
Abstract
Introduction
Following thoracic endovascular aortic repair (TEVAR) for aortic dissection, visceral arteries arising from the false lumen may require revascularization when communication between the true and false lumens is naturally occluded or iatrogenically sealed. This study describes an endovascular technique using a Wingman catheter for intimal flap fenestration to establish access for revascularization of abdominal visceral arteries originating from the false lumen.
Materials and Methods
A coaxial system was developed by inserting an LRK-shaped catheter within a RE-SS-shaped guiding catheter to maintain shape retention. The Wingman 14C catheter was advanced coaxially through this system to penetrate the intimal flap under biplane fluoroscopic guidance. The created fenestration was dilated with an angioplasty balloon, and this communication pathway was utilized for stent-graft placement to revascularize abdominal visceral arteries arising from the false lumen.
Results
In 1 patient with type B aortic dissection requiring revascularization of the right renal artery, the coaxial insertion of a Wingman 14C catheter through the preshaped guiding catheter successfully achieved obtuse-angle penetration of the intimal flap without complications. Revascularization of the right renal artery was accomplished, with postoperative imaging demonstrating near-complete false lumen thrombosis and favorable aortic remodeling at 6-month follow-up.
Conclusion
This approach represents a useful and safe technique for establishing access to the false lumen in aortic dissection patients when communication between lumens has been eliminated, enabling successful revascularization of visceral arteries originating from the false lumen.
Introduction
Entry closure with thoracic endovascular aortic repair (TEVAR) is commonly indicated for patients with complicated type B aortic dissection or high-risk patients with uncomplicated type B aortic dissection. 1 While false lumen thrombosis in type B aortic dissection has been reported as a protective factor against aortic-related adverse events, 2 TEVAR alone often provides insufficient thrombosis in the thoracoabdominal and abdominal segments, making adequate aortic remodeling difficult to achieve. 3 Therapeutic intervention is required when aneurysmal formation of the aorta occurs. Given the high invasiveness of open surgical artificial graft replacement, endovascular therapy targeting false lumen flow reduction through closure of residual entry tears is frequently employed as an alternative treatment.4-6 The targets for closure are typically entry tears located in the visceral or iliac arteries. However, closure of these entry tears results in decreased blood flow to aortic branches originating from the false lumen, necessitating revascularization of these branches through stent placement. When communication between the true and false lumens is either naturally occluded or closed by therapeutic devices, access from the true lumen to the false lumen is required, followed by catheter-based approach to the abdominal visceral branches arising from the false lumen.
This technical note reports endovascular fenestration of the intimal flap using a Wingman catheter (ReFlow Medical, Inc., CA, USA) for revascularization of abdominal visceral arteries during re-entry closure procedures in aortic dissection.
Materials and Methods
Via a femoral approach, a shaped guiding catheter and angiographic catheter are positioned in either the true or false lumen as perpendicular as possible to the planned puncture site of the dissected aortic membrane. A Wingman 14C catheter (ReFlow Medical, Inc., CA, USA) is then advanced coaxially to penetrate the intimal flap. The created fenestration is subsequently dilated with an angioplasty balloon, and this communication pathway is utilized for revascularization of abdominal visceral arteries arising from the false lumen. This endovascular fenestration technique enables access to visceral arteries originating from the false lumen in situations where entry tears are unclear or have been closed by previous interventions.
This technique was employed in the treatment of a male patient in his 50s with type B aortic dissection. Initial treatment consisted of TEVAR using a combination of a proximal endograft (TX-D endovascular graft 32 mm × 200 mm, Cook Medical, IN, USA) and a distal bare metal stent (TX-D endovascular stent 36 mm × 164 mm, Cook Medical, IN, USA). Despite treatment, the abdominal aorta continued to demonstrate progressive dilatation. Therefore, closure of abdominal entry sites was planned to reduce false lumen flow. The celiac artery originated from the false lumen and exhibited ostial stenosis due to median arcuate ligament compression, prompting coil embolization of this vessel (Target XXL, Stryker, MI, USA). Subsequently, for the superior mesenteric artery involved in the dissection, a stent graft (Viabahn 8 mm × 50 mm, W.L. Gore & Associates, AZ, USA) was placed from the aortic true lumen into the superior mesenteric artery through the struts of the aortic stent to occlude the entry within this vessel. Following the second endovascular intervention, aortic diameter expansion persisted with a false lumen index of 0.54 at the maximally dilated abdominal aortic level and 0.52 at the maximally dilated left common iliac artery (LCIA) level. The false lumen index was calculated by dividing the false lumen diameter by the whole lumen diameter. Therefore, additional closure of the entry tear in the LCIA was planned to promote false lumen thrombosis. However, contrast-enhanced CT and aortography revealed the absence of an entry tear near the right renal artery (RRA), suggesting that simple closure of the LCIA entry would potentially compromise right renal perfusion. Prophylactic revascularization of the RRA was deemed essential prior to additional entry closure (Figure 1). Initial treatment and follow-up imaging of Type B aortic dissection. (A, B) TEVAR was performed for Type B aortic dissection using a combination of proximal endograft and distal bare metal stent. Subsequently, coil embolization of the celiac artery and stent graft placement in the superior mesenteric artery were performed to achieve reentry closure. (C-F) Despite two interventional procedures, progressive dilatation of the abdominal aorta and left common iliac artery persisted. The right renal artery (C, arrow) and inferior mesenteric artery (D, arrow) originated from the false lumen. TEVAR: thoracic endovascular aortic repair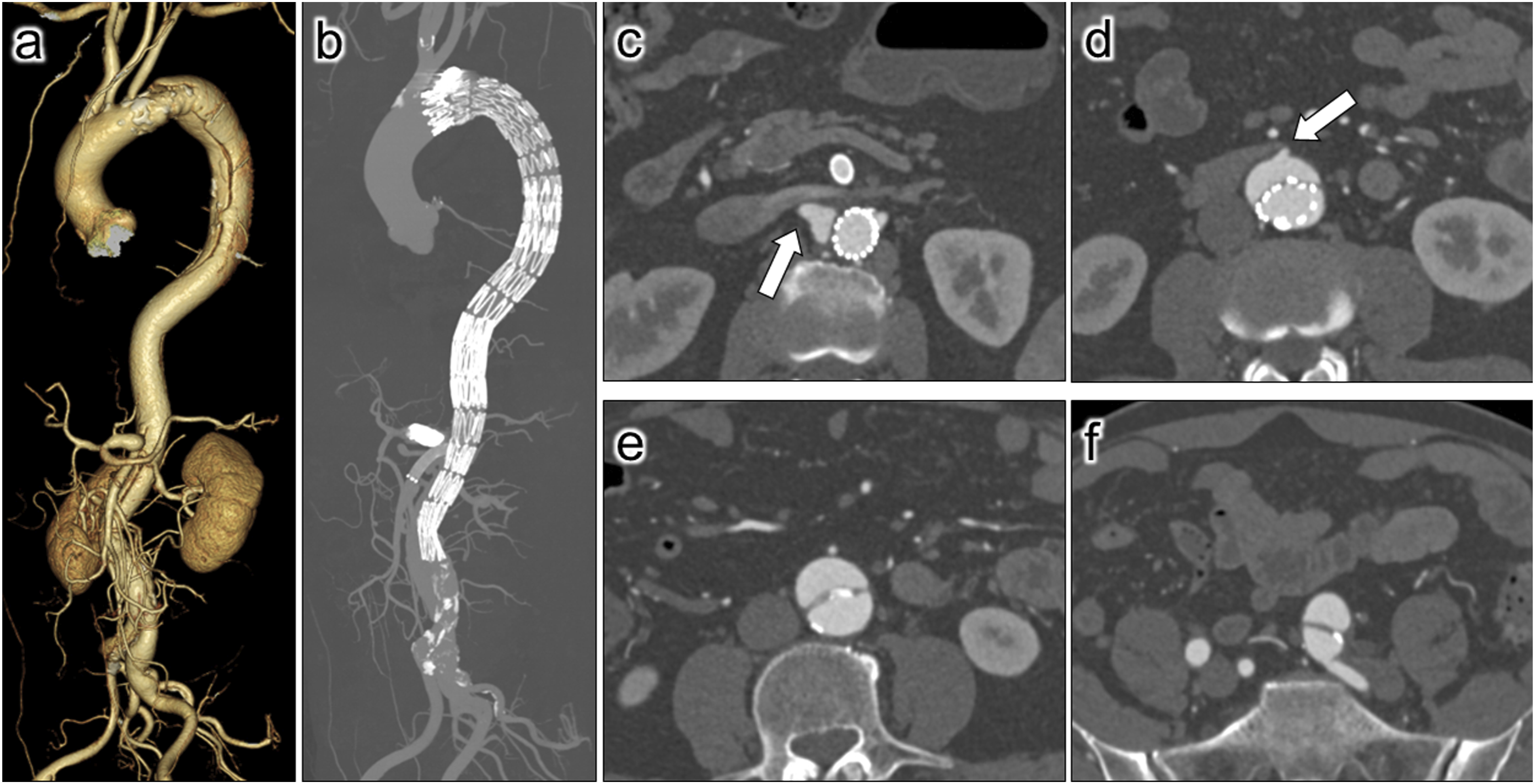
A 7-Fr guiding sheath (Flexor Ansel, Cook Medical, IN, USA) was introduced into the aortic true lumen through the right common femoral artery (CFA), while a 6-Fr sheath (Supersheath, Medikit, Tokyo, Japan) was placed in the false lumen through the left CFA. Following intra-arterial heparin administration (4000 units), aortography performed from both lumens demonstrated no entry tear near the right renal artery, thus confirming the necessity for endovascular fenestration.
A 4-Fr LRK catheter (Seiha; Medikit Co., Tokyo, Japan) was positioned within a 6-Fr RE-SS guiding catheter (Mach 1; Boston Scientific, MA, USA) in the false lumen. The Wingman 14C catheter was then advanced coaxially and, under biplane fluoroscopic guidance, used to penetrate the dissection membrane through the stent mesh. After confirming that the cannula tip of the Wingman 14C catheter was positioned within the true lumen, a 0.014-inch guidewire (Aguru support, Boston Scientific, MA, USA) was advanced from the false lumen into the true lumen, where it was captured by a snare catheter (Atrieve vascular snare kit, COSMOTEC Co, Tokyo, Japan) positioned within the true lumen, thereby establishing a through-and-through wire. The communication created by fenestration was expanded using an angioplasty balloon (SHIDEN 4 mm × 20 mm, KANEKA Medics, Kanagawa, Japan). Through this communication, a stent-graft (VBX 7 mm × 39 mm, W.L. Gore & Associates, AZ, USA) was navigated from the true lumen via the false lumen to the right renal artery ostium. Subsequently, the stent-graft was deployed to bridge from the true lumen to the right renal artery, effectively sealing the communication between the lumens. Aortography from both the true and false lumens confirmed successful revascularization of the right renal artery and closure of the fenestration site (Figure 2). For the inferior mesenteric artery originating from the false lumen, a communication between the true lumen and the false lumen was identified at the IMA level, and a stent-graft (Viabahn 5 mm × 50 mm, W.L. Gore & Associates, AZ, USA) was deployed from the aortic true lumen into the inferior mesenteric artery through this communication to seal the entry at this location. Finally, a stent-graft (Viabahn 10 mm × 50 mm, W.L. Gore & Associates, AZ, USA) was implanted to seal the entry tear within the LCIA. Hemostasis was achieved using vascular closure devices at bilateral groin sites without bleeding complications. Wingman catheter-assisted endovascular fenestration technique. (A, B) True lumen aortography failed to opacify the right renal artery in the early phase (a). In contrast, false lumen aortography revealed opacification of the right renal artery without filling of the aortic true lumen (b). (C, D) The Wingman catheter was positioned in the aortic false lumen to puncture the intimal flap, and the beveled tip (arrow) was advanced into the aortic true lumen through the stent struts of the aortic stent under biplane fluoroscopy. (E, F): A 0.014-inch guidewire was inserted into the true lumen followed by establishing a through-and-through wire (e). Subsequently, the fenestration dilated using an angioplasty balloon (f). (G) A stent graft was deployed through this fenestration from the aortic true lumen via the false lumen into the right renal artery. (H) True lumen angiography confirmed successful right renal artery revascularization and showed that flow through the fenestration was effectively sealed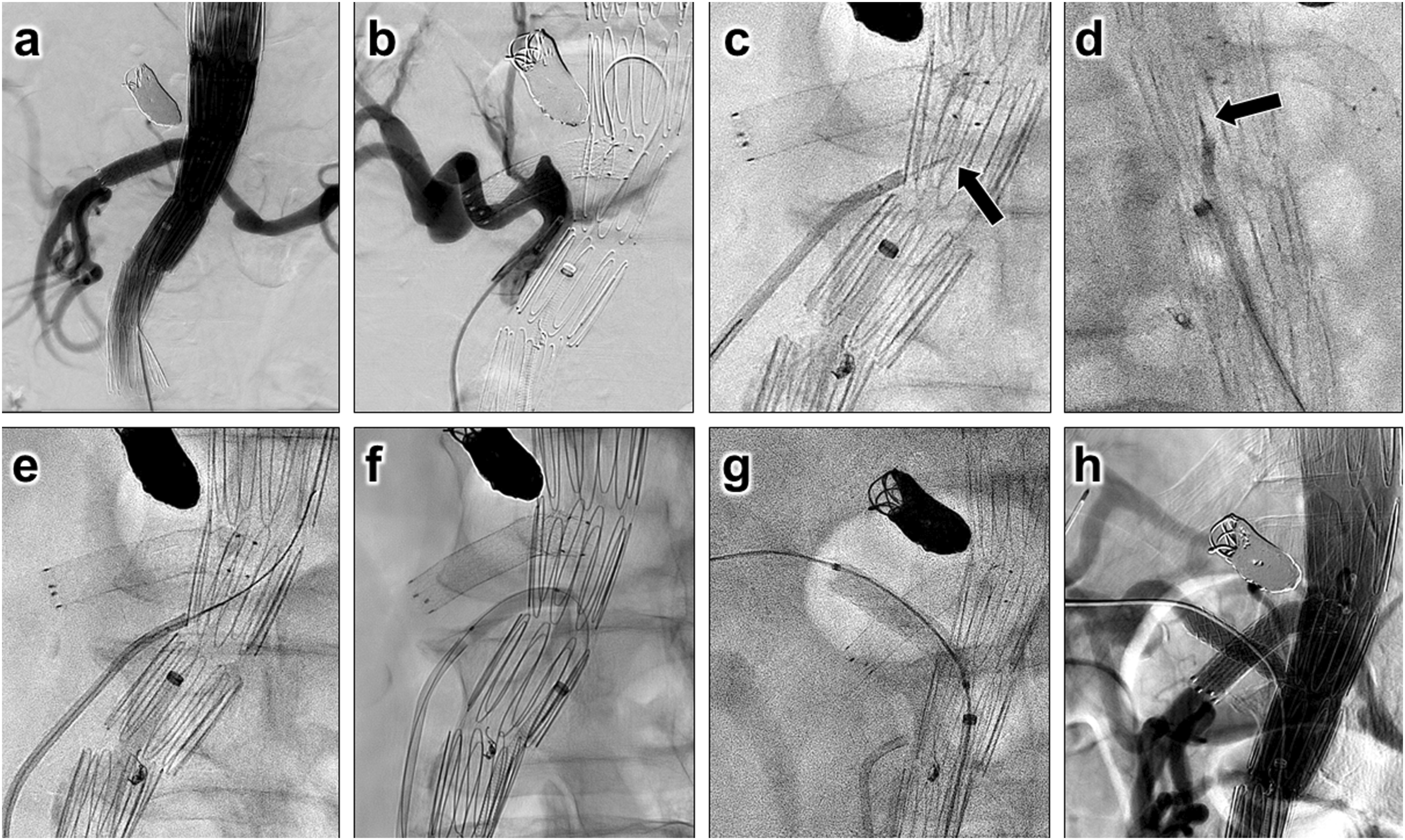
Results
No complications were encountered during the perioperative period. Postoperative contrast-enhanced computed tomography (CECT) at 1 month revealed near-complete false lumen thrombosis with the stent graft placed in the right renal artery remaining patent, with 6-month imaging demonstrating favorable aortic and iliac arterial remodeling (Figure 3). At 6 months, the false lumen index was 0.11 in both the abdominal aorta and the LCIA, representing a significant improvement compared to the preprocedural CT findings. Imaging follow-up. Follow-up CT at 1 month revealed predominantly thrombosed aortic false lumen (A-D), while imaging at 6 months demonstrated reduction in the diameters of both the aorta and left common iliac artery (E-H). (A, E) Right renal artery level, (B, F) Inferior mesenteric artery level, (C, G) Maximally dilated abdominal aorta level, (D, H) Iliac artery level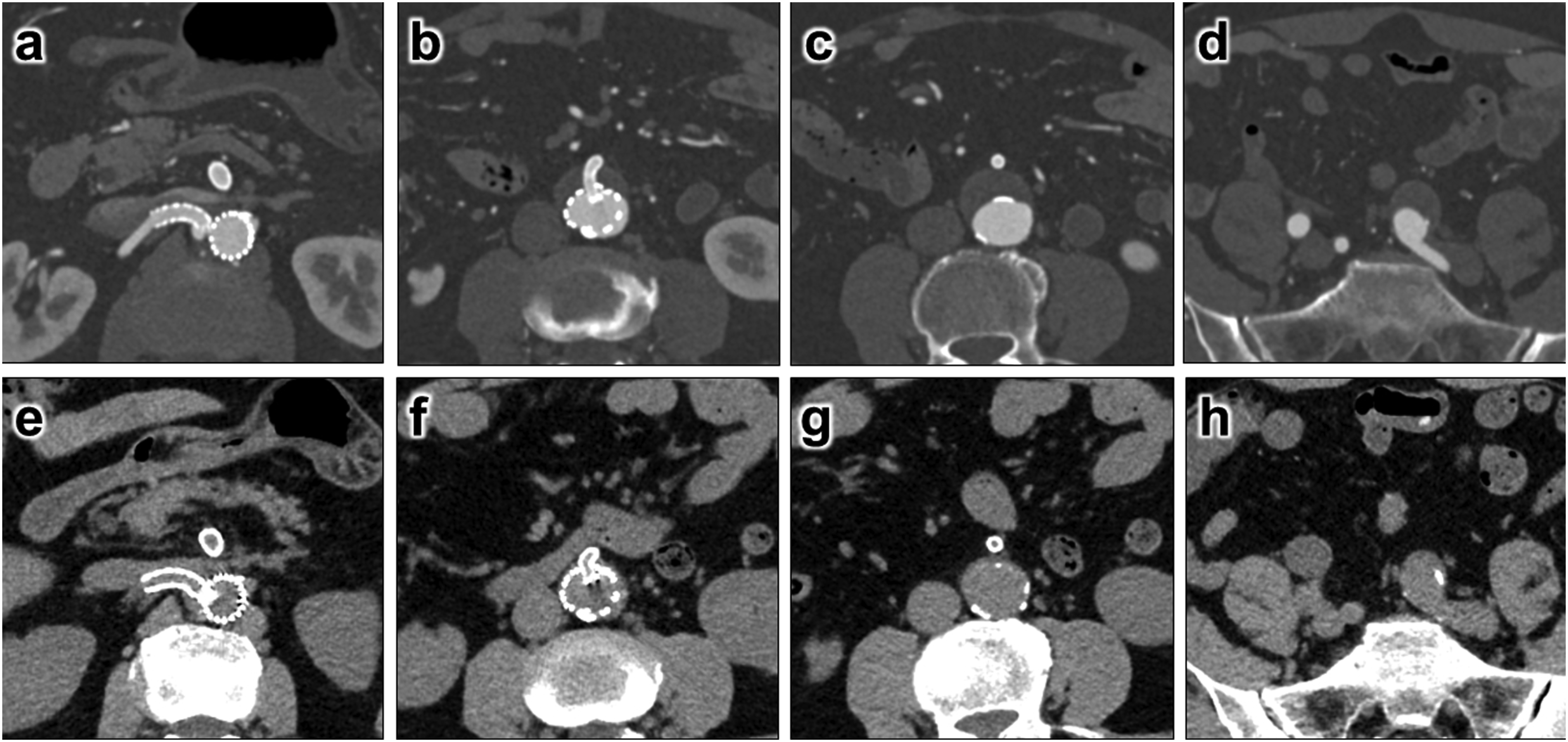
Discussion
Aneurysmal degeneration of the thoracoabdominal or abdominal aorta following TEVAR for type B aortic dissection, with subsequent requirement for therapeutic intervention, is not uncommon.2,3,7 For these patients, endovascular treatment aims to reduce false lumen flow, which is the underlying cause of aortic expansion, by occluding remaining large entry tears. These procedures often require access from the true lumen to the false lumen. However, in cases where communication between the true and false lumens has been naturally obliterated or occluded by previous interventions, fenestration of the intimal flap becomes necessary to establish an access route to the false lumen. 8 Traditionally, intimal fenestration in aortic dissection has been performed to create communication between the true and false lumens, thereby augmenting perfusion to aortic branches arising from the false lumen and resolving organ malperfusion. 9
Various devices have been reported for puncturing the intimal flap, including the Rosch-Uchida needle, transseptal puncture needle, and reentry devices.9-11 The Rosch-Uchida needle and transseptal puncture needle possess high rigidity and tend to track parallel to the aortic course after insertion. Consequently, penetration of the intimal flap at an obtuse angle is challenging with these devices. Regarding reentry devices, the predetermined cannula length may result in inadequate penetration when the intimal flap is thickened.
In this report, a system was developed by coaxially inserting an LRK-shaped catheter within a RE-SS-shaped guiding catheter to maintain shape retention. This configuration allowed the RE-SS shape to be preserved even when the Wingman 14C catheter cannula was inserted within the LRK catheter, and also contributed to the stability of the Wingman catheter position within the RE-SS catheter (Figure 4). This system enabled precise puncture by directing the cannula at an optimal angle to the target puncture site. Conversely, when the Wingman 35 catheter was inserted into the same system ex vivo, catheter straightening occurred with loss of the RE-SS shape, suggesting that smaller-diameter Wingman catheters are preferable for maintaining guiding catheter shape during puncture. Although steerable sheaths are not covered by national health insurance for thoracoabdominal aortic procedures in Japan, they could be a valuable alternative approach in this setting. This technique has several limitations. To avoid serious complications such as aortic hemorrhage from inappropriate puncture during intimal fenestration, the procedure should be performed under multidirectional fluoroscopic guidance or with simultaneous monitoring using fluoroscopy and adjunctive modalities such as intravascular ultrasound. Additionally, in chronic aortic dissection cases with significant intimal thickening or calcification, puncture may be challenging. Schematic illustration of the Wingman catheter-assisted endovascular fenestration technique. By inserting an LRK-shaped catheter into a RE-SS-shaped guiding catheter and coaxially advancing a Wingman 14c catheter through it, puncture of the intimal flap becomes feasible while maintaining the configuration of the guiding catheter. TL: true lumen, FL: false lumen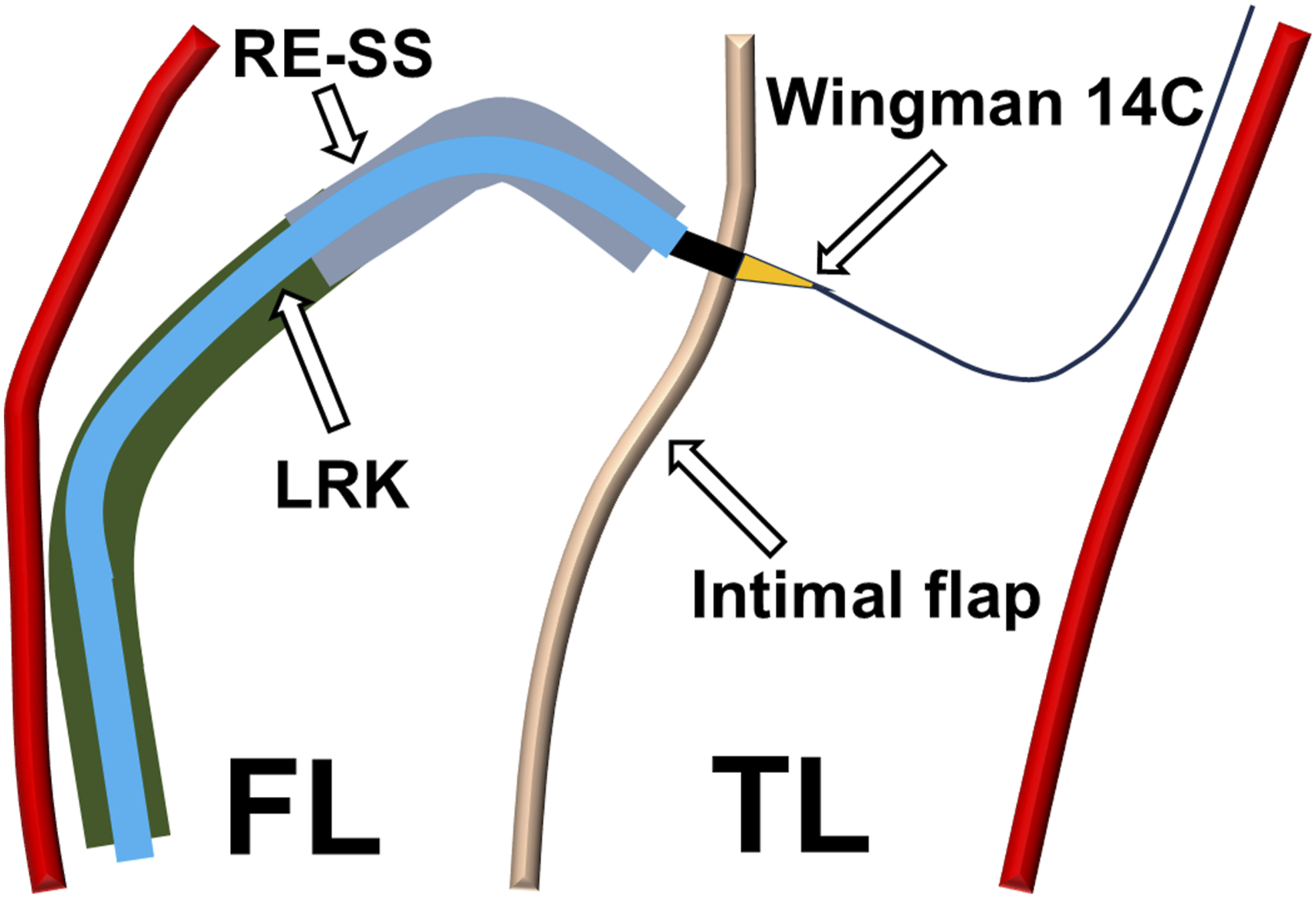
The coaxial insertion of a Wingman 14C catheter through a preshaped guiding catheter facilitates obtuse-angle penetration of the intimal flap during endovascular fenestration, achieving accurate and safe puncture of the target location. This approach represents a useful technique for establishing access to the false lumen in aortic dissection patients where communication between the true and false lumens has been eliminated.
Footnotes
Consent to Participate
Informed consent was obtained from all individual participants included in this study.
Consent for Publication
Consent for publication was obtained for every individual person’s data included in this study.
Funding
This study was not supported by any funding.
Declaration of Conflicting Interests
The authors declare that there is no conflict of interest.
Prior presentation
There have been no presentation about this report.