
Abstract
Background
Major vascular injuries during orthopedic procedures such as open reduction and internal fixation (ORIF) of acetabular fractures are rare but potentially fatal. The iliac veins are particularly vulnerable during anterior approaches due to their close proximity to the pelvic brim.
Purpose
To describe the management of an iatrogenic external iliac vein injury sustained during acetabular ORIF via a modified Stoppa approach and to highlight the role of endovascular techniques as a rescue strategy.
Research Design
Descriptive case study and literature review.
Study Sample
Single patient undergoing acetabular ORIF complicated by intraoperative external iliac vein injury.
Data Collection and/or Analysis
Intraoperative findings, management strategy, and postoperative outcomes were systematically documented. A narrative review of the contemporary literature on endovascular management of iliac and inferior vena cava injuries was performed.
Results
The injury resulted in sudden, massive hemorrhage that could not be controlled through open exposure due to limited visualization and significant bleeding risk. An intraoperative endovascular approach was therefore adopted. Sequential deployment of aortic cuff stent-grafts via femoral access achieved rapid hemostasis while preserving venous patency. Postoperative imaging confirmed patent stents without evidence of extravasation.
Conclusions
Endovascular stent grafting represents a viable and potentially life-saving alternative to open repair for major iliac venous injuries, particularly in anatomically challenging settings. This paper demonstrates the importance of preoperative vascular preparedness and the integration of endovascular rescue strategies into orthopedic trauma surgery.
Introduction
Iatrogenic vascular injuries can be fatal in orthopedic surgery, especially during complex pelvic fracture repair. The iliac veins are particularly at risk during open reduction and internal fixation (ORIF) of acetabular fractures due to their proximity to the acetabulum.1-3 Such injuries can cause severe hemorrhage and hemodynamic instability, requiring prompt recognition and management.
Historically, open surgical repair was the standard approach. 4 However, this can be challenging in patients with obesity or distorted pelvic anatomy. Recently, endovascular techniques—such as stents and aortic cuffs—have become effective alternatives, offering lower morbidity.5,6 Yet, their use remains limited and underreported in orthopedic trauma.
In this study, we describe the management of an iatrogenic right iliac vein injury during ORIF of an acetabular fracture via a modified Stoppa approach. Due to limited exposure and persistent bleeding, an interdisciplinary team performed endovascular rescue using sequential aortic cuffs and iliac vein stenting. This paper shows the importance of early vascular consultation, preoperative imaging, and surgical adaptability. Endovascular strategies should be more widely considered in such cases.
Case Presentation
A 63-year-old male with a body mass index (BMI) of 50 was involved in a motorcycle collision. On initial assessment, he was found to have multiple traumatic injuries, including a right shoulder dislocation, bilateral rib fractures, and a right T-type acetabular fracture. Preoperative pelvic x-ray and CTA imaging confirmed the fracture patterns (Figure 1). Preoperative pelvic radiographs. (A) AP pelvis showing the right acetabulum and pelvis without hardware. (B–C) Portable AP pelvic views demonstrating the right acetabular fracture with associated disruption of the anterior column and pubic rami. No hardware is present in any panel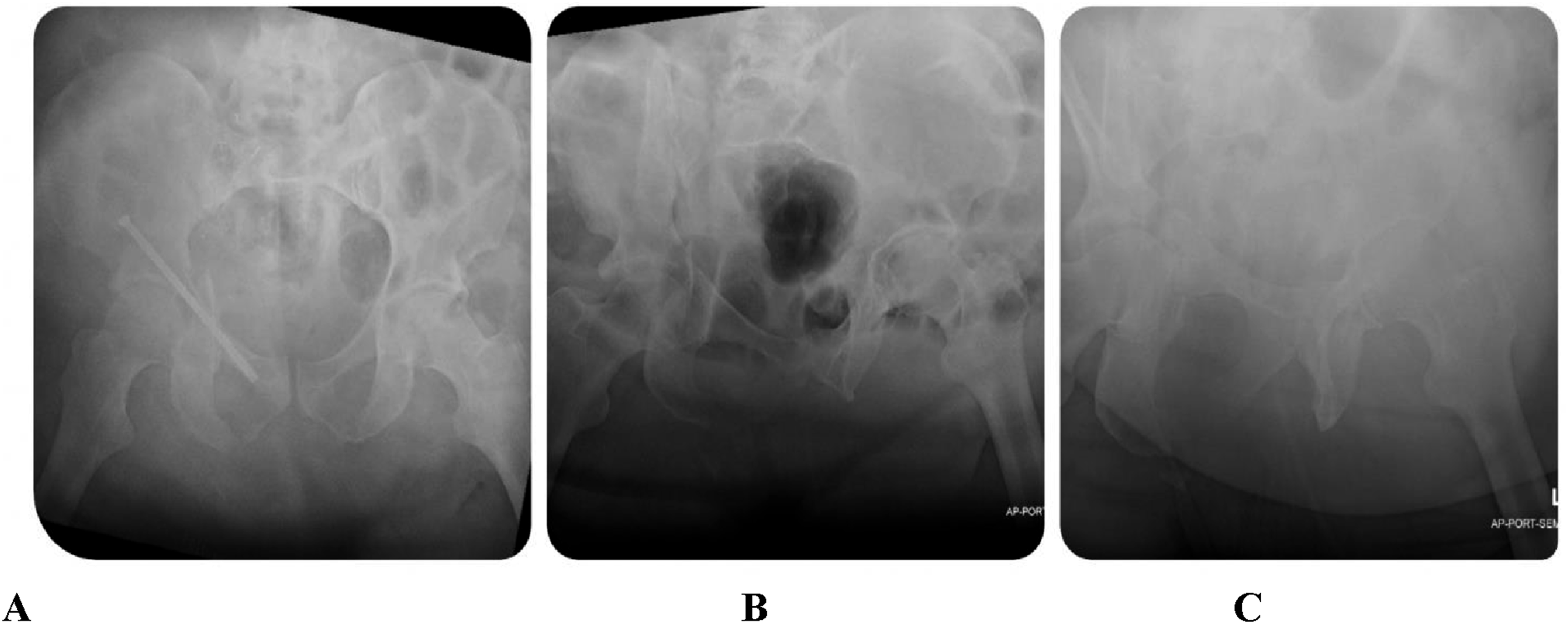
The patient was taken to the operating room (OR) by the orthopedic surgery team for open reduction and internal fixation (ORIF) of the right acetabular fracture via a modified Stoppa approach. The approach was made in the standard fashion, with dissection carried along the pelvic brim using Bovie cautery. Visualization was challenging due to the patient’s morbid obesity. During repositioning of retractors along the iliac fossa to improve exposure, brisk hemorrhage occurred, consistent with an external iliac vein injury. The wound was packed with lap sponges, and the vascular surgery team was urgently consulted.
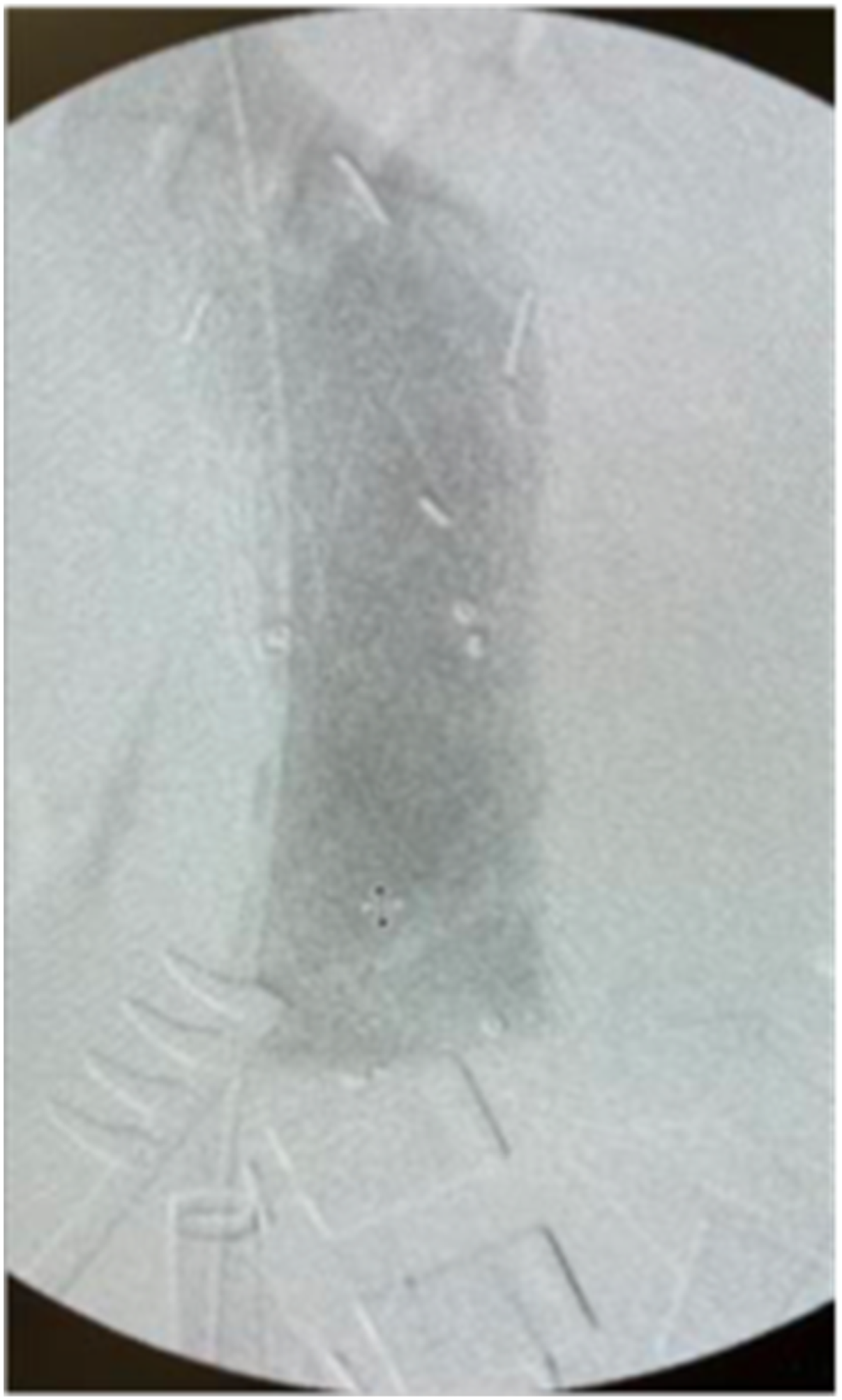
The wound was initially explored to localize the source of bleeding, but due to poor visualization and persistent hemorrhage, the injury could not be identified. After temporary hemodynamic improvement with packing and aggressive blood product resuscitation, brisk bleeding resumed when packing was removed. Given the limited exposure and high risk of exsanguination, an endovascular approach was selected. Bedside ultrasound evaluation of the ipsilateral femoral vein was performed prior to access; however, due to the patient’s hemodynamic instability and hypovolemia, the vein was collapsed and percutaneous cannulation under ultrasound guidance was unsuccessful despite attempts. Given the urgency of hemorrhage control, a small right mid-thigh incision was made to expose the femoral vein via open surgical cut-down. An initial 6 Fr sheath was placed for diagnostic purposes. A right femoral, iliac, and IVC venogram demonstrated extravasation from the external iliac vein (Figure 2). The lesion was crossed with a 0.035 Bentson wire and 45 cm vertebral catheter, followed by exchange for a Rosen wire positioned into the IVC. The 6 Fr sheath was upsized to a 16 Fr sheath over the Rosen wire to accommodate stent-graft delivery. A Gore 26 mm × 3.3 cm aortic cuff and a Medtronic Endurant 25 mm × 4.9 cm aortic cuff were sequentially deployed to seal the injury (Figure 3). The Gore cuff was deployed first to cover the primary injury site in the external iliac vein. Completion venography demonstrated slight residual extravasation from the proximal aspect of the first graft; the Medtronic Endurant cuff was therefore deployed proximally with deliberate overlap, extending into the common iliac vein, to achieve complete hemostasis. Completion venography confirmed hemostasis with preserved IVC flow. Intra-operative venogram showing extravasation at the site of Iliac vein injury Status post placement of Gore 26 mm × 3.3 cm aortic cuff followed by Medtronic Endurant 25 mm × 4.9cm aortic cuff
Following vascular repair, fracture visualization remained limited, and the patient had already sustained major blood loss. Reduction was improved with a spiker pusher, and a percutaneous anterior column screw was placed under fluoroscopic guidance. Using obturator outlet and inlet views, a guidewire was advanced into the superior ramus, overdrilled, and secured with a partially threaded 7.3 mm cannulated screw. The case was concluded without fixation of the posterior column. Postoperative radiographs confirmed successful anterior column fixation.
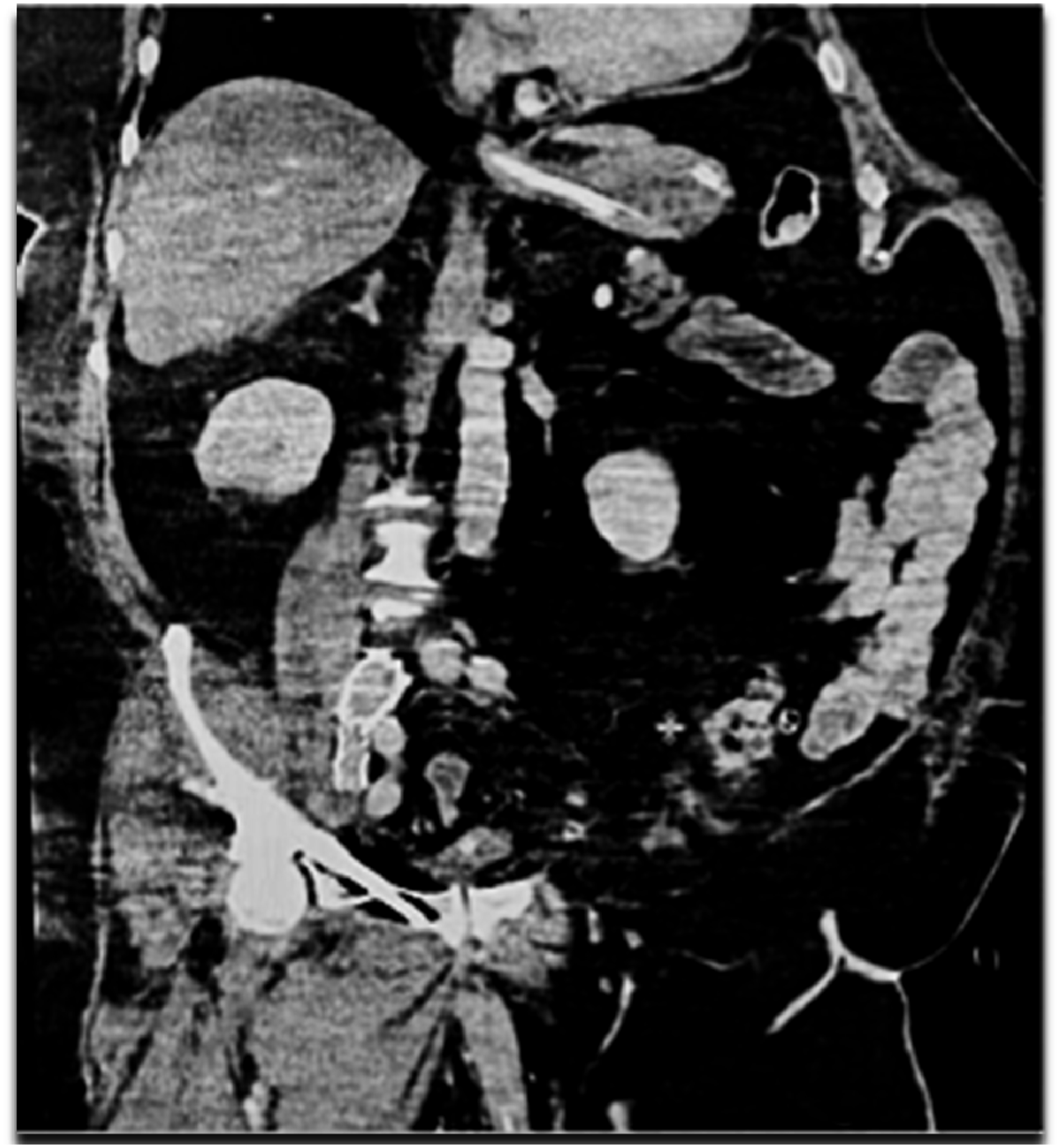
Postoperatively, the patient developed bilateral femoral-popliteal deep venous thromboses (DVTs), likely due to immobility, trauma, and obesity, requiring inferior vena cava (IVC) filter placement (Figure 4). Therapeutic anticoagulation was subsequently initiated. Follow-up CTA demonstrated patent iliac vein stents with no residual extravasation (Figure 5). IVC filter in place for bilateral femoral-popliteal DVT Follow-up CTA demonstrating patent iliac vein stents without residual leak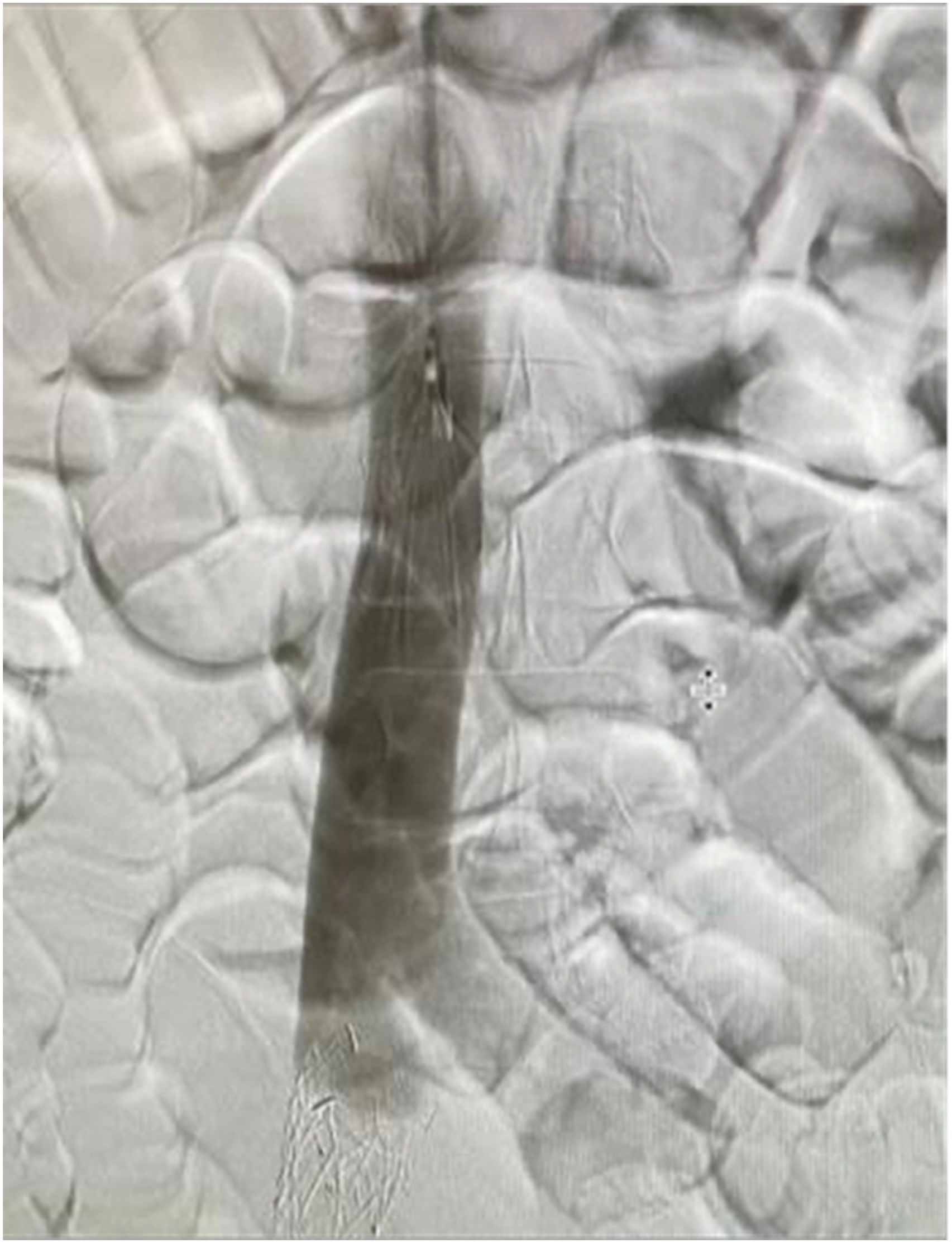
Discussion
The proximity of the external iliac vein to the acetabular brim situates this vessel in a critical “danger zone” of anterior pelvic exposures. In this morbidly obese patient, limited visualization coupled with retractor manipulation likely resulted in avulsion of the vein with brisk hemorrhage. When open control is technically limited or unsafe, endovascular stent-grafting is an effective rescue strategy. Covered stents rapidly achieve hemostasis while maintaining venous continuity and avoid the morbidity associated with open repair or ligation. In this case, the application of aortic cuff-type stent grafts resulted in immediate control of bleeding with preservation of iliac venous patency, enabling safe completion of fixation.
Stent sizing in the setting of acute venous hemorrhage presents unique challenges. The standard external iliac vein diameter is approximately 12 mm. However, ensuring an accurate intraprocedural measurement is often not feasible in hemodynamically unstable patients with collapsed veins. In this case, the preoperative CTA was performed as a trauma study and did not include a dedicated venous phase of the iliac system. Bedside ultrasound confirmed venous collapse prior to access, precluding reliable diameter measurement at the time of intervention. The decision to use 25-26 mm aortic cuff stent-grafts was driven by available inventory: the only covered stents immediately accessible were iliac limb extensions measuring 12 mm and 14 mm in diameter, which were judged inadequate for achieving a reliable hemostatic seal given the patient’s large body habitus and the degree of hemorrhage. Although the degree of oversizing relative to the standard iliac vein diameter is acknowledged, and carries a theoretical risk of device infolding or secondary occlusion, hemostasis was achieved and follow-up CTA confirmed stent patency without evidence of these complications. This case sheds light on the importance of maintaining a readily accessible inventory of varied stent-graft sizes in institutions managing complex pelvic trauma, and of performing dedicated venous-phase CT imaging in the preoperative workup when time permits. 7
The use of 2 stent-grafts in this case warrants clarification. The Gore 26 mm × 3.3 cm aortic cuff was deployed first to cover the primary injury in the external iliac vein. Post-deployment venography demonstrated slight residual extravasation from the proximal aspect of the first graft, indicating incomplete seal at the proximal landing zone, most likely due to injury extension into the distal common iliac vein rather than stent migration. A second covered stent — the only remaining available device, a Medtronic Endurant 25 mm × 4.9 cm aortic cuff — was deployed proximally with deliberate overlap to complete the repair; when 2 stents are required, overlapping by at least 2 cm is recommended to ensure seal integrity. 8 The stent-graft construct extends to the level of the common iliac vein; intraoperative venography did not demonstrate occlusion of the ipsilateral hypogastric vein, and no clinical sequelae attributable to hypogastric venous insufficiency were observed postoperatively. Bilateral femoral access was not utilized in this case given the urgency of hemorrhage control; however, bilateral access should be considered in less emergent settings as it provides superior visualization of the caval bifurcation and both common iliac systems, facilitating more precise anatomic localization and stent positioning. 9 The intraoperative imaging in this report was acquired with a mobile C-arm fluoroscopic system rather than a fixed angiographic suite, which limits spatial resolution and reconstruction capability compared to a hybrid operating room environment; this represents a recognized limitation of endovascular rescue performed in a standard orthopedic theater.
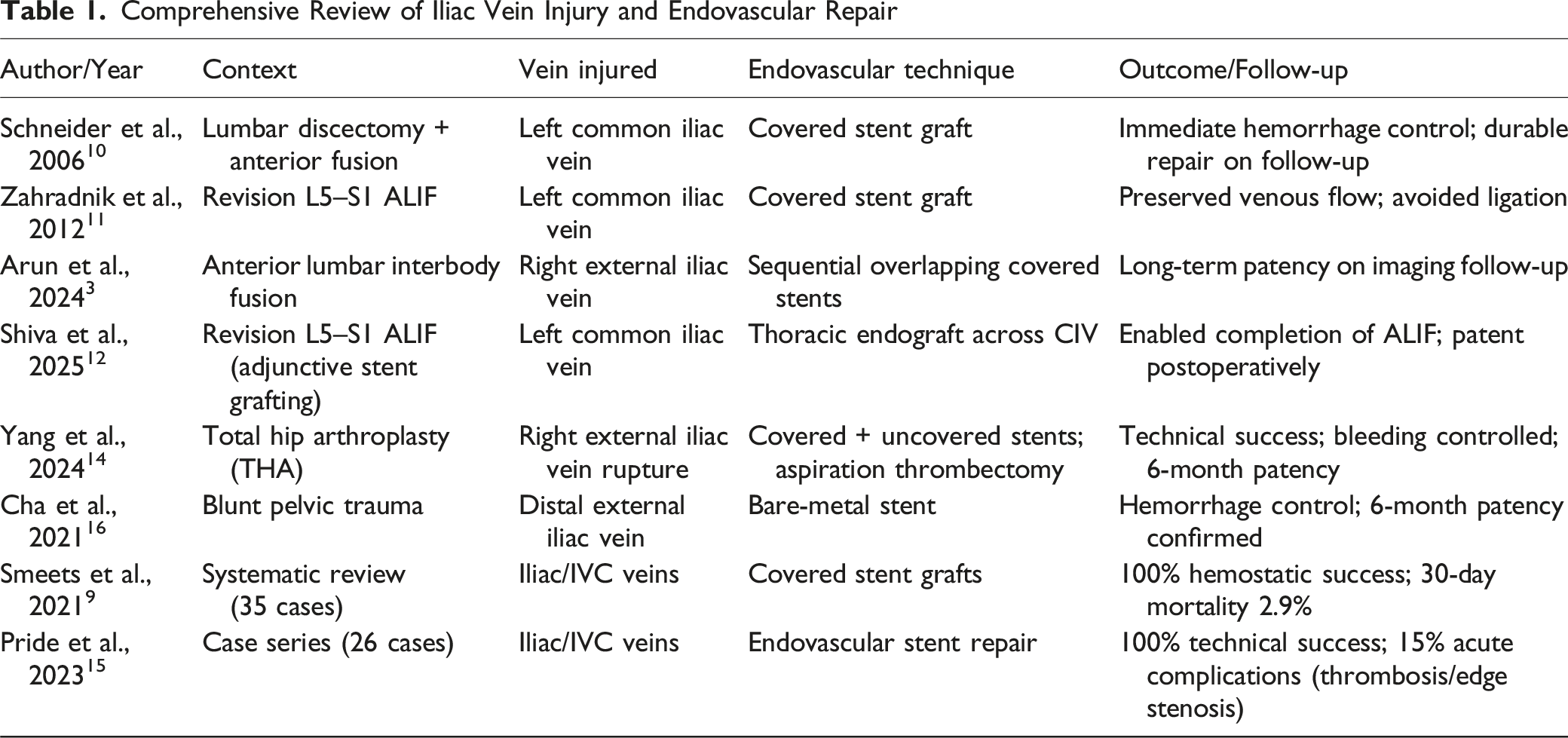
Although reports are limited, there is evidence supporting the effectiveness of endovascular repair for intraoperative venous injury. In spine surgery, Schneider et al. (2006) described emergent covered-stent repair of a left common iliac vein laceration during lumbar discectomy with durable success. 10 Zahradnik et al. (2012) reported 2 anterior lumbar fusion revisions complicated by iliac vein tears, both treated with covered stents that preserved flow without ligation. 11 Likewise, Arun et al. (2024) similarly documented successful sequential stent-graft repair of an external iliac vein injury during ALIF, and subsequent reports have described thoracic endograft use across the left common iliac vein to complete revision ALIF procedures without there being major hemorrhage. 12 Collectively, these studies confirm that endovascular “bailout” with covered stents is both technically feasible and clinically effective in confined pelvic surgical fields.
Comprehensive Review of Iliac Vein Injury and Endovascular Repair
Our patient developed early bilateral femoral-popliteal deep-vein thromboses, likely related to trauma, immobility, and obesity. These were successfully managed with inferior vena cava filter placement followed by anticoagulation. In this patient, standard DVT prophylaxis was administered by the orthopedic service during the perioperative period. Following diagnosis of bilateral femoral-popliteal DVTs, anticoagulation was escalated to full therapeutic dosing. Given the combination of venous stents, documented DVT, and ongoing thrombotic risk factors (morbid obesity, prolonged immobility, and prior trauma), the patient was transitioned to long-term therapeutic anticoagulation at discharge, on which he remains. Optimal post-stenting antithrombotic regimens remain undefined, as published protocols vary widely, underscoring the need for standardized guidance balancing thrombosis prevention with bleeding risk.
To our knowledge, this represents one of the first documented uses of endovascular stent-grafting for an external iliac vein injury sustained during acetabular ORIF via a modified Stoppa approach. Unlike anterior spinal exposures, acetabular ORIF affords even more limited visualization of the pelvic vasculature, especially in obese or traumatized patients. Our experience shows that with prompt recognition and early vascular collaboration, endovascular rescue can be successfully executed in this challenging orthopedic setting, thus extending the applicability beyond spine and vascular trauma to orthopedic trauma surgery, where hybrid readiness is usually underemphasized. Our technique ensures immediate hemostasis, thereby preserving the continuity of venous flow and reducing the morbidity associated with open repair. Our case also shows the importance of multidisciplinary readiness and postoperative anticoagulation planning. Long-term management protocols will be refined with more reports or larger scale studies on similar experiences, thus firmly establishing the place of endovascular rescue in complex pelvic and orthopedic trauma management.
Footnotes
Consent to Participate
Institutional review board (IRB) approval was not required for this single-patient case report, as per the policies of the authors’ institution. Written informed consent was obtained from the patient for publication of this report and associated images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient Perspective
The patient expressed satisfaction with the prompt, minimally invasive management and appreciated the collaborative surgical care.