
Abstract
Introduction
We present a case of acute limb ischemia (ALI) in a morbidly obese patient with prior femoro-popliteal artery PTFE bypass occlusion successfully treated with a hybrid femoral-to-posterior tibial artery bypass utilizing the previously occluded graft.
Case Report
A 69-year-old morbidly obese woman presented with acute left leg pain and numbness with preserved motor function. Computed tomography angiography (CTA) demonstrates chronic superficial femoral artery and femoro-popliteal PTFE bypass occlusion with a new native popliteal artery thrombosis and loss of tibial runoffs. After systemic heparinization, the leg was revascularized through a small medial thigh incision and a jump PTFE bypass to the posterior tibial artery. The previously occluded femoro-popliteal artery bypass was accessed to re-establish proximal flow through a retrograde endovascular construction using a 7 mm by 25 cm Viabahn (Gore, Flagstaff, AZ) stent. This stent was used as a bridge with distal deployment within a new 6 mm PTFE graft, which was then anastomosed in an end to side fashion to a Linton patch of the posterior tibial artery. There were no postoperative complications, and the ankle-brachial-index was measured to be 0.98 with a CTA with runoffs confirming bypass patency.
Discussion
ALI in the setting of a prior bypass occlusion in a morbidly obese patient reflects the typical contemporary patient and disease complexity, which demands corrective revascularization with appropriate mitigation/prevention of other postoperative complications. A limited thigh exposure to access a previously occluded bypass can successfully restore in-line flow in these high-risk patients.
Conclusion
Hybrid lower extremity revascularization is an alternative surgical modality to restore in-line flow to a lower extremity as a limb salvage option while avoiding groin re-exploration in a previously accessed groin for bypass construction in a morbidly obese patient.
Keywords
Introduction
Acute limb ischemia (ALI), or sudden decrease in arterial blood flow to the extremities can threaten the viability of tissues. 1 The estimated incidence is approximately 14 cases per 100 000 persons per year, and despite a decline in the overall number of cases, its mortality and amputation rates remain high, with up to 25% and 30%, respectively. 2 The classic presentation of ALI includes acute onset of pain, pallor, pulselessness, poikilothermia, paresthesia, and paralysis. 3 Initial assessment should prioritize the evaluation of limb viability, usually through physical examination alone. However, additional imaging studies may be useful under certain circumstances that modify the management approach, such as a previous history of limb revascularization, inconclusive physical examination findings, or unusual clinical scenarios. In this context, computed tomography angiography (CTA) is the imaging of choice. Magnetic resonance angiography (MRA) is often reserved for patients with contraindication to iodinated contrast, whereas digital subtraction angiography (DSA) remains the gold standard for definitive anatomical assessment, when intervention is planned. 3 The management of ALI relies on systemic anticoagulation (unless contraindicated) and timely revascularization. 3
Even though treatment algorithms are well established for ALI, the approach becomes more challenging in the scenario of morbid obesity and patients with previous open failed revascularization operations.4,5 Therefore, hybrid revascularization strategies, combining open and endovascular techniques, are an alternative in such cases to limit morbidity from a redo groin exposure. 3 We present a case of ALI in a woman with an occluded femoro-popliteal PTFE bypass and morbid obesity successfully treated with a hybrid femoral-posterior tibial artery (PTA) revascularization avoiding groin re-exploration.
Case Report
A 69-year-old woman presented to the emergency department with acute left lower extremity pain and numbness at rest for approximately 10 h. Her past medical history was significant for peripheral arterial disease (PAD) with an extensive left lower extremity revascularization history performed at an outside institution, including bilateral common femoral artery endarterectomy in 2018, subsequent left superficial femoral artery (SFA) stenting, and a left SFA-to-above-knee popliteal artery bypass with a PTFE graft performed in 2021. In February 2024, she presented with an episode of acute limb ischemia requiring surgical thrombectomy of the bypass graft. Her other comorbidities included diabetes mellitus, hypertension, hyperlipidemia, morbid obesity (BMI >40), chronic obstructive pulmonary disease, obstructive sleep apnea, hypothyroidism, autoimmune hepatitis, and cirrhosis. On examination, the left lower extremity was cold and pale, with diminished sensation and absent pedal pulses; motor function was preserved. She was subsequently heparinized and admitted for revascularization.
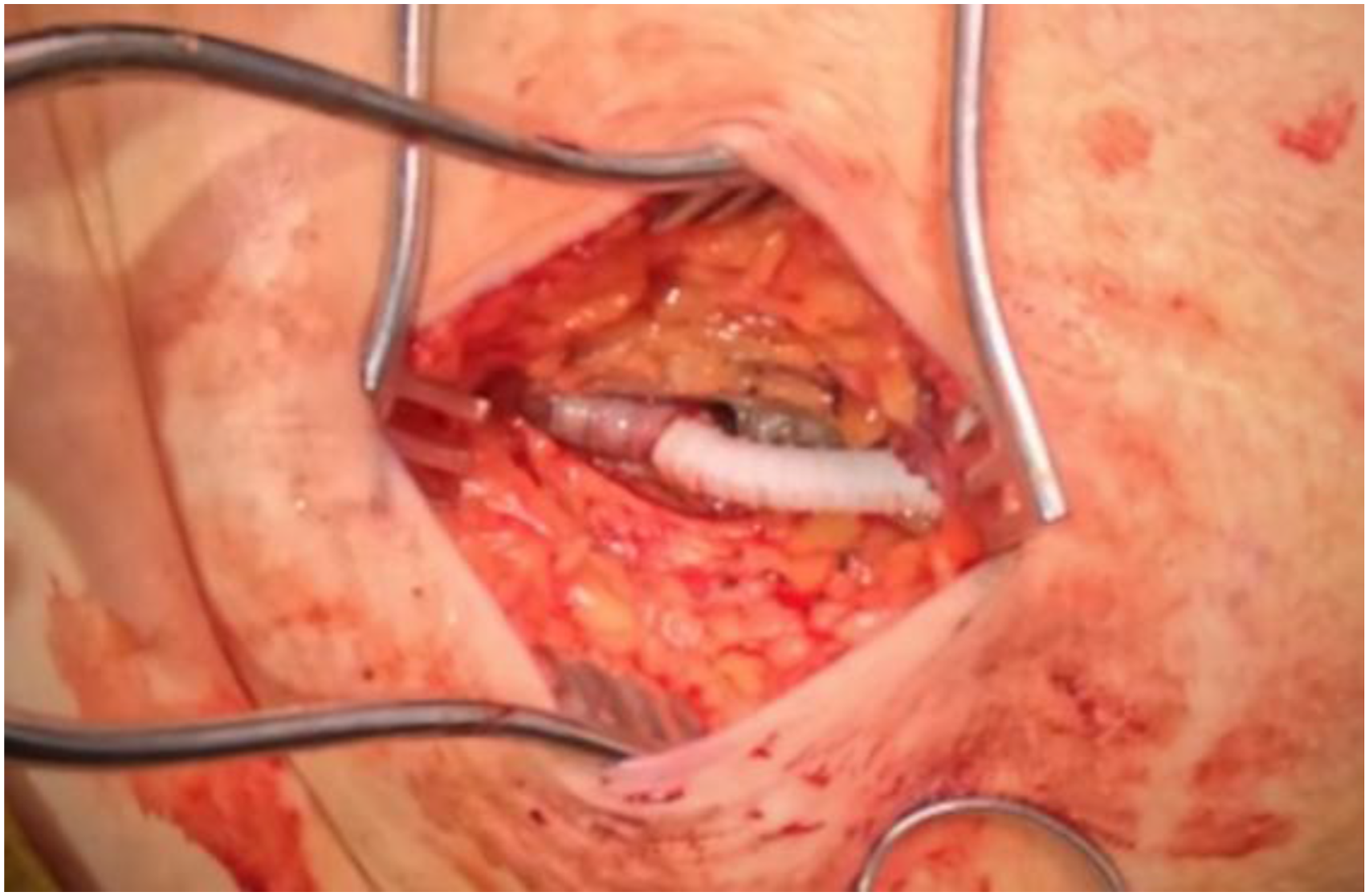
Initial workup included a Doppler ultrasound with no detectable arterial signals in the distal tibial vessels and a CTA that showed chronic occlusion of the left SFA and prior femoro-popliteal PTFE with additional new occlusion of the popliteal artery and loss of tibial runoffs (Figure 1). The surgical strategy consisted of a hybrid left femoral-to-posterior tibial artery (PTA) bypass with a PTA patch using great saphenous vein. We localized the most superficial portion of the occluded femoro-popliteal PTFE graft in the medial upper aspect of the left thigh using ultrasound guidance. Following this, a 5 cm longitudinal incision was made over the medial thigh, and the PTFE graft was accessed with a micropuncture needle followed by the insertion of a 7-French Ansel sheath, which was inserted through a second 6 mm PTFE graft. Using wire and catheter technique, the left external iliac artery was accessed in a retrograde fashion under fluoroscopic guidance. Subsequently, a 7 mm × 25 cm Viabahn stent (Gore, Flagstaff, AZ) was advanced and deployed at the origin of the PTFE graft and balloon angioplastied using a 7 mm by 150 cm balloon. With subsequent distal inflation of this balloon, the Viabahn stent was further inflated within the second PTFE graft over the Ansel sheath (Figure 2). (A) Coronal views of pre-operative CTA with runoffs with occluded popliteal artery and loss of runoffs (yellow arrows). (B) Post-operative CTA demonstrating patent hybrid bypass graft (blue arrows) Photograph of the proximal segment of the hybrid revascularization (PTFE with new PTFE extension with Viabahn stent relining)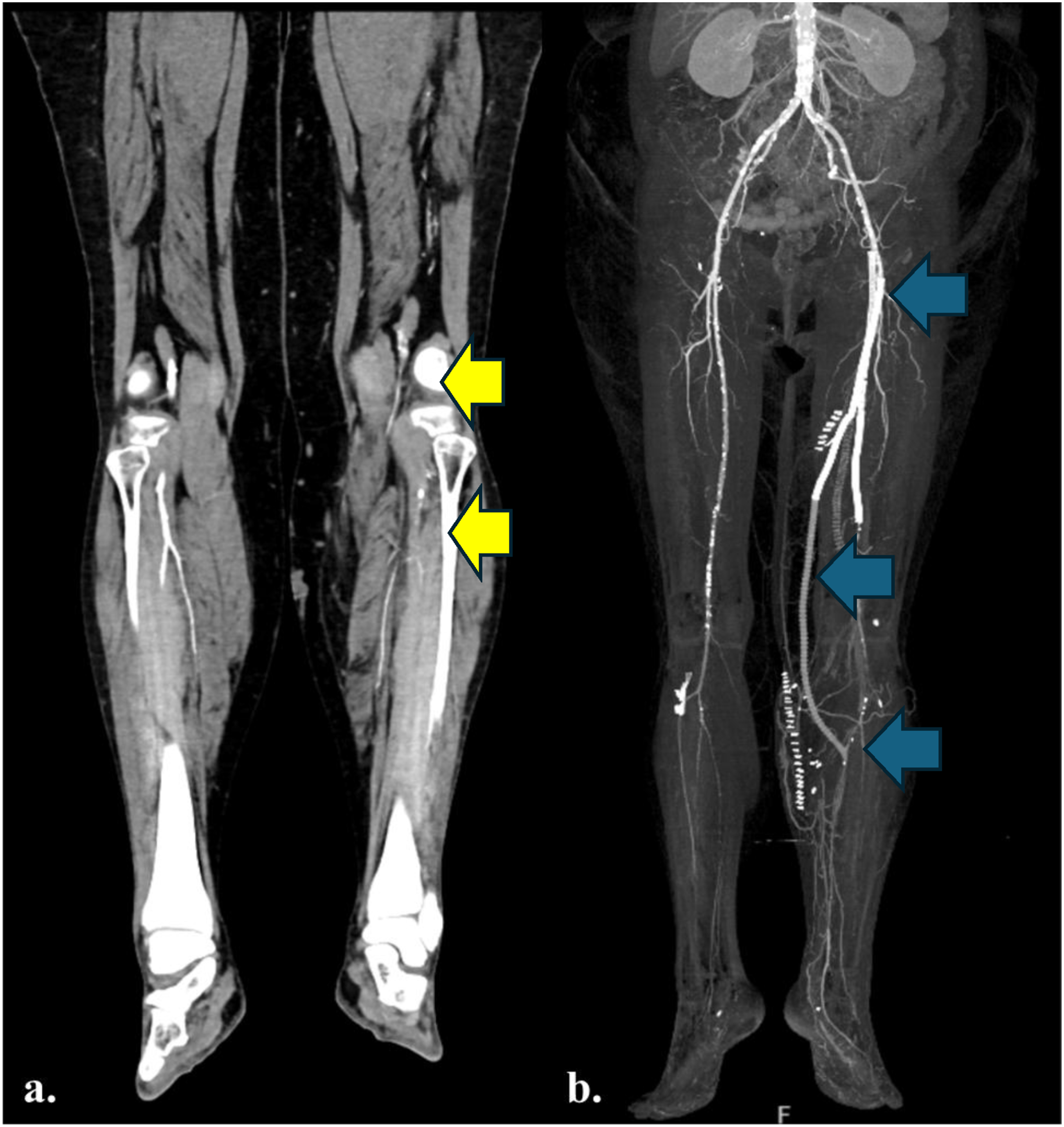
Concurrently, the PTA below-the-knee was explored; although the great saphenous vein (GSV) was insufficient for a full bypass conduit, it was adequate to complete the patch angioplasty. The new PTFE graft was then tunneled down to the calf to perform an end-to-side anastomosis to the Linton patch (Figure 3). Postoperatively, we confirmed biphasic PTA and dorsalis pedis artery signals. The patient was discharged home on postoperative day 2. Patient follow-up at 1 week showed improvement of ankle-brachial index (ABI) at 0.98. At the 3-week follow-up visit, the patient continued to recover and the CTA with runoffs revealed patent fem-PTA artery bypass (Figure 1). At 3-month follow-up, the patient remained asymptomatic with normal bilateral ABIs and a patent left femoral-to-posterior tibial bypass on duplex ultrasound without anastomotic stenosis. Distal end-to-side anastomosis to GSV patch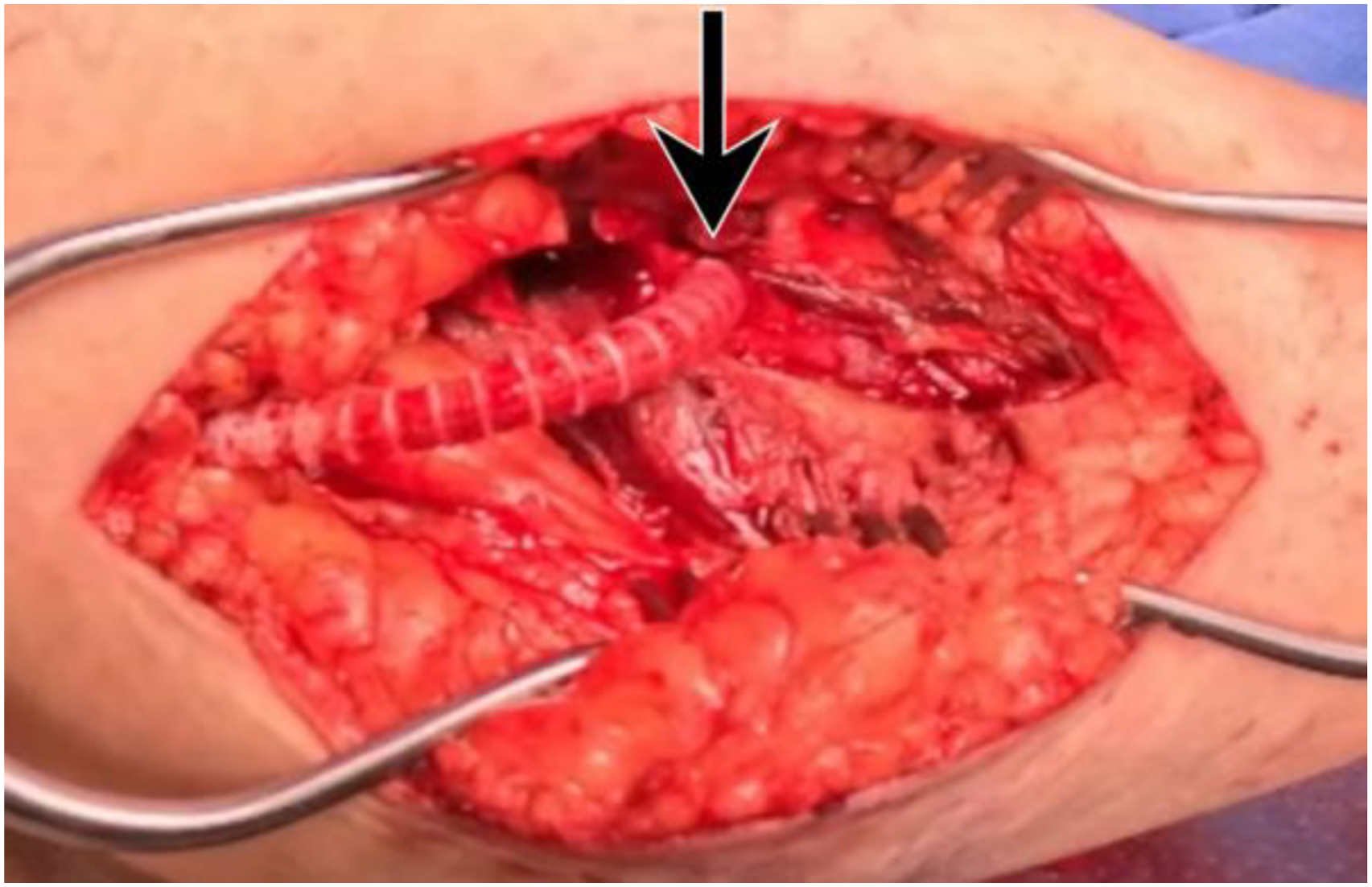
Discussion
The management of ALI in the context of previously failed prosthetic bypass revascularization represents a clinical and surgical challenge. Redo bypass using autologous vein would be the ideal approach due to lower rates of major adverse limb events (MALE) compared to other strategies.6,7 For patients considered unfit for open surgery, endovascular techniques such as catheter-directed thrombolysis, mechanical aspiration thrombectomy, and recanalization of the native artery are safe alternatives; however, they may not be sufficient in this scenario.1,2,8 Hybrid revascularization has emerged as an effective strategy to restore perfusion while reducing morbidity in high-risk patients. 3 Accordingly, the decision to use that approach was primarily driven to avoid the previously explored groin and mitigate the severe wound and cardiorespiratory risks inherent to prolonged operations in the obese population.
To better understand the role of obesity in this scenario, we conducted a literature review in PubMed using the terms: “complications”, “obese”, “obesity”, “BMI”, “infrainguinal bypass”, “lower extremity bypass.” We included only articles in English and we excluded those articles, with a principal diagnosis other than PAD, ALI or critical limb threatening ischemia. We included 9 studies for the review as described in Figure 4. PRISMA flow diagram of literature search specifically looking for complications due to obesity following lower extremity bypass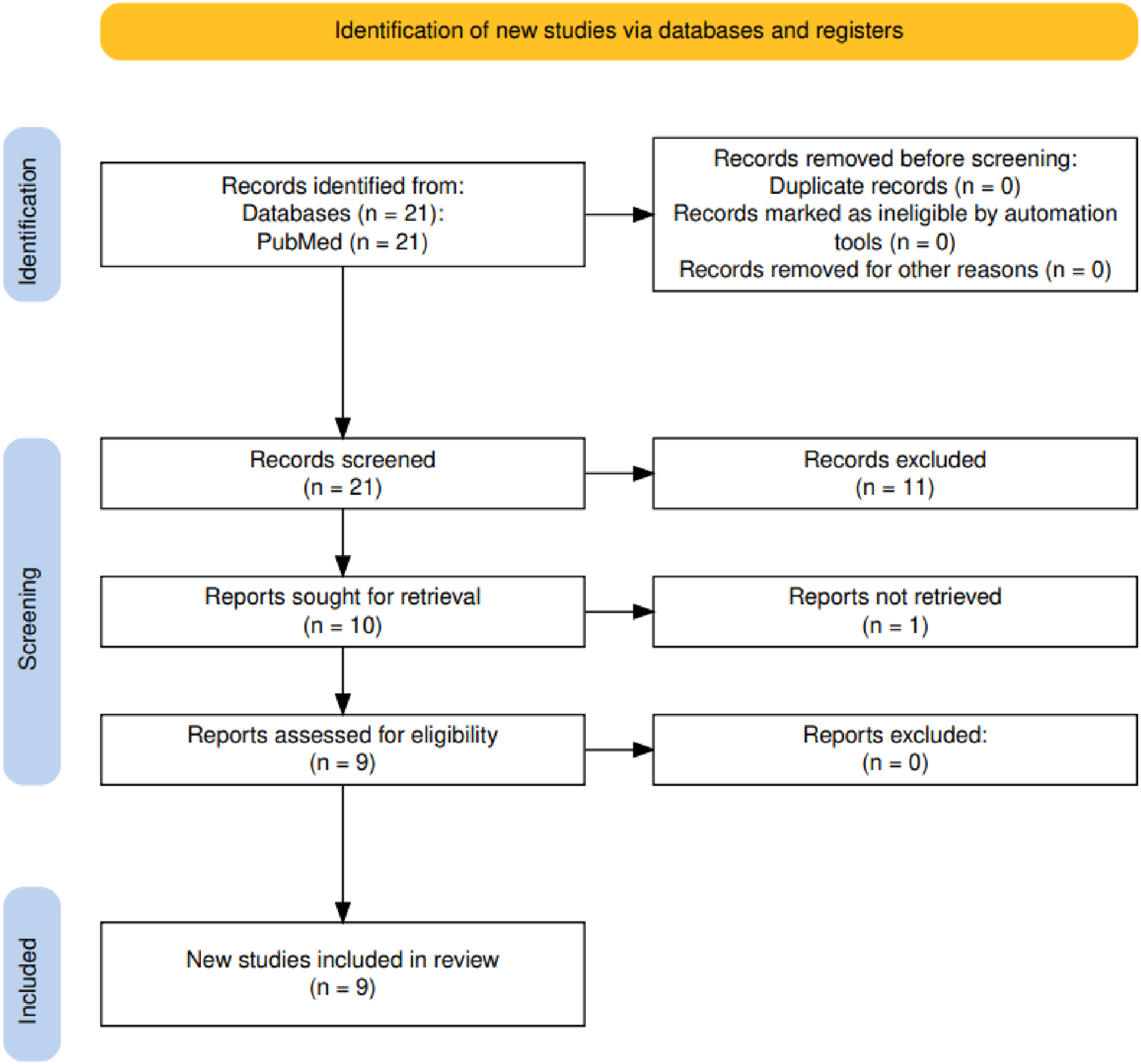
Manuscripts Depicting Complications of Obesity in Infrainguinal Bypass Surgery
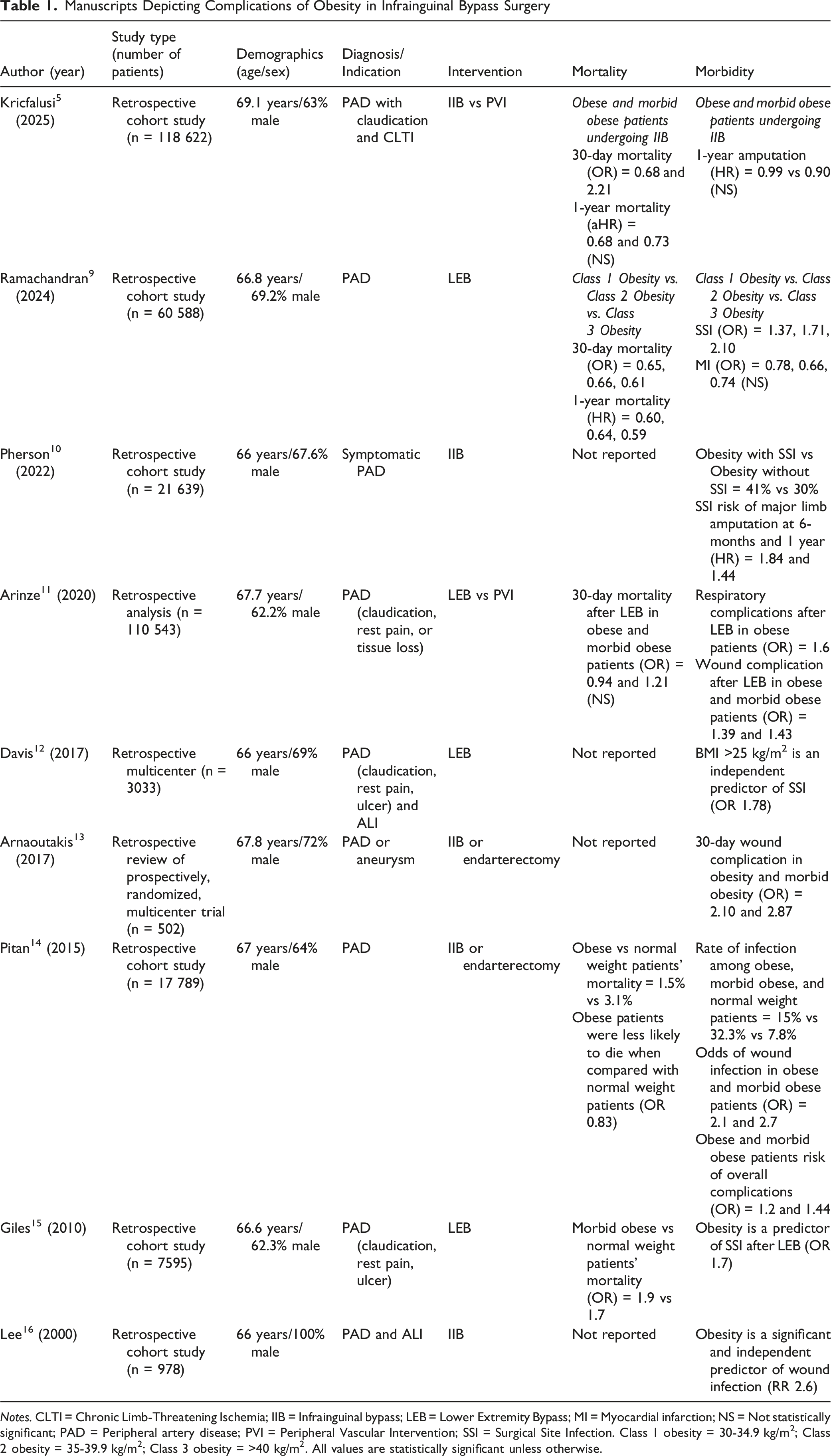
Notes. CLTI = Chronic Limb-Threatening Ischemia; IIB = Infrainguinal bypass; LEB = Lower Extremity Bypass; MI = Myocardial infarction; NS = Not statistically significant; PAD = Peripheral artery disease; PVI = Peripheral Vascular Intervention; SSI = Surgical Site Infection. Class 1 obesity = 30-34.9 kg/m2; Class 2 obesity = 35-39.9 kg/m2; Class 3 obesity = >40 kg/m2. All values are statistically significant unless otherwise.
In reference to the endovascular technique employed, relining of an occluded prosthetic conduit is a viable alternative to graft explantation or redo femoral anastomosis, especially with the premise of avoiding groin re-exploration.3,12,13 Consequently, we performed a PTFE-in-PTFE reconstruction via retrograde access to the left common femoral artery through the previously occluded PTFE graft. The deployment of a Viabahn stent (Gore, Flagstaff, AZ) allowed us to trap chronic thrombus and atherosclerotic plaque between the new endoprosthesis and the old graft, while the balloon angioplasty ensured adequate graft expansion and wall apposition. 18
Regarding conduit selection, the great saphenous vein is often unavailable in redo surgeries, as it was for this case, appearing in only approximately 25% to 40% of patients in certain cohorts.6,19,20 In the absence of an adequate vein, prosthetic alternatives such as PTFE are an inferior but acceptable option with a long-term primary patency close to 65% in infragenicular zones.6,21 Nevertheless, the abrupt transition between a PTFE to a native artery promotes neointimal hyperplasia and contributes to graft failure due to wall shear stress and focal turbulence at the distal anastomosis. To overcome this compliance mismatch, a Linton patch is often utilized. 22 Registries and cohort studies support using a distal vein adjunct since it is associated with significantly improved primary assisted patency and reduced MALE compared to direct prosthetic anastomosis.19,23
Kukulski et al supports that hybrid revascularization strategies have a technical success rate of approximately 88.5%. 24 In terms of patency, for this type of approach that uses a PTFE graft and Linton patch, some studies have found a primary and secondary patency of 54% and 66% at 5 years. 25 Despite a limited primary patency, hybrid strategies achieve reasonable limb preservation, with an amputation-free survival of 68.5% at 1 year and 48.2% at 3 years. 24 Notably, wound complications are reduced compared with open groin re-exploration, with SSI reported in approximately 3.9% of hybrid cases.11,24 Relating to mortality, some cohorts report a 30-day mortality near 0%, while broader multilevel hybrid reconstructions described early mortality ranging from approximately 1.2% to 6.7%. 24
Conclusion
ALI is particularly challenging in morbidly obese patients with prior bypass surgery, considering the higher odds of mortality, surgical site infections, respiratory complications, and major limb amputation. In this setting, hybrid lower extremity revascularization is an alternative revascularization procedure that provides limb reperfusion while avoiding groin re-exploration in a previously exposed femoral artery.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
The patient provided informed consent for participation.
Consent for Publication
The patient provided consent for the publication of this case report.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are not publicly available due to patient privacy and ethical restrictions. No datasets were generated or analyzed beyond those presented in this article.