
Abstract
Introduction
Aortocaval fistula (ACF) is a rare complication of abdominal aortic aneurysm (AAA), involving less than 1% of all AAA and about 3% of ruptured aortic aneurysms.
The conventional management of aortocaval fistula involved an open surgical approach, burdened by high mortality rates, while the endovascular repair has progressively become the mainstay of the vascular treatment.
Case Report
A 73-year-old male patient presented to the emergency room with acute respiratory failure and signs of heart failure. A computed tomography angiography (CTA) demonstrated the presence of a 10 cm AAA, with a spontaneous rupture into the adjacent inferior vena cava (IVC). A bifurcated aortic endograft was therefore successfully deployed to exclude the ruptured AAA, with an immediate resolution of symptoms and an improvement in hemodynamic parameters. Nevertheless, a type IA endoleak was detected at a post-operative control CTA: its perfusion was sustained by communication with the IVC. A secondary intervention was deemed necessary, including both the proximal sealing fixation and the fistula closure. The aneurysmal sac was embolized with coils passing through the ACF, then, after performing the Intravascular Lithotripsy (IVL) of the right iliac axis, the Heli-FX EndoAnchor ® system was advanced and used to fix the proximal sealing zone, with a good angiographic and long-term, post-operative result.
Conclusion
The endovascular treatment of ruptured AAA with ACF has proven to have lower morbidity and mortality than the surgical treatment. Numerous endovascular treatments have been used to treat aortocaval fistula: in the present case, the choice was dictated by the need to occlude the aneurysmal sac and to seal the type Ia endoleak in the same intervention. The combination of the aneurysmal sac embolization passing through the IVC and the Heli-FX EndoAnchor ® system seems to be a safe alternative in ruptured AAA with ACF.
Introduction
The aortocaval fistula (ACF) is a rare complication of an abdominal aortic aneurysm (AAA), involving less than 1% of all AAA and about 3% of ruptured aortic aneurysms (rAAA).1,2
The presentation can be atypical, leading to a delayed diagnosis: clinical features include syncope, hypotension, high-output cardiac failure, bilateral pedal edema, renal insufficiency and continuous bruit in the abdominal region. 2
The conventional management of ACF has historically involved an open surgical approach, burdened by perioperative mortality rates of up to 60%, due to massive blood loss during surgery, pulmonary embolic events, and cardiac complications. 3
Nowadays, endovascular aneurysm repair (EVAR) has progressively become the mainstay of vascular interventions, including in this field of application. 4 However, a secondary intervention may be needed to cope with any complications developing after the first procedure. We report the case of a patient treated via endovascular approach for an AAA associated with an ACF, which developed a type IA endoleak sustained by blood flow in the Inferior Vena Cava (IVC), through the ACF, requiring a secondary intervention.
Case Report
A 73-year-old male patient presented to the emergency department with acute respiratory failure with signs of heart failure, associated with lower back pain, asthenia and hypotension.
The abdominal examination showed an abdominal mass with a continuous vascular bruit, and for this reason the patient a computed tomography angiography (CTA) was performed. This demonstrated the presence of an AAA with a maximum diameter of 10 cm, with a spontaneous rupture into the adjacent inferior vena cava (IVC). The CTA revealed an angulated and reverse-tapered neck, with circumferential thrombosis, and the presence of a calcified small iliac access bilaterally (Figure 1). The patient was deemed unfit for the open surgery repair due to the respiratory and cardiac status, so the patient was submitted to EVAR as a matter of urgency. Under local anesthesia, bilateral femoral percutaneous access was performed and then a low-profile, bifurcated aortic endograft (Cordis INCRAFT) was deployed successfully to seal the ruptured AAA (rAAA). After the graft deployment, the patient’s dyspnea immediately resolved and the hemodynamic parameters improved. The final angiography showed the exclusion of the aneurysmal sac, in the absence of any signs of endoleak. Preoperative CTA demonstrated a large aneurysm associated with an aortocaval fistula, with opacification of the inferior vena cava in the arterial phase, as shown in the longitudinal view (A), 3D multiplanar reconstruction (B), and axial view (C)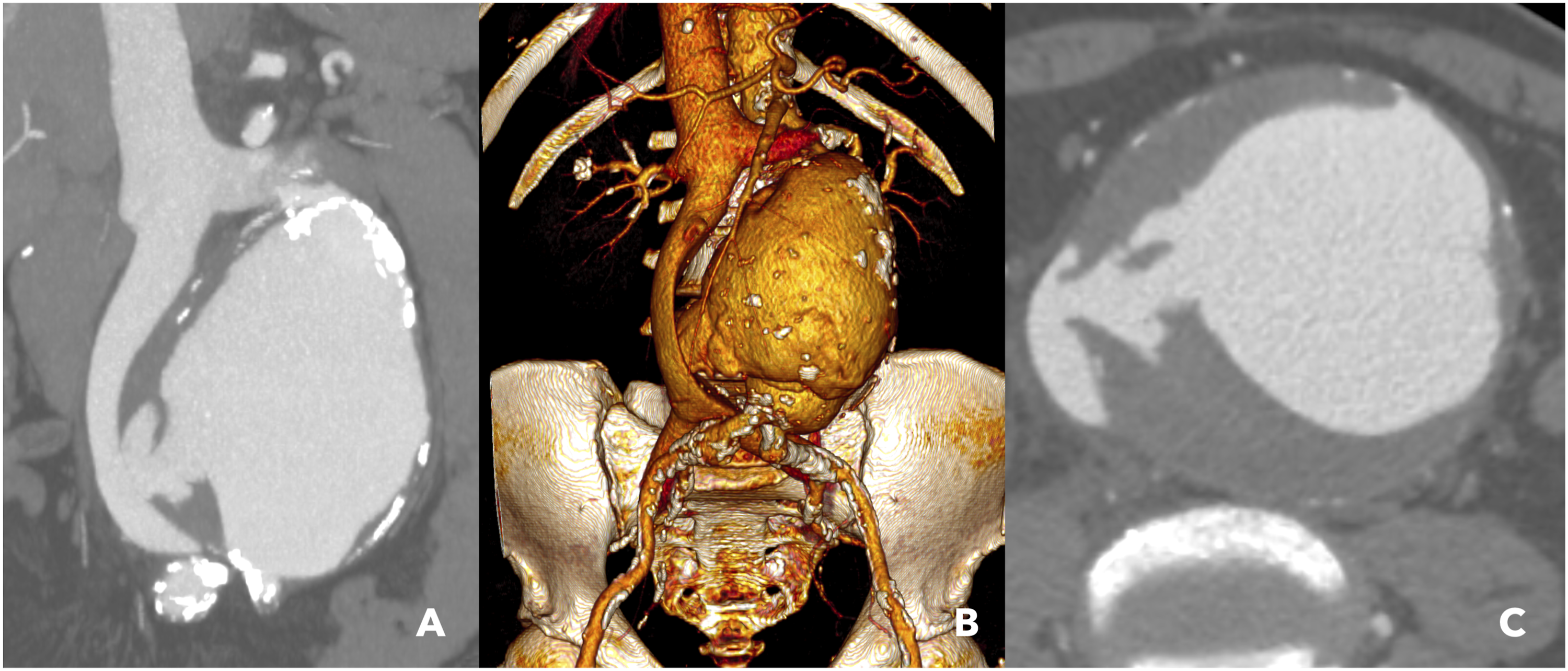
However, a post-operative CTA was performed as the standard protocol for rAAA, which showed the graft patency, with a type IA endoleak, sustained by the communication with the IVC. A secondary intervention was deemed necessary, including both the proximal sealing fixation and the ACF closure. (Figure 2). Postoperative CTA showed patency of the bifurcated endoprosthesis; however, a type IA endoleak was detected in both the longitudinal (A) and sagittal views (B), sustained by communication with the inferior vena cava, as demonstrated in the axial view (C)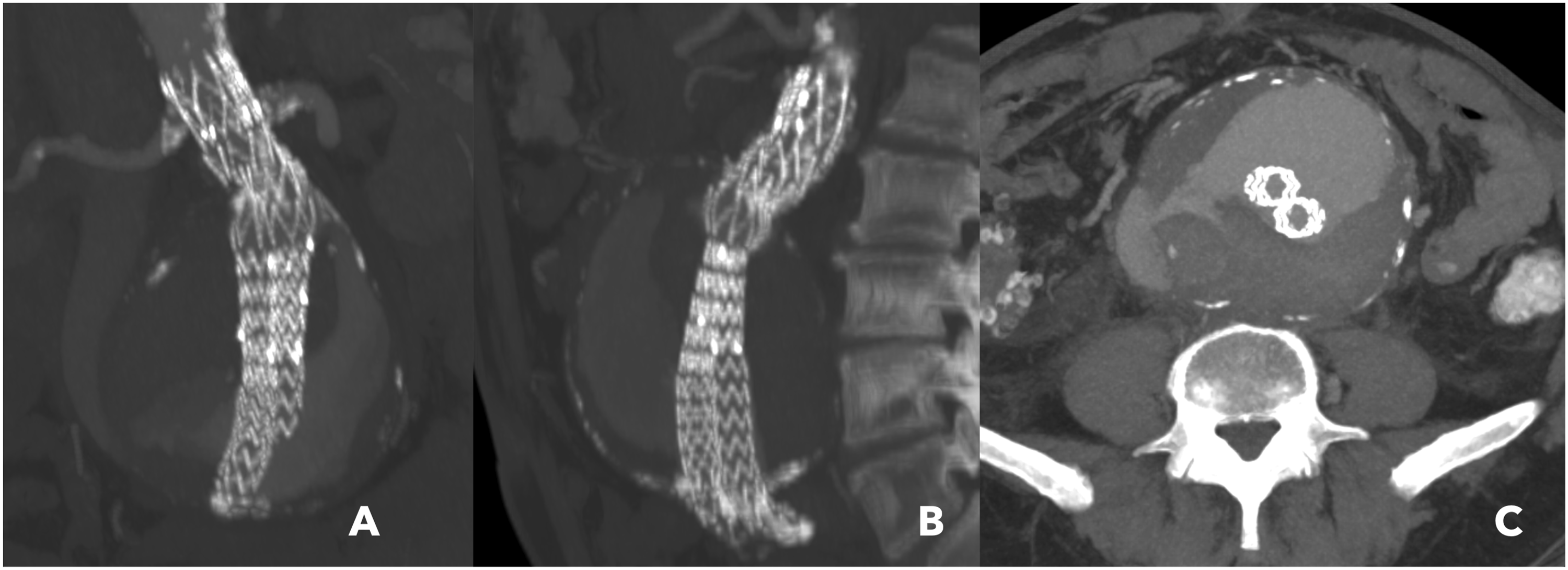
Under local anesthesia, a left common femoral vein access was therefore performed and the ACF was cannulated to reach the aneurysmal sac. The aneurysmal portion near the ACF was then embolized with Penumbra Ruby standard detachable coils, to reduce the outflow through the IVC. The post-embolization angiography showed the persistency of the endoleak, despite outflow reduction (Figure 3). Completion angiography after embolization with Penumbra Ruby coils showed reduced outflow through the IVC, with persistence of the endoleak
Then, after performing the Intravascular Lithotripsy (IVL) of the narrow and calcified right iliac axis to improve vessel compliance, the Heli-FX EndoAnchor ® system (Medtronic; Minneapolis, Minnesota, USA) was advanced and used to fix the proximal sealing zone: eight anchor screws were deployed, achieving a satisfactory angiographic result (Figure 4). Completion angiography following deployment of eight Heli-FX EndoAnchors (Medtronic; Minneapolis, Minnesota, USA) demonstrated a satisfactory angiographic result, with no evidence of endoleak
The post-operative course was uneventful, and the CTA performed 4 days after reintervention showed the resolution of both the ACF and the endoleak.
The patient was discharged in good clinical conditions. The last follow-up CTA at 4 years showed the aneurysmal sac shrinkage and the complete resolution of the ACF (Figure 5). Postoperative CTA demonstrated complete resolution of both the aortocaval fistula and the endoleak (A, C), whereas the 4-year follow-up CTA demonstrated a significant shrinkage of the aneurysmal sac (B, D)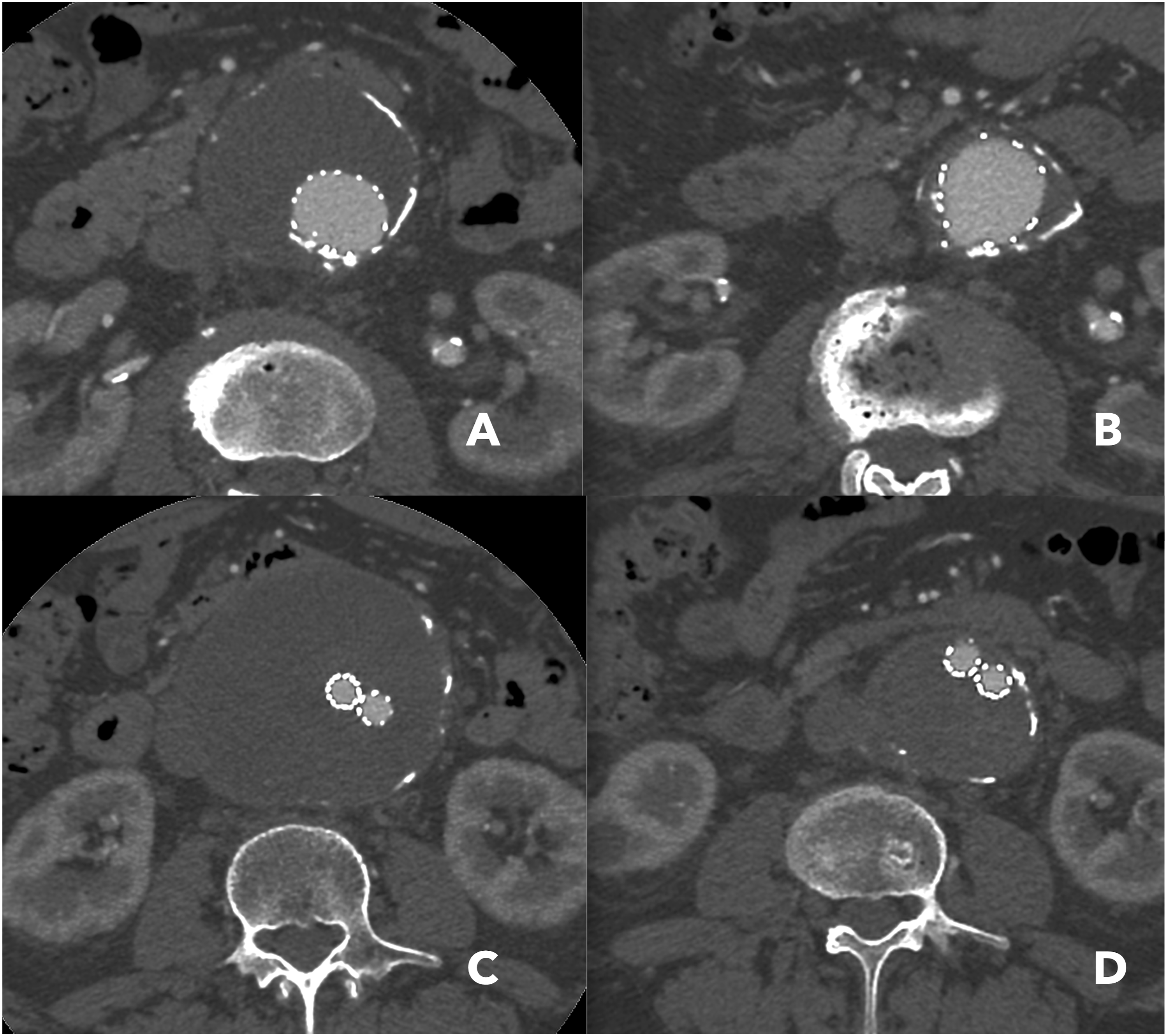
Discussion
The first case of ACF was described by Syme 5 in 1831, while DeBakey, Cooley and colleagues 6 reported the first successful surgical repair of an ACF complicating an AAA in 1958. The open surgery approach, consisting of the direct suturing of the fistula from within the aneurismal sac followed by aortic reconstruction, is burdened by high mortality and morbidity rates.
In fact, in a systematic review by Calligaro et al. 7 the 30-day survival rate was 72%, with a mortality of 30% even in semi-elective cases. With the endovascular advancement, Woolley 8 in 1995 reported the first case of aortic exclusion used in the management of an ACF, and the endovascular repair has proven to be a solid option, particularly in high risk patients, as reported by Beveridge et al, 9 as well as by Gandini et al and Ascoli Marchetti et al.10,11
The mortality in the endovascular treatment is lower than after open surgery, with a documented mortality rate of 12% and of 3.8% respectively, documented by Orion et al. 4
The hostile neck anatomy can lead to further adjunctive procedures to achieve proximal sealing 12 and can lead to the development of a Type Ia endoleak.13,14
In the case reported, the patient developed an early type Ia endoleak after EVAR, and it was decided to use EndoAnchors to correct it. EndoAnchors were approved for commercial use in 2011 and are now firmly established as a prophylactic tool for obtaining a proximal seal both during the index EVAR and as a rescue tool.14-16 The primary indication is to secure the proximal or distal landing zones in hostile necks, intraoperative endoleaks, or inadequate apposition to the aortic wall. Gaffey et al 17 has reported a technical success of 90-100% and a freedom from recurrent endoleak of 95-97% after EndoAnchors were used to treat type Ia endoleaks. 18
Numerous endovascular treatments have been used to treat ACF, from the direct aortic stent graft coverage of the inflow orifice to orifice embolization with Amplatzer Occluder. 19
The choice in the present case was dictated by the need to occlude the aneurysmal sac and to seal the type Ia endoleak with EndoAnchors.20,21
Conclusion
The endovascular treatment of rAAA with ACF has proven to have lower morbidity and mortality than the surgical treatment.
However, the presence of an ACF can replenish the aneurysmal sac and, also in association with hostile necks, could lead to further aortic procedures. In this particular case, the embolization of the aneurysmal sac from the aortocaval fistula and the proximal fixation led to sac shrinkage after 4 years.
Footnotes
Consent for Publication
The patient has signed an informed consent form for the procedure and the publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.