
Abstract
This study examines caregivers’ perceptions of participation patterns and environmental supports and barriers for young children with and without developmental disabilities within their child care/preschool and community settings. The Young Children’s Participation and Environment Measure (YC-PEM) was completed by 151 parents of Singaporean children (0-7 years old) with and without developmental disabilities. Setting-specific summary and item-level scores of these children were compared using ANCOVA, Mann–Whitney U, and Pearson chi-square tests. Children with developmental disabilities had significantly lower participation and environment summary scores in both settings as compared with children without developmental disabilities (p < .05;
Introduction
Childhood occupations are culturally valued activities and tasks that young children do to occupy themselves, including self-care, leisure, and educational activities. Participation in occupations are means to achieve the positive development of young children (Dunst, Hamby, Trivette, Raab, & Bruder, 2002; R. W. Larson & Verma, 1999; Law, 2002) and are influenced by the interactions between a persons’ health condition and contextual factors (UNICEF, 2013; World Health Organization [WHO], 2001). The development and use of the WHO’s International Classification of Functioning, Disability and Health for Children and Youth (ICF-CY) has led to increasing emphasis on participation and environment and efforts to develop instruments to measure these important constructs in children (WHO, 2007). Assessing participation at the same time as environment can increase our understanding of the environmental factors that influence young children’s participation in specific settings (Khetani, Graham, & Alvord, 2013). With this understanding, early intervention providers can consider the full range of factors that might impact participation problems in a specific setting (Simeonsson, 1991).
While young children typically participate in occupations at home, at child care or preschool, and in the community, how their time use is allocated across settings can vary across cultures and over time (Dunst et al., 2002; R. W. Larson & Verma, 1999). In Singapore, a country that relies on human resources for economic development (Ng, 2011), government policies have been implemented to encourage women to continue to be in the workforce after they have children (Quek, Knudson-Martin, Orpen, & Victor, 2011). These policies have led to the growth of alternative child care arrangements such as child care and preschool facilities (Honig & Lim, 1998). Young Singaporean children thus spend more time in child care/preschool and the community than in their homes at a young age. This social phenomenon is also common in America where young children are spending more time in day care than at home due to work commitments of their parents (ChildStats, 2014). In addition, transport networks are increasingly accessible and children are able to travel out of home into the community. In child care/preschool, children can participate in a variety of activities like group learning and socialization with peers. In the community, examples of participation range from running errands with their parents to playing in the park.
Despite the significant amount of time that young children spend in out-of-home environments, research suggests that young children with developmental disabilities participate less frequently and in a smaller variety of activities in comparison with children without developmental disabilities (LaVesser & Berg, 2011; Leung, Chan, Chung, & Pang, 2011). Among American preschoolers with developmental disabilities, 39.3% were reported to experience community participation difficulty in at least one activity (Khetani et al., 2013). LaVesser and Berg (2011) found that parents of preschoolers with autism spectrum disorder provided them with opportunities to participate in activities, but the children could not capitalize on these opportunities. Participation difficulties have been associated with several factors, including those related to the child (behavioral and social difficulties), the family (income, parental education levels, informal family support, parents’ confidence in managing their child’s behavior), and the environment (social support, transportation; Khetani et al., 2013; Khetani, Orsmond, Cohn, Law, & Coster, 2012; LaVesser & Berg, 2011; Leung et al. 2011; Rosenberg, Ratzon, Jarus, & Bart, 2012; Soref et al., 2012). The community environment may pose more barriers to children’s participation than the home environment, where parents typically have more control to promote participation in occupation (E. A. Larson, 2000; Rosenberg et al., 2012).
There are more studies about the out-of-home participation of children with disabilities aged 6 years and above than about younger children (Raghavendra, 2013). In part, this is due to a lack of instruments to measure both participation and environments of younger children (Law, King, Petrenchik, Kertoy, & Anaby, 2012). There are studies on young children’s participation, but they are limited in the types of diagnoses (LaVesser & Berg, 2011; Rosenberg et al., 2012; Soref et al., 2011) and settings (Khetani et al., 2013; Khetani et al., 2012; Leung et al., 2011), and the majority involve children from North America. Internationally, efforts have been made to ensure optimal participation for children with disabilities. Occupational therapy approaches such context-focused therapy and Occupational Performance Coaching (OPC) have been developed to guide parents to think about the demands of the activities/environment and how to intervene on immediate environmental factors to promote participation outcomes (Darrah et al., 2011; Graham, Rodger, & Ziviani, 2009). Service delivery models such as the Response to Intervention (RtI) Framework and Partnering for Change (P4C) have also been developed to improve participation of school-aged children with disabilities in schools (Cahill, 2010; Missiuna et al., 2012). Appropriate interventions have thus been developed with knowledge about the participation levels of children with disabilities and environmental influences on their participation.
To our knowledge, this is the first study that focuses on participation and environment of children with developmental disabilities in both the child care/preschool and community settings in Singapore. The incidence of developmental disabilities among children younger than 7 years in Singapore was estimated at about 7,000 (or 3.2% of the child population) in 2010 (Enabling Masterplan [EM] 2012-2016 Steering Committee, 2012). Focus groups were conducted with parents of children with developmental disabilities to understand their needs (EM 2012-2016 Steering Committee, 2012). The parents raised concerns such as lack of knowledge, information, resources, and services to support their children and the lack of public awareness and acceptance from society (EM 2012-2016 Steering Committee, 2012). These environmental barriers to inclusion appear to be of pronounced importance to parents and should be understood in greater depth and on a larger scale. With knowledge about the participation levels of young children with disabilities in the Singapore cultural context, interventions can be developed to bridge any potential gaps between the participation of young children with and without disabilities. Therefore, the research questions addressed in this article were as follows:
Method
Recruitment of Participants
In Singapore, children with developmental concerns are referred to one of three government hospitals in Singapore with a child development unit (Lian et al., 2012). The developmental pediatrician assesses the child and refers the child to an Early Intervention Program for Infants and Children (EIPIC) for long-term early intervention services, run by Voluntary Welfare Organisations (VWO). Due to the VWO’s manpower and resource constraints, the children are often placed on a waitlist before enrollment in EIPIC. While waiting, they are provided with interim therapy services at the government hospitals.
For this study, caregivers of children with disabilities were recruited from a government hospital, KK Women’s and Children’s Hospital’s (KK Hospital) Department of Child Development (DCD) and VWOs with EIPIC located at various geographical regions in Singapore. The recruitment period was from July to December 2013. Caregivers of children without disabilities were recruited from government-funded and private kindergartens. The centers that agreed to participate in the study were informed of the participants’ inclusion criteria. They were provided with the questionnaires and consent forms to be given out to participants who met the inclusion criteria and agreed to participate in the study after they have received a letter that introduces the study. Caregivers met the following eligibility criteria: (a) They identified themselves as a parent or legal guardian of the child who is the focus of the survey, (b) they were able to read and write English, (c) their child was between 0 and 7 years old at the time of enrollment, and (d) children with disabilities met the eligibility criteria for enrollment in EIPIC. Children were eligible for EIPIC if they were (a) below 7 years of age; (b) a Singapore citizen or permanent resident; (c) diagnosed with developmental, intellectual, sensory, or physical disabilities, or a combination of disabilities; and (d) recommended for EIPIC by a doctor from one of the three government hospitals in Singapore with a child development unit (SG Enable, 2015).
The Young Children’s Participation and Environment Measure (YC-PEM; Singapore; C. Y. Lim, Law, Khetani, Pollock, & Rosenbaum, 2015) was disseminated to 200 caregivers of young children with (n = 100) and without (n = 100) disabilities. The YC-PEM was completed by 151 parents of children with (n = 83) and without (n = 68) disabilities in Singapore (Table 1). The demographic characteristics of both groups of parents were similar except for employment characteristics and annual income: 91% of parents of typically developing children were working full-time (n = 62) while 59% of parents of children with disabilities were working full-time (n = 49). Parents of children without disabilities had higher income levels than parents of children with disabilities. Among children with disabilities, 81 (98%) attended EIPIC and/or child care/preschool while 61 (90%) typically developing children attended child care/preschool, indicating that majority of the whole sample spent time in out-of-home environments. Among children with disabilities, 36 (43%) had developmental/intellectual delay and 19 (23%) had emotional/behavioral difficulty. There were none with physical or sensory disabilities. Therefore, children with disabilities are collectively referred to as having developmental disabilities.
Respondent and Child Characteristics.
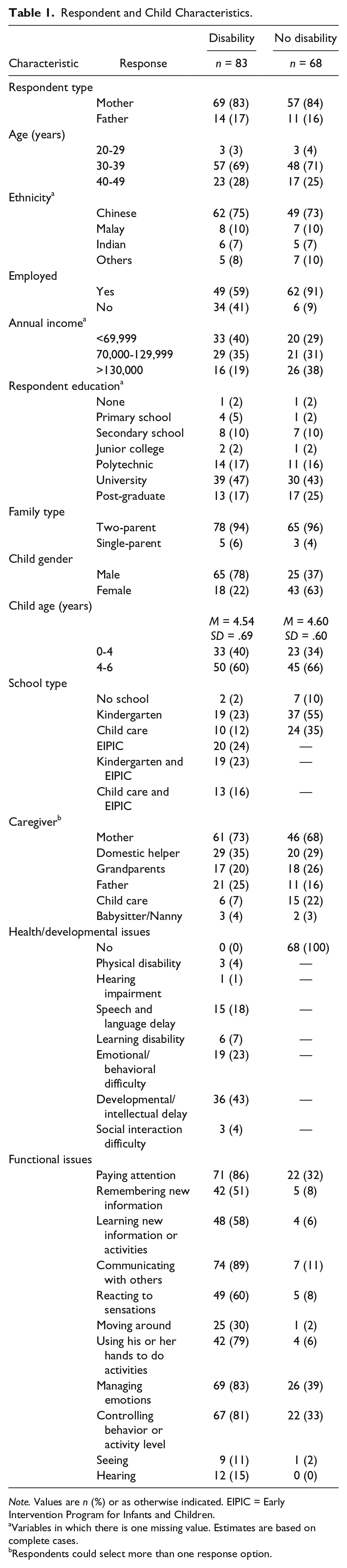
Note. Values are n (%) or as otherwise indicated. EIPIC = Early Intervention Program for Infants and Children.
Variables in which there is one missing value. Estimates are based on complete cases.
Respondents could select more than one response option.
Measures
Researchers in North America developed the YC-PEM to address the need for instruments that measure both participation and environment of young children (Khetani, Cohn, Orsmond, Law, & Coster, 2011; Khetani, Graham, Davies, Law, & Simeonsson, 2015). The YC-PEM was found to have significant associations for all items in all five ICF-CY environmental domains (Khetani et al., 2015). Khetani et al. (2015) used the original North American version of the YC-PEM and found disparities in young children’s out-of-home participation. The YC-PEM has been recently culturally adapted for use in Singapore (C. Y. Lim, Law, Khetani, Pollock, & Rosenbaum, 2015).
The YC-PEM (Singapore) is a caregiver-report questionnaire used as the primary measurement tool in this study to examine the participation patterns of young children with and without developmental disabilities, and the environmental influences on their participation in the child care/preschool and community settings (C. Y. Lim, Law, Khetani, Pollock, & Rosenbaum, 2015). The participants completed paper versions of the YC-PEM (Singapore; C. Y. Lim, Law, Khetani, Pollock, & Rosenbaum, 2015) and a demographic questionnaire. The demographic questionnaire gathered information about the child and family, such as child’s age, main caregivers, developmental issues, and family’s socioeconomic status. The YC-PEM (Singapore) includes 29 items that examine participation and environment at home (14 items), at child care/preschool (three items), and in the community (12 items). We used data only from the child care/preschool and community items for this study. Child care/preschool activities pertain to educational programming in the form of group learning, socializing with friends, and school excursions and events. Caregivers complete the child care/preschool section based on information they received from the child care/preschool teachers. They typically receive information about their children’s child care/preschool participation at the parent–teacher meeting that occurs twice a year. Some caregivers obtain regular updates about their children’s participation in child care/preschool activities through informal conversations with teachers when they send or pick their children up from school. Community activities fall into one of the following categories: (a) excursions and outings, (b) classes and groups, (c) community-sponsored activities, and (d) recreation. For each activity, the parent is asked to identify how frequently (over the past 4 months) the child has participated (8-point scale: never [0] to once or more each day [7]), how involved the child is while participating (5-point scale: not very involved [1] to very involved [5]), and whether the parent would like to see the child’s participation in this type of activity change (no or yes). If the parent desires change, the caregiver is asked to specify the type of change desired (do more often, do less often, be more interactive, be more cooperative, and/or participate in a broader variety of activities). Caregivers are also asked to describe strategies that they have tried to promote the child’s participation in that type of activity.
After completing the participation items for a setting, parents are asked to evaluate the impact of the child’s environment on participation in that setting. They are asked whether certain features of the environment, for example, the physical layout, help or make it harder for the child to participate in activities in that setting (3-point scale: not an issue/usually helps [3] to usually makes harder [1]). The parents are also asked if resources, for example, programs and services, are available and/or adequate to support the child’s participation in that setting (3-point scale: not needed/usually yes [3] to usually no [1]).
The YC-PEM (Singapore) has been shown to be a reliable and valid tool for children with and without developmental disabilities in Singapore (C. Y. Lim, Law, Khetani, Rosenbaum, & Pollock, 2015). Internal consistency ranged from .59 to .92 for participation scales and .73 to .79 for environment scales. Test–retest reliability ranged from .39 to .89 for participation scales and .65 to .80 for environment scales within a 2- to 3-week period. Moderate to large group differences were found in participation and perceived environmental support between disabled and non-disabled groups, supporting the construct validity of the YC-PEM (Singapore). YC-PEM summary scores were calculated for each setting: (a) Frequency was calculated as the average of all ratings within a setting (range = 0-7); (b) Level of Involvement was calculated as the average of all ratings within a setting (range = 1-5); (c) Desire for change was calculated by summing the number of items scored as “yes, change desired,” divided by the total number of items, and multiplied by 100 (range = 0-100); and (d) Environment support was calculated by summing ratings across all environmental features and resources items and dividing by the maximum possible score, and multiplied by 100 (range = 0-100).
Procedures
SingHealth Institutional Review Board and McMaster University Research Ethics Board approved the study prior to participant recruitment and data collection. Letters of invitation were sent to the people in charge of KK Hospital, EIPIC, kindergartens, child cares, and infant cares to invite them to participate in the study. Interested centers were informed of the eligibility criteria for the parents to participate in this study. Individually packed envelopes containing a participant information sheet, consent form, family background questionnaire, and YC-PEM form were given to the person in charge of the center who disseminated them to eligible parents in their center who agreed to participate in the study. All participants were given a SGD$5 shopping voucher upon return of each completed YC-PEM form to the project office.
Data Analysis
Data were entered into IBM SPSS 22.0 for analyses. Descriptive statistics were used to describe characteristics of study participants. Radar plots are effective in illustrating the interaction among variables related to participation (Mallinson & Hammel, 2010), and were used to explore the relationship between the disability and non-disability groups, and environmental supports/barriers to participation. Data were screened for normality by visual inspection (histogram and Q-Q plot). Parametric tests were used when the data were normally distributed and the variance was tested to be equal. Otherwise, non-parametric tests were used. ANOVAs were used to compare group differences on variables (family income, age, and gender) to determine potential covariates based on findings from previous literature (Coster et al., 2011; Khetani et al., 2013; Khetani et al., 2015; King et al., 2007; Law et al., 2012). Age and gender of children were identified as covariates. Several studies have indicated family income as a potential covariate with mixed conclusions (Khetani et al., 2013; Khetani et al., 2015; Law et al., 2012; Law, King, et al., 2006). In this study, one-way ANOVAs did not indicate income as a covariate, and therefore, it was not controlled for in further analyses.
For item-level analyses, (a) ANCOVA (adjusting for age and gender category) and partial eta squares were used to compare mean item-level responses for participation frequency, and (b) Mann–Whitney U test was used to compare median item-level scores for participation involvement between children with and without developmental disabilities. Pearson chi-square analyses were used to compare the percentage of respondents in each group who responded (a) “never participates” for participation frequency items; (b) “yes” for desired change items; (c) “usually makes harder,” and “not an issue/usually helps,” to environmental support and barrier items; and (d) “usually, no” and “not needed/usually yes” to availability/adequacy of resources items. To reduce Type I error due to multiple comparisons, Bonferroni adjustments were made to significance levels by dividing .05 by the number of comparison tests conducted for each set of analyses. This resulted in a p value of <.01 and <.006 for child care/preschool participation and environment items, respectively, and <.004 and <.007 for community participation and environment items, respectively. For analysis of summary scores, ANCOVAs were used to control for age and gender while comparing child care/preschool and community summary scores of participation frequency, extent of involvement, change desired and environmental support between children with and without developmental disabilities. Partial eta squares (
Results
Frequency Item-Level Responses
Tables 2 and 3 include results that describe and compare participation at the item level for children with and without developmental disabilities in the child care/preschool and community environment. Among children with developmental disabilities, 15 (18.1%) never participated in school excursions and events while all children without developmental disabilities did. The mean participation frequency of children with developmental disabilities in school excursion and events was also significantly lower than typically developing children. Among children with developmental disabilities, 42 (50.6%) never participated in enrichment classes compared with 18 (26.5%) typically developing children. For child care/preschool participation frequency, there were similarities in group learning and socializing with friends between children with and without disabilities but not involvement and parental desire for change. For community participation frequency, there were similarities in all activities except for organized physical activities.
Differences in Child Care/Preschool Participation Items.
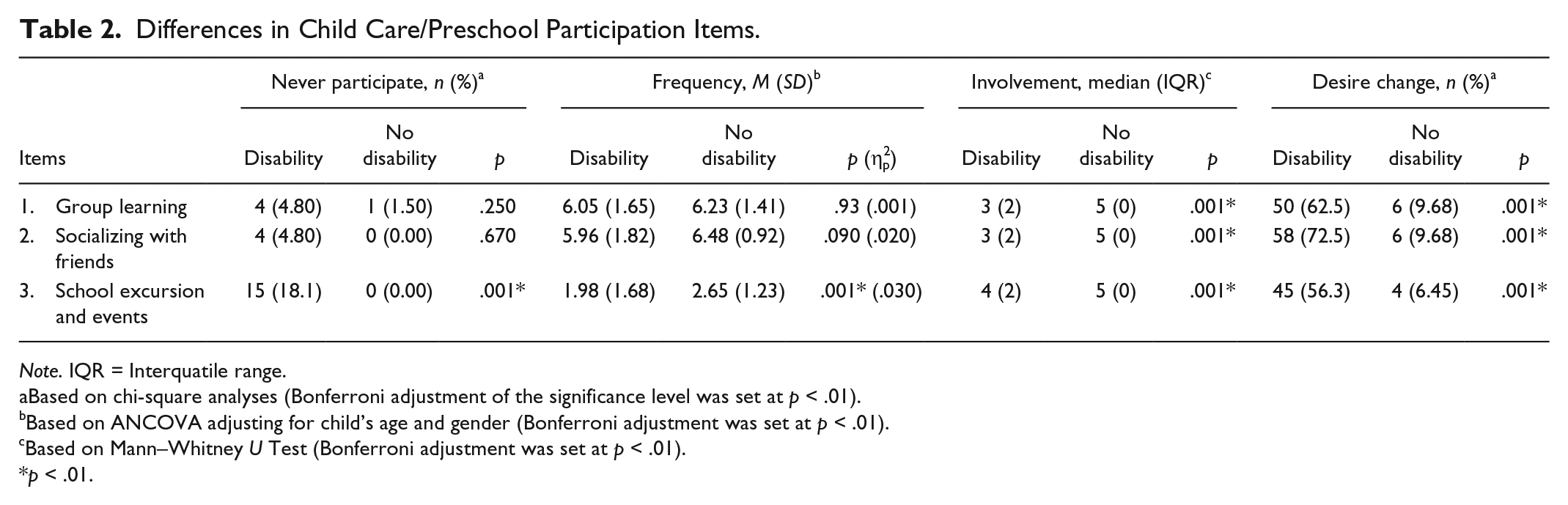
Note. IQR = Interquatile range.
Based on chi-square analyses (Bonferroni adjustment of the significance level was set at p < .01).
Based on ANCOVA adjusting for child’s age and gender (Bonferroni adjustment was set at p < .01).
Based on Mann–Whitney U Test (Bonferroni adjustment was set at p < .01).
p < .01.
Differences in Community Participation Items.
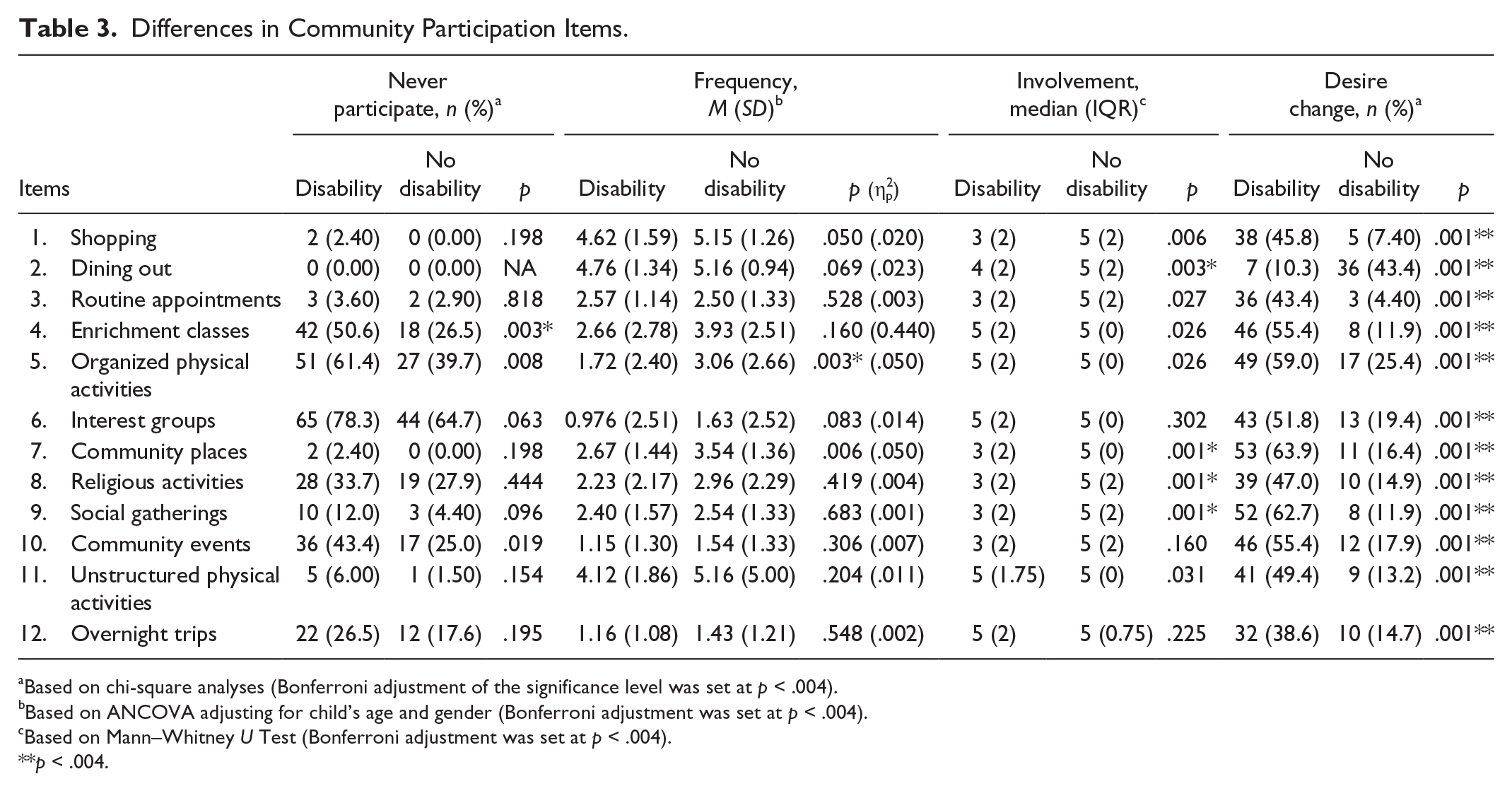
Based on chi-square analyses (Bonferroni adjustment of the significance level was set at p < .004).
Based on ANCOVA adjusting for child’s age and gender (Bonferroni adjustment was set at p < .004).
Based on Mann–Whitney U Test (Bonferroni adjustment was set at p < .004).
p < .004.
Involvement Item-Level Responses
Children with developmental disabilities had significantly lower median involvement scores for group learning, socializing with friends, and school excursions and events when compared with children without developmental disabilities. Despite similarities in how often their children participate in community activities, children with developmental disabilities were less involved in some activities including dining out, community places, religious activities, and social gatherings but not for the rest of the community items.
Change Desired Item-Level Responses
Parents of children with developmental disabilities desired more change in their children’s child care/preschool and community participation in all areas in comparison with parents of children without developmental disabilities.
Perceived Environmental Support/Barrier Item-Level Responses
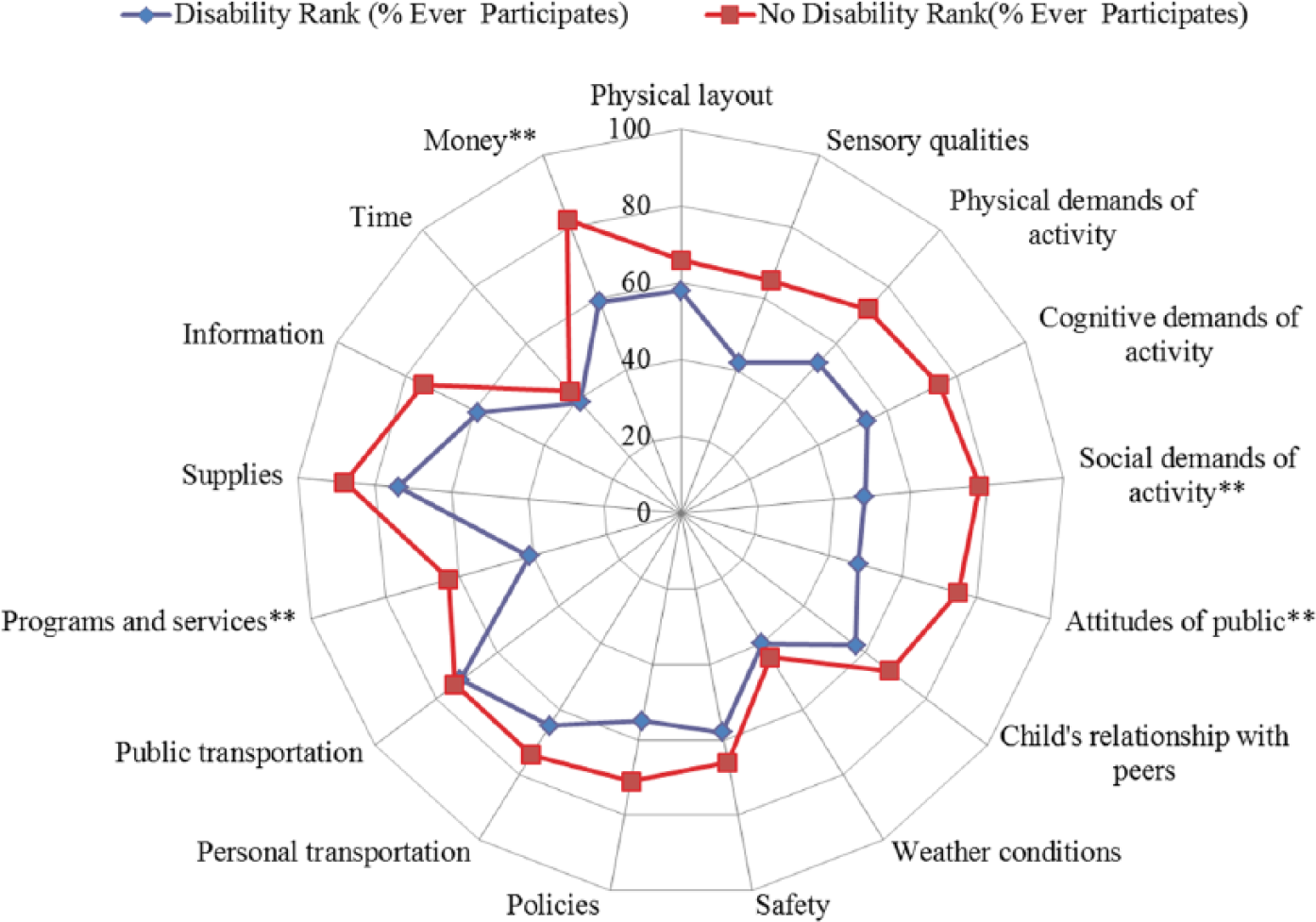
Figures 1 to 4 illustrate the percentages of parents who perceived the item as an environmental support or barrier to child care/preschool and community participation. Results for availability/adequacy of resources items (e.g., policies/procedures, access to personal/public transportation, programs and services, supplies, information, sufficient time, and money) are reported with environmental support/barrier items. There were no significant differences between groups for most of the child care/preschool and community environmental support and barrier item scores. Parents perceived the child care/preschool and community environments as having more supports (“usually helps”) than barriers (“usually makes harder”). In the child care/preschool setting, significantly fewer parents of children with developmental disabilities perceived their child’s relationships with their peers and money as environmental supports. In the community setting, significantly fewer parents of children with developmental disabilities perceived the social demands of activity, attitude of the public, availability of programs and services, and money as an environmental support to community-based participation when compared with parents of children without developmental disabilities.
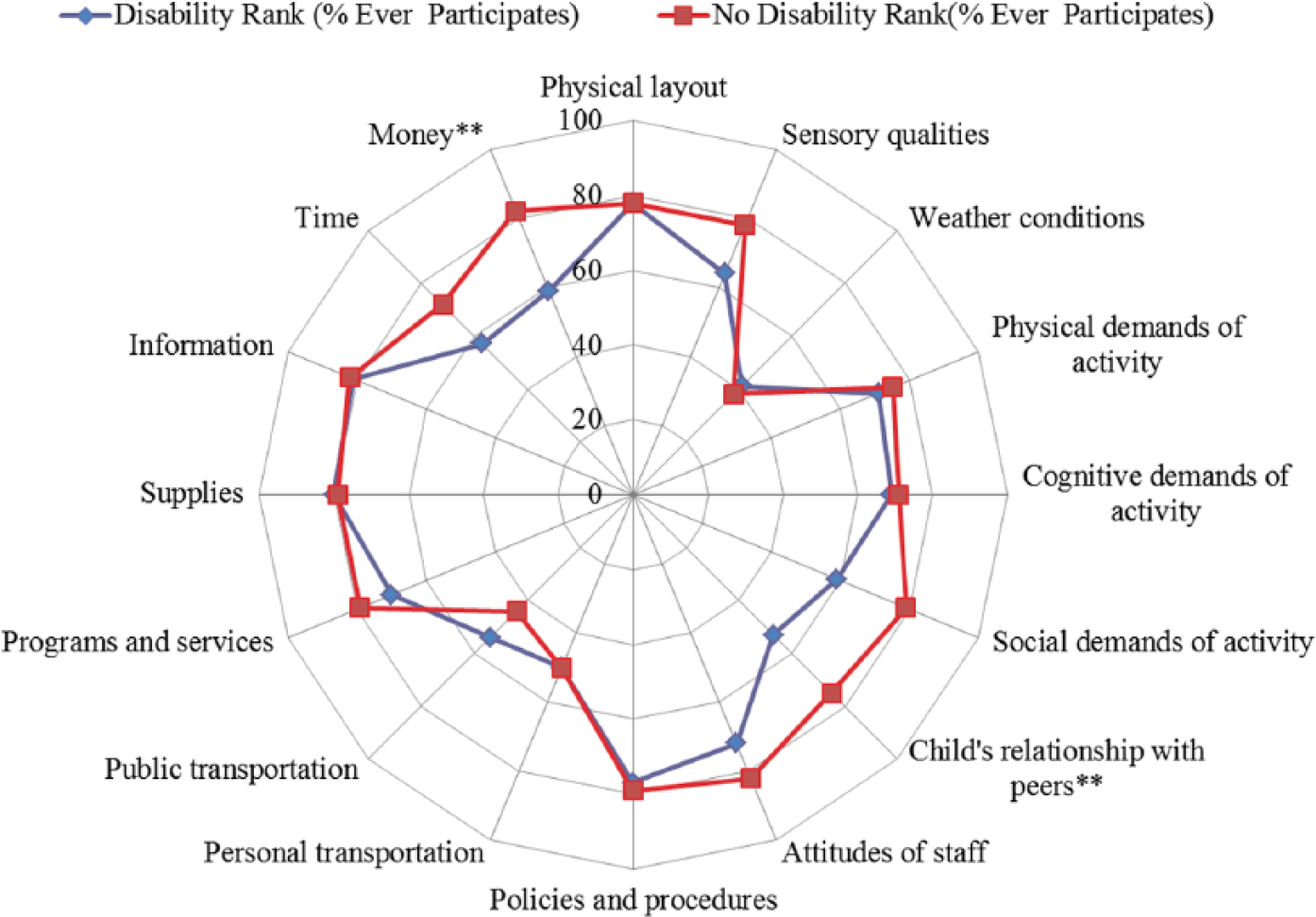
Percentage of parents who perceived the item as a support to child care/preschool-based participation.
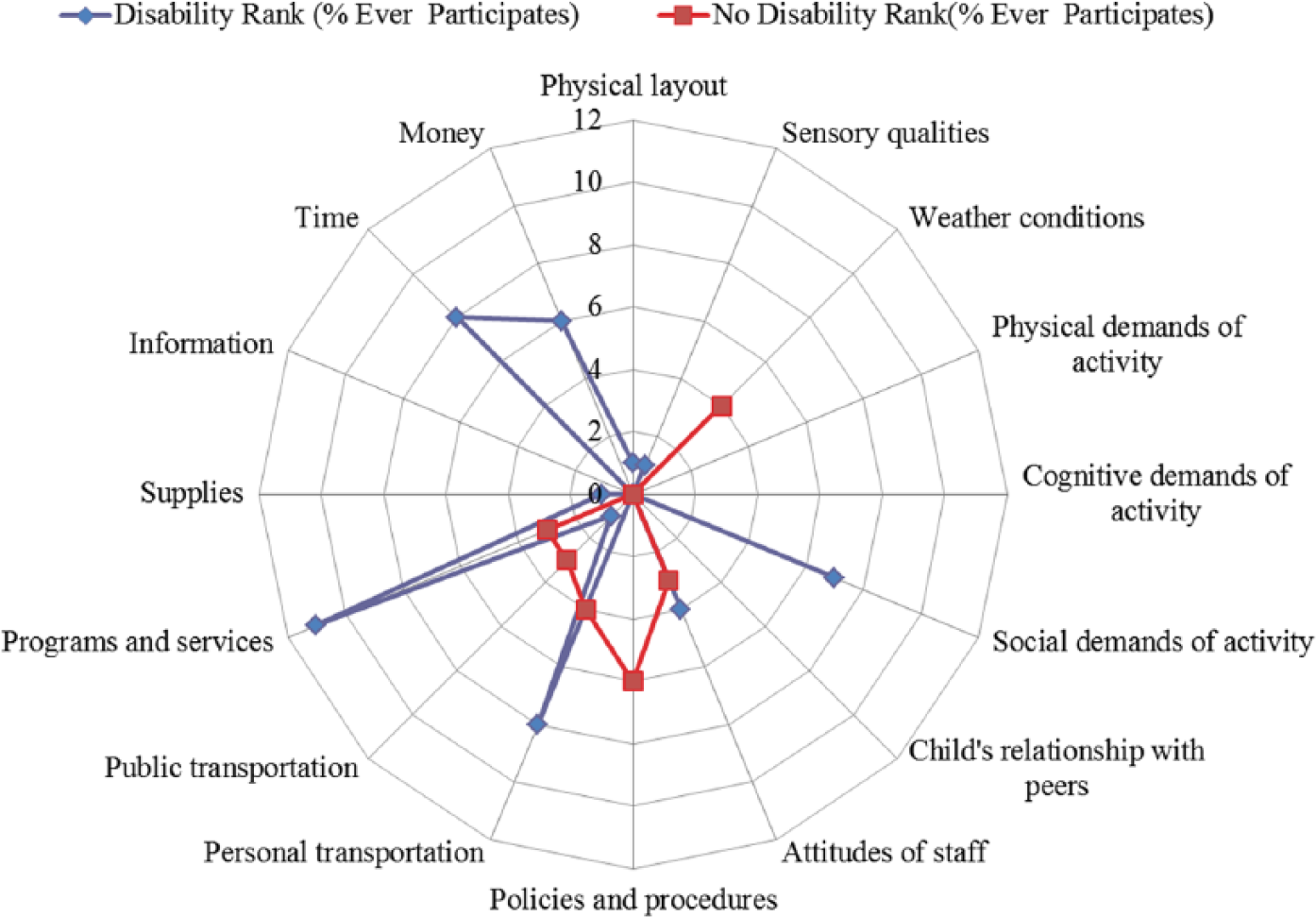
Percentage of parents who perceived the item as a barrier to child care/preschool-based participation.
Percentage of parents who perceived the item as a support to community-based participation.
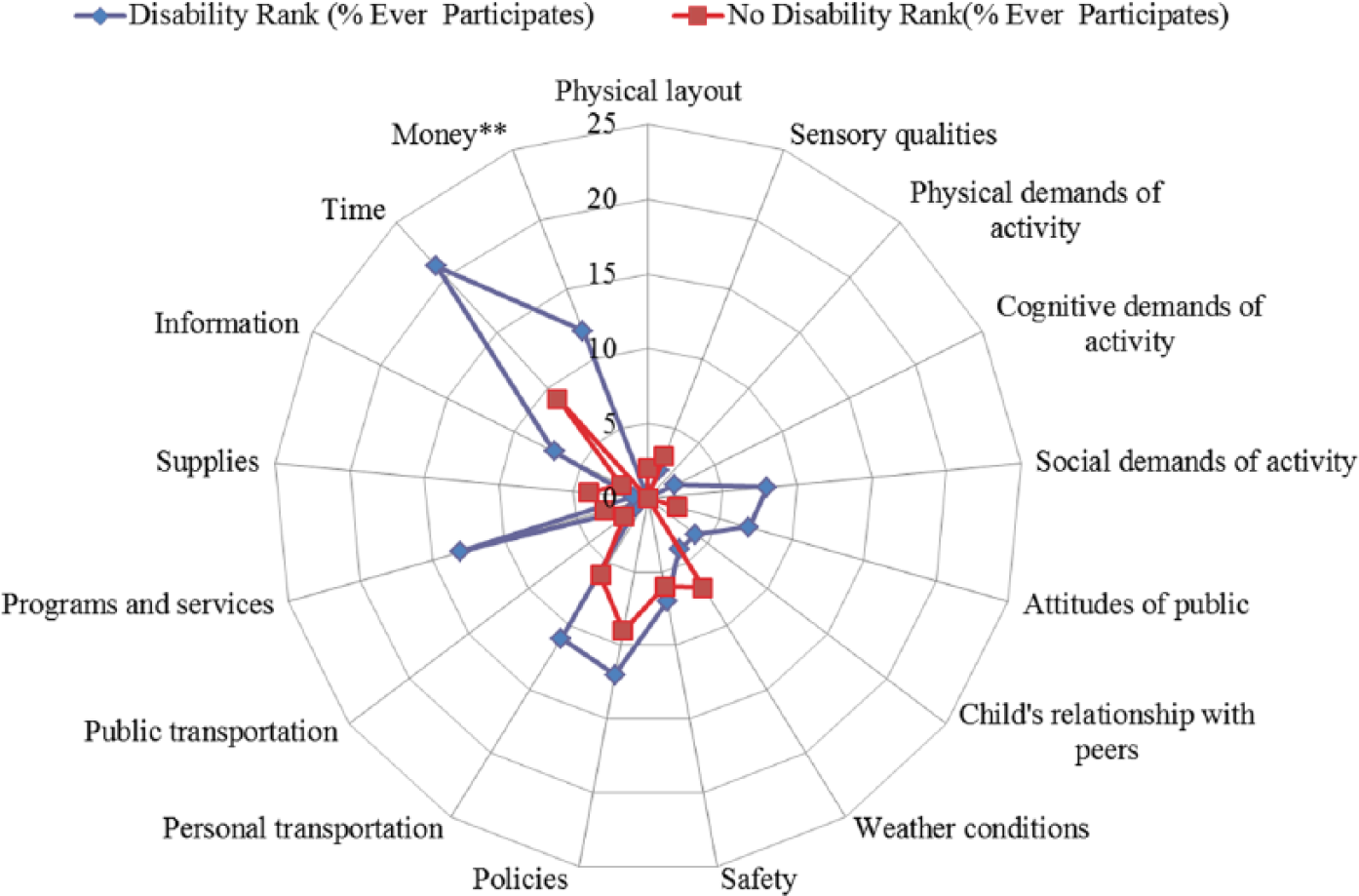
Percentage of parents who perceived the item as a barrier to community-based participation.
Summary Scores
Table 4 illustrates the differences in summary scores of children with and without disabilities in the child care/preschool and community settings. In the child care/preschool setting, significant differences were found in level of involvement, change desired, and perceived environmental support. In the community setting, significant differences were found in frequency of participation, level of involvement, and change desired. The greatest difference between the groups was desire for change in participation in child care/school and community settings.
Differences in Summary Scores.
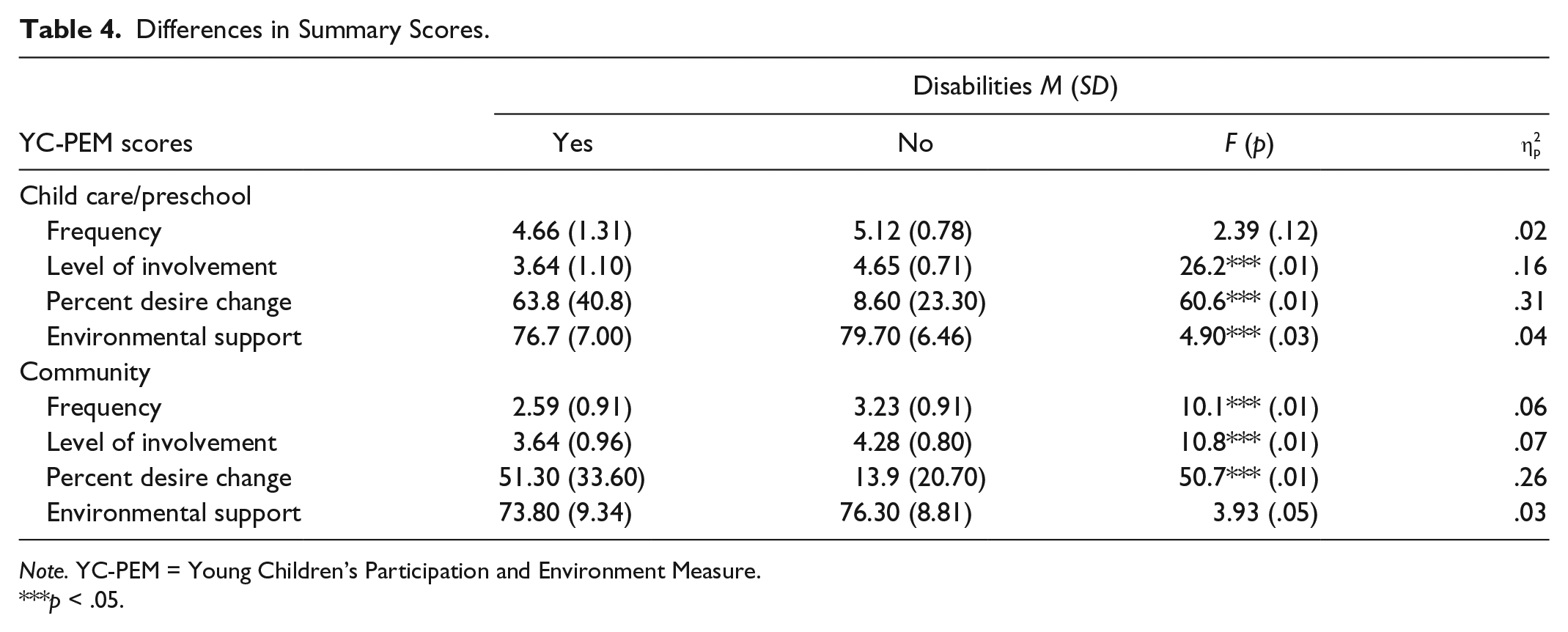
Note. YC-PEM = Young Children’s Participation and Environment Measure.
p < .05.
Discussion
The findings from this study extend the base of culturally relevant knowledge about participation and environmental supports/barriers among young children within child care/preschool and community environments. Significant group differences were found on most participation summary scores, illustrating that parents of children with developmental disabilities generally perceived that their children participated less frequently and were less involved in child care/preschool and community activities than typically developing children. More specifically, children with disabilities were less involved in activities that required socialization in child care/preschool and community settings. The environmental supports/barriers to child care/preschool and community participations that were identified to be significantly different between young children with and without disabilities in this study were largely related to the ICF’s environmental factors, namely, supports and relationships, attitudes and services, and systems and policies (WHO, 2001), thus supporting the relationship between participation and environment within the ICF. These findings were also consistent with the studies that have made similar comparisons with young children using the North American version of the YC-PEM (Khetani et al., 2015) and school-age children using the Participation and Environment Measure for Children and Youth (PEM-CY; Bedell et al., 2013; Coster et al., 2013).
Similar to studies of out-of-home participation involving school-age children with and without disabilities (Bedell et al., 2013; Coster et al., 2013), we found fewer differences in participation frequency between children with and without developmental disabilities in both child care/preschool and community settings compared with their level of involvement in activities. As routines and policies may determine frequency of participation (Coster et al., 2013), it is possible that preschoolers with developmental disabilities can be given similar opportunities with respect to how often they participate in activities but still differ in their level of engagement (Khetani et al., 2011; LaVesser & Berg, 2011). Consequently, findings from this study lend further support to the need for multi-dimensional assessment of children’s participation (Bedell, Khetani, Cousins, Coster, & Law, 2011; Coster & Khetani, 2008; Coster et al., 2012; Khetani et al., 2011; McConachie, Colver, Forsyth, Jarvis, & Parkinson, 2006). Frequency might not be the best metric for evaluating participation outcomes, as discrepancies were more evident within the Involvement scale. The findings from this study also indicated that participation differences begin in early childhood and persist through school age. It is therefore important to assess children with developmental disabilities fully at an early age so that strategies can be put in place to improve participation over time.
Parents of children with developmental disabilities desire change in participation for most activities compared with parents of typically developing children, particularly those activities that involve socialization. Children with developmental disabilities may have difficulties socializing independently, as they often have poor emotional/behavioral regulation (J. K. Baker, Fenning, Crnic, Baker, & Blacher, 2007), which was one of the most reported developmental problems in our sample. One potential way to improve on their socialization in out-of-home environments is to have programs and services that provide support for teachers and parents, to develop an understanding and effective social environment to facilitate socialization with peers, especially in unstructured activities. Parents of children with developmental disabilities in our study reported lack of programs and services as an environmental need, and studies with school-age children have also found that schools and the community lack programs and services specifically designed to meet the social needs of children with disabilities (Borell & Hemmingson, 2002; Brewin, Renwick, & Schormans, 2008; Carter, Sisco, Brown, Brickham, & Al-Khabbaz, 2008; Coster et al., 2013; Egilson & Traustadottir, 2009; Eriksson, Welander, & Granlund, 2007). In Singapore, emerging government programs, such as the Developmental Support Program (DSP), that support children with mild developmental disabilities such as delayed literacy and language development in preschools (Chong et al., 2014) should also focus on their socio-emotional support. Another participation issue raised was that children with developmental disabilities participated in fewer school excursions/events, similar to what previous studies have found (Colver, Hammal, Jarvis, & Welsh, 2006; Mancini & Coster, 2004; Simeonsson, Carlson, Huntington, McMillen, & Brent, 2001). Parents and teachers may find it difficult to manage the challenging behaviors of children with developmental disabilities due to the unpredictability of community places (B. L. Baker, Blacher, Crnic, & Edelbrock, 2002; Khetani et al., 2012; E. A. Larson, 2000; LaVesser & Berg, 2011; Maul & Singer, 2009). In Singapore, programs such as the Signposts for Building Better Behaviour program (Yap et al., 2014) have proven effective in increasing parents’ self-efficacy in managing their children’s behavior and should be made available to more parents. The program by Yap et al. (2014) guides parents to understand the purpose of their child’s behavior through systematic observation and to change either the trigger or the consequences to effect change in the child’s behavior. Future research is needed to determine if these programs and services are able to improve participation outcomes.
Besides the parents’ perceived lack of programs and services, they also perceived public attitude as a lack of environmental support to community-based participation. Based on an international literature review on parents’ experiences in caring for children with autism, parents experience stress and embarrassment when their children exhibit difficult behaviors in the community, because the public often misunderstands and relates the behavior to poor parenting (Chua, 2012). This is especially so in an Asian society where children are expected to demonstrate self-control and compliance at a younger age as compared with their Western counterparts (S. M. Lim, Rodger, & Brown, 2013). In addition, studies on Asian countries found that Asian culture’s focus on social identity and value might result in an increased stigma related to disability (Mak & Kwok, 2010; Sheridan & Scior, 2013). Chinese parents of children with developmental disabilities were also found to internalize the stigma and blame themselves for their child’s condition, which is detrimental to their psychological well-being (Mak & Kwok, 2010). This could be applicable to Asian families in Asian countries or those who have migrated to other countries. As research indicates that informal social support is associated with increased community-based participation among children with developmental disabilities (Khetani et al., 2012), strategies could be developed to help Asian families establish support from the public, relatives, and friends.
As parents with developmental disabilities in this study perceived public attitude as a lack of environmental support to community-based participation, societal attitudes should also be addressed. Poorer societal attitudes toward people with disabilities could be due to the lack of inclusive education in Singapore (L. Lim, 2009; Yeo, Neihart, Tang, Chong, & Huan, 2011). Inclusive education supports children with and without disabilities to study along side each other and the experience of being in contact with persons with disabilities can be more effective in changing attitudes than only information provision to increase public awareness of the needs of children with developmental disabilities and their families (Daruwalla & Darcy, 2005). Countries, such as Singapore, who have not adopted inclusive education, should consider adopting inclusive education as a way of changing societal attitudes toward children with developmental disabilities. For countries where there is social stigma toward people with disabilities, increasing public awareness through showcasing the abilities of people with disabilities and governmental initiatives such as hosting the Paralympic games can potentially change societal attitudes toward people with disabilities.
Parents in our study reported money as an environmental factor that is potentially important for child care/preschool and community-based participation. On average, children attended enrichment classes a few times a month. To keep up with their peers, parents of children with developmental disabilities enroll their children in early intervention programs, enrichment classes, and organized physical activities. Parents have to pay for these costly programs and classes, on top of the regular preschool fees. In addition, the majority of the parents of children with developmental disabilities in our sample have lower income than children without developmental disabilities. Due to the higher functional limitations of children with developmental disabilities, most families may rely on a single-income, and one parent, typically the mother, would stay home to care for the child full-time. This child care arrangement reduces the family’s combined income. Law et al. (2012) and Soref et al. (2012) found that the diversity and intensity of participation among young children with physical disabilities were significantly influenced by family income. If parents of children with developmental disabilities raise financial concerns as a restriction for their child to participate optimally, service providers should link them up with social workers to explore governmental subsidies or link them up with community resources that are more affordable.
To promote participation outcomes, context therapy and OPC could be considered. Context therapy could potentially improve participation outcome because it provides a way for occupational therapists to change the task and environmental factors to achieve participation goals (Darrah et al., 2011). For example, based on results from this study, occupational therapists could suggest ways to increase peers’ understanding of the social needs of children with disabilities to improve their child care/preschool participation. A randomized controlled trial conducted with 128 young children with cerebral palsy found that context-focused therapy approaches were as effective as child-focused therapy approaches and should be considered as a viable treatment strategy (Law et al., 2011). However, if it is logistically difficult to conduct therapy in the natural environment of the child such as at home or at preschools, OPC (Graham et al., 2009) could also be considered. OPC utilizes collaborative problem solving within a coaching relationship to guide parents to recognize and apply social and physical environmental changes that support more successful participation outcomes for themselves and their children (Graham et al., 2009). For example, based on results of this study, occupational therapists could coach parents to choose community activities that are less socially demanding to improve on the community participation of children with disabilities. Law, Anaby, Imms, Teplicky, and Turner (2015) found that using a coaching approach collaboratively with youths with physical disabilities and their families was effective in identifying and implementing strategies to remove environmental barriers to leisure participation.
Apart from direct intervention, occupational therapists should also advocate for their clients and intervene through community-building (Law et al., 2006), as enabling participation is a multi-method and multi-level approach (Law et al., 1996). Occupational therapists should be working beyond the acute hospitals and within the community to develop programs and services that support the participation of children with developmental disabilities. Two service delivery models have been developed to enable participation of school-age children with disabilities in schools. An example is the involvement of occupational therapists working within the RtI Framework (Cahill, 2010). Adopted by the U.S. Department of Education, the RtI guides implementation of special education programs in schools (National Center on RtI, 2010). The RtI benefits students with various learning needs by providing a system for delivering responsive instructional interventions that integrate academic instruction with positive behavioral support (American Occupational Therapy Association [AOTA], 2008). Occupational therapists have been increasingly involved in preschools within the context of RtI in the areas of handwriting, self-regulation, and self-management (Cahill, 2010; Frolek Clark, Brouwer, Schmidt, & Alexander, 2008; Henry, Ecker, Glennon, & Herzberg, 2009; Kiss, 2007). There appears to be great potential for occupational therapists to contribute to RtI in improving the participation of children within preschools because of their knowledge and skills in changing the environment to enable children of various learning needs to participate in preschool activities. A school-based occupational therapy service delivery model, P4C, emphasizes the partnership of the therapist with teachers and parents to change the life and daily environment of a child with developmental coordination disorder (Missiuna et al., 2012). P4C focuses on building the capacities of teachers and parents through collaboration and coaching in context with the goal of successful participation without referring them all for individualized, specialized intervention (Missiuna et al., 2012). RtI and P4C are potential service delivery models that can improve child care/preschool participation of young children with disabilities. Apart from service delivery models within schools, service delivery models within the community should also be developed to enable participation of young children with developmental disabilities in the community.
Limitations
The sample was not randomly selected and might not be representative of the general population. A more diverse sample in terms of children’s developmental/health issues and functional abilities should be obtained, as most of the children with developmental disabilities in our study had more social, emotional, and behavioral challenges than physical challenges. The participation profile and environmental needs of young children with physical disabilities impairments may differ from those of children with social, emotional, and behavioral difficulties and should be understood as well.
Future Directions
Future directions for research include examining participation in home environments for children with and without developmental disabilities (Law et al., 2013) and if they differ from participation in out-of-home environments. The types of changes that parents of children with developmental disabilities desire in their children’s participation could also be explored by examining the individual item responses to determine whether parents would like more or less frequency of participation, for their child to be more cooperative or interactive, or to participate in a broader variety of activities. Detailed information about the type of changes desired could guide occupational therapists in working on specific types of activities according to the types of change that the family desires, thus providing family-centered intervention. Future research could also examine the strategies that parents have used to enhance their children’s participation, as a previous study reported that parents found it easier to associate participation with environment when they describe the strategies that they have used to enhance their children’s participation (Khetani et al., 2011). Understanding the strategies that parents have utilized in our context could provide detailed information about environmental impact on participation. In addition, parent-reported strategies could offer service providers as well as policy makers ideas that could facilitate participation of children with developmental disabilities in their child care/preschool and community environments.
Footnotes
Acknowledgements
The authors thank KK Women’s and Children’s Hospital (Singapore), Department of Child Development, especially Ms. Teo Hui Fang, for their assistance in recruiting participants and for providing logistical support. They also thank Dr. Nancy Young from Laurentian University (Canada) for reviewing an earlier draft of this manuscript. Lastly, they thank all parents who supported and participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was obtained from Hamilton Health Science Faculty of Health Sciences Research Ethics Board at McMaster University (13-241-S) and KK Hospital Institutional Review Board in Singapore (2013/166/E) to conduct this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted with grants awarded by Singapore Association of Occupational Therapists and National Institutes of Health (K12 HD055931).