
Abstract
Objective
To evaluate the clinical outcomes and safety of a triple percutaneous treatment protocol involving mechanical thrombolysis, direct thromboaspiration, and low-dose tPA thrombolysis in patients with moderate to high or high-risk pulmonary embolism (PE).
Design
Single-center retrospective cohort study.
Methods
We included patients aged 18 years or older with moderate to high or high-risk PE, as determined by a chest vascular scan. The primary outcome was survival. Secondary outcomes included functional capacity (FC), systolic pulmonary artery pressure (sPAP), right ventricle (RV) dilation, and tricuspid annular plane systolic excursion (TAPSE). All outcomes were assessed at 48-h post-procedure and at the 6-month follow-up. Additionally, the incidence of adverse events was evaluated during the 48-h following the procedure.
Results
Thirty-five patients were included, comprising 51.43% males, with a mean age of 55 years (SD 18). Survival at 48-h post-procedure was 97%. Of the 19 patients who followed up for 6 months, 95% survived. Eight patients (23%) had FC I-II at admission, which increased to 91% at 48-h post-procedure and 100% at 6 months of follow-up. At admission, 25 patients (71%) had moderate to severe RV dilation. In contrast, 33 patients (94%) had a normal or slightly dilated RV at 48-h post-procedure, and 100% (n/N 19/19) at 6 months of follow-up. In addition, there was a significant reduction in mean baseline sPAP to 36 mmHg (SD 10.3) at 48-h post-procedure and to 29 mmHg (SD 4.9) at 6-month follow-up (P < .001). TAPSE increased significantly to 20.8 mm (SD 4.8) at 48-h post-procedure and to 22.3 mm (SD 2.8) at 6-month follow-up (P < .001). No adverse events occurred.
Conclusion
In patients with moderate to high or high-risk PE, the triple percutaneous treatment protocol appears to be an effective and safe intervention. This strategy achieves high survival and adequate FC, normalizing pulmonary vascular pressures and RV function.
Introduction
Venous thromboembolic disease is the third most prevalent acute cardiovascular syndrome, following myocardial infarction and stroke. 1 It is characterized by deep vein thrombosis (DVT) or pulmonary embolism (PE) and affects approximately 1 to 2 individuals per 1000 annually. 1 PE is associated with a mortality rate of approximately 11.5%, accounting for roughly 100 000 deaths per year in the United States and 350 000 in the European Union. 2
PE exhibits a spectrum of clinical manifestations. Low-risk PE typically does not result in significant functional impairment, with an estimated 90-day mortality rate of approximately 2%. 3 Moderate-risk PE is characterized by an increased embolic burden that elevates pulmonary arterial pressure, often leading to right ventricular (RV) dysfunction; this subgroup has a 90-day mortality rate of about 15%. 3 In high-risk PE, extensive RV collapse and widespread hemodynamic instability are observed, with mortality reaching approximately 58% within 90 days post-event. 3 Moreover, survivors of high-risk PE are at increased risk of developing severe secondary pulmonary hypertension, which can impair long-term functional capacity (FC).4,5
Considering the significant incidence and heterogeneity in the severity of PE, rapid and readily accessible clinical and laboratory markers have been established to facilitate the identification of the most severe cases. 6 Hemodynamic instability, characterized by systolic blood pressure (SBP) less than 90 mmHg, serves as a critical indicator of high-risk PE. 6 Conversely, elevated levels of troponin and B-type natriuretic peptide (BNP), along with RV dilation observed through echocardiography, are indicative of moderate to high risk PE. 6 These markers enable clinicians to stratify patients effectively and determine those who may benefit from more aggressive therapeutic interventions.
The current management of PE primarily involves initiating anticoagulation therapy with heparin. Depending on the severity of the presentation, additional interventions such as systemic thrombolysis, endovascular procedures, or surgical interventions may be employed.7,8 These approaches, while associated with improved prognoses, also carry a higher risk of complications. Endovascular treatment modalities encompass direct fragmentation using a pigtail catheter, thrombectomy and aspiration techniques, thrombolytic thrombectomy, and ultrasound-assisted lysis. 9 Systemic thrombolysis with tissue plasminogen activator (tPA) is recommended for patients with moderate to high and high-risk PE and has shown significant reductions in mortality. However, this therapy is linked to an increased incidence of major bleeding events, including a threefold elevation in the risk of intracranial hemorrhage. 10
In patients with moderate to high and high-risk PE, strategies to mitigate these risks include the use of reduced doses of thrombolytics, aiming to preserve therapeutic efficacy while decreasing adverse events. 11 Consequently, protocols that integrate endovascular therapies with low-dose thrombolytic agents are becoming increasingly attractive, offering the potential for effective treatment while minimizing the complication profile. This study aimed to evaluate the clinical outcomes and safety of a triple percutaneous treatment protocol, which included mechanical thrombolysis, direct thromboaspiration, and low-dose tPA thrombolysis, in patients with moderate to high or high-risk PE.
Methods
Participants and Setting
We conducted a retrospective cohort study at a single center, analyzing patients admitted to the Santa María Clinic in Santiago, Chile, between April 2018 and January 2021. The study included patients aged 18 years or older diagnosed with moderate to high or high-risk PE. The diagnosis was confirmed through computed tomography pulmonary angiography (CTPA) with PE protocol (Siemens Somatom Sensation 64-slice CT scanner). Images were acquired with thin detector collimation and high temporal resolution, and contrast bolus timing was optimized to maximize opacification of the pulmonary arteries. The 64-slice capability and advanced reconstruction algorithms supported accurate assessment of vascular filling defects. No alternative imaging modalities were used to confirm eligibility. Patients were classified based on risk severity: moderate to high risk if they exhibited a high thrombotic burden in the pulmonary arteries on CTPA, along with at least one of the following parameters—elevated troponin or pro-BNP levels, or RV dilation and dysfunction identified via echocardiography; high-risk if hemodynamic instability was also present, indicated by SBP <90 mmHg. Patients with contraindications to thrombolytic therapy were excluded from the study. The study was approved by the Scientific Ethics Committee of Dipreca Hospital (Santiago, Chile) on November 6, 2023 (Registration number: 50).
Procedures
All patients were provided with an explanation of their condition, the available treatment options, and the benefits and risks associated with each procedure. Patients signed a clinical informed consent form for any procedure they chose to undergo.
At admission, assessments included echocardiography and measurement of biochemical parameters. Additionally, a peripheral vascular Doppler ultrasound of the lower extremities was performed to evaluate the femoral veins. In the interventional hemodynamics unit, the femoral vein was punctured to insert an 8 Fr introducer. To confirm the presence of thrombi, bilateral pulmonary arteriography was performed using a 5 or 6 Fr pigtail catheter in both the left and right pulmonary arteries. Mechanical thrombolysis and aspiration of thrombi were carried out in the main, lobar, and segmental arteries. Following reperfusion, selective intra-arterial infusion of alteplase was administered via a pigtail catheter at 20 mg or 10 mg over 20 min, with the dose determined by thrombotic burden, intra-arterial manipulation, and patient fragility. Systolic pulmonary artery pressure (sPAP) was monitored during the procedure.
Post-procedure, patients were transferred to the cardiac intensive care unit. Echocardiographic evaluations were performed at 48-72 h post-procedure, focusing primarily on sPAP and RV function.
Outcomes
The primary outcome was survival, assessed at 48-h post-procedure and at 6-month follow-up. Secondary outcomes included FC, classified according to the New York Heart Association (NYHA) functional classification: Class I indicates no limitation of physical activity; Class II signifies mild limitation; Class III denotes marked limitation; and Class IV reflects the inability to perform any physical activity without symptoms. Additionally, echocardiographic parameters such as sPAP, RV dilation, and tricuspid annular plane systolic excursion (TAPSE) were measured at 48-h post-procedure and at 6-month follow-up. Safety assessments involved cerebral hemorrhage, hemoptysis, and puncture site hematomas within 48 h post-procedure.
To analyze the learning curve associated with the procedure, statistical methods were employed to determine the number of patients required for the procedure time to stabilize.
Data Collection and Statistical Analysis
One researcher collected the data, and a second researcher reviewed it. We used a customized data extraction form in a Microsoft Excel spreadsheet (Microsoft 365 MSO, version 2508 build 16.0.19127.20192).
For data analysis, we used RStudio software (version 2025.09.0 Build 387; copyright 2009-2025 Posit Software, PBC). We presented quantitative variables as means and standard deviations (SD), and categorical variables as counts and percentages. Due to patient attrition at the 6-month follow-up, we used a paired-comparison Student's t-test for repeated measures to assess differences in sPAP and TAPSE between baseline, 48-h post-procedure, and 6-month follow-up. To determine the learning curve, we compared the mean time required for the procedures of the first two patients with that of the remaining patients. If the difference was statistically significant, we then compared the mean time for the first three patients with that of the remaining patients. We continued this process until the difference was no longer statistically significant. For this, we used Student's t-test for independent samples with Welch’s correction. We considered P-values ≤.05 to be statistically significant for all analyses.
Results
Baseline Characteristics of Patients
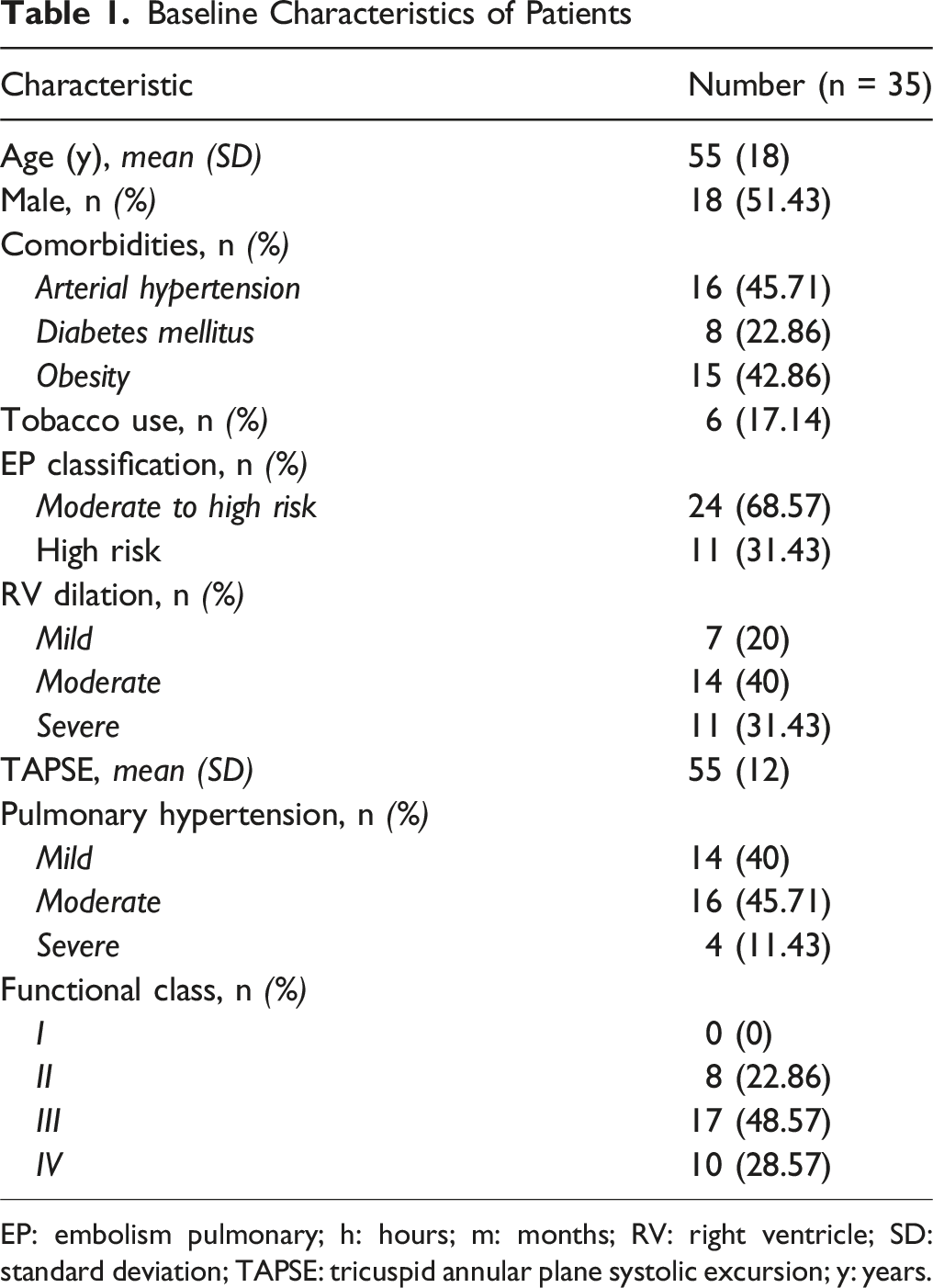
EP: embolism pulmonary; h: hours; m: months; RV: right ventricle; SD: standard deviation; TAPSE: tricuspid annular plane systolic excursion; y: years.
A mean of 2.6 (SD 0.8) lobar arteries were recanalized per patient. The mean intervention duration was 85 minutes (SD 29). The triple percutaneous treatment protocol was safe, as there were no intracerebral hemorrhages, hemoptysis, or hematoma at the puncture site, nor any other type of adverse event.
Overall survival at 48-h post-procedure was 97.14%, and 94.74% of the 19 patients who completed the 6-month follow-up. In patients with moderate to high-risk PE, survival rates were 100% at 48-h post-procedure and 6-month follow-up. In contrast, in patients with high-risk PE, the rates were 90.91% at 48-h post-procedure and 83.33% at 6-month follow-up. Eight patients (22.86%) had CF I-II at admission (Table 1), which increased to 91.43% at 48-h post-procedure and 100% at 6-month follow-up (Figure 1). Progression of functional class. FC: functional class; NYHA: New York heart association; h: hours; m, months. *At the 6-month follow-up, information was available for 19 patients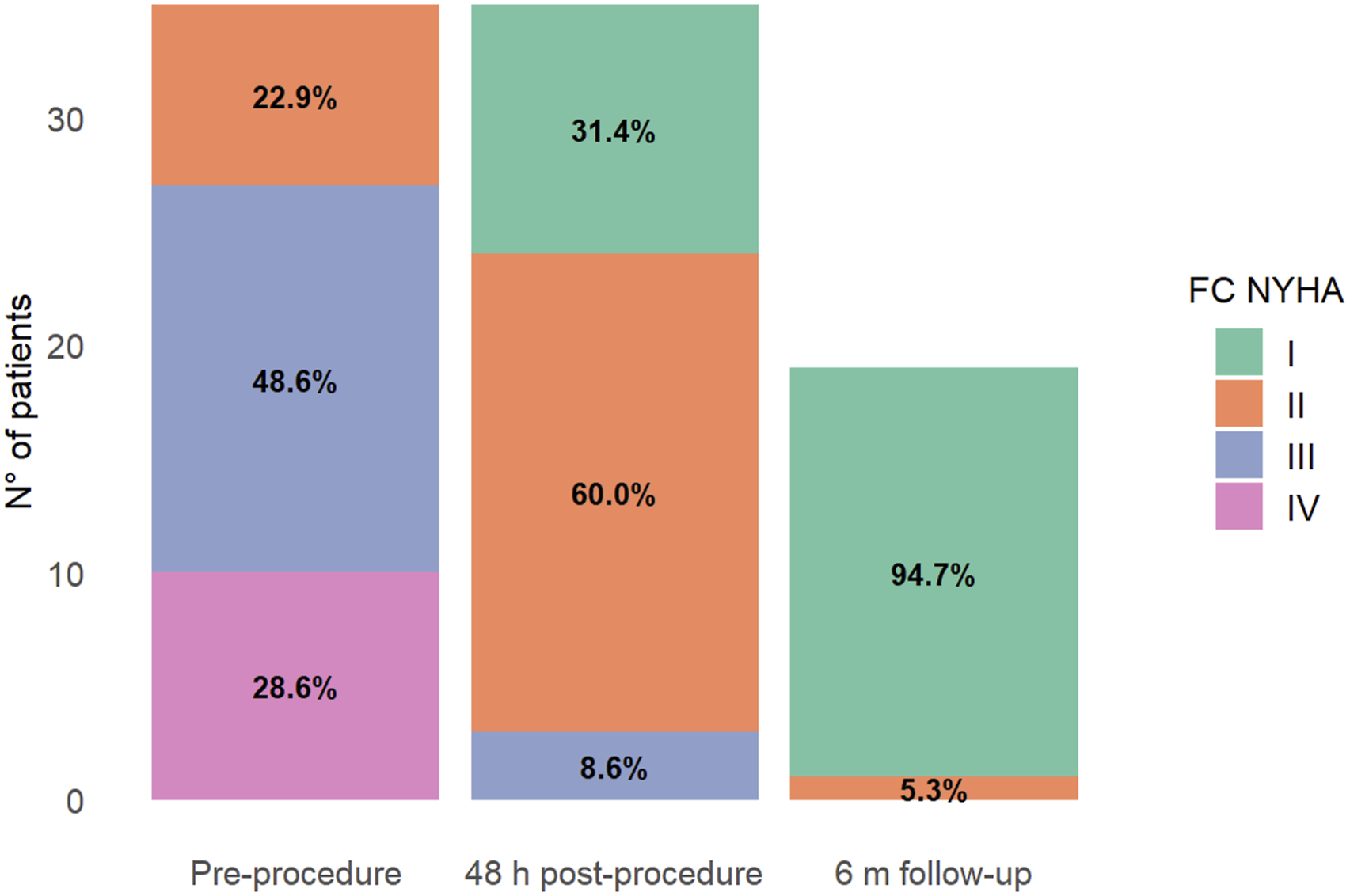
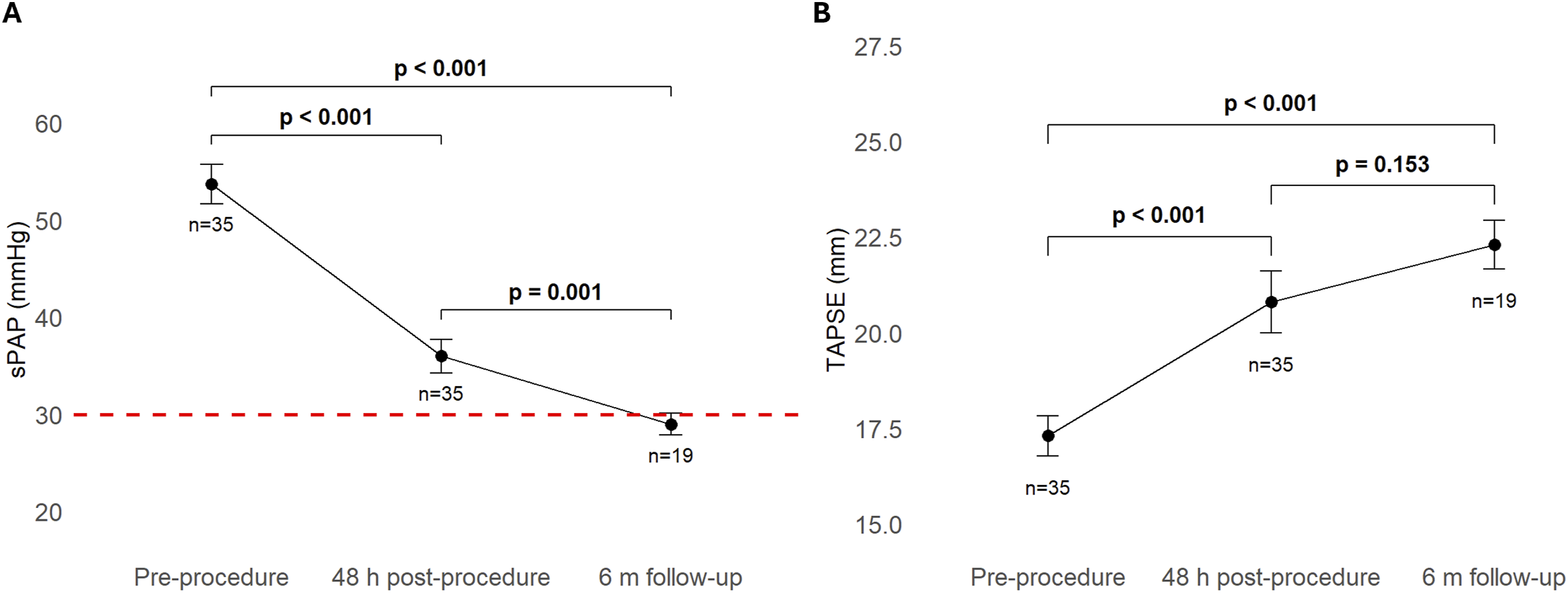
At admission, 25 patients (71.43%) had moderate to severe RV dilation (Table 1). In contrast, 33 patients (94.29%) had a normal or slightly dilated RV at 48-h post-procedure, and 100% at 6-month follow-up (Figure 2). In addition, there was a significant reduction in mean baseline sPAP to 36 mmHg (SD 10.3) at 48-h post-procedure and to 29 mmHg (SD 4.9) at 6-month follow-up (P < .001) (Figure 3A). TAPSE increased significantly to 20.8 mm (SD 4.8) at 48-h post-procedure and to 22.3 mm (SD 2.8) at 6-month follow-up (P < .001) (Figure 3B). Progression of RV dilation. RV: right ventricle; h: hours; m: months. *At the 6-month follow-up, information was available for 19 patients Progression of sPAP and TAPSE. 3A: Comparison of the sPAP at the three assessment moments; 3B: Comparison of the TAPSE at the three assessment moments. sPAP: systolic pulmonary artery pressure; TAPSE: Tricuspid annular plane systolic excursion; h: hours; m: months. *At the 6-month follow-up, information was available for 19 patients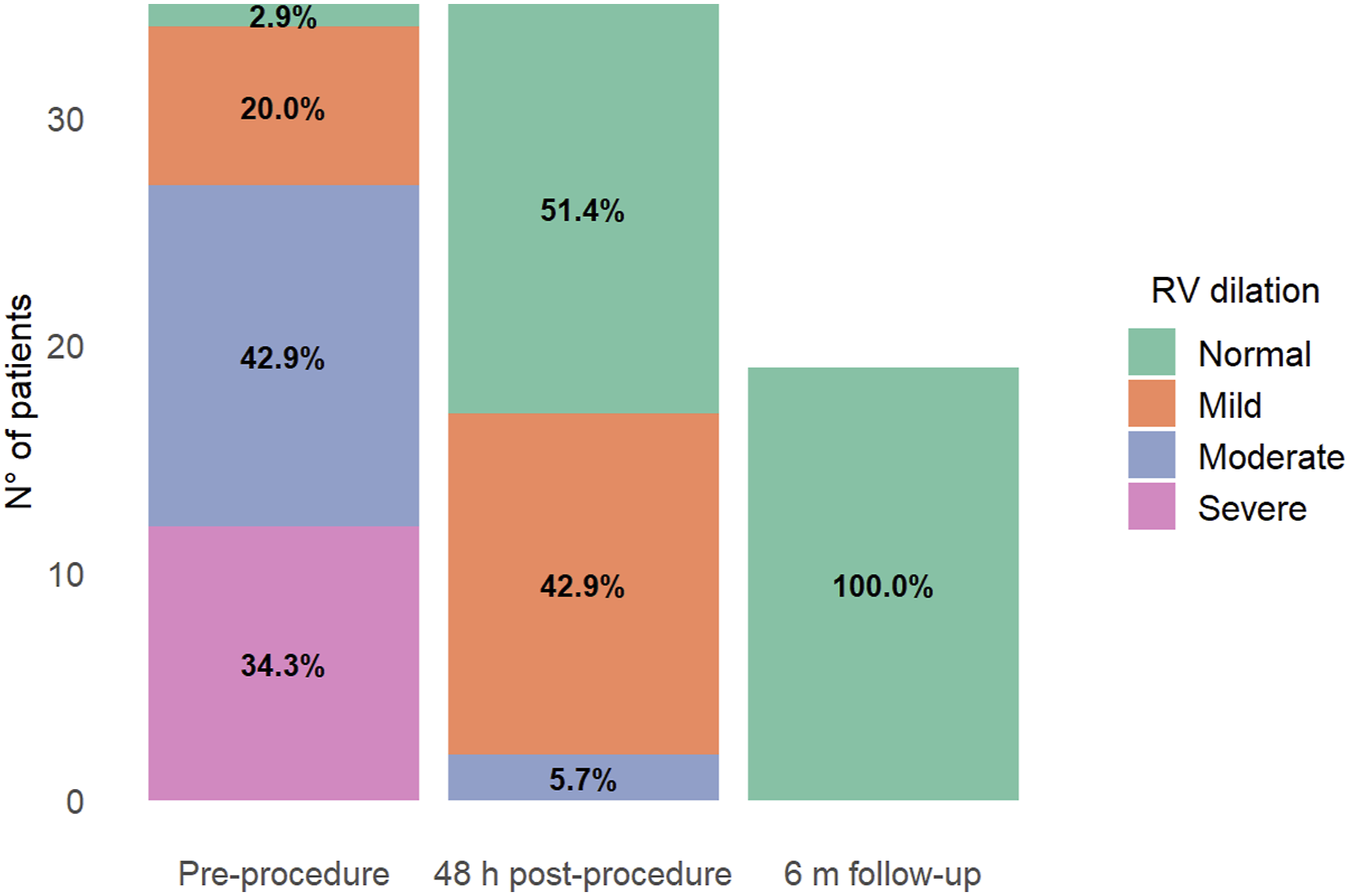
Eleven procedures were necessary to achieve a regular application time for the triple percutaneous treatment protocol. In the first 11 patients, the mean procedure time was 114 min (SD 25). In the subsequent patients, it was reduced to a mean of 70.5 min (SD 18) (P < .001), a time that remained stable until the last patient.
Discussion
Our data indicate that the triple percutaneous treatment protocol, which combines mechanical thrombolysis, direct thromboaspiration, and minimal pharmacological thrombolytic therapy, appears to be a safe and effective intervention for improving clinical outcomes in patients with moderate to high or high-risk PE. Moreover, this therapeutic approach has the potential to prevent the development of pulmonary hypertension in both the short and medium term, which is a common complication associated with thrombotic syndrome.
The management of PE has undergone significant evolution over recent years. 8 The primary objective is to restore blood flow through the early recanalization of occluded venous segments. This strategy aims to prevent vessel stenosis caused by clot organization,12,13 thereby reducing the risk and severity of pulmonary hypertension as well as post-thrombotic syndrome. 14
To date, there have been few reports of mixed percutaneous mechanical thrombectomy using our triple percutaneous treatment protocol. In 2018, Liu et al. conducted a study where percutaneous mechanical thrombectomy was combined with catheter-directed thrombolysis to treat acute PE and DVT of the lower extremities. 15 This study, conducted in China, included 20 consecutive patients with mixed emboli. 15 Like our study, Liu et al. reported significant clinical improvement, with a 100% clinical and technical success rate, and no significant adverse events during hospitalization. 15 Another finding reported by Liu et al. is that no PE recurred at 16-month (SD 6.8) follow-up. 15
Likewise, in 2022, a successful case of hybrid catheter-directed thrombolysis and pharmacomechanical thrombolysis for PE was reported. 16 A 65-year-old female patient with a history of cardiovascular disease, who had been experiencing dyspnea, tachycardia, and hypotension for 20 days, underwent computed tomography pulmonary angiography due to suspected PE. 16 This examination revealed a saddle embolus in the basal lobar arteries and bilateral trunk, causing RV dilatation and hepatic reflux. In response, the patient underwent emergency right heart catheterisation for thrombus fragmentation and catheter-assisted pharmacological thrombolysis. A single dose of 15 mg of alteplase, diluted in 100 mL of 0.9% saline solution, was administered over 8 h. As the procedure was unsuccessful the first time, it was performed again without complications, and this time it was successful. 16
There are other satisfactory reports of mixed percutaneous thrombectomy; however, these have been performed in patients with DVT in the lower extremities. In China, Jiang et al. evaluated the efficacy and safety of combining percutaneous mechanical thrombectomy with catheter-directed thrombolysis and stent placement in the iliac vein. 17 This technique proved to be a safe and effective treatment option for patients with acute proximal DVT caused by venous compression syndrome. 17
Concerning acute PE, mechanical thrombectomy and catheter-directed thrombolysis have been studied separately. Inci et al. compared both techniques in patients with PE in the United States. 18 Catheter-directed thrombolysis was performed in 266 patients, and mechanical thrombectomy was performed in 192, with no differences in hospital mortality, hemorrhage, hemodynamic complications, or catheter-related complications. 18
Our study has limitations. The retrospective design, small sample size, and lack of a control group limit our ability to establish a causal relationship between the triple percutaneous treatment protocol and clinical outcomes. Additionally, patient attrition at the 6-month follow-up may be related to the outcomes assessed. This led us to perform pairwise comparisons between different evaluation times to avoid reducing the number of patients included in our study. Therefore, the results at the 6-month follow-up should be interpreted with caution. Nonetheless, given the limited reports on the effects of mixed percutaneous thrombectomy, our study provides valuable insights, especially regarding immediate post-procedure results. Multicenter clinical trials with larger sample sizes comparing the triple percutaneous treatment protocol to each intervention alone are needed to determine its superiority. Moreover, robust strategies to ensure high patient retention are crucial for establishing long-term effectiveness and safety.
Conclusion
In patients with moderate to high or high-risk PE, the triple percutaneous treatment protocol — ie, mechanical thrombolysis, direct thromboaspiration, and low-dose tPA thrombolysis — appears to be an effective and safe intervention. This strategy achieves high survival and adequate FC, normalizing pulmonary vascular pressures and RV function.
Multicenter clinical trials with larger samples and robust long-term follow-ups, comparing the triple percutaneous treatment protocol with each intervention separately, are needed to assess its superiority.
Footnotes
Ethical Considerations
The study was approved by the Scientific Ethics Committee of Dipreca Hospital (Santiago, Chile) on November 6, 2023 (Registration number: 50).
Consent for Publication
Considering the retrospective design of the study, the Scientific Ethics Committee of Dipreca Hospital (Santiago, Chile) granted us an exemption from obtaining informed consent from each patient.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.