
Abstract
Musculoskeletal sonography is rapidly extending beyond radiology; however, best practices for successful integration into new practice contexts are unknown. This study explored non-physician experiences with the processes of training and integration of musculoskeletal sonography into rehabilitation. Qualitative data were captured through multiple sources, and iterative thematic analysis was used to describe two occupational therapists’ experiences. The dominant emerging theme was competency, in three domains: technical, procedural, and analytical. In addition, three practice considerations were illuminated: (a) understanding imaging within the dynamics of rehabilitation, (b) navigating nuances of interprofessional care, and (c) implications for post-professional training. Findings indicate that sonography training for rehabilitation providers requires multi-level competency development and consideration of practice complexities. These data lay a foundation on which to explore and develop best practices for incorporating sonographic imaging into the clinic as a means for engaging clients as active participants in the rehabilitation process to improve health and rehabilitation outcomes.
Introduction
The use of musculoskeletal sonography is rapidly extending beyond its traditional implementation by radiology professionals and is no longer used exclusively as a diagnostic tool. Researchers and practitioners are beginning to document potential uses of sonography to enhance patient care in a variety of ways (Akkaya, Ulasli, & Ozcakar, 2013). In rehabilitation, sonography has the potential to enhance practice by occupational and physical therapists (Roll, 2015; Roll, Asai, & Tsai, 2016; Roll, McLaughlin Gray, Frank, & Wolkoff, 2015; Teyhen, 2007) specifically in monitoring changes over time (Pong et al., 2009), individualizing treatments (Hsu et al., 2006), measuring therapeutic outcomes (Chon, Yoon, & You, 2010), and providing biofeedback (Hides et al., 2010; Teyhen et al., 2005).
Although there is a call for increased utilization of sonography by non-physician allied health providers (Estrach & Thompson, 2009), there is currently limited imaging content within professional curricula, and multiple challenges exist in developing post-professional education and competency requirements. First, there is the lack of consensus regarding standardized training, relevant competencies, and best practices for implementation across countries and disciplines (Cunnington, Hide, & Kane, 2005; Cunnington, Platt, Raftery, & Kane, 2007; Speed & Bearcroft, 2002; Wakefield et al., 2004). Second, developing competency in sonographic imaging requires significant hands-on experience, much of which is beyond clinical hours. As many as 500 scans may be necessary following formal didactic training (Speed & Bearcroft, 2002), and the total average time required for the entire post-professional training process could require more than 100 hr (Brown et al., 2004). Finally, to ensure effective implementation, consistent expert mentoring is an important component of the post-professional process (Cunnington et al., 2007), something not readily available for non-physician rehabilitation providers.
In addition to complexities of training, integrating sonography into rehabilitation requires consideration of the ways in which therapists reason and interact with patients, which are unique from that of physicians and radiology professionals. The overall goal of therapy is to promote optimal function through clarification of the diagnosis, identification of areas for improvement in function, and selection of therapeutic activities (Stucki, Cieza, & Melvin, 2007; Zanca & Dijkers, 2014). Change is targeted at numerous levels, from body structures to participation in daily life, and a variety of treatment theories and methods are used to concurrently address multiple goals (Whyte, 2014; Zanca & Dijkers, 2014). The therapeutic process reflects an ongoing integration of assessment and treatment in which therapists tailor activities in response to patient performance (Whyte, 2014). For successful implementation, the use of sonography in clinical practice by rehabilitation providers must be fully integrated with these complex and concurrent therapeutic processes.
Given the identified challenges in post-professional training and the unique circumstances surrounding implementation of musculoskeletal sonography by rehabilitation providers, careful investigation of the training and implementation process is needed. The purpose of this research was to gather information on factors involved in implementing sonography within occupational therapy to gain deeper understanding of these processes and identify challenges to successful integration. Because little is known, a qualitative approach was used to preliminarily explore the following question: How do occupational therapists experience the process of training and implementation of musculoskeletal sonography into upper extremity rehabilitation? The results of this study present salient issues related to developing competence in imaging for rehabilitation professionals and particular challenges with clinical implementation, which give direction for expanded research to better understand therapist and patient experiences.
Method
The researchers used a qualitative descriptive research design (Sandelowski, 2000, 2010) to conduct a preliminary investigation of therapists’ experience of implementing sonography in an upper extremity rehabilitation setting as part of a feasibility study. As a preliminary investigation, the purpose of this study was to explore this novel practice technique to provide foundational insight into the development of best practices for training and implementation. Rigorous procedures were used throughout an iterative process of data collection, analysis, and interpretation (Patton, 2002; Strauss & Corbin, 1990). The institutional review board (IRB) of the academic medical center approved the use of human subjects in this study, and both the therapists and patients provided informed consent to participate.
Participants
Purposeful sampling was used to recruit occupational therapists selected on the criteria of (a) specialization in hand rehabilitation, (b) contrasting levels of experience, (c) availability to participate in the training and to implement the sonography in a clinical setting, and (d) willingness to provide data and be interviewed. Two occupational therapists working in an outpatient hospital-based hand rehabilitation clinic were available and agreed to participate in the training and implementation process. One of the therapists (Therapist 1 [T1]) was a Certified Hand Therapist (CHT) with more than 20 years of experience. The other (Therapist 2 [T2]) was an entry-level therapist completing a residency in hand therapy as partial requirement for a clinical doctorate. Patient participants were recruited from the therapists’ caseloads using a convenience sampling method; recruitment of patients occurred when both the therapist and patient had time available at the end of the evaluation session, and patients expressed interest in being scanned with sonography. In addition, to be included, patients were above the age of 18; had no open sores, wounds, or casts; and were English speaking. Patient diagnoses were reflective of a typical outpatient hand therapy practice, varying and including crush injury, tendon rupture, release of the dorsal extensor component, ganglion cyst, tenosynovitis of the thumb extensors, and general hand pain.
Study Phases
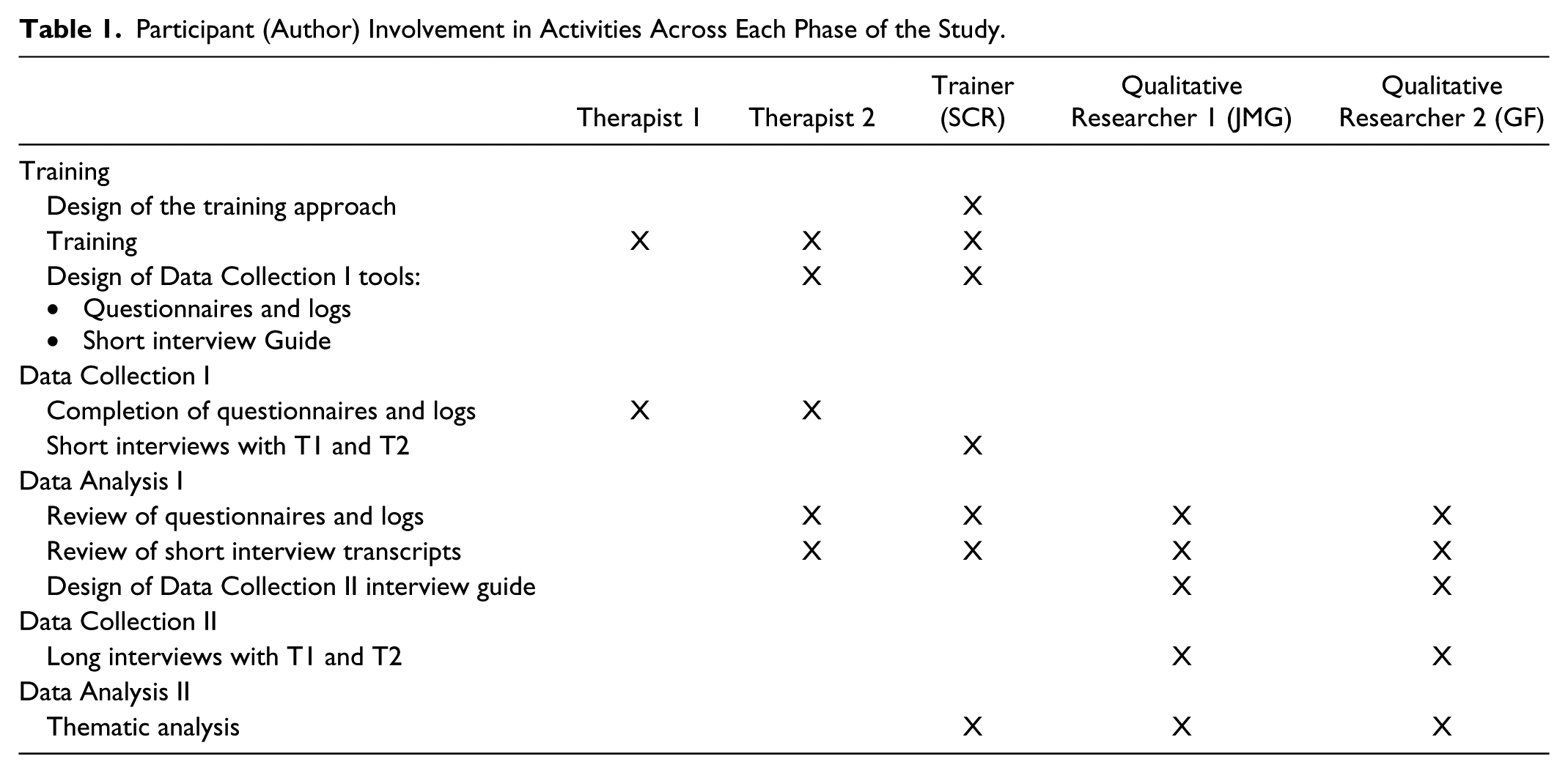
The feasibility study took place over 12 months in five phases: Training, Data Collection I, Data Analysis I, Data Collection II, and Data Analysis II. The roles of each team member were structured to maximize the qualifications of the research team as a whole, while maintaining rigor and trustworthiness of the design, data, and findings (Lincoln & Guba, 1985). It is noted that one of the occupational therapists (T2) had a dual researcher–participant role during Data Collection and Analysis I; however, the researcher aspect of T2s role ended prior to Data Collection and Analysis II. Table 1 summarizes the activities and participants in each phase.
Participant (Author) Involvement in Activities Across Each Phase of the Study.
Training
Both occupational therapists participated in 12 training sessions for a total of 28 hr of direct training in the use of sonography for the upper extremity. All sessions were conducted by the researcher/trainer, an occupational therapist also registered in musculoskeletal sonography (RMSKS). No standardized protocols or curriculum exist for training in the use of musculoskeletal sonography, let alone training targeted specifically to non-physician, non-sonographer rehabilitation providers. Therefore, the trainer developed modules using a textbook (Jacobson, 2007) and scanning protocols/guidelines published by professional organizations (i.e., American Institute of Ultrasound in Medicine, European Society of Musculoskeletal Radiology). Training included an initial session providing an overview of ultrasound physics and operation of the equipment, followed by 10 sessions covering anatomical reviews, scanning protocols, and hands-on practice to identify musculoskeletal structures of the distal upper extremity. Competency was assessed in the final session using case studies for which each therapist had to demonstrate (a) appropriate clinical decision making regarding sonography use and (b) the selection and successful completion of a scanning protocol with output of quality images. Following formal training, the therapists independently practiced with the sonography intermittently for a month prior to implementation with patients.
Data Collection and Analysis I
Data Collection I was conducted over a 3-month period as the therapists began clinical implementation of sonography. Nine patients were recruited and imaging was conducted at the beginning of treatment, at discharge from their course of standard therapy, or at both time points. Data were collected using a scan log during each scan, an open-ended questionnaire following each scan, and semi-structured interviews, each developed specifically for use in this study. The scan log documented a patient’s diagnosis, the structure(s) of interest, and the therapist’s purpose for obtaining each image or video during the scan. The questionnaire captured information about the therapist’s confidence with sonography use, patient characteristics, perceived usefulness of the scanning, and barriers and facilitators to use. Information provided by the therapists on the scan log and in questionnaire responses were reviewed by the trainer and were used to inform semi-structured short interviews (about 15 min each). A total of five short interviews were conducted intermittently throughout the implementation period with the purpose of exploring the therapists’ evolving experience with the implementation process, specifically their perceptions of implementing sonography into hand therapy, and clinical reasoning surrounding sonography use. Each subsequent interview provided an opportunity for the therapists to expand upon comments made in the questionnaires and to reflect on new experiences and revelations that occurred since the previous interview. Conducting this series of interviews over time allowed for increased data capture to assist in identifying recurrent themes and move toward data saturation given the limited sample size. In Data Analysis I, the study team expanded to include two expert qualitative researchers who acted as peer auditors to debrief and identify possible biases of the RMSKS researcher/trainer and the dual-role participant–researcher (T2). The team reviewed the scan logs, questionnaire responses, and transcribed interviews and identified preliminary themes via open coding (Patton, 2002). Reflecting the iterative process of qualitative research, these preliminary themes informed the development of a second semi-structured interview guide used to gather a more detailed understanding of the therapists’ experience with implementing sonography.
Data Collection and Analysis II
Data Collection II involved semi-structured, open-ended interviews (about 1 hr each) with T1 and T2 conducted by the qualitative researchers. To minimize response bias and enhance credibility of the data, the RMSKS researcher/trainer was not present during the interviews. The interviewers elicited reflections on (a) experiences using sonography with specific patients and (b) general perceptions and reflections about using sonography in hand therapy. In Data Analysis II, the RMSKS researcher/trainer rejoined the two qualitative researchers for an iterative process of reading, rereading, and coding the new transcripts. The research team discussed and reconciled questions or inconsistencies between the new transcripts and the previously analyzed data. Data were coded to determine categories to which specific statements and assertions belonged, and to explore the meanings suggested by these statements within the research and clinical contexts. Numerous iterations of data analysis occurred through multiple discussions among the study team, resulting in a final synthesis of the data into meaningful thematic units concerning the domains of competency and contextual considerations required for successful use of sonography in hand therapy.
Results
The results of this study illuminate the occupational therapists’ experiences with training and implementation of musculoskeletal sonography, while elsewhere is reported their overall perceptions of how musculoskeletal sonography might complement rehabilitation practice (Roll et al., 2015). The dominant theme of these data concerns competency, within three domains: technical, procedural, and analytical. Closer exploration of the data indicated that competence in practice resulted not only from skills in each of the three domains but also through the complex interaction of the three domains. Moreover, implementation of sonography took place within specific social and institutional contexts of practice (Figure 1).
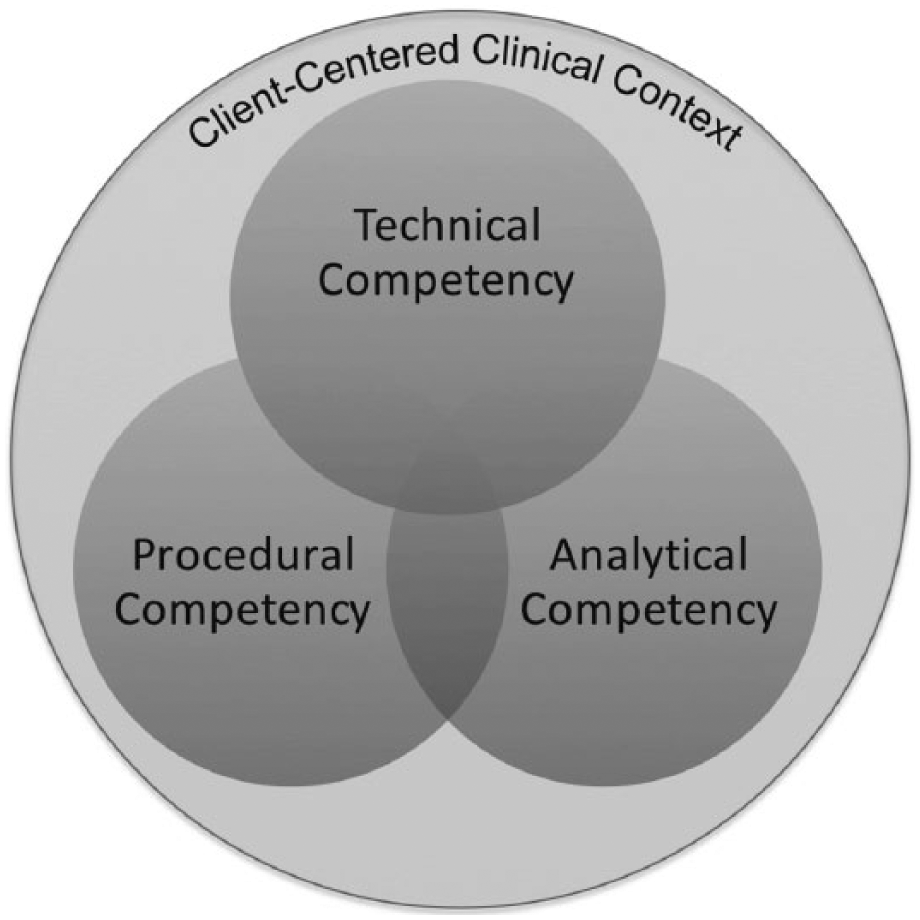
Interrelationship of various competencies required for successful integration of sonography into rehabilitation.
Competencies
Competency domains
After the training period, the therapists experienced challenges while implementing sonographic imaging with their patients. The data exposed the therapists’ awareness of specific areas in which they needed to become more proficient. T2, who had assisted in the design of the first phase of the research, articulated three areas of competency that she considered central to integrating sonography in her practice: These three [competencies] . . . are pivotal in learning to use musculoskeletal ultrasound. The first is the technical aspect, learning to operate the machine; the second is . . . figuring out what structures to scan, where to place the transducer, how to actually get the image quality that you want; and then the third is . . . being able to read the information that you’ve gathered. (T2)
This comment by T2 provided an insightful conceptual framework to organize the data in the study. During Data Analysis II, the researchers formalized and defined these domains as technical, procedural, and analytical competency, finding them to be useful and reasonably exhaustive of the contents of the data set.
Technical competencies primarily related to the operation of the machine itself, specifically, adjusting settings, capturing and storing images and videos, positioning the transducer, and changing imaging modes. As an example, early in the implementation process, T1 expressed a desire for more training and practice in “the buttons . . . how to just set a person up and take the scans, pictures and video.” She described her challenges with these various functions: I got confused at saving an image versus video and pulled out my notes. I think I did Doppler one time but not sure . . . if it doesn’t follow the exact scenario I don’t know what to do. So when the screen [froze], I didn’t know what to do. (T1)
Over time, new technical challenges arose as the therapists learned the capabilities of the equipment and became more adept at assessing the quality of the images taken. For example, T2 remarked, “I know how to adjust settings, but the adjustments don’t always seem to help image clarity.” The therapists also struggled with technical aspects related to interfaces among themselves, the patients, and the equipment. There were concerns about body mechanics and ergonomics, as well as the safety and comfort of patients when utilizing the ultrasound. One therapist noted, “a lot of twisting and bending to prevent twisting and bending of the patient” (T2), whereas the other experienced “mild soreness” (T1) due to awkward neck rotation to look at the screen and difficulty sustaining grasp on the transducer for the duration of the scan.
The second competency domain, procedural, encompassed, yet went beyond, technical competencies and involved deciding which structures to scan and how to capture a high quality image of those structures. Given her more than 20 years of experience treating the hand and upper extremity, T1 remarked that she “[likes] to think [she’s] good at knowing what to scan.” Nevertheless, a challenge arose in the transition from that initial decision to the final product of a high quality image or video. She described her efforts toward acquiring this procedural competency: I bought an ultrasound book just because I need to look at it and study it a little bit more. . . . looking at their case studies, what was confusing to me was, I need to see normal and abnormal and they were just going through normal . . . that’s just a teaching style and that’s how the book presented it, and I understand that now, but at first . . . you know, I can’t tell you. (T1)
The other therapist remarked on how this became evident as soon as she began to implement the technology in the clinic: Once we got the ultrasound in the clinic we started recruiting patients pretty quickly and so we were immediately jumping into the abnormal and I was realizing that, first off, I didn’t really know what to expect with the abnormal. (T2)
The development of procedural competency also involved a process of prioritization by both therapists. One therapist described a particular patient stating that there was “so much involved, [she] had trouble deciding where to start/what to look for” (T2). With complex cases, identifying structures of interest seemed to be only the first step. One therapist noted that she “would have liked to look for scar adhesion during limited [movements], such as thumb [abduction and extension with forearm supination/pronation], but had difficulty doing so” (T2). Executing a scan to capture high quality dynamic images remained a challenge beyond simply identifying structures.
Analytical competency, the third domain identified in the therapists’ responses, included accurate reading of images obtained—a more sophisticated (diagnostic) differentiation between normal and abnormal—along with incorporation of this knowledge into intervention planning. One therapist noted, “I’m still trying to figure out what I’m seeing internally” (T1). The other therapist commented, Even once I got to the point where I was able to get a good quality image, reading it was difficult because there’s just, I felt like I didn’t have the experience and I hadn’t seen the number of scans to fully understand what I was seeing. (T2)
She expressed her ongoing struggles with making sense of the images: In terms of evaluating what I’m seeing, I’m still struggling . . . I think now I can see it [the pathology] once I’ve been told, but we aren’t seeing the same thing repeatedly so each time I do a scan it’s something new I have to look for, and so I’m back at square one with not knowing how to evaluate the image. (T2)
Both therapists identified the need for increased familiarity with identification of abnormal structures. T2 summarized this the best in stating “I definitely feel like I would have liked to see a lot more normal anatomy on ultrasound images and a lot more—much, much more—pathological images.”
Interaction among competency domains
The therapists’ experiences with implementing sonography revealed that the competency domains were not mutually exclusive or as discrete as expected, but rather interconnected in multiple different ways. At times, competencies appeared to be nested within one another. For example, one therapist noted that her confidence in mastering technical competencies was first necessary to move forward in confidently mastering procedural and analytical competencies: When you have limited experience and limited knowledge of how to use the technology and you know what you’re expecting to see but you don’t see it, my immediate response was to think I was holding the transducer wrong . . . and so I think [with] a lot of my images I spent so much time trying to make it look the way I expected it to see, that I didn’t realize that for this specific patient it’s not going to look anything like I expected it to look because there was so much involved. (T2)
In most circumstances, the process of competency development was concurrent across the three domains, requiring the therapists to master combining several competencies at once. In one instance, the therapist described her confidence in procedural competency, but expressed concerns with concurrent technical and analytical competencies (i.e., obtaining images and discussing images with the patient): I’m okay with what to scan, but while I’m scanning, I’m watching the transducer. I wanna make sure it’s at 90 degrees and I feel like if I watch the picture then I’m not gonna be holding that transducer the way I want, so I’m not really watching the picture. So, even if I was to use it for [patient education], I would have to replay the picture . . . because I have to really watch where my hand is and what I’m doing. (T1)
Similarly, the other therapist commented that she “was really concentrating and had difficulty multitasking enough to educate” the patient (T2). Intersections among all three domains of competency are also evident in the following excerpt in which one therapist describes the complex process involved in mastering the machine, capturing appropriate structures, and interpretation of the images being obtained: I’m still trying to figure out what I’m seeing internally, and so I’m again back to, “Is there scarring?,” “Is there collagen?,” because the first day I saw her it was . . . very angry red puffy scar and it’s calmed down a lot since then. So I don’t know if that got picked up on these scans. I can’t tell by looking at the pictures and I did compare right and left. I hit the screen funny at one point so I didn’t know how to get out of that. I think it was Doppler. I’m not sure. Then I wanted to do a video and I don’t know if that worked either, so, for me, it’s just practicing and finding the buttons and things. (T1)
On-site mentoring during the implementation phase was crucial in competency development. Both therapists frequently looked to the RMSKS trainer for ongoing feedback on their technique, instructions on operation of the machine, assistance in improving the quality of their images, and guidance in evaluating those images. In one of the weekly interviews, one participant remarked to the trainer: It might be good for you to be there when I do one [scan] and see if I’m holding the transducer the right way. I mean, I think I am, but I don’t know. When I think I’m fanning, am I really fanning? If I’m seeing a dark spot, is that really fluid or anisotropy? . . . I wanna get better at it and I don’t know if I’m even holding it the right way. (T1)
Speaking of her mentorship experience, the other therapist noted, Even once I got to the point where I was able to get a good quality image, reading it was difficult because I felt like I didn’t have the experience and I hadn’t seen the number of scans to fully understand always what I was seeing. And so meeting with [the trainer] has been really helpful for that because a lot of times I’ll do a scan and have absolutely no idea what I’ve found, and then we sit down and he can identify exactly what I was scanning without looking at my notes and he can point out scar tissue that I hadn’t noticed was there and the impact it’s having on the tendon that I hadn’t noticed. (T2)
Reviewing images with the mentor enhanced the therapists’ understanding of proper technique as well as assisted them in analyzing the resultant images and problem solving how scans could be done differently the next time. Moreover, beyond competency, the mentorship seemed necessary for validating reasoning, perhaps supporting the development of confidence within and across each competency domain.
[The trainer] was going through the scan with the ganglion, the little ganglion cyst, and he said, “Well, I would have scanned it this way next,” and I said, “Well, that’s what I did.” Then he said, “And then I would have scanned it . . . ” “Oh, that’s what I did!” You know, so, yes, my clinical reasoning did help me to see what was hanging up and where I was going [with my treatment]. (T1)
Context of Practice
Careful review of the therapists’ experiences also revealed ways in which competency development and implementation were situated within the context of client-centered rehabilitation. Integration of this new technology required time, both the therapists’ and patients’; space; and resources. In addition, individual therapist and patient factors, as well as consideration of the complexities of integrating the imaging within a patient’s overall intervention plan, each contributed to the complexity of successful implementation. Finally, an unanticipated, yet frequently mentioned, factor involved the interprofessional rehabilitation culture. At times, contextual factors were constraints, hindering the use of sonography in situations in which the therapists ordinarily would have used it readily, while at other times, they were simply viewed as challenges.
Time was the most frequently mentioned contextual factor, and in several instances was reported to be a constraint. This factor was discussed in terms of the extended time the therapists required to complete a scan due to developing competencies, as well as the already limited time for the entire patient evaluation and intervention. Of these two constraints, the therapists’ limited efficiency with the technology seemed paramount. In early stages, the time needed to perform a scan exceeded the therapists’ expectations and interfered with implementation in some instances. One remarked, It takes me a while to position the probe correctly and I feel like I don’t have time to localize all the structures I’m interested in . . . at the end of the hour I still feel like I couldn’t cover everything that I wanted to cover. (T2)
The more experienced therapist recognized the need to increase efficiency to include sonography as a reimbursable service as part of the evaluation: I think we’d get better with practice—but for right now it’s thirty minutes to an hour of scanning; and so if you got better with that you could say that’s just part of your eval, and . . . pictures would be very powerful as documentation, too, if we started to use it for that purpose. (T1)
The other concurred, “It does take time, you know, to pull it out and set it up and if you only have half an hour treating somebody maybe you can’t do it every time” (T1). She noted that incorporating sonography for patient education would also take more time: just whipping out a book—you know where certain pages are that you want. That’s faster . . . So this is a little bit more time, you know, the set-up, bringing it out, and putting the gel on . . . (T1)
T2 was in agreement and identified a possible solution: If we’re using it for education I don’t think we could spend more than 15 minutes on it, and even that may be too much. But, if you’re using it for them to watch the muscle contract while they’re doing exercises, then it would give you more time. (T2)
The individual characteristics of the therapists were a second important factor that influenced how each was able to develop competency and integrate the sonography into her practice, specifically, experience and technical aptitude. Although neither therapist had prior experience with sonography, the novice therapist noted that proficiency with anatomy was essential to implementation: For this to be able to be implemented in a clinical setting, I think access to a machine and emphasis on the importance of practicing on oneself and anyone available is, is really important, and really, really being competent in the normal anatomy before scanning patients. (T2)
Although the novice therapist had less experience with clinical reasoning and typical anatomy, she had an advantage with some of the technical competencies. As the more experienced therapist explained, It is simple technology, but I’m not a computer person . . . I think new generations are like, “oh, okay!” and they just do it. But I had to write down [the steps] and then sort of study . . . So it was a little more challenging for me but still doable . . . It’s just frustrating that the machinery for me is a little more complicated, but I’m getting it, you know, I’ll keep working on it and I’ll get it. (T1)
Individual patient characteristics, both physical and psychosocial, also influenced the process of competency development, the nature of the competencies required, and the ways in which sonography was implemented. Depending on stage of recovery and clinical presentation, use of sonography was limited for certain patients. For one patient, T1 described, “Right now, there’s an open pin site, so we wouldn’t be able to do [sonography] yet,” and for another, “I don’t even know if we can scan her because she still has sutures.” Although these types of constraints were transient and would resolve as the patients progressed, other patients had physical conditions that did not prohibit, but certainly complicated sonography use: I’m on the fence because she’s really hypersensitive so I don’t know if the ultrasound will bother her . . . I noticed scarring right under that incision, so I don’t know . . . I mean it’s very pin-pointable, so I’m not sure . . . knowing that it’s there, how that will guide me, and if it’s painful, I don’t want to do it, but I’ll see, I’ll see how she’s doing with some of the little things I gave her. (T1)
Another patient reported having a sacral fracture, which necessitated evaluation/scanning in supine. The therapist noted that the patient’s “hand was positioned on a pillow which didn’t feel as stable as the table” (T2). Similarly, external rotation of the shoulder was contraindicated for another patient for whom the therapist noted, “sometimes there was artifact when I would try to work around his [limited] mobility” (T2).
T1 described a situation in which she opted not to use the sonography at all because of where the patient was in his or her overall recovery and psychosocial adaptation: She has a lot of questions—so I think I need to just sit down with her and spend time just talking to her, versus scanning—and a lot of other medical issues which shouldn’t affect this, but she needs TLC. (T1)
Although both therapists believed the sonography presented an untapped potential to positively influence patient engagement, the use of the sonography for patient education and motivation also raised concerns. Therapists worried about how patients might respond emotionally if ultrasound findings did not confirm progress or indicated poor potential for recovery. As T1 explained, “Telling her that it’s working means she can have hope and she can improve it. If it’s not working, and the doctor said that’s something he’s repaired, I’d rather talk to the doctor about it” (T1). T2 had this experience with a patient: It was really interesting because my therapy up to this point has been focusing on trying to get that tendon gliding, to get more motion at the interphalangeal joints (IPs), and we’ve realized from this scan that progress there is likely pretty limited . . . and that brought up an interesting consideration. I was curious . . . how that is going to impact morale, because that can be really disheartening, especially since he understands and he knows. (T2)
This situation was unique in that the patient was a radiologist; thus, he was knowledgeable about the implications of his sonography. In both cases, the therapists felt a need to be able to manage patients’ reactions to potentially disappointing findings.
In addition to managing patient response to disappointing or incidental findings, the therapists discussed these concerns within the context of interprofessional care. Specifically, the therapists observed the potential for sonography to reveal new information about the diagnosis made by a referring physician. As one therapist commented, “Really the physicians should be diagnosing, but to say ‘you’ve got some scar tissue here after the incision,’ I think we would be fine with saying that, or ‘look there’s swelling here,’ and measure the swelling” (T1). However, concerns about navigating interprofessional relationships were more complicated when sonography revealed information that seemed contradictory to the physician’s summary. T2 described the dilemma posed by identification of a ganglion when tenosynovitis was diagnosed: I would have to think about what I would do in that situation, ‘cause there’s not a whole lot you can do therapeutically for a ganglion, and we aren’t allowed to use this tool diagnostically, so I don’t really know how I would bring it to the referring physician’s attention. (T2)
The other therapist described a similar dilemma, avoiding providing contradictory information to a patient: Well, the only thing is not being able to diagnose, not being able to say to that person, “okay this is going on,” especially if you see that something’s not working . . . So, we’re looking at them . . . we can’t diagnose, and . . . so I just educated her a little bit. But she did want to know “Is this one working?” and I said, “I can’t tell.” I just said that. (T1)
Together, these dilemmas reflected that assumed professional boundaries, especially regarding the diagnostic process, may become blurred when implementing sonography in a rehabilitation context.
Discussion
Recent professional literature suggests that allied health professionals might routinely complete sonographic scans to supplement their evaluations and enhance client-centered rehabilitative care (Estrach & Thompson, 2009; Roll, 2015; Teyhen, 2007). To advance this perspective, the goal of this study was to examine occupational therapists’ experiences with training and implementation of sonography in upper extremity rehabilitation. Along with findings on how sonography might be used in this setting (Roll et al., 2015), this study revealed three interrelated competencies and various complexities of integrating sonography into a rehabilitation context. These data illuminate three primary considerations for the implementation of sonography by rehabilitation providers: (a) understanding the place of imaging within the complex dynamics of rehabilitation, (b) navigating interprofessional care and nuances of the evolving diagnostic process, and (c) developing appropriate post-professional training.
There is an ongoing dialogue regarding the complex dynamics of the therapeutic processes involved in rehabilitation (Dijkers, Hart, Tsaousides, Whyte, & Zanca, 2014), which includes physical and temporal settings, equipment, frequency and type of cueing or patient assistance, activity performance and modification, treatment approaches, and interdisciplinary collaborations (Zanca & Dijkers, 2014). A key tenet of successful rehabilitation is the full integration of these dynamics or factors, along with the therapeutic relationship between the patient and practitioner (Kayes & McPherson, 2012), all of which can modify the delivery or effects of the rehabilitation process (Hart et al., 2014). In addition, patient education and training are often coincident with activities, and treatments often address multiples goals at once. Given these therapists’ experiences, when used in rehabilitation, sonography becomes part of the complex clinical dynamic via the evolving and intricate relationships among the technology, patient, and therapist. Moreover, as a mind–body intervention, the ability of sonography to show a patient his or her own tissues and pathology is potentially a very powerful active ingredient in the rehabilitation process (Dijkers et al., 2014).
In addition to influencing the complex dynamics of implementing care in rehabilitation, sonography played a key role in the therapists’ iterative clinical reasoning. Specifically, implementation of sonography as part of the rehabilitation process enhanced the therapists’ understanding of each patient’s condition and, in turn, revealed nuances of the evolving diagnostic process. As healing and recovery are not stagnant, neither is a patient’s diagnosis. As such, a physician’s diagnosis might be best viewed as an element of clinical history that can be further informed by sonographic imaging (Penny & Zachariason, 2015). Accordingly, the referring physician’s diagnosis might be considered a working diagnosis, and the sonography implemented in therapy becomes investigative imaging to identify specific tissue pathology (Baun, 2004; Penny & Zachariason, 2015). Although the working diagnosis may be determined based on the patient’s clinical signs and symptoms, establishing a sonographic diagnosis advances and refines the care process (Baun, 2004).
Not only does understanding specific tissue involvement advance clinical reasoning and treatment planning by the rehabilitation provider, but sonography also provides a means for evaluating a patient’s physiological response to treatment as he or she recovers. This ability to evaluate and document the healing process supports ongoing efforts to classify and understand the complex process and outcomes of rehabilitation (Dijkers et al., 2014). Despite the potential for sonography to support clinical reasoning, treatment planning, and evidence building, there is a need to identify best practices for interprofessional communication, and determine decision-making authority throughout this evolving diagnostic process, especially related to negative or incidental findings.
Leveraging the advantages of sonography in rehabilitation and developing best practices for interprofessional care are dependent upon adequate training of rehabilitation providers. Although limited instructions on integrating imaging into a care plan are beginning to appear within entry-level curricula in the therapeutic professions (Commission on Accreditation in Physical Therapy Education, 2013), training in image acquisition and analysis is not widely included. With limited imaging instructions, the complex integration of all three domains of competency, as identified in this study, is likely not addressed at all. This study suggests that sonography training in the three interrelated competencies (i.e., technical, procedural, analytical) needs to also account for complexities unique to the rehabilitation context. Post-professional training structured around an iterative process of didactic learning, clinical practice experience, and mentoring will likely be more effective than one that is strictly linear and sequential. The training should account for the ways in which sonography use by rehabilitation providers differs from other professionals. To maximize care, therapists must develop the ability to evaluate and interpret findings as part of the clinical reasoning and evolving diagnostic process (Baun, 2004), and navigate the complex dynamics of the therapist–patient–machine interface.
This research provides a preliminary investigation into the complexities involved in training non-physician practitioners, specifically occupational therapists, and implementing sonography as part of the client-centered rehabilitation process. Because this is an area of practice innovation not yet widely implemented and the research required participants who were able to dedicate time to both training and data collection, this study involved a limited number of participants. Moreover, because the qualitative data were obtained as part of a feasibility study with a pre-determined timeline, repeated interviewing was restricted to this timeline and may have limited the opportunity to achieve rich data saturation. Given these limitations, findings are not meant to be widely generalized, and may not fully represent experiences of all occupational therapists in this area of practice. Instead, these preliminary findings are meant to provide initial insight and a foundation upon which researchers and practitioners can build as the profession considers adopting the technology into practice. These findings can and should be further explored in more diverse and larger contexts to develop and evaluate different models of training and mentoring, as well as to identify best practices for clinical implementation of sonography to advance clinical reasoning and patient outcomes, while navigating the intersections among training competencies, rehabilitation dynamics, and interprofessional care. Once training and best practices are addressed, the effects of clinical sonographic use as a rehabilitation intervention on patient outcomes and exploration of patient experiences of the use of sonography in rehabilitation can be explored.
Conclusion
This research provides insight into the complexities of training and implementation of sonographic imaging into a rehabilitation context by non-physician practitioners to improve the health outcomes and well-being of patients. Given the experiences of therapists in this study, training for occupational therapists and other rehabilitation providers may differ from that of other radiology and physician providers due to the complex dynamics of the rehabilitation process. In addition to imaging competency development, training must consider clinical reasoning, evolving diagnostics, and therapist–patient–equipment interactions, and provide extensive mentoring in context. Furthermore, these data identify a need for best practices in navigating and maximizing the interprofessional rehabilitation environment. When appropriately deployed, the unique training and integration processes will afford further study on the piloting of real-time implementation and reimbursement and the effects of point-of-care sonographic imaging on patient engagement and participation, as well as potential effects on improvement in health outcomes.
Footnotes
Acknowledgements
The authors wish to acknowledge and thank Monique Wolkoff, OTD, OTR/L, for her assistance with this research.
Authors’ Note
Portions of these data were presented in an abbreviated format at the American Institute of Ultrasound in Medicine Conference in Orlando, Florida, in March 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institutes of Health (NIH) Rehabilitation Research Career Development Program Grant (K12 HD055929). The contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health (NIH).