
Abstract
Introduction
Heparin-induced thrombocytopenia (HIT) is an acquired prothrombotic state from anti-heparin platelet-factor 4 (PF4) antibodies inducing the immune-mediated activation of platelets. 1 HIT occurs in 0.5-5.0% of patients exposed to unfractionated heparin. Risk factors include the post-operative setting, treatment duration longer than 4 days, prior heparin exposure, and use of unfractionated heparin (UFH) more so than low-molecular weight heparin (LMWH). 2 HIT should be suspected in patients with unexplained thrombus or 30-50% decrease in platelet count 5-10 days after initial heparin exposure. 3 However, HIT less commonly presents within 24 hours of heparin administration and up to 3 weeks after discontinuation. Clinical suspicion is important given 25% of patients will generate HIT-induced thrombus more than a day before laboratory evidence of thrombocytopenia. 4
Laboratory testing commonly includes screening with anti-PF4 immunoassay and confirmatory serotonin release functional assay (SRA). 5 Immunoassays, such as Enzyme-Linked Immunosorbent Assays (ELISA), afford high sensitivity in the detection of anti-PF4-antibodies with sensitivity as high as 99% and robust negative predictive value. 6 However, specificity is suboptimal (30-70%) as immunoassays also detect clinically insignificant antibodies from asymptomatic seroconversion after heparin administration. Confirmatory testing with SRA detects the activation of donor platelets in the patient’s serum. With high specificity (89-100%), it is considered the gold standard for confirmation of HIT. 7 At our institution, in 2024, an anti-PF4 assay costs approximately $218 and results within 1-4 hours. Confirmatory SRA costs approximately $265 and results within 5 days.
Given the strong negative predictive value of anti-PF4 immunoassays, it is exceptionally rare for patients to develop HIT with a negative result. In our literature search, we found reports of clinical HIT with negative anti-PF4 and SRA. However, we did not find any report of negative anti-PF4 with positive SRA.
Case Report
A 74-year-old male presented as a transfer from an outside hospital for evaluation of coronary artery disease (CAD) and ventricular tachycardia (VT). His history includes prior CABG (heparin exposure) complicated by free wall rupture status-post myomectomy, systolic heart failure (EF 35%), cardiac resynchronization therapy, atrial fibrillation, diabetes, emphysema, hemochromatosis, and active smoking. The morning of his admission to the outside hospital, his implantable cardiac defibrillator (ICD) fired twice, prompting him to contact emergency medical services. The ICD continued to fire an additional 5 times before he was started on amiodarone and lidocaine, and the patient was transferred to another facility with percutaneous coronary intervention (PCI) capabilities. Cardiac catheterization demonstrated high-risk multivessel stenosis prompting transfer to our quaternary medical center 7 days later for a higher level of care. He arrived having already been placed on a heparin drip.
On hospital day 10 at our facility, he suddenly lost sensation and pulses in the left lower extremity (LLE) (Figure 1). He had no prior history of claudication, rest pain, or lower extremity wounds and had palpable pedal pulses on admission. He was insensate with intact motor function constituting Rutherford IIa acute limb ischemia in the left lower extremity. His vascular exam demonstrated a right femoral pulse, biphasic left femoral signal, and absent signals distally. Labs were remarkable for therapeutic PTT of 62 seconds and platelet count of 89K from 134K the day prior, down trending from 236K on admission. CT angiography showed filling defects in the left common iliac and occlusion of the left external iliac artery with reconstitution of the superficial femoral and popliteal artery with poor contrast opacification distally. There was mild to moderate calcific and atherosclerotic burden in the infrarenal aorta, common iliac arteries, and common femoral arteries. The right common femoral artery was occluded with a diminutive profunda and no contrast distally. He was asymptomatic in the right lower extremity. He remained on heparin and was taken to the OR for revascularization of his acute limbs. Timeline of Hospitalization Including Anticoagulation Status, Platelet Count, and Pertinent Events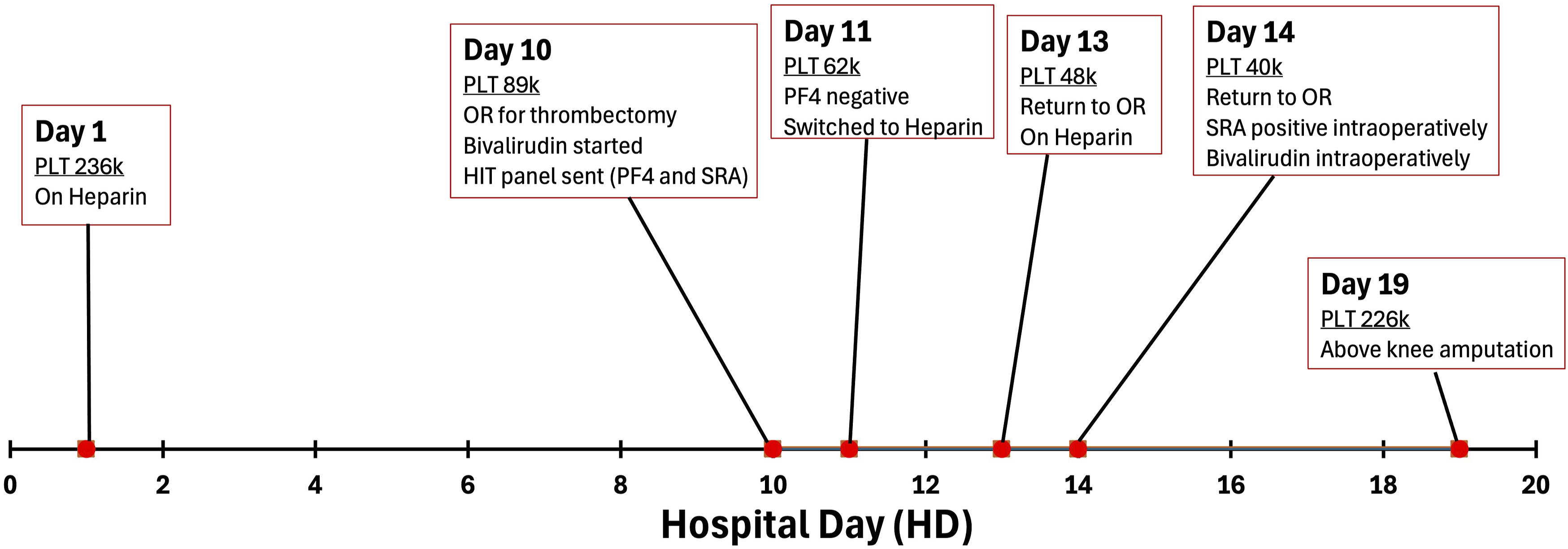
He underwent bilateral open femoral artery thrombectomies and left iliac artery bare metal stenting with return of multiphasic pedal signals at the case’s conclusion. The thrombectomy returned white thrombus suspicious for HIT in the setting of down trending platelets. The patient transitioned from heparin to bivalirudin postoperatively and anti-PF4 immunoassay with SRA was obtained.
The next morning, on hospital day 11, about 18 hours after bivalirudin initiation, the anti-PF4 assay returned negative, and the patient was transitioned back to heparin at the vascular medicine service’s recommendation. The platelet count at that time was 68K from nadir of 62K.
Two days later, on hospital day 13, the patient again had loss of sensation and left popliteal and tibial signals absent. His platelet count was 48K at the time. He was taken back to the OR and underwent left lower extremity thrombectomy from a below-knee incision, left superficial femoral artery antegrade bare metal stenting, and focal left femoral endarterectomy, with return of signals.
On hospital day 14, 22 hours after leaving the OR, the patient again had loss of signals prompting return to the OR. He underwent bilateral groin re-exploration, bilateral aortoiliac thrombectomy and bare metal stenting, left lower extremity thrombectomy, and left common femoral to below-knee popliteal artery bypass with ringed PTFE. Two hours into the case, the SRA obtained 3 days prior resulted positive for HIT and the patient was again transitioned from heparin to bivalirudin intraoperatively. Completion angiogram demonstrated thrombus that already started to line the PTFE bypass graft that was retrieved with balloon thrombectomy. The patient had a posterior tibial artery signal at the conclusion of the case.
The patient remained hypercoagulable despite bivalirudin and lost signals shortly after returning to the ICU. He then demarcated and was taken for a left above knee amputation 9 days after his index operation. Repeat PF4 and SRA were obtained and resulted negative four days after the initial SRA positive test result. Pathology ultimately resulted as acute thrombus rich with fibrin and platelets. The patient was managed as clinical HIT and discharged on Warfarin 49 days after admission.
Discussion
A 74-year-old male underwent multiple operations for acute left lower extremity ischemia in setting of suspected hypercoagulable state with negative PF4 and subsequently positive SRA suggestive of HIT. Given the historically robust negative predictive value of the PF4 immunoassay, the patient was maintained on heparin throughout his revascularization attempts leading to recurrent thrombosis. Based on known atherosclerotic disease, he was clinically treated as acute on chronic ischemia.
Our literature search yielded few examples of patients that had clinical HIT despite initial negative laboratory evaluation.8,9 However, in these examples, repeat testing turned positive, making it plausible that the initial negative results were explained by low levels of antibodies early in the disease course. In our case, the patient had been on heparin at least 10 days prior to initial anti-PF4 and continued to remain negative on repeat testing. We were not able to find any documented examples of patients with clinical HIT who remained negative on repeat PF4.
Prior heparin exposure is a risk factor for the development of HIT. Our patient was exposed to heparin during CABG 28 years prior. It is unlikely that this exposure would contribute to HIT as it was older than 100 days. 10 However, it is unclear if he had a more recent exposure to heparin that could have primed his immune response.
The patient was converted back to heparin from bivalirudin shortly after anti-PF4 turned negative. Although this is an exceptionally rare occurrence, it may be appropriate to remain off heparin until clear resolution of clinical HIT. Moreso in instances where there is not a clear alternate explanation for the clinical picture. While our patient had a history of atrial fibrillation and atherosclerosis of the lower extremities, this would not likely explain his short-term recurrent bilateral limb ischemia while inpatient.
Conclusion
Here we present a 74-year-old male that had clinical HIT with a false negative anti-PF4 and subsequently positive SRA. Delay in cessation of heparin may have led to recurrent thrombosis with a poor outcome. We re-emphasize the importance of clinical presentation and suspicion in management of patients with suspected HIT.
Footnotes
Author Note
This report was presented as a poster at the 2024 Midwest Vascular Surgery Society Annual Meeting, Chicago, September 12-14, 2024.
Consent for Publication
Informed consent was obtained for the publication and presentation of this case report and associated images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.