
Abstract
Background
Few single center studies with small sample size have been published showing clinical benefits of endovascular intervention specifically using mechanical suction thrombectomy for P.E. without systemic/catheter lytic therapy. This study will analyze our initial experience and clinical outcomes in the treatment of P.E. using Inari FlowTriever thrombectomy device.
Patient Population/Methods
A single center retrospective study of 50 consecutive patients with acute P.E. were treated with the INARI FlowTriever device between January 2019 to June 2023. All patients were submassive P.E. with right ventricular strain (RV/LV ratio >0.9) and requiring oxygen therapy or having increase in oxygen therapy from baseline. Procedural and clinical success (Improvement in intraoperative pulmonary artery pressures and oxygen therapy) were evaluated along with in hospital procedural related complications with a mean follow up of 8 months (range 1-22.5 months).
Results
All patients were stratified as intermediate high-risk PE with a mean age of 68 years. Right ventricular dilation was present in 100% of patients with a mean RV/LV ratio of 1.55 (range 0.9-2.7). Mean pre-op Troponin was 434 (median 318, range 6-2332) and mean BNP was 352 (median 154, range 60-1787). Procedural success as defined by SIR guidelines was achieved in 100% of patients. There was 0% hospital mortality, device related mortality, or complications including bleeding, and acute kidney injury (AKI). Significant improvement in FiO2 was noted when comparing the mean pre-procedural FiO2 of 40.6% (range of 21%-100%) to a mean of FiO2 of 28.3% (range of 21%-52%) at 24 h post procedure (P < .0001). Proportion of patients on room air increased from 0% pre procedure to 94% at 48 h. The mean pre-op pulmonary artery pressure improved from 47 mm Hg (range 20-74) to mean post pulmonary artery pressure of 34 mm Hg (range 19-65) P < .0001. 97% of patients had a decrease in their pre-op pulmonary pressures intraoperatively.
In late follow-up when evaluating pre to post intervention 36/38 (94.4%) of our patients were back to baseline with regards to oxygen requirement. Proportion of patients on room air increased from 0% pre procedure to 94.4% post procedure. 34/38 (89%) of patients reported they were back to baseline in regard to physical activity and 37/38 (97%) of patients reported their breathing status was back to baseline from prior to procedure. Using the modified Medical Research Council Dyspnea Score, 93% of patients reported a pre-op score of four (highest) while 70% reported scores of zero (normal) and or score of one post intervention with 100% showing improvement at 8 month follow up.
Conclusion
Our study demonstrates both safety and effectiveness in using the INARI FlowTriever for patients with submassive acute pulmonary embolism.
Introduction
Pulmonary Embolism is a leading cause of cardiovascular mortality with over hundreds of thousands of deaths per year. 10-30% of these patients will die within three months of diagnosis.1-3
Few single center studies have been published showing clinical benefits of endovascular intervention for pulmonary embolism specifically mechanical suction thrombectomy without systemic and or catheter lytic therapy. The largest multi-center prospective study to date remains the FlowTriever All- Comer Registry for Patient Safety and Hemodynamics (FLASH) registry of 800 patients (Industry Sponsored). The interim analysis of the first 250 patients were predominantly intermediate risk (93%) and showed very low major adverse events (1.2%), all of which were major bleeds that resolved. All-cause mortality was 0.4% at 30 days and average reduction in mean pulmonary artery pressure was 7.1 mm Hg. Patient symptoms and cardiac function improved as well. 4
The FlowTriever Pulmonary Embolectomy Clinical Study (FLARE) comprised of 106 patients at 18 institutions with acute intermediate risk PE with RV/LV ratio >0.9 had FlowTriever thrombectomy and showed improvement in RV/LV ratio with minimal ICU stay/major bleeding. 5
The chest Guidelines recommends catheter directed therapy and or systemic lysis for PE patient with signs of hemodynamic or respiratory deterioration, however it is a weak recommendation, 6 meanwhile the Pulmonary Embolism Response Team (PERT) Consortium recommends the use of catheter directed lytic therapy for intermediate high risk PE patients with relative contraindication to thrombolytics and use of catheter directed thrombectomy in patients with absolute contraindication to thrombolytics and or failed thrombolytic therapy. 7
Our present study will analyze the clinical outcomes of patients at a single center (not industry sponsored) presenting with intermediate risk PE, with RV/LV ratio >0.9 and respiratory deterioration using mechanical suction thrombectomy.
Patient Population and Methods
Study Design and Patient Population
50 Patients with intermediate Risk PE with elevated RV/LV ratio and respiratory deterioration were consented to mechanical suction thrombectomy using the INARI FlowTreiver device. All procedures were performed at Charleston Area Medical Center (CAMC) in Charleston, WV between January 2019 to May 2023. The study was approved by the Institutional Review Board of CAMC/West Virginia University, Charleston Division. Inclusion criteria required informed consent of patients deemed appropriate candidates for PE thrombectomy. In assessing candidacy all patients underwent CTA Chest PE protocol to determine extent of main pulmonary artery thrombus and RV/LV ratio to be greater than 0.9. Patients had to be requiring oxygen therapy and or increase in oxygen therapy from baseline before admission.
Patient demographics and clinical characteristics/comorbidities where recorded. These included: coronary artery disease, diabetes Mellitus, congestive heart failure, chronic kidney disease, history of stroke, cancer, active or history of COVID 19, hypercoagulable disorders, history of deep venous thromboembolism, concomitant deep venous thromboembolism, and recent surgery/trauma.
The highest troponin, BNP, and pulmonary artery systolic pressure were measured before and after intervention. Date/time of transfer from ICU to lower level of care, baseline home FiO2, Max FiO2 pre and post procedure and discharge FiO2 requirements were also evaluated in all patients during their hospital stay.
Exclusion criteria included patients with previous history of venous thrombectomy, patients with a IVC filter, patients who received any prior thrombolytic therapy within 30 days, patients with contraindication to anticoagulant therapy, patients who were deemed too high risk medically and or unstable to be placed in a angiography suite. This was defined as anyone with pressor requirements, systolic blood pressure under 90 mmHg and heart rate above 120 beats/min.
Procedures were considered successful once no more clots were retrieved from the thrombectomy catheter and a completion angiogram showed no residual clot.
Perioperative Protocol
All patients underwent systemic heparin protocol with ACT checks once diagnosed with acute pulmonary embolism. Once planned and consented, all interventions were done under local with moderate sedation. Inari thrombectomy device was used for all patients without previous systemic and or local lytic catheter therapy. All patients had dual ProGlide placement at the start of the procedure. Postoperative surveillance included clinical and pulmonary evaluation while in the hospital with eventual clinical office follow-ups.
Outcome Measures and Statistical Methods
Primary outcome measures included oxygen saturation and oxygen therapy pre and post procedure, intraoperative pulmonary artery pressure pre and post procedure, and In-Hospital Mortality. Secondary outcomes included bleeding, which was classified as mild vs major (major defined by bleeding at a critical site), intracranial bleed, other central nervous system hemorrhage, pericardial tamponade, extremity bleed, hemothorax, abdominal, retroperitoneal bleed, hemodynamic instability, overt bleeding with hemoglobin drop equal to or greater than 2 g/dL or administration of equal to or greater than two units of blood), 8 reintervention, and acute kidney injury.
All patients underwent a clinical questionnaire in office and or through telecommunication by phone. The questions included: When evaluating pre to post intervention of pulmonary artery thrombectomy were patients back to baseline with regards to oxygen therapy, physical activity and breathing status. Patients were also graded using the Modified Research Dyspnea Scale pre to post intervention on a value from 0 to 4. Zero was graded for patients with dyspnea only with strenuous exercise, one was for patients with dyspnea hurrying or walking up a slight hill, two was for patients walking slower than people of the same age due to dyspnea or having to stop for breath when walking at own pace, three was having to stop for breath after walking 100 yards of after few minutes and four was being too dyspneic to leave the house or breathless when dressing. 9
Results
Demographics and Co-Morbid Conditions
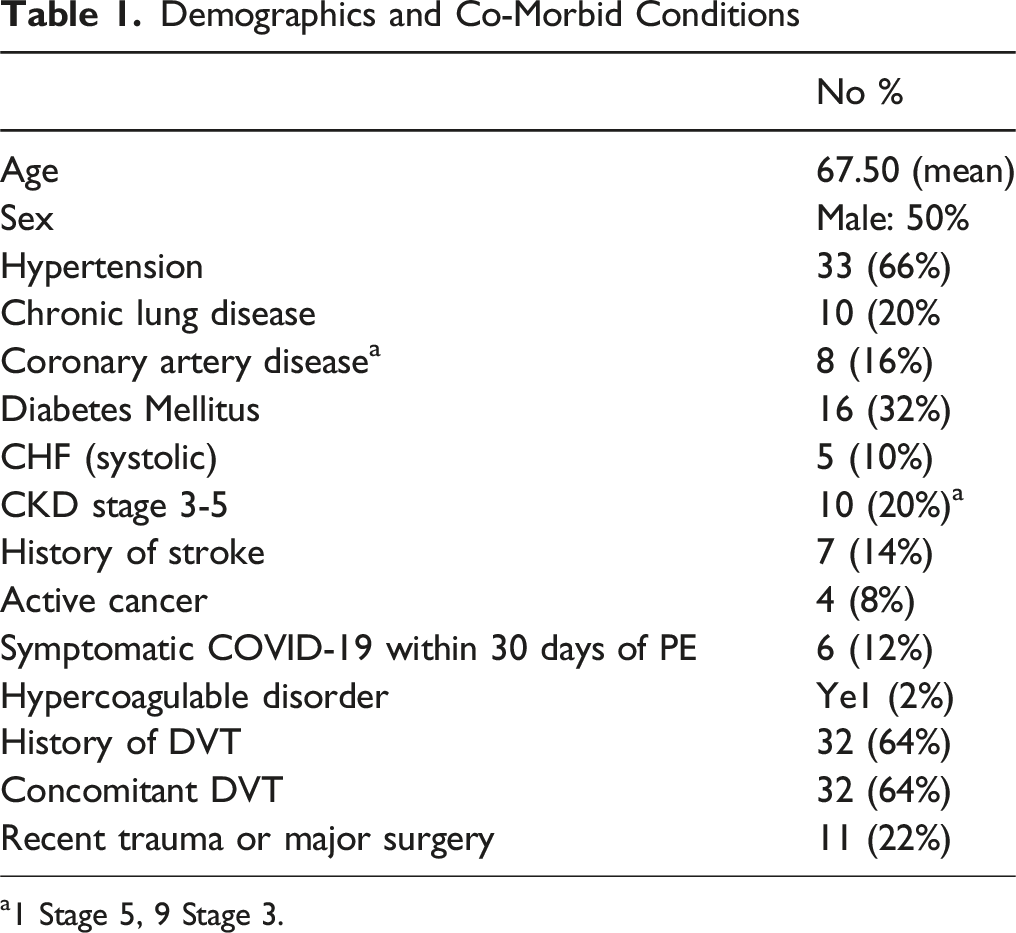
a1 Stage 5, 9 Stage 3.
48 of 50 patients (96%) had 1 or more troponin levels drawn. Max troponin levels were recorded if patients had more than one troponin result. Mean troponin 434, median 317.5 with a range of 6-2332. 48 of 50 patients (96%) had a BNP drawn. The Mean BNP was 352, median 153.5 with a range of 60-1787.
Hemodynamics: Pulmonary Artery Pressures, O2 Need
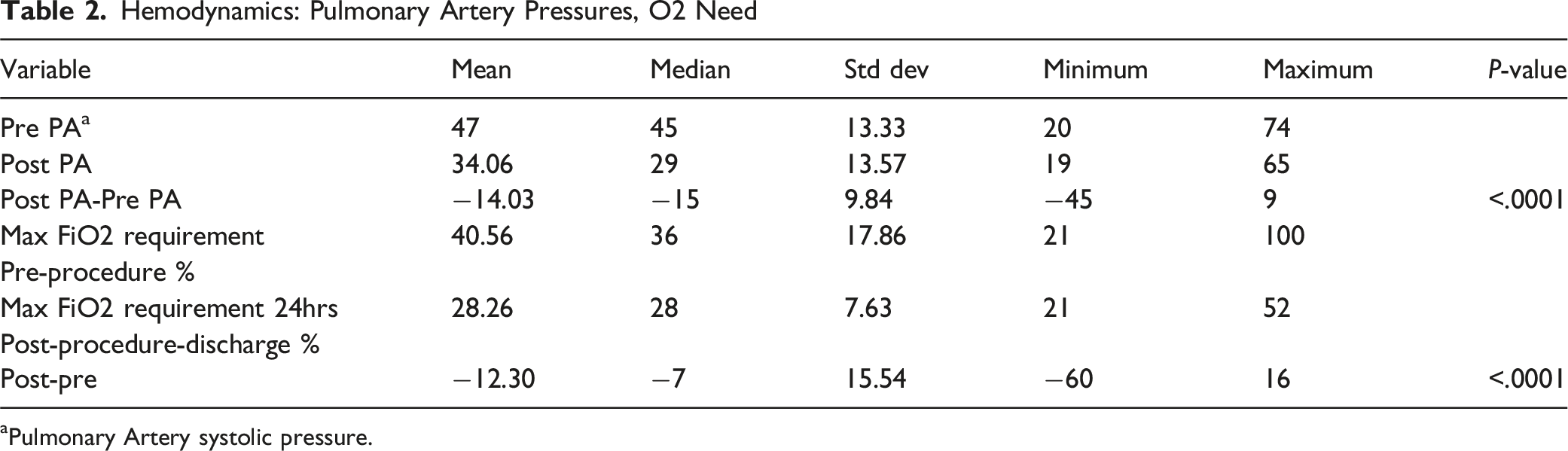
aPulmonary Artery systolic pressure.
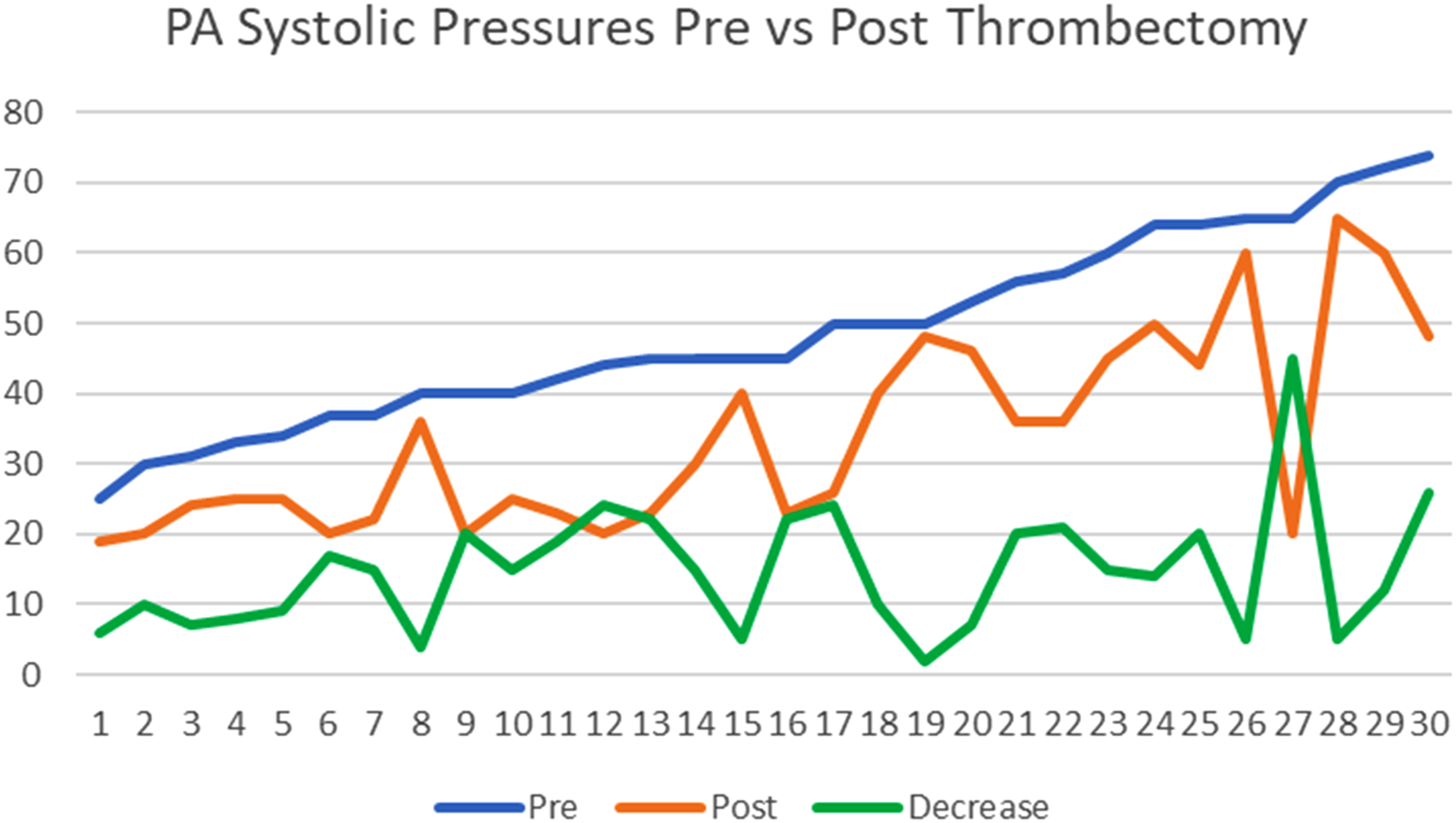
PA Systolic Pressures Pre vs Post Thrombectomy
Hemodynamic Parameters
6% of our patient population were on home oxygen at baseline. The max Fio2 pre procedure was 40.56%(mean) with a range of 21-100% while 24 h post procedure was 28.26% (mean) with a range of 21-52%. Only 6.5% of patients who were not on O2 at baseline went home on O2 at discharge.
Pre procedural intraoperative pulmonary artery systolic pressure (N = 36) showed a mean of 47.6 mm Hg with a range of 20-74. Post procedural intraoperative pulmonary artery systolic pressure (N = 33) showed a mean of 34.1 mm Hg with a range of 19-65. This showed a decrease in PA systolic pre vs post: 13.5 mm Hg. Of those patients with a Pre and Post procedural intraoperative pulmonary artery systolic measurement, 97% had a decrease in their pressures.
Both in-hospital all-cause mortality and procedural related mortality was 0%. There was no procedure related major bleeding or post-procedure acute kidney injury (AKI) (defined as 1.5 X baseline creatinine).
Modified Research Dyspnea Scale (MRDS)/Clinical Follow-Up
The mean preoperative MRDS scale was 3.85 with range 1-4 vs post mean scale of 1.92 with range 1-4. A total of 38/50 patients were able to be reached by phone or were evaluated in the clinic at a mean follow-up time of 249 days with a range of 22-674. When evaluating pre-to-post intervention 36/38 (94.4%) of our patients were back to baseline regarding oxygen therapy. Proportion of patients on room air increased from 0% pre procedure to 94.4% post procedure at 48 h. 2/38 (5.3%) were on a higher amount of oxygen than baseline prior to procedure. 34/38 (89%) of patients reported they were back to baseline regarding physical activity. 37/38 (97%) of patients reported their breathing status was back to baseline from prior to procedure. 1/38 (2.6%) breathing was worse compared to before the procedure.
Discussion
The progression and natural history of submassive PE continues to remain in question, with modern mortality rates remaining between 3 and 14.2%. 10 Long term morbidity remains poorly documented within the current body of literature. Post pulmonary embolism syndrome is far less well defined than post thrombotic syndrome. This is defined as chronic exertional dyspnea, exercise limitation, and reduced quality of life for longer than 3 months after effective anticoagulation for acute PE. Many patients may still have symptoms from their initial acute event. This nomenclature broadly encompasses multiple post embolic phenomenon, including chronic thromboembolic pulmonary hypertension (CTEPH) and chronic thromboembolic disease (CTED). Data on the prevalence of CTEPH in patients up to 4 years from experiencing a pulmonary embolism is 0.8-3.8%.11,12 Regardless of its known existence, post PE syndrome has very limited high-quality data, and most of the literature is focused on the lifestyle of the patient.
Our single center study analyzed the clinical outcome of intermediate PE patients using the INARI suction mechanical thrombectomy device. Our results were very favorable to the FLASH and FLARE trials. Major adverse events as defined by device related death, major bleeding, intraprocedural device or procedure related events occurred in none of our patients with no reinterventions needed. Major adverse events in FLASH by comparison was 1.2% compared to 3.8% for FLARE. No major bleeding events occurred in our study compared to 11 in FLASH and 1 in the FLARE. Neither our study nor the FLASH/FLARE studies had any cases of intracranial hemorrhage. Our study and FLASH had no access complications. FLARE had one access complication (0.4%). Mortality in our study was 0% at 30 days as compared to FLASH which reported 1.1% all-cause mortality but no device related death at 30 days. FLARE also had no device related deaths. These studies had low mortality in comparison to meta-analysis of catheter directed lysis studies for intermediate PE. 13
When evaluating pulmonary artery pressures from prior to post intervention 62% of our patients that were documented had a mean of 13.5 mm Hg reduction post operatively. FLASH in comparison had a pulmonary artery pressure drop by a mean of 7.6 mm Hg. The effects of consistently elevated pulmonary artery pressures have well described physiological alterations to pulmonary and right ventricular flow. With high pressure, highly pulsatile pulmonary arterial flow demonstrates significant decrease in nitric oxide synthase and increased expression of endothelin and angiotensin- converting enzyme in animal models, each of which contribute to development of a distal proliferative vasculopathy. This vasculopathy ultimately leads to irreversible pulmonary arterial branch changes and right ventricular hypertrophy. Therapy to acutely reduce these effects have been theorized to increase pulmonary arterial compliance and might prevent critical remodeling which leads to pulmonary hypertension. 12
When evaluating pre-to-post intervention 94.4% of our patients were back to baseline regarding oxygen therapy-Proportion of patients on room air increased from 0% pre procedure to 94.4% at 48 h in contrast to FLASH which showed a 60% change. 89% of patients reported they were back to baseline regarding physical activity and 97% reported their breathing status was back to baseline from prior to procedure. Of 38/50(76%) patients who had MRDS, 93% reported a Modified Research Dyspnea Score of 4 with 100% showing improvement and 70% reporting scores of 0 and or 1 post intervention and at 8-month follow-up. 9
Few single center studies using the INARI thrombectomy device for mostly submassive PE patients have been published in the literature- Wible et al in 2019 published a study of 46 patients using the Inari thrombectomy device showed pulmonary artery pressure improvements from 33.9 to 27 mm Hg post procedure with 100% patient survival and over 70% reduction in oxygen requirements. They also reported two major bleeds (4.6%) which required blood transfusion and intubation for hemoptysis. 14
Pizano in 2022 published a study of 14 patients using the Inari thrombectomy device showing a significant reduction of pulmonary artery pressure from 60 to 40 mm Hg. Few patients in this study did require thrombolysis but there was no device related complication, bleeding event, MI or death. 15
Elmoghrabi published a single center study evaluating 38 patients using the Inari thrombectomy device for mostly submassive PE patients. Average pulmonary artery pressure from pre to post intervention was improved by 22%; two patients (5.26%) had significant adverse events- one had access complication requiring blood transfusion and another developed massive hemoptysis leading to cardiac arrest. Overall length of stay was 7 days with 79% survival at hospital discharge. 16 Markovitz published a small single center study using the Inari thrombectomy device for massive and submassive PE consisting of 13 patients showing 100% technical success with no major or minor adverse events, technical complications or death within 30 days. Mean pulmonary artery pressure decreased by 19% from 32.5 to 26.3 mm Hg post procedure. Oxygen saturation improved by 4% from 93.6 pre to 97.5% post intervention while heart rate decreased from 106 bpm to 84 bpm. 17
Our study, like many of the above demonstrates the safety and efficacy of the INARI suction mechanical thrombectomy device from a single center in a real-world PE population. All-cause mortality in our study was 0% and patients demonstrated a significant improvement in hemodynamic and clinical outcomes.
Limitations of our study included being a single center with possible bias of intervention when using the device due to no comparisons to other devices along with the technical comfort of the device to the interventionalists. There was subjective recall bias with regards to outpatient phone call questionnaire and understanding of questions as presented by the residents, and physicians to the patient population. Lastly, we did not have pulmonary pressure taken pre/post operatively in all patients- only 62% of total patients had this documented from interventionalists and 76% of patients were able to be reached by phone or seen in clinic for follow-up post intervention. Future investigation will continue at our institution with more patients being added to the study along with continued follow-up.
Conclusion
Our study demonstrates both the safety and effectiveness of percutaneous suction mechanical thrombectomy using the INARI FlowTriever for acute intermediate risk PE with the majority of patients having physiological and functional improvement following therapy and up to 8 months follow-up. Further study is needed to assess low and or high-risk PE patients along with comparisons to other catheter therapy modalities.
Footnotes
Author Note
Presented at the Society for Clinical Vascular Surgeons 51st Annual Symposium, Scottsdale, Arizona March 16-20, 2024.
Ethical Consideration
This study was approved by the CAMC Health Education Research Institute IRB#22-897.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.