
Abstract
Introduction
Extrinsic compression of celiac artery (CA) by median arcuate ligament (MAL) is quite common, and is usually asymptomatic. 1 Other arteries that arise from aorta near the diaphragmatic aortic hiatus, like right or left renal arteries (LRA/RRA) and superior mesenteric artery (SMA), may also be rarely compressed by MAL, either in isolation or in addition to CA compression. 2 Here we report a case of young man who presented with combined compression of CA and RRA by MAL and was successfully treated by surgical MAL release. Patient consent and institute ethics committee waiver was taken for this report.
Case Details
A 20-year-old man presented with moderate-to-severe post-prandial epigastric pain for the past 1 year, resulting in fear of food, self-imposed diet restriction and a 5 kg weight loss. He had no urinary complaints. On examination, he was thin built with a body mass index of 17.4 kg/m2, a blood pressure (BP) was 130/80, and a normal abdominal examination. His blood tests were unremarkable except for mildly raised serum creatinine of 1.06 mg/dL. After a normal abdominal ultrasonography and upper gastrointestinal endoscopy, he was evaluated with contrast-enhanced computed tomography (CT) with abdominal CT angiography (CTA) to find the cause for his troubling symptoms. CTA showed proximal CA compression by MAL with 60% narrowing, post-stenotic dilatation and a ‘hook’ sign in sagittal reconstruction. There was also compression of proximal RRA by MAL with 40% narrowing and small-sized yet functional right kidney (measuring 7.8 cm in length) (Figure 1). A renal scintigraphy to assess the right kidney function could not be done due to a long waitlist at our institute. A diagnosis of MALS was made. After multi-disciplinary team discussion, it was decided to do surgical MAL release at both sites. As the patient desired a minimally invasive surgery, a laparoscopic approach was planned. Pre-operative CT angiography. (A) Axial, (B) Coronal images depicting the compression of right renal artery origin from aorta by the median arcuate ligament red arrows). (C) Coronal image shows small right kidney (7.8 cm in length) with compensatory hypertrophy of left kidney (9.8 cm). (D) Sagittal image showing significant compression of celiac axis at origin by MAL with hook sign and post-stenotic dilatation (green arrow). (E) Coronal 3D Volume rendered image confirming multiple collaterals between celiac axis and SMA branches (blue arrows)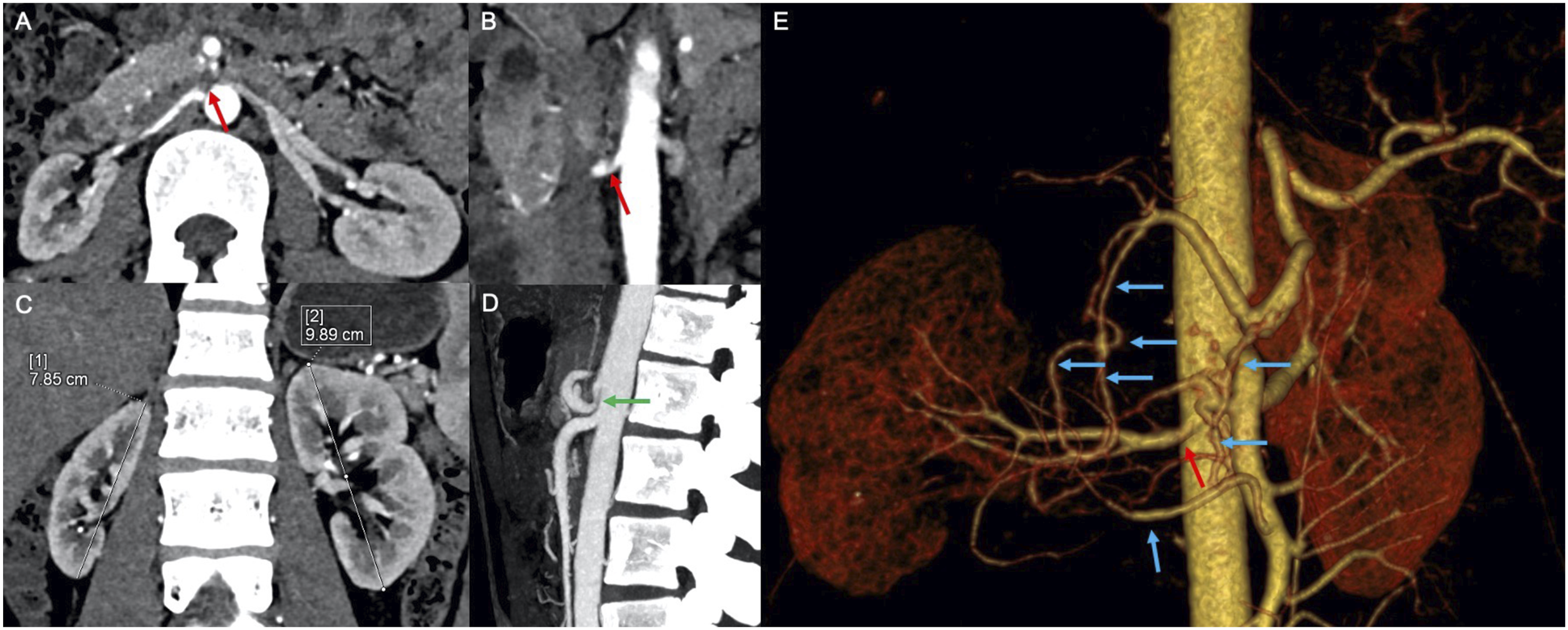
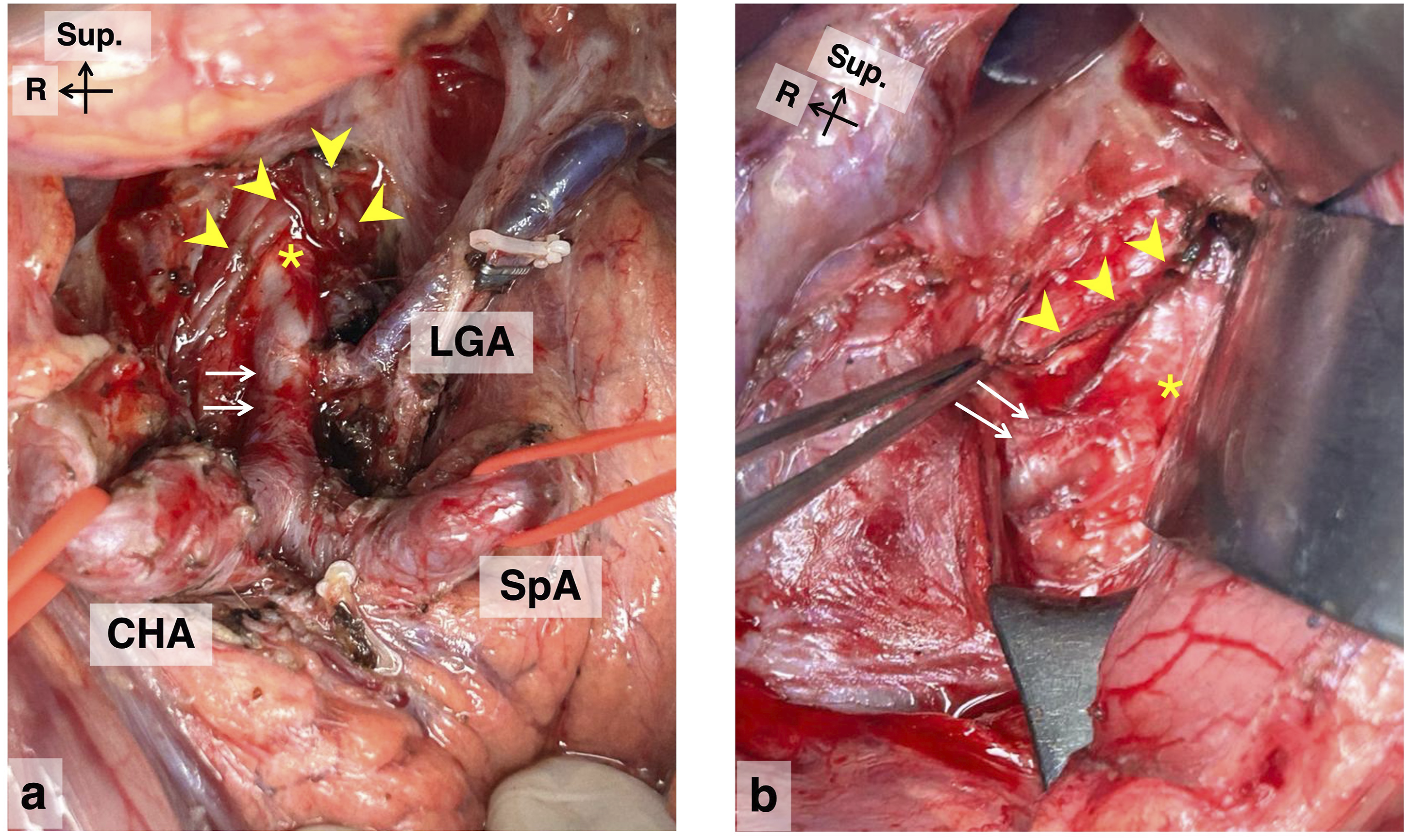
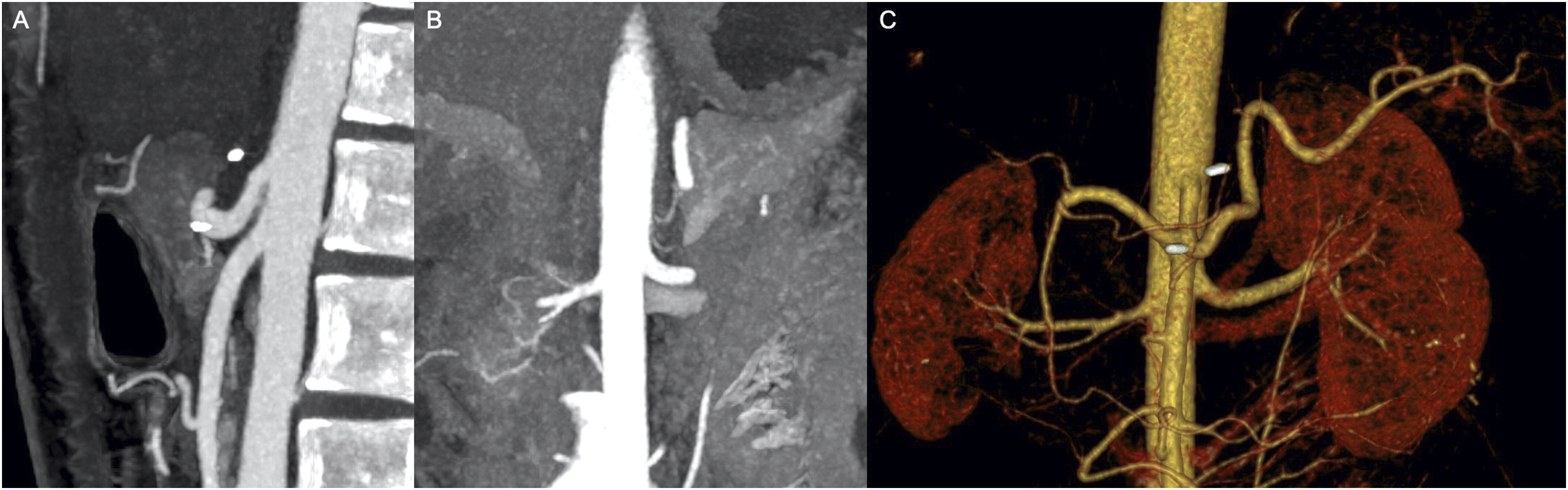
Under general anesthesia, with the patient in reverse Trendelenberg position and legs split, 4 ports were placed: one 12 mm supraumbilical camera port, two 5 mm bilateral subcostal working ports and a 5 mm left lumbar assistant port. The left gastric artery (LGA) was looped, the phrenoesophageal ligament incised and abdominal aorta was identified at its hiatus from where the crus fibres were cut in a ‘top to down’ approach to identify the CA origin (Figure 2). The station 8a lymph node was dissected out identifying the common hepatic artery (CHA) and its junction with the splenic artery (SpA) and LGA. The CA was looping behind the pancreatic neck going further caudally and we couldn’t visualise its origin from aorta in laparoscopy; hence the procedure was converted to open. CA origin was identified and overlying thick and tight fibrotic MAL of about 15 mm length was divided carefully resulting in visibly improved bounding pulsations in the CA. The duodenum was then kocherised, the RRA identified and traced proximally (Figure 3). The right limb of the thick fibrotic MAL and the right crus fibres were found compressing proximal RRA for about 10 mm, which were also carefully divided. The operative duration was 200 mins with 50 mL blood loss. Post-operatively, the patient had an uneventful recovery, tolerated a soft diet without post-prandial pain on day 2 and was discharged on the same day. At 12-month follow-up, he is asymptomatic, serum creatinine has become normal and has gained 8 kg weight. Follow-up CTA at 2 months showed a normal CA and RRA (Figure 4). Intraoperative photos - Laparoscopic phase (A) Looping of gastroesophageal junction and external retraction. (B) Looping of left gastric vessels. (C) Identification of abdominal aorta (yellow asterisk) at diaphragmatic hiatus. (D) Exposure of anterior surface of aorta in a ‘top down’ approach by dividing crus muscle. (E) Removal of neurolymphatic tissue to expose coeliac artery. (F) Celiac artery (white arrows) looping behind pancreas inferiorly and origin not visible in laparoscopy Intraoperative photos – Open phase (A) The celiac artery (white arrows) at its origin from aorta (asterisk) after median arcuate ligament release (yellow arrowheads). The branches of celiac artery are seen – common hepatic artery (CHA), splenic artery (SpA) and left gastric artery (LGA). (B) The right renal artery (white arrows) at its origin from aorta (asterisk) after release of overlying right crus and right limb of median arcuate ligament (yellow arrowheads). (Black arrows at left upper corner are for orientation of the image. Sup – superior, R – right side) Post-operative CT angiography after 2 months. (A) Sagittal image shows significantly increased caliber of Celiac axis at origin with metallic surgical clips nearby. (B) Coronal image depicts the released origin of right renal artery. (C) Coronal 3D volume rendered image confirming disappearance of collaterals between celiac axis and SMA branches
Discussion
The MAL is a fibrotic band that connects both the diaphragmatic crura and forms the inferior boundary of the aortic hiatus, usually at the upper level of L1 vertebra. 3 The CA usually originates at the T12-L1 junction while the renal arteries at the L1-L2 level. MAL can compress CA or renal arteries due to developmentally more cranial origin of these arteries (eg, at T12 level for CA and T12/upper L1 level for renal arteries) or a caudal location of MAL (eg, extension till L2). 4 MAL compressing CA is quite common, seen in 10-24% of general population incidentally, but is symptomatic in only a minority when it is called MALS. Its estimated incidence is 2 in 100,000 and usually presents between 30-50 years of age with 75-80% being females.3,5 Patients present typically with moderate to severe post-prandial upper abdominal pain which may last for 1- 4 hrs and leads to fear of food, reduction of food intake and unintentional weight loss. The two theories for MALS symptoms are: a. ‘Ischemia’ theory due to the inability of CA blood flow to increase for post-prandial metabolic demands; b. ‘Neurogenic’ theory due to irritation of celiac ganglion by the MAL, leading to pain and splanchnic vasoconstriction. MAL compressing renal arteries is very rare with only about 21 cases reported till date. 6 The usual clinical presentation is a young to middle aged patient having uncontrolled hypertension or a hypertensive emergency and evaluation showing unilateral or bilateral proximal renal artery narrowing by external compression. Our patient was a 20-year-old man, normotensive and symptomatic only with post-prandial abdominal angina.
MALS is a diagnosis of exclusion as the other causes of upper abdominal pain like gallstone disease, acid peptic disease, gastroesophageal reflux etc. are more prevalent. Current guidelines recommend a MALS diagnosis to be made based on the classical symptoms described above, CA compression by MAL on imaging and a multi-disciplinary discussion between gastroenterologists, surgeons and radiologists. 7 As doppler ultrasound is widely available and radiation-safe, it is usually the first investigation for suspected MALS and shows celiac trunk deflation along with peak systolic velocity >200 cm/sec in expiration. 3 CTA is the gold standard for confirming MALS and it shows proximal CA narrowing within 5 mm of its origin, post-stenotic dilatation, collateral arteries between SMA and CA (gastroduodenal, inferior pancreato-duodenal) and on sagittal images, a characteristic ‘hook’-like appearance. CTA in expiration phase may show the deflation angle of CA >45-50°. 3 CTA can also screen for and detect MAL compression of other upper abdominal arteries like RRA, LRA and SMA. In our patient, MAL compression of RRA was incidentally identified on CTA. Although his blood pressure was normal, his serum creatinine was mildly elevated with a small right kidney.
Surgical MAL release is the most effective treatment for symptomatic MALS, giving durable relief in >70% cases, and can be done by open, laparoscopy or robotic approaches. 5 Minimally invasive methods are preferred nowadays due to their magnified view, smaller surgical wound, less postoperative pain, better cosmesis and faster recovery. The MAL area can be exposed either by an antegrade ‘top to down’ approach by dividing crus fibres and exposing anterior surface of aorta at its hiatus or a retrograde ‘bottom to top’ approach by proximally tracing the CA from the confluence of CHA, SpA and LGA or a combination of both approaches. The hallmark of MAL is the thick fibrous tissue just abutting CA which is very difficult to lift up by the surgical instrument, despite significant effort by the surgeon (the so called ‘lift’ test). This is then carefully divided while protecting the major vessels nearby. The inferior phrenic arteries can originate from aorta or CA very close to MAL and if injured, can lead to significant bleeding. Though compressed, the CA and renal arteries are not diseased in MALS, unlike in atherosclerosis (calcified arteries) or in autoimmune disorders and hence vascular reconstruction is rarely needed except in chronic cases.5,6 Primary endovascular treatment is contra-indicated as the stent may not fully expand or may fracture and migrate distally. In our case, after MAL release, both the CA and RRA were normal with bounding pulsations. Conversion to open from minimally invasive approach is reported in 0- 9% cases with the commonest cause being bleeding.1,8 In our case, due to the caudal position of CA origin behind the pancreatic neck, we could not visualise it for its safe division and hence converted to open.
In conclusion, we report a rare case of 20-year-old man with symptomatic MAL compression of CA and co-incidental RRA compression, both of which were successfully released surgically. CTA is the diagnostic modality of choice for MALS. The learning point from this case is that one should carefully inspect the other upper abdominal arteries for MAL-related compression as they may be asymptomatic, and this enables simultaneous treatment at these sites in a single surgery.
Footnotes
Ethical Considerations
Institute Ethics Committee has given a waiver for this publication.
Consent to Participate
Informed consent taken from the patient.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All original data available with corresponding author and can be provided upon justified reasonable request.