
Abstract
Optimal child development is supported by services, policies, a social determinants of health (SDOH) frame, and meaningful participation (as defined by the International Classification of Functioning, Disability, and Health–Children and Youth [ICF-CY]). This scoping review describes the social determinants that may affect the participation of young children aged 0 to 3 years with developmental disabilities (DD) in the United States. Scoping review of studies including U.S. children with DD aged 0 to 3 years, from 2000 to 2016, were used. 5/979 studies met inclusion criteria. Two researchers independently coded studies to align them with both ICF-CY and SDOH. Studies found determinants of participation stemming from the child (e.g., individual) and multiple contexts: immediate, community, and policy. The emergent literature continues to primarily focus on child determinants but suggests participation of young children with DD is affected by social determinants stemming from the community and policy contexts. The literature underrepresents children from racial/ethnic minority backgrounds.
Introduction
In the United States, young children with developmental disabilities (DD) aged 0 to 3 years are eligible to receive early intervention (EI) services under the Individuals with Disabilities Education Act, Part C (IDEA Part C, Public Law 108-446). Rehabilitation professionals who provide EI services are informed by the World Health Organization’s (WHO) International Classification of Functioning, Disability, and Health–Children and Youth (ICF-CY; WHO, 2007). Research guided by the ICF-CY has revealed the dynamic relationship between personal and environmental factors and the participation of children with DD (Anaby et al., 2013; Fauconnier et al., 2009; Palisano et al., 2011; Soref et al., 2012; WHO, 2007). Increased attention in rehabilitation to the physical and social environments of children with disabilities coincides with health care and public health’s increased attention to the social determinants of health (SDOH). SDOH have been defined as the structural determinants and conditions in which children are born and in which they grow (Marmot et al., 2008). These determinants stem from multiple “spheres of influence” or contexts (e.g., immediate home and family, community, and policy) that shape children’s everyday experiences (Marmot et al., 2008).
The ICF-CY and the SDOH bring unique perspectives to understanding health. The ICF-CY considers how a child’s body structures and functions interact dynamically with the environment to result in disability, which is defined as limitations in activity and participation (WHO, 2007). An SDOH perspective is explicitly focused on the cultural, political, racial, and economic structures that directly or indirectly affect people’s health and well-being (Bambra et al., 2009; Braveman, Egerter, & Williams, 2011; Braveman & Gottlieb, 2014). The ICF-CY is a consensus taxonomy put forth by the WHO (2007). Although the SDOH is widely employed in public health, there is no consensus taxonomy akin to the ICF-CY. Both frameworks recognize the dynamic influence of the environment on individuals, reflecting a shared social ecological perspective on health. Yet, the frameworks differ in their approach due to the outcome of interest. The ICF-CY focuses on participation by explicating the individual and environmental factors that affect valued and culturally meaningful participation in everyday life situations. The SDOH perspective is not focused on disability per se but rather explores how multilevel concerns affect a population health outcome, such as disability. Therefore, a thorough understanding of the social ecological context of children’s health and participation requires both the ICF-CY and SDOH.
Young children with DD may be more vulnerable to negative social determinants given their increased need for services and supports (Acevedo-Garcia, Rosenfeld, Hardy, McArdle, & Osypuk, 2013; Marmot et al., 2008). For example, children with DD may require specialized health, educational, and social supports that can be difficult to obtain, especially, if families live, work, and play in a community and policy context that repeatedly exposes them to negative SDOH. Such negative determinants may include insecure and unsafe housing, unreliable transportation, and/or underresourced, low quality schools and organizations/agencies (Acevedo-Garcia et al., 2014). Such determinants could also restrict participation of young children with DD in everyday life situations that provide opportunities for further development such as completing self-care tasks, attending preschool, or developing relationships with peers.
Early childhood is a crucial period in which outcomes have ramifications across the life course. Exposure to suboptimal or adverse conditions, especially for children younger than 3 years, subsequently influences cognition, mental health, health biomarkers, and educational attainment into adulthood (Black et al., 2017; Walker et al., 2011). The recently launched and U.S. federally-funded Early Childhood Comprehensive Systems Collaborative Improvement and Innovation Network emphasizes the necessity of focusing on both social determinants and developmental milestones for children aged 0 to 3 years (Health Resources & Services Administration, 2017; Levesque, Hamilton, & Devlin, 2018; National Institute for Children’s Health Quality, 2018). In the United States, the developmental needs of the youngest children aged 0 to 3 years can be met through EI services that support physical, cognitive, community, social, and adaptive development (Public Law 108-446). Given the latest science, rehabilitation professionals working in EI must also address the relationship between social determinants, participation, and children’s development.
Despite the potential of integrating the ICF-CY and SDOH to improve service systems and developmental outcomes, there is little research exploring the relationship between social determinants and participation of the youngest children with DD aged 0 to 3 years. Such a focus could help systems and professionals identify structural changes that allow for improved outcomes for children with DD and their families.
The purpose of this scoping review is to critically evaluate the literature and describe the social determinants that may affect the participation of young children aged 0 to 3 years with DD. This review focuses explicitly on young children with DD living in the United States. Given the influence of policy, culture, and health systems on both social determinants and participation, an important first step is to better understand the relationship between social determinants and participation for young children living in a specific country. For this work, we define participation for children aged 0 to 3 years as engagement in life situations occurring in the home and community that are essential for positive early development (Chiarello et al., 2012; WHO, 2007). Everyday life situations in the home that may contribute to children’s development include engagement in family routines, self-care routines, play, and familial relationships (Adolfsson, 2013; Case-Smith & O’Brien, 2015; Simeonsson, Scarborough, & Hebbeler, 2006). In addition, participation in the broader community provides important opportunities for development, including outdoor play, attending daycare or preschool, and social interactions with nonfamily members (Adolfsson, 2013; Simeonsson et al., 2006). The review was guided by the following research question:
Method
A scoping review is a useful method to critique the extent, range, and nature of research on a broad topic and to identify new conceptual and methodological directions needed to advance knowledge (Arksey & O’Malley, 2005). In this review, we applied a coding strategy to integrate findings across studies and align them with both an ICF-CY and SDOH framework. This approach allows us to critically evaluate whether social determinants of participation are being explored in research.
We searched three databases that index studies of young children with disabilities from health, rehabilitation, and educational disciplines: PubMed, PsycINFO, and ERIC. In each database, we applied broad keywords in an attempt to capture all literature pertaining to participation (participation, quality of life, inclusion) and our targeted population (parents of young children with disabilities, EI, young children with disabilities). Keywords were replaced with database-specific indexing terms when available. We also conducted hand searches of five targeted journals (Developmental Medicine and Child Neurology; Child: Care, Health and Development; Journal of Early Intervention; Infants and Young Children; Topics in Early Childhood Special Education) and conducted further snowball sampling by searching for articles that cited the ones selected for inclusion or that were cited within included articles. We identified additional literature through consultation with authors whose articles met inclusion criteria (discussed below). Descriptive studies using qualitative, quantitative, and mixed methods approaches were considered for inclusion. We conducted our search in November and December 2016 (one article was In-Press and published in 2017) and completed the literature analysis in 2017.
The following inclusion criteria were applied: (a) Study sample includes children or parents of children with DD, defined as a disability attributable to a mental and/or physical impairment with onset before 22 years of age that is expected to continue and who need support in at least three areas of major life activities (U.S. Developmental Disabilities Assistance and Bill of Rights Act of 2000, Public Law 106-402); (b) At least 2/3 (65%) of the study sample includes children from the United States; (c) At least 20% of the study sample of children with disabilities is aged 0 to 36 months; (d) Data source is parents of children with disabilities or professionals; (e) Study investigated at least one participation outcome aligned with our definition; (f) Published from 2000 through 2016. We chose this time period as it aligns with the likely impact of 1997 (final regulations issued in 1999), 2004, and 2011 IDEA Part C updates, in which mandated changes to EI services could subsequently affect young children’s participation and the conclusions drawn from this review. The literature in this area is limited and has not been explored previously; therefore, the inclusion criteria b, c, and f are sufficiently broad to allow us to capture as many studies as possible, as appropriate for a scoping review. Exclusion criteria included studies examining access to and use of EI services, parents’ participation (e.g., employment), or children with health care needs with no clear developmental disability (e.g., asthma).
Two individuals independently reviewed all abstracts identified in the searches for inclusion criteria. A full text copy of the article was further examined when both reviewers determined the article met all criteria or were unable to determine from the abstract whether all criteria were met for sample characteristics. When reviewers did not achieve consensus, a third reviewer (second author) provided a third, independent evaluation. Figure 1 depicts the article identification and inclusion process.
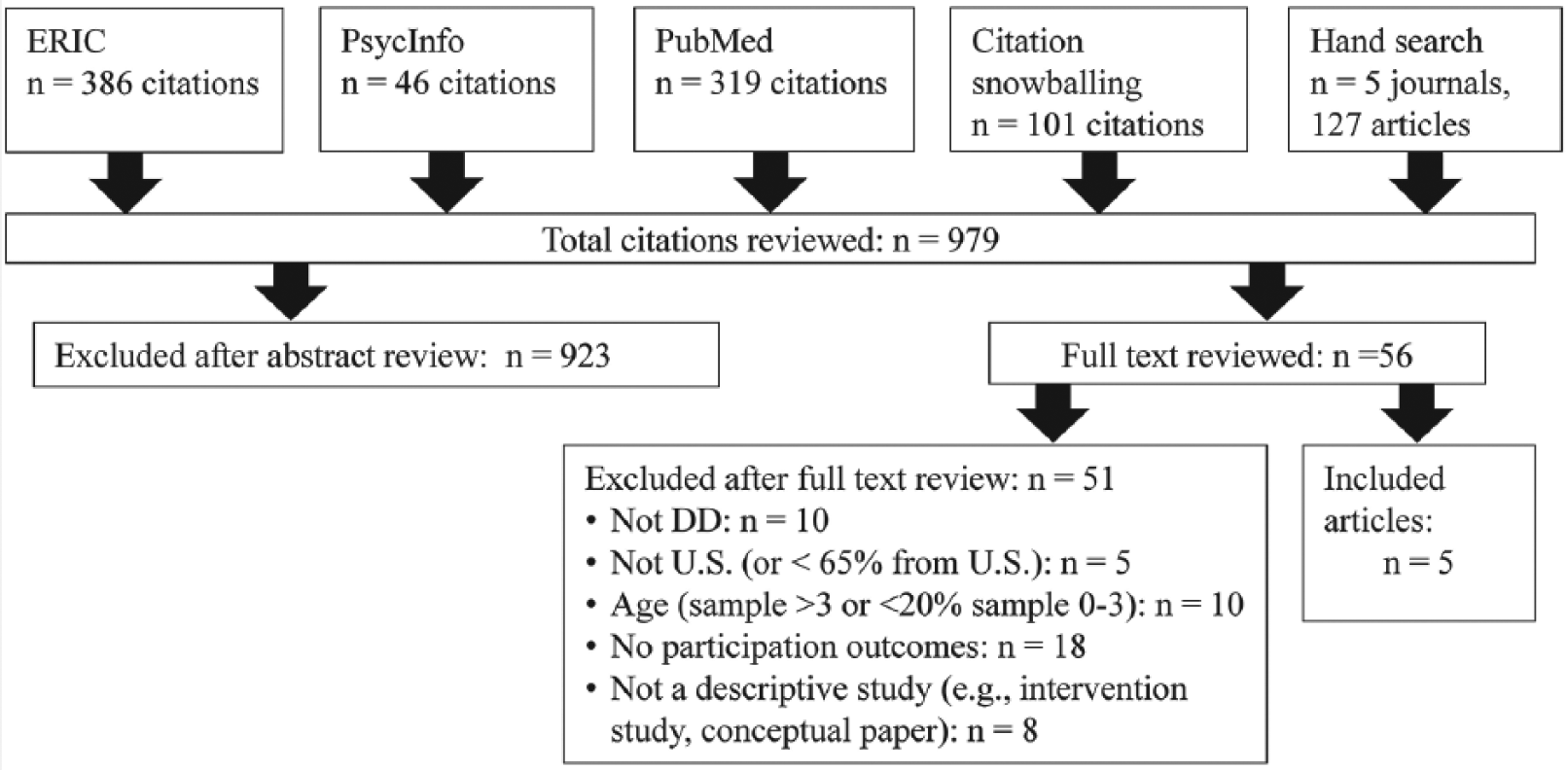
Literature search and inclusion process.
For each included study, information about study aims, sample, methods, operationalization of participation, and findings were extracted and coded by a primary reviewer and confirmed by a second, independent reviewer. A finding was defined as a relationship between the participation outcome and a single variable (i.e., quantitative data) or single idea (i.e., qualitative data). In quantitative studies, we only coded variables associated with statistically significant findings.
First, each finding was coded using the ICF classification system (Adolfsson, 2013; McLaughlin, Snyder, & Algina, 2015). This system includes five environment “chapters” and nested classification codes. Second, findings were grouped into related thematic categories. These categories were created to reflect important details in findings that were not captured in the ICF classification system. Third, categories were then classified as aligned or not aligned with SDOH (Marmot et al., 2008). Fourth, each thematic category was classified by social ecological context: Individual, Immediate/Home, Community, or Policy (Marmot et al., 2008; WHO, 2007).
Results
Description of Articles
The search process retrieved 979 articles of which 923 were excluded. After review of 56 full articles, an additional 51 articles were excluded, for a total of 5 articles (Table 1). Included articles were published between 2011 and 2017, suggesting that this area of research is emerging. One research team (identified by the consistent involvement of one key scholar, Khetani) produced three included articles.
Included Articles’ Study Aims and Methods for Investigating Participation.
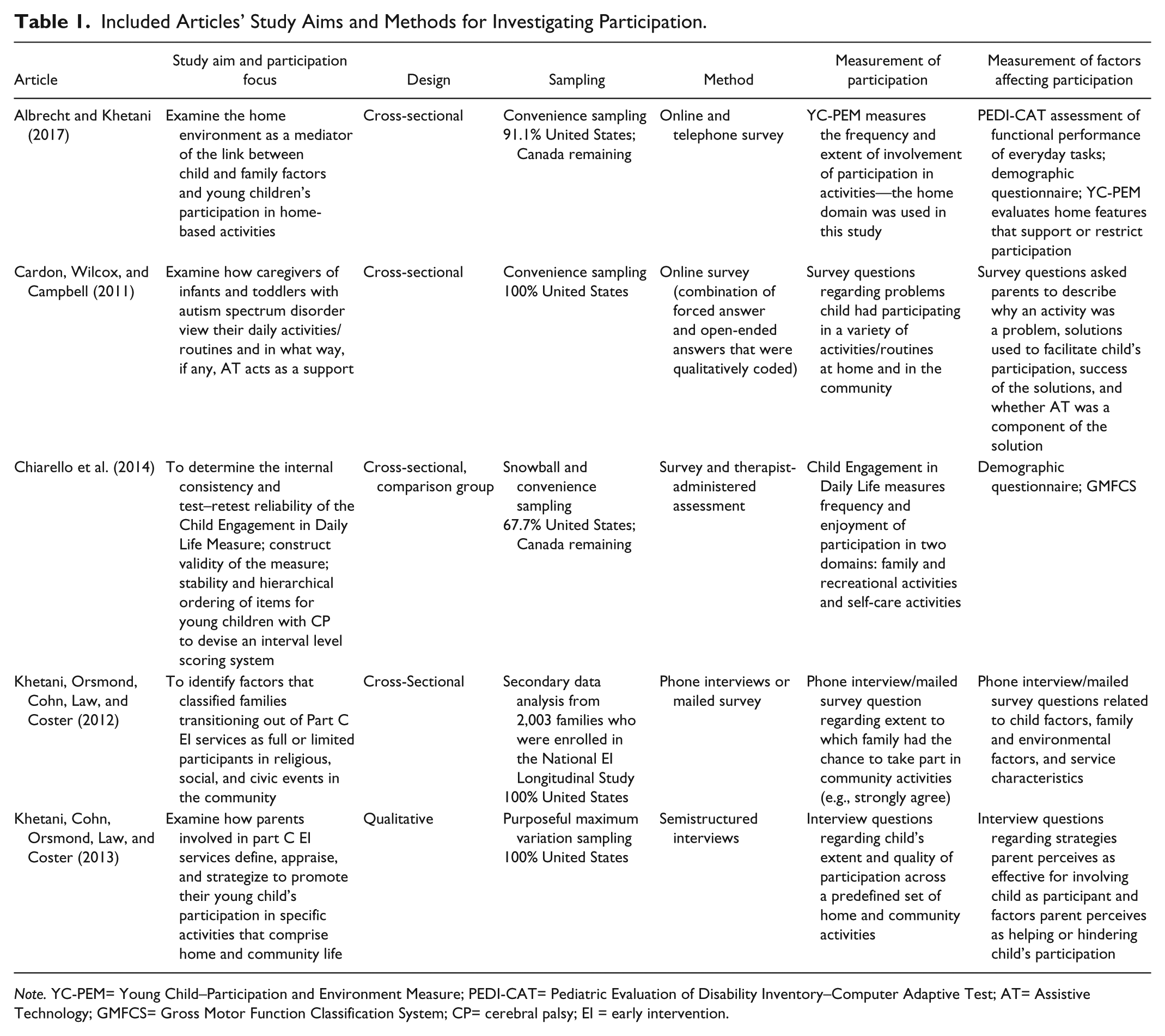
Note. YC-PEM= Young Child–Participation and Environment Measure; PEDI-CAT= Pediatric Evaluation of Disability Inventory–Computer Adaptive Test; AT= Assistive Technology; GMFCS= Gross Motor Function Classification System; CP= cerebral palsy; EI = early intervention.
Outcome measures
The measurement of participation and factors affecting participation varied among the included articles (Table 1). Three studies (Cardon, Wilcox, & Campbell, 2011; Khetani, Cohn, Orsmond, Law, & Coster, 2013; Khetani, Orsmond, Cohn, Law, & Coster, 2012) used semistructured interview or survey questions; the questions were unique to each study. Two studies measured participation using validated instruments: the YC-PEM (Albrecht & Khetani, 2017) and the Child Engagement in Daily Life (Chiarello et al., 2014). These measures were specifically developed to assess participation of young children; these studies also used other gold standard instruments to measure factors associated with participation.
Description of Participants
The ages of the children in the included samples ranged from 1 to 3 years (Table 2). In four articles, children aged 3 years and younger (≤36 months) were a subsample of participants that also included children up to 5 years old; only the Cardon and colleagues (2011) sample was comprised solely of children ≤3 years old. The nature of the disabilities and diagnoses included in the articles varied and reflect the unique diagnostic approach used with young children. Two articles (Albrecht & Khetani, 2017; Khetani et al., 2012) only specified the percentage of the participants qualifying for services under a general developmental delay versus a diagnosed condition but did not report specific details about the children’s diagnoses. The one qualitative study used purposeful sampling to include children with a range of qualifying conditions (Khetani et al., 2013). The remaining articles comprised a condition-specific sample: autism and cerebral palsy (Cardon et al., 2011; Chiarello et al., 2014). All studies included more male participants, which reflects the pattern of EI usage and diagnostic prevalence by gender (Rosenberg, Robinson, Shaw, & Ellison, 2013; Scarborough et al., 2004). Finally, the informant for most of the studies was the mother of the child with the disability.
Included Articles’ Sample Characteristics.
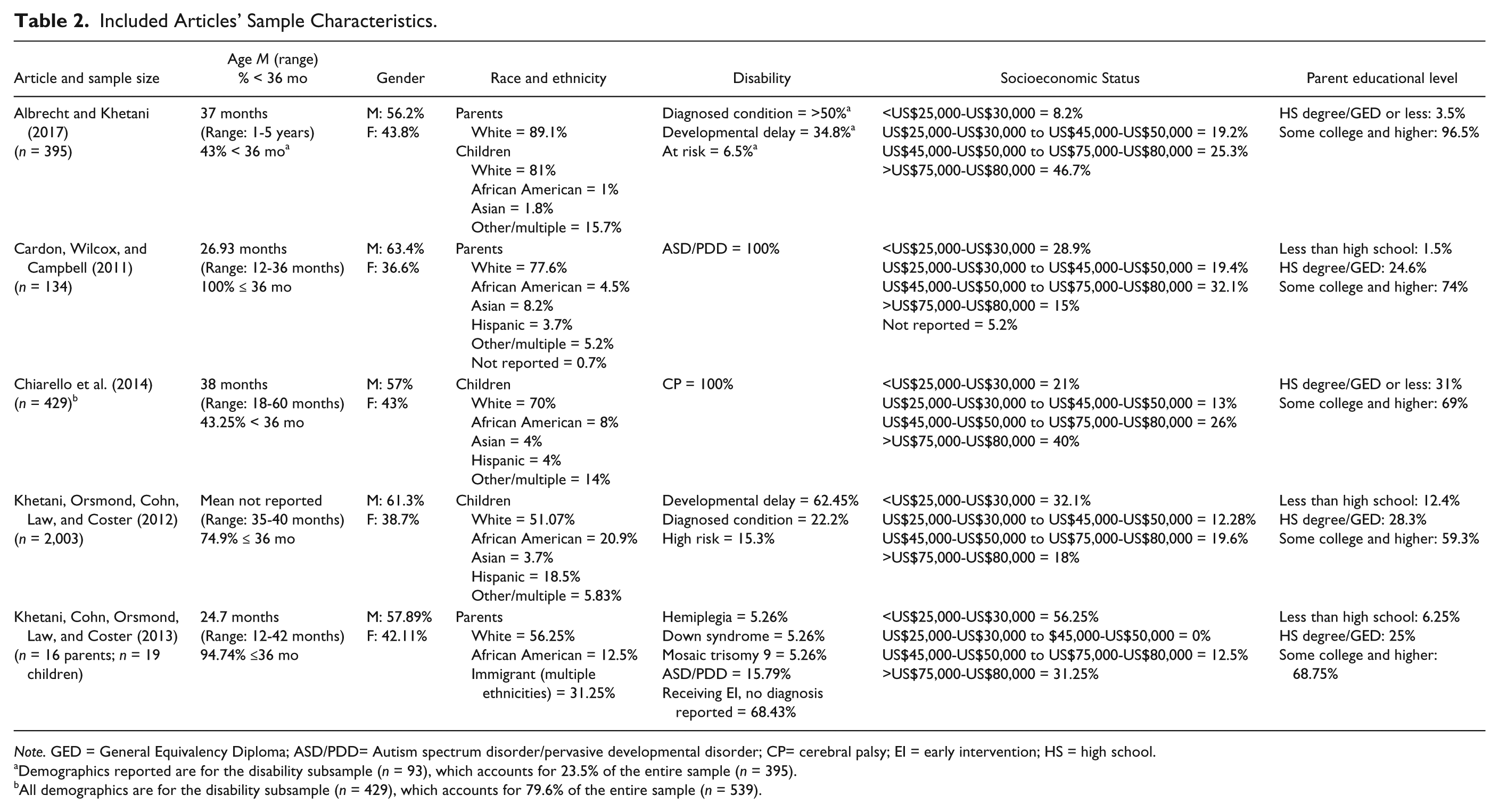
Note. GED = General Equivalency Diploma; ASD/PDD= Autism spectrum disorder/pervasive developmental disorder; CP= cerebral palsy; EI = early intervention; HS = high school.
Demographics reported are for the disability subsample (n = 93), which accounts for 23.5% of the entire sample (n = 395).
All demographics are for the disability subsample (n = 429), which accounts for 79.6% of the entire sample (n = 539).
Across all studies, the majority of participants identified as Caucasian/White (from 51%-89%). All studies included children from families with a broad range of household incomes. Across all studies, 8% to 56% of the participants reported an annual household income of <US$30,000. However, all studies also included families with significantly higher annual incomes, with 15% to 46% reporting more than >US$75,000 annually. Parental educational levels were generally high across studies: 59% to 96% of parents reported attending or completing college, whereas 1.5% to 31% of parents reported a high school/General Equivalency Diploma (GED) or less.
Determinants of Participation of Young Children With DD
Across studies, the determinants of participation stemmed from the child (e.g., individual) as well the immediate, community, and policy social contexts (Table 3). Five articles reported a relationship between the individual level (e.g., child) and participation. Examples of the individual level include child’s body structures and function (e.g., sensory system), the child’s functional performance (e.g., self-care, communication), and the child’s interests and preferences; these factors are not social determinants. Three articles (Albrecht & Khetani, 2017; Khetani et al., 2013; Khetani et al., 2012) found relationships between social determinants stemming from the immediate (e.g., home) context and participation including parent’s educational attainment, financial commitments to extended family members, supportive family relationships, and the sensory qualities of the home. The same three articles also found social determinants stemming from the community context and participation. Examples include service provider attitudes about disability, the availability of information regarding activities and programs, and the support of friends (Albrecht & Khetani, 2017; Khetani et al., 2013; Khetani et al., 2012). Two articles (Albrecht & Khetani, 2017; Khetani et al., 2013) reported relationships between social determinants stemming from the policy context and the participation of young children with disabilities. Examples include housing policies, transportation availability and quality, employment policies regarding flexibility in scheduling work time and location (telecommuting), and the availability of programs and services for young children with disabilities and their families.
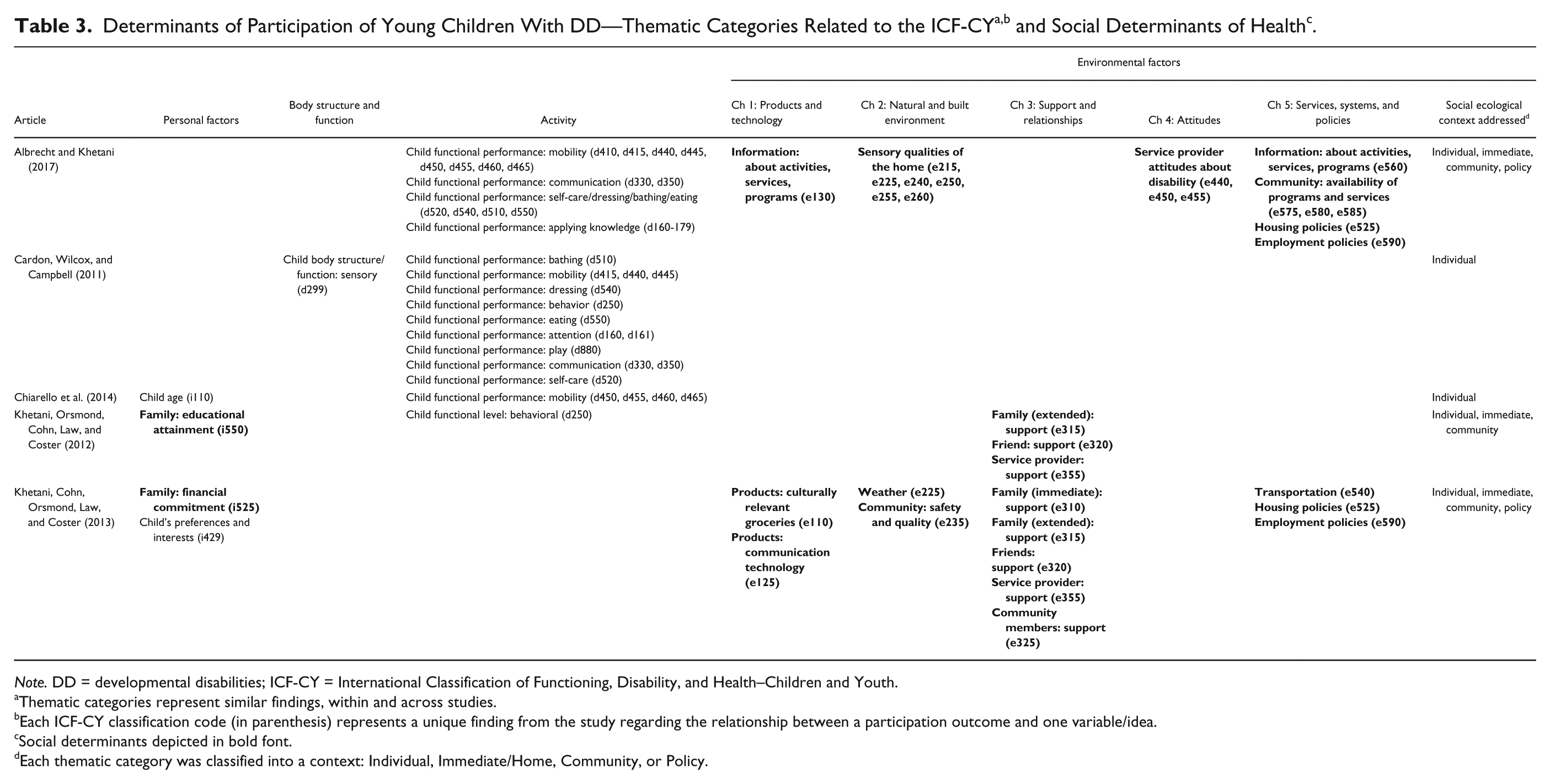
Note. DD = developmental disabilities; ICF-CY = International Classification of Functioning, Disability, and Health–Children and Youth.
Thematic categories represent similar findings, within and across studies.
Each ICF-CY classification code (in parenthesis) represents a unique finding from the study regarding the relationship between a participation outcome and one variable/idea.
Social determinants depicted in bold font.
Each thematic category was classified into a context: Individual, Immediate/Home, Community, or Policy.
Discussion
The emergent literature exploring the relationship between social determinants and participation of young children with DD aged 0 to 3 years in the United States suggests participation may be affected by multiple “spheres of influence” including immediate, community, and policy contexts. However, the breadth and depth of literature is generally limited, especially considering structural factors stemming from the U.S. community and policy context. Overall, the literature focuses on a “medical” model of disability and children’s impairments rather than a comprehensive, multilevel focus on the social ecological nature of children’s health and participation as framed by the ICF-CY and the SDOH.
In addition, study sample populations likely reflect gaps in our understanding of how structural factors influence the participation of diverse children in the United States. These samples likely underrepresent families of children with DD identifying as racial/ethnic minorities, reporting lower incomes and reporting lower levels of educational achievement. Such children may be more likely to be affected by negative SDOH. For example, in the United States, children living in poverty are more likely to be diagnosed with DD, and African American and Latino children are less likely to receive services even when eligible (Feinberg, Silverstein, Donahue, & Bliss, 2011; Magnusson, Minkovitz, Kuhlthau, Caballero, & Mistry, 2017; Magnusson, Palta, McManus, Benedict, & Durkin, 2016; Rosenberg et al., 2013; Rosenberg, Zhang, & Robinson, 2008). Two studies in our review recruited a broader sample and therefore were better able to explore the relationship between social determinants and participation (Khetani et al., 2013; Khetani et al., 2012). Yet, specific diagnoses of children were also unclear in many of the studies. This variation in sample population and results makes it difficult to draw final conclusions; certainly, further research is needed to explore the ways in which equitable participation for all children, particularly, children with DD, is shaped by specific disabilities, race/ethnicity, socioeconomic status, and more.
Also evident from this review is the need for high quality measures of participation for young children with DD. The field of pediatric rehabilitation will be stymied in further exploring the relationship between social determinants and children’s participation if we lack the tools to measure the quality of participation. Two newly designed measures, the Young Child–Participation and Environment Measure (YC-PEM, Khetani, Graham, Davies, Law, & Simeonsson, 2015) and the Child Engagement in Daily Life (Chiarello et al., 2014), assess participation at the home and community levels. Both measures have the potential to provide an understanding of the relationship between social determinants and participation as they avoid operationalizing participation only as frequency of engagement. A common critique of participation measures is the assumption that more frequent participation represents the “optimal” or more desired outcome (Heinemann et al., 2010). Rather, these measures provide a more nuanced understanding of participation by assessing frequency of participation along with level of engagement and satisfaction, or with enjoyment of participation. Assessing participation from these multiple viewpoints including frequency, engagement, and satisfaction (Imms et al., 2016) provides new opportunities to conduct rigorous research that documents the needs and current participation experiences of young children with DD in relationship to SDOH.
Together, the ICF-CY and SDOH provide a more robust understanding of the factors that affect participation of young children with DD. Take the example of children with DD living in areas with public transportation that meets the regulations put forth by the Americans with Disabilities Act of 1990 (Public Law No. 101-336). An SDOH analysis might suggest that the regulations (e.g., policy) positively affect child health, whereas an ICF-CY analysis might suggest that increased community mobility and subsequent participation in community, social, and health activities are driving improved child health. Together, we have a full picture. In addition, the ICF-CY considers aspects of the environment that may not be considered in traditional SDOH research. For example, the participation of children with DD may be affected by weather, the availability of adaptive technology, and the built environment (e.g., the presence of stairs; Hammel et al., 2015). These aspects of the environment may be instrumental in optimizing the participation and development of young children with DD. Finally, the ICF-CY provides those using a SDOH framework a more robust approach to conceptualizing and measuring function and participation at the individual as well as population level (McLaughlin et al., 2015; Simeonsson et al., 2006). By incorporating the ICF-CY, SDOH research can go beyond the health outcomes measurement (e.g., presence or absence of disease) or developmental status (e.g., meeting development milestone expectations) and explore participation as the primary outcome of interest (Adolfsson, 2013).
Implications for Practice
EI professionals routinely consider the impact of the environment on the development and participation of children with DD. For example, they suggest home and activity modifications that can foster participation and independence (Campbell, Milbourne, & Wilcox, 2008) and provide parents and siblings with strategies to support social interactions and positive relationships (Vivanti, Dissanayake, & The Victorian ASELCC Team, 2016; Zwaigenbaum et al., 2015). Yet, it is equally critical to consider the impact of community and policy contexts on the child and their family. Results of this review suggest some families may be unable to access community social events, health care, or other educational services because of transportation restrictions or the parents’ employer policies regarding family leave or paid sick days. Barriers stemming from these contexts may be less frequently considered as within EI professionals’ scope of practice, despite their potential negative impacts on children’s long term development and equitable participation. EI professionals play a vital role in helping families identify barriers stemming from these contexts and connecting families with resources and supports to resolve such barriers (Dunst & Bruder, 2002). Incorporating the ICF-CY and SDOH to create a guiding framework during evaluation and intervention planning can direct professionals to precisely evaluate and take action on the root causes of barriers to participation. Two newly designed measures of participation included in this review, the YC-PEM (Khetani et al., 2015) and Child Engagement in Daily Life (Chiarello et al., 2014) can help such professionals to assess current challenges and family goals for young children’s engagement at home and in the community.
Limitations and Future Research
Several limitations exist in our review. First, studies were excluded if the sample comprised <20% of children below the age of 36 months, even though the studies may have generally focused on participation of children and related social determinants. Second, we attempted to capture as many studies as possible that included children with DD aged 0 to 3 years in the United States; as a result, two studies also included data from children living in Canada and four studies included data from children up to 5 years of age. We were unable to extract factors associated with participation only for children meeting our age and origin inclusion criteria. Finally, we did not evaluate included articles for risk of bias, given our aim to include all available information in this initial scoping review; results therefore do not account for study quality beyond being published in the peer-reviewed literature.
Social determinants may affect participation of young children differently, depending on country and age. Therefore, future research must explore potential differences across countries and age groups and compare the relative impact of social ecological factors on participation and developmental outcomes to identify the social and service systems that foster the best outcomes for all children (Braveman & Gottlieb, 2014).
Conclusion
This scoping review provided a useful, though preliminary, understanding of the relationship between social determinants and the participation of children ages 0 to 3 years with DD in the United States. The dual application of the ICF-CY and SDOH frameworks, with their shared social ecological framing, could lead to research and practice that reveals how multiple contexts, including the immediate, community, and policy environments, can support optimal development and equitable participation for all children.
Footnotes
Acknowledgements
We would like to thank research assistants Justine Zayhowski, I-Ting Hwang, and Cara Dart for their diligent work with this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the American Occupational Therapy Foundation’s Intervention Research Grant (AOTFIRG14, PI: Kramer).
Research Ethics
Human subjects protections and review is not applicable to this scoping review.