, mortality did not significantly differ between those treated outIFU vs inIFU (P = 0.08), suggesting that the increased mortality may be specific to T2E patients with hostile anatomy. The elevated mortality in patients with hostile anatomy may reflect procedural complexity, with longer anesthesia times and an increased need for secondary interventions, 30 making them poor candidates for open repair. In addition, in our cohort, patients with T2E outIFU had longer hospitalization stays and higher reintervention rates than those inIFU group. Although the increased mortality is not directly related to the aorta, adherence to IFU criteria is required for the medical device’s safety, quality, and performance. 27
Limitations
The limitations of this study are primarily due to its retrospective nature. In addition, the follow-up had a mean of 2.7 ± 2.4 years, with a maximum of 10 years, not fully capture late outcomes and may be underpowered to detect mortality effects related to sac behavior. The relatively low annual procedural volume could also introduce variability in technique, device selection, and operator experience across the study period. Furthermore, this is a single-institution study, whose conclusion may not be generalized to an entire population of EVAR patients. In addition, even after matching and adjustment, residual confounding by indication is likely. Patients treated outIFU often have more hostile anatomy and higher operative risk or contraindications to open repair, factors that may not be fully captured by measures covariates. Notably, about 40% of off-IFU cases were marginally outside IFU which may limit the generalizability of the ‘off-IFU’ effect. Also, because T1E can make T2E branches function as outflow, misclassification is possible; therefore, we emphasize the subgroup analysis that excluded all T1E cases. Despite these limitations, this is one of the few studies that addresses complications and mortality in patients with T2E whose EVAR did not follow IFU criteria.
Conclusion
Our study found a 37.6% prevalence of T2E, with a median diagnosis of 0.6 years (range: 0.1-2.2) post-EVAR. While T2E is linked to sac growth and increased risk for reinterventions, it does not impact mortality. Higher reintervention rates did not improve outcomes, supporting a less invasive management approach. T2E management should be personalized, considering life expectancy, other concurrent endoleaks, financial burden, and patient preference. Subgroup analysis demonstrated that patients with T2E repaired outIFU had longer hospitalizations, required more reinterventions, and had a higher all-cause mortality, though aneurysmal-related mortality remained unaffected. T2E patients treated outIFU could benefit from a more individualized follow-up.
Supplemental Material
Supplemental Material - Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use
Supplemental Material for Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use by Camila Esquetini-Vernon, Houssam Farres, Camilo Polania-Sandoval, Yetzali Claudio-Medina, Hennessy Morales-Arroyo, Charles Ritchie, Christopher Jacobs, Ricardo Paz-Fumagalli, Beau Toskich, Jonathan Vandenberg, Biraaj Mahajan, Young Erben in Vascular and Endovascular Surgery
Supplemental Material
Supplemental Material - Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use
Supplemental Material for Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use by Camila Esquetini-Vernon, Houssam Farres, Camilo Polania-Sandoval, Yetzali Claudio-Medina, Hennessy Morales-Arroyo, Charles Ritchie, Christopher Jacobs, Ricardo Paz-Fumagalli, Beau Toskich, Jonathan Vandenberg, Biraaj Mahajan, Young Erben in Vascular and Endovascular Surgery
Supplemental Material
Supplemental Material - Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use
Supplemental Material for Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use by Camila Esquetini-Vernon, Houssam Farres, Camilo Polania-Sandoval, Yetzali Claudio-Medina, Hennessy Morales-Arroyo, Charles Ritchie, Christopher Jacobs, Ricardo Paz-Fumagalli, Beau Toskich, Jonathan Vandenberg, Biraaj Mahajan, Young Erben in Vascular and Endovascular Surgery
Supplemental Material
Supplemental Material - Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use
Supplemental Material for Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use by Camila Esquetini-Vernon, Houssam Farres, Camilo Polania-Sandoval, Yetzali Claudio-Medina, Hennessy Morales-Arroyo, Charles Ritchie, Christopher Jacobs, Ricardo Paz-Fumagalli, Beau Toskich, Jonathan Vandenberg, Biraaj Mahajan, Young Erben in Vascular and Endovascular Surgery
Supplemental Material
Supplemental Material - Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use
Supplemental Material for Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use by Camila Esquetini-Vernon, Houssam Farres, Camilo Polania-Sandoval, Yetzali Claudio-Medina, Hennessy Morales-Arroyo, Charles Ritchie, Christopher Jacobs, Ricardo Paz-Fumagalli, Beau Toskich, Jonathan Vandenberg, Biraaj Mahajan, Young Erben in Vascular and Endovascular Surgery
Supplemental Material
Supplemental Material - Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use
Supplemental Material for Higher Risk for Morbidity and Non-Aortic Related Mortality in Type 2 Endoleak Patients Treated Outside of Instructions for Use by Camila Esquetini-Vernon, Houssam Farres, Camilo Polania-Sandoval, Yetzali Claudio-Medina, Hennessy Morales-Arroyo, Charles Ritchie, Christopher Jacobs, Ricardo Paz-Fumagalli, Beau Toskich, Jonathan Vandenberg, Biraaj Mahajan, Young Erben in Vascular and Endovascular Surgery
Footnotes
Ethical Considerations
This retrospective study was reviewed by the Mayo Clinic Institutional Review Board – Florida Campus (IRB# 24-004735) and was determined to be exempt under 45 CFR 46.104(d), Category 4(iii) on May 8th, 2024. The reviewer approved a waiver of HIPAA authorization in accordance with applicable regulations, and informed consent was not required as all data were de-identified.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.