
Abstract
Adults with type 2 diabetes (T2D) experience decline in cognitive function compared with controls. Cognitive function is a major component in the performance of daily activities that involve motor components. The aim of this project was to evaluate working memory cognitive deficits and sensorimotor deficits in adults with T2D versus healthy participants. Ten community-dwelling persons with T2D and 10 age- and sex-matched healthy controls were recruited. Cognitive function, tactile function, motor function, and health state measures were evaluated. Reduced cognitive function, tactile function, and motor function were exhibited in the T2D group. Cognitive and motor functions remained impaired versus controls during tasks with both cognitive and motor components (dual tasks). Health state measures were found to covary with measures of interest. The conclusions of this article are as follows: (a) systemic deficits beyond tactile dysfunction contribute to reduced hand/finger function in T2D, and (b) participants with T2D demonstrate impairments in working memory, tactile function, and motor function.
Introduction
More than 422 million (8.5%) individuals worldwide over the age of 18 are currently living with type 2 diabetes (T2D; “Diabetes,” n.d.). Recent work suggests that T2D and cardiovascular disease (CVD) share an underlying constellation of causes, a theory known as the “common soil” hypothesis (Lebovitz, 2006). Common CVD complications of T2D include coronary heart disease, large vessel atherosclerosis, stroke, nephropathy, and neuropathy (Grundy et al., 1999). Recent evidence suggests that in addition to these well-known complications, adults with T2D experience decline in cognitive functions (mild cognitive impairment, MCI) compared with individuals without T2D. MCI is defined as a slight, yet noticeable and measurable decline in cognitive abilities (“Mild Cognitive Impairment—Signs, Symptoms, & Diagnosis,” n.d.) that may be present in different domains such as memory or executive function. The risk of developing MCI increases with age, such that persons over the age of 60 are at increased risk, with persons over the age of 60 and living with T2D at an even higher risk than individuals without T2D (Biessels, Deary, & Ryan, 2008; Creavin et al., 2011; Fontbonne, Berr, Ducimetière, & Alpérovitch, 2001; Strachan, Reynolds, Marioni, & Price, 2011; van den Berg et al., 2008). Underlying CVD with poor glucose control has been cited as the source of MCI development in patients with T2D (Biessels, Strachan, Visseren, Kappelle, & Whitmer, 2014; McNay & Recknagel, 2011).
Cognitive deficits have been defined by impairment in one or more cognitive domains (Bennett et al., 2002; Meyer, Xu, Thornby, Chowdhury, & Quach, 2002). Failure in specific domains, such as working memory, has been recently documented in T2D patients (Christman, Vannorsdall, Pearlson, Hill-Briggs, & Schretlen, 2009; Creavin et al., 2011), whereas all other domains (beyond working memory) appear to remain intact. Cognitive impairment adversely affects the ability to manage complex daily T2D self-management tasks such as meal preparation, taking medications, and exercise (Christman et al., 2009; Gold, 2012; Vance, Larsen, Eagerton, & Wright, 2011). Many of these self-care tasks involve the use of one or both upper extremities; reduced upper extremity function thus presents significant challenges in maintaining self-care routines.
In addition to observing differences in cognitive function, there are also apparent differences in sensory function (e.g., tactile function) and motor function in people with and without T2D. Tactile and motor functions of all four extremities are impaired in persons with T2D (Gorniak, Khan, Ochoa, Sharma, & Phan, 2014; Ochoa, Gogola, & Gorniak, 2016; Ochoa & Gorniak, 2014). Patients have poor awareness of their cognitive, tactile, and motor changes, leading to resistance of aid in managing daily tasks (Christman et al., 2009). The aggregation of these cognitive, tactile, and motor changes presents major challenges in clinical management and self-care of T2D.
Currently, little is known about cognitive–motor deficits (also known as cognitive–motor interference, CMI) in adults with T2D. CMI is defined as a deterioration in the performance of cognitive and/or motor tasks during simultaneous performance of cognitive and motor tasks (Plummer et al., 2013). CMI is associated with loss of functionality in daily life, including reduced ability to perform essential self-care tasks such as meal preparation and taking one’s medication (Chen, Leys, & Esquenazi, 2013). CMI has been documented in other populations with CVD (e.g., stroke; Chen et al., 2013; Dennis et al., 2011). Similar deficits have been found in a number of patient populations, particularly in cases where only motor deficits were clinically assumed (e.g., Parkinson’s disease; Frankemolle et al., 2010). Previously, we have found CMI in adults with T2D during tasks involving whole body balance (Gorniak, Lu, Lee, Massman, & Wang, 2019) in which participants stood upright on a force platform and responded to auditory stimuli which stimulated participants’ short-term memory. However, we have not probed for CMI in adults with T2D during performance of hand/finger tasks, despite evidence of subtle hand/finger motor impairment in patients living with T2D (Gorniak et al., 2014; Ochoa et al., 2016; Ochoa & Gorniak, 2014).
Accordingly, the goal of this study was to explore potential CMI in persons with T2D during a task with working memory components (cognitive task) and a motor task involving the upper extremity. As force control has been linked to reduced manual dexterity and self-care, we tested upper extremity motor function via force production control (Cole, Rotella, & Harper, 1999; Kilbreath & Heard, 2005). This study was a first step toward understanding the specific challenges in CMI with respect to hand/finger tasks in persons with T2D. Specifically, we hypothesize that (a) persons with T2D will demonstrate impairment in baseline evaluations and in cognitive, tactile, and motor tasks as compared with healthy age- and sex-matched controls, and (b) persons with T2D will demonstrate further impairment in one or both the cognitive and motor domains during dual tasks compared with healthy age- and sex-matched controls. No hypotheses regarding changes in cognitive and motor performance with disease state were developed a priori, as exploration of deterioration with disease state was an exploratory aim of this study.
Materials and Methods
Participants
Ten right-handed individuals with T2D voluntarily participated in this study (four men and six women). Ten right-handed healthy age- and sex-matched controls also participated in each of the evaluations as a control comparison group. Handedness was determined by the Edinburgh Inventory (Oldfield, 1971). The sample size used in this study was determined via a power analysis based on previous work in T2D manual dysfunction (Gorniak et al., 2014; Ochoa et al., 2016; Ochoa & Gorniak, 2014). Measures of approximate entropy (ApEn) and coefficient of variation (CV; Gorniak et al., 2014) were used in our power analysis (ApEnT2D = 0.24 [unitless], ApEnControls = 0.38 [unitless], ApEn common standard deviation = 0.12 [unitless]; CVT2D = 0.073 [unitless], CVControls = 0.032 [unitless], CV common standard deviation = 0.025 [unitless]). Both measures indicated that an n = 10 per group would provide power of 0.8 with α = .05.
Table 1 contains the patient demographics, and Table 2 contains the control participant demographics. Study participants were excluded if they had a history of other confounding neuromuscular disorders (e.g., stroke, Parkinson’s disease, etc.). Participants with T2D had a confirmed diagnosis of T2D either with or without diagnosis of peripheral neuropathy (PN) per physician. All study procedures were carried out in a quiet environment. Participants provided written informed consent in accordance with the procedures provided by the Institutional Review Boards of the University of Houston and University of Texas Health Science Center at Houston.
Demographic and Clinical Characteristics of T2D Participants.
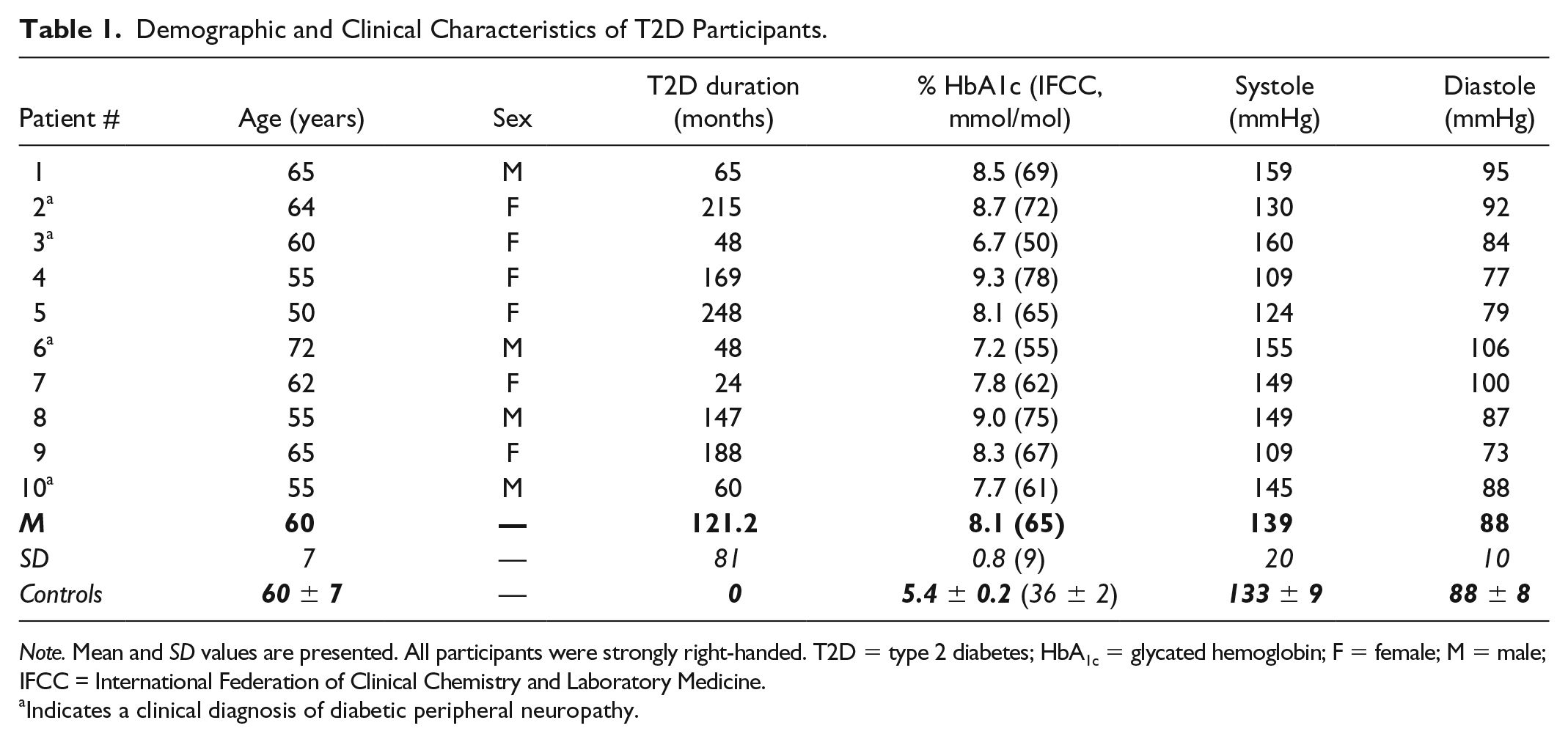
Note. Mean and SD values are presented. All participants were strongly right-handed. T2D = type 2 diabetes; HbA1c = glycated hemoglobin; F = female; M = male; IFCC = International Federation of Clinical Chemistry and Laboratory Medicine.
Indicates a clinical diagnosis of diabetic peripheral neuropathy.
Demographic and Clinical Characteristics of Control Participants.
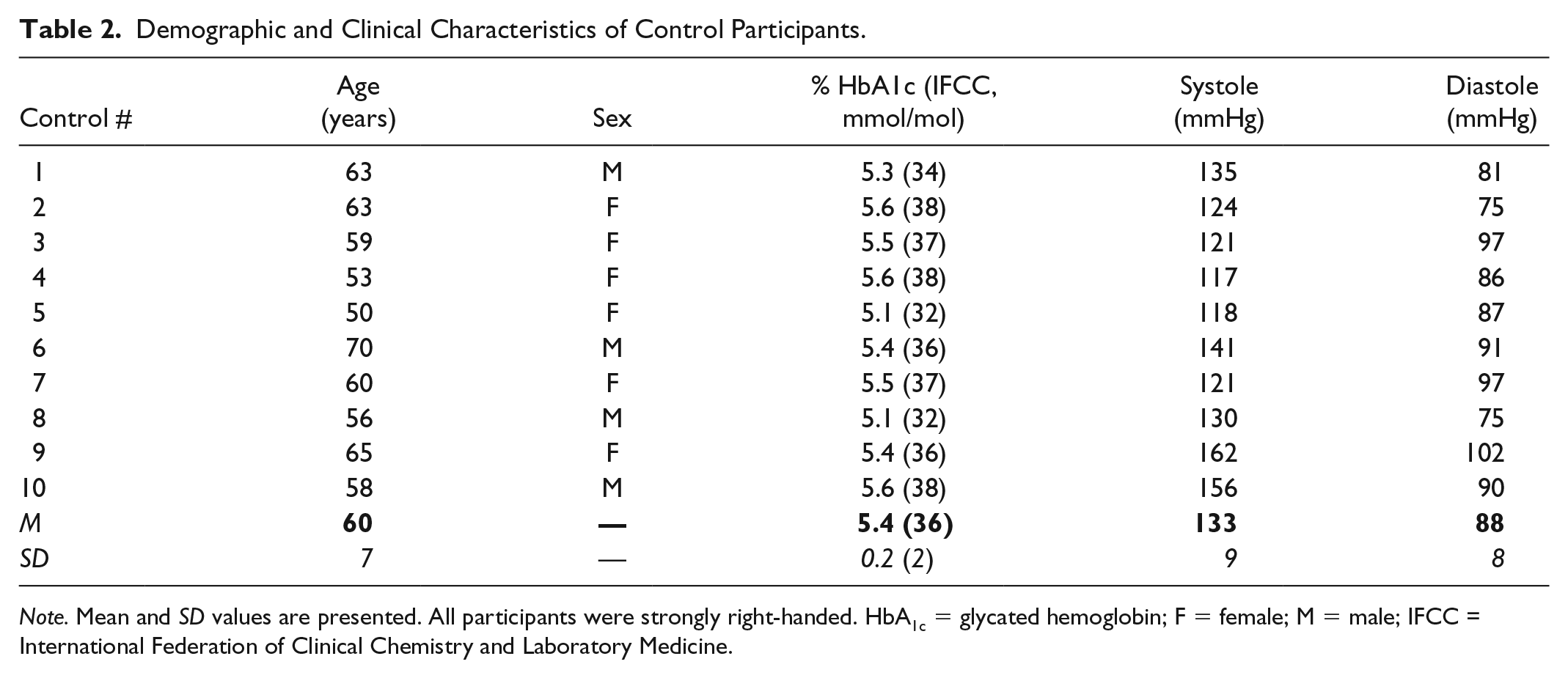
Note. Mean and SD values are presented. All participants were strongly right-handed. HbA1c = glycated hemoglobin; F = female; M = male; IFCC = International Federation of Clinical Chemistry and Laboratory Medicine.
Health Status Information
Blood pressure and glycated hemoglobin (HbA1c) values were assessed for all study participants on site. HbA1c values were assessed using a commercially available point of care evaluation kit (HbA1c Now+; PTS Diagnostics, Indianapolis, IN, USA). Blood pressure was measured 5 to 10 min after the informed consent process while participants were resting in a seated position, using a commercially available device (Omron Intellisense 10 series Blood Pressure Monitor, Model BP785, Bannockburn, IL, USA). The presence of PN (PN status) was determined by abnormalities on either clinical examination or electromyography/nerve conduction study testing (per physician).
Tactile Evaluation
Tactile sensation of the hands was tested using the Semmes Weinstein Monofilament Test as per the recommendations made in the study by Bell-Krotoski (1990). Tactile function testing sites for the hand consisted of the tip of digit 1 (median nerve) and the tip of digit 5 (ulnar nerve). During the test, participants kept their eyes closed and verbally indicated if and where they perceived the monofilament. The monofilament size was increased until the subject was able to detect light touch a minimum of two times at the same location.
Cognitive Evaluation
Montreal Cognitive Assessment
Cognitive function of each participant was screened using the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005). This brief cognitive examination is used to evaluate the cognitive domains of attention and concentration, executive function, memory, verbal fluency, visuoconstructional skills, conceptual thinking, calculations, and orientation. Number of years of patient education is accounted for within the MoCA scoring structure.
Working memory (N-back) evaluation
Working memory of each participant was probed using the N-back evaluation. This test required participants to repeat the “Nth” word back in a list of random words. Three conditions of the N-back task were assigned to each subject (0, 1, and 2 back). Presentation of conditions was block randomized across participants. Participants wore a headset with headphone/microphone capabilities (Plantronics Inc., Santa Cruz, CA, USA), through which they heard a randomized sequence of words every 4 s generated by custom software (Visual C++; Microsoft Corp., Redmond, WA, USA; Gorniak et al., 2019). Participants were instructed to repeat the words into the headset in the correct sequence for a task duration of three 30 s trials for each condition. Working memory function was probed at baseline (single task) as well as during motor function evaluations (dual task). All single tasks occurred prior to dual tasks to avoid confusion. The percentage of correct responses and verbal reaction time were recorded by the Visual C++ software and extracted to evaluate performance. Three trials were collected in each of the N-back conditions for both single and dual task evaluation.
Motor Evaluation
Maximal pinch strength was assessed using a pinch dynamometer and wireless DataLOG system (Precision Pinchmeter P200, DataLOG model MWX8; Biometrics Ltd., Newport, UK). Three trials were conducted on the dominant hand. The greatest value of the three was documented as the maximum voluntary contraction (MVC). Consistent with previously documented protocol (Gorniak et al., 2014; Ochoa et al., 2016; Ochoa & Gorniak, 2014), the pinchmeter was placed 16 in. anterior to the patient torso, 6 in. away from the midline of the body toward the dominant (right) hand. The wrist orientation was such that the hand was in a neutral position (neutral flexion/extension, neutral radial/ulnar deviation, and neutral pronation/supination) during testing. Hand orientation was maintained during testing. The arms were unsupported during testing. The same table and chairs were used during each testing session.
A submaximal force production task (described by Gorniak et al., 2014; Ochoa et al., 2016) was conducted to measure force production of digits 1 and 2 with feedback via a computer screen. All forces and moments of force were measured and recorded simultaneously (Nano-25; ATI Industrial Automation, Garner, NC, USA). While performing the task, participants sat with erect posture in a chair facing a small table. Two different force production levels were tested: 15% and 40% of MVC. The 15% and 40% MVC values were calculated from MVC. Each subject participated in three trials per condition with trials lasting 30 s each. Participants were required to reach and maintain the designated force production level within the first 5 s of each trial. Data shown in the results are averaged across the three trials per condition. Four conditions were tested within each force production level in the submaximal task. The first was a quiet sitting controlled condition to assess baseline motor function. Afterward, three dual task conditions were evaluated using the 0, 1, and 2 back working memory evaluation in a block randomized manner.
Force data collected via the ATI transducers were amplified and multiplexed using ATI hardware prior to being routed to an analog to digital converter (via cDAQ-9174 chassis and NI-9205 input modules; National Instruments, Austin, TX, USA). Customized Labview programs (National Instruments, Austin, TX, USA) were used for data acquisition, and customized MATLAB (Mathworks Inc., Natick, MA, USA) programs were written for data processing. Signals were sampled at 100 Hz and low-pass filtered at 10 Hz using a second-order, zero-lag Butterworth filter.
Kinetic analyses
Submaximal force production data were analyzed with respect to both linear (via root mean square error [RMSE] and CV) and nonlinear measures (via ApEn and detrended fluctuation analysis [DFA]). Details regarding these analyses can be found in the studies by Gorniak et al. (2014), Ochoa et al. (2016), and Ochoa & Gorniak (2014).
Statistics
The data are presented in the text and figures as mean ± standard errors. Repeated measures analyses of variance (RM-ANOVAs) were performed on all data with the main factors of Group (two levels; T2D or Control). Evaluation of additional factors was included in test-specific RM-ANOVA analyses: Condition (three levels for N-back: 0, 1, and 2 back), Task (two levels: single or dual task), Site (two levels for the monofilament test: median and ulnar nerves), and Level (two levels for the submaximal test: 15% and 40% MVC). Follow-up analyses of covariance (ANCOVAs) were performed using health state measures of HbA1c, duration of diagnosis, diagnosis of PN (via indicator variable), and monofilament data as covariates to investigate the relationship between disease state indicators and observed cognitive, tactile, and motor function measures. In the event of significant covariates, follow-up correlation analyses were performed between the health state measure and the observed cognitive, tactile, and motor function data of interest. Monofilament data were log transformed prior to analyses, due to nonlinearity and heteroskedasticity. Non-transformed data are shown in figures to clarify study procedures. In multiple comparison situations, Bonferroni corrected post hoc was used.
Results
Health State Measures
A summary of health state measures for each study participant is given in Tables 1 and 2. Briefly, Group-based differences were found in HbA1c, F(1, 17) = 102.34, p < .001, but not in blood pressure measurements. A sex-based difference was found in Systole, F(1, 17) = 5.94, p < .05, but not in Diastole.
Tactile Evaluation
Significant impairment in tactile detection thresholds was found in the T2D group as compared with controls via RM-ANOVA (Group: F(1, 24) = 23.1, p < .001; Figure 1a). Tactile detection threshold values did not differ between tested sites. None of the patient health state measures were found to covary with tactile detection thresholds, including PN status.
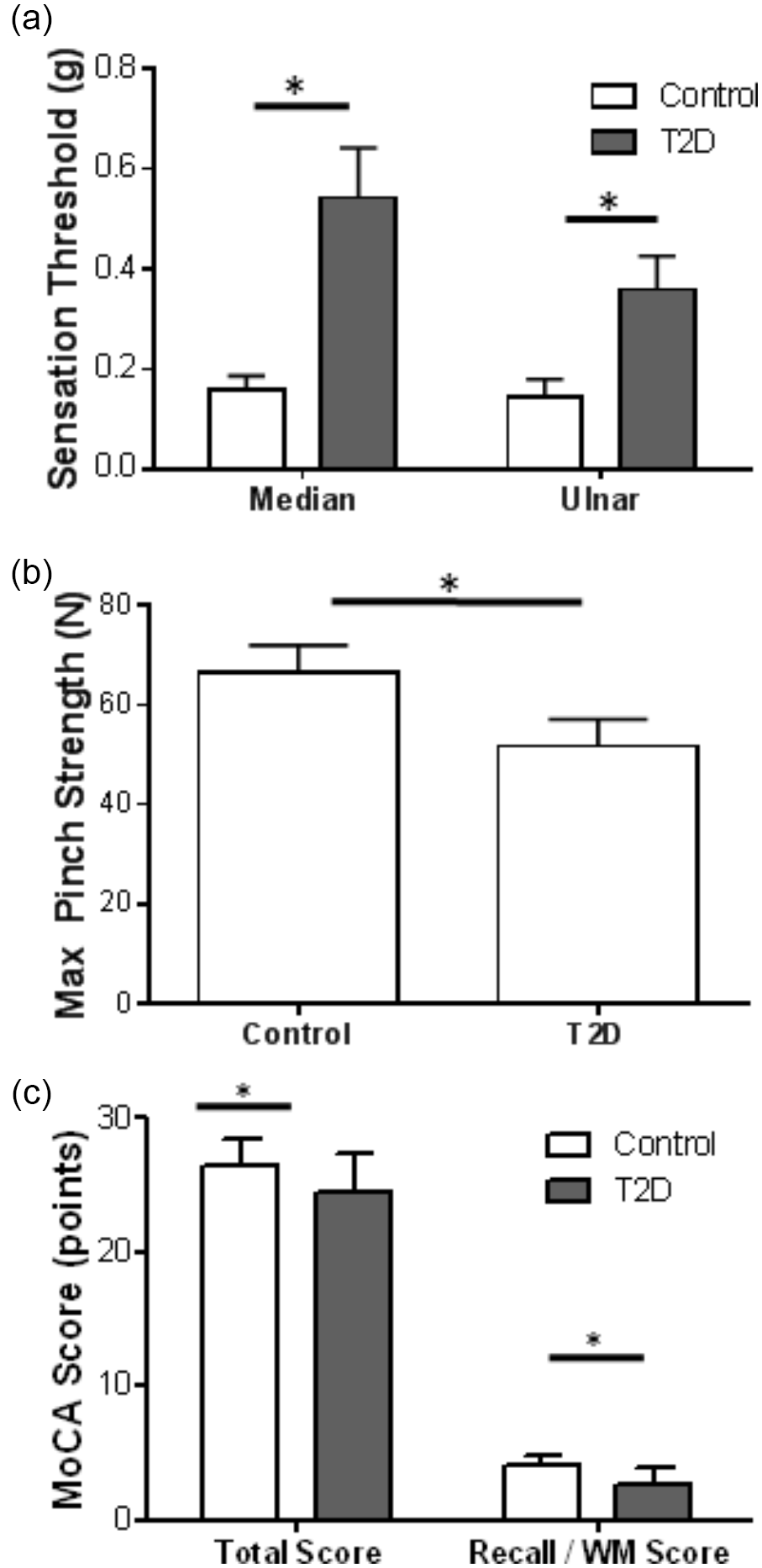
Mean and standard error for tactile detection thresholds, maximal force production, and cognitive function data.
Maximal Force Production
Between Group, F(1, 9) = 6.26, p < .05, differences emerged via RM-ANOVA indicating reduced pinch strength in T2D patients (Figure 1b). A covariate effect of Systole was found, F(1, 8) = 6.78, p < .05, via ANCOVA, enhancing the Group effect. Bivariate correlation analysis indicated that pinch strength was increased with Systole (r20 = .41, p < .05). Partial correlation accounting for Group status enhanced the positive relationship between pinch strength and Systole (r17 = .50, p < .05).
Cognitive Function
MoCA
RM-ANOVA of MoCA results indicated a significant Group difference, F(1, 9) = 6.56, p < .05, such that total MoCA scores were lower on average in the T2D group versus controls (Figure 1c). ANCOVA of the total MoCA scores with health status covariates indicated a significant effect of Systole, F(1, 8) = 20.43, p < .05, while a Group difference, F(1, 8) = 8.77, p < .05, persisted. Bivariate correlation indicated a negative relationship between total MoCA score and Systole (r20 = −.438, p < .05). Partial correlation accounting for Group status enhanced the negative relationship between total MoCA score and Systole (r17 = −.587, p < .005).
RM-ANOVA of each MoCA domain revealed Group differences only in the recall/working memory domain, F(1, 9) = 10.74, p < .05, such that scores exhibited by T2D patients in the working memory/recall were significantly lower than controls (Figure 1c). ANCOVA of the working memory/recall domain MoCA scores with health status covariates indicated a significant effect of Diastole, F(1, 8) = 6.71, p < .05, whereas the Group difference, F(1, 8) = 18.75, p < .005, was magnified. Correlation analyses did not yield significant results based on Group and Diastole differences in working memory/recall.
N-back/working memory
ANCOVA revealed a trend toward a Group difference, F(1, 145) = 3.029, p = .08, and significant effects of Condition, F(2, 145) = 47.83, p < .001, and Task, F(1, 145) = 5.68, p < .05, on reaction time, indicating that reaction time of the T2D group was longer (Figure 2a). The data also indicate that reaction time increased with N-back difficulty but was lower in dual task conditions (Figure 2b). Reaction times in the 2 back conditions were significantly longer than for the 0 and 1 back Conditions, confirmed via post hoc.
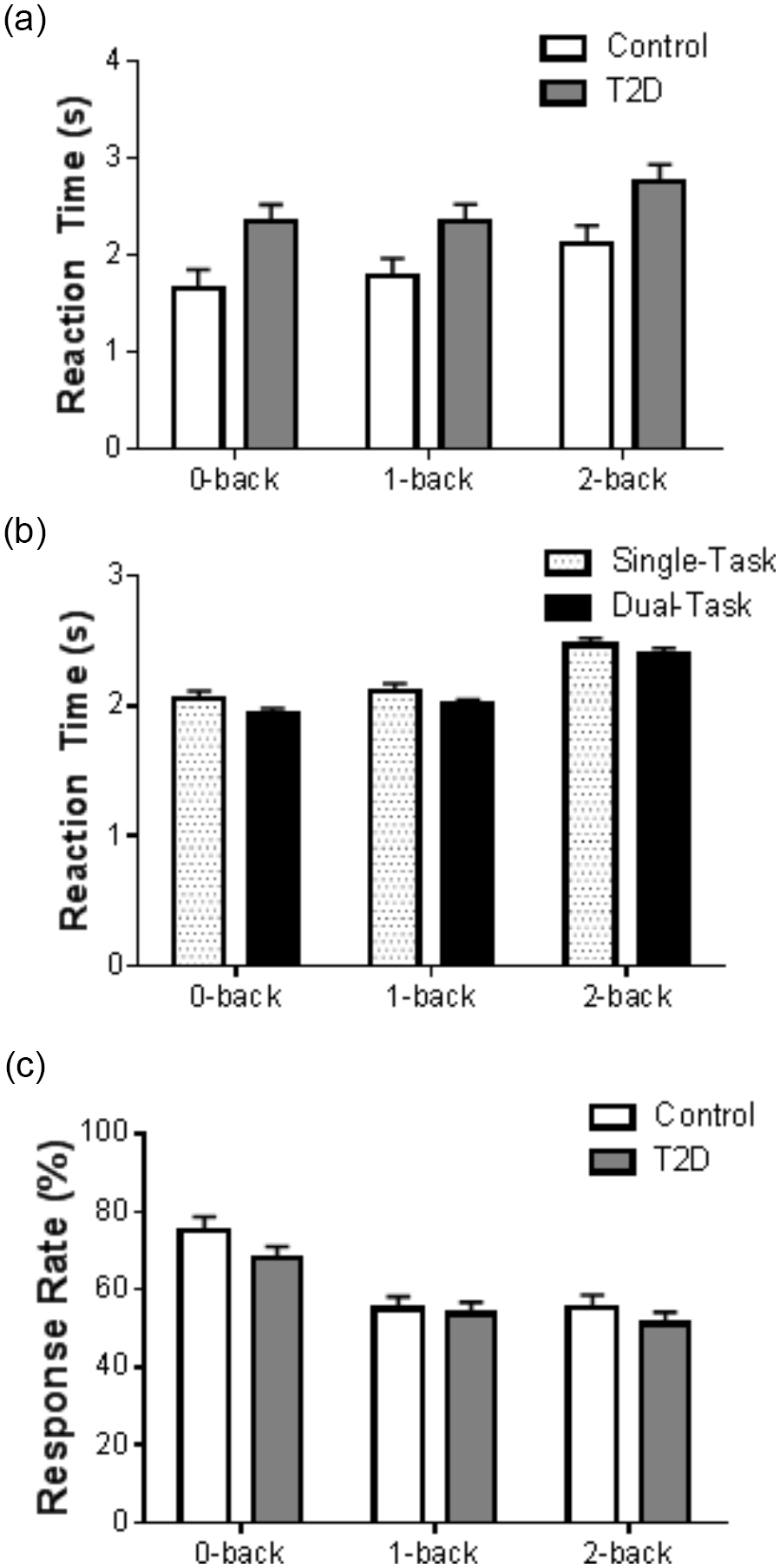
Mean and standard error for working memory data.
The accuracy of responses also did not show a difference across Group in the initial RM-ANOVA, despite Condition effects, F(2, 143) = 21.71, p < .001. The percentage of correct responses produced per trial was significantly higher in the 0 back condition, compared with both the 1 and 2 back conditions, verified via post hoc (Figure 2c). ANCOVA revealed a Group difference, F(1, 143) = 4.23, p < .05, in addition to the persistent Condition differences, along with the significant contribution of disease state markers to error rate production (HbA1c: F(1, 143) = 7.29, p < .01; Duration: F(1, 143) = 6.56, p < .05; Diastole: F(1, 143) = 4.13, p < .05). The Group difference that emerged with covariates indicates that performance by the T2D group would be improved with better health state measures (e.g., lower HbA1c, lower diastole measures) while performance of the controls would be drastically impaired with worsened health state indices (e.g., higher HbA1c, higher diastole measures). These data not shown as error rates for the T2D group are predicted as negative via ANCOVA.
Motor Function
RMSE values were significantly larger in the T2D Group versus controls, F(1, 133) = 3.94, p < .05, via RM-ANOVA (Figure 3a and 3b). Increased RMSE values were associated with increased %MVC Level, F(1, 133) = 32.17, p < .001 (Figure 3a). RMSE values did not differ across Condition. ANCOVA indicated that HbA1c, F(1, 128) = 5.26, p < .05; Diastole, F(1, 128) = 11.97, p < .001; and PN status, F(1, 128) = 9.90, p < .005, presented with significant effects on RMSE, and together they account for the Group effect in the initial model. Subsequent bivariate correlations indicated a positive relationship between RMSE and HbA1c (r158 = .202, p < .05) as well as RMSE and Diastole (r158 = .212, p < .01).
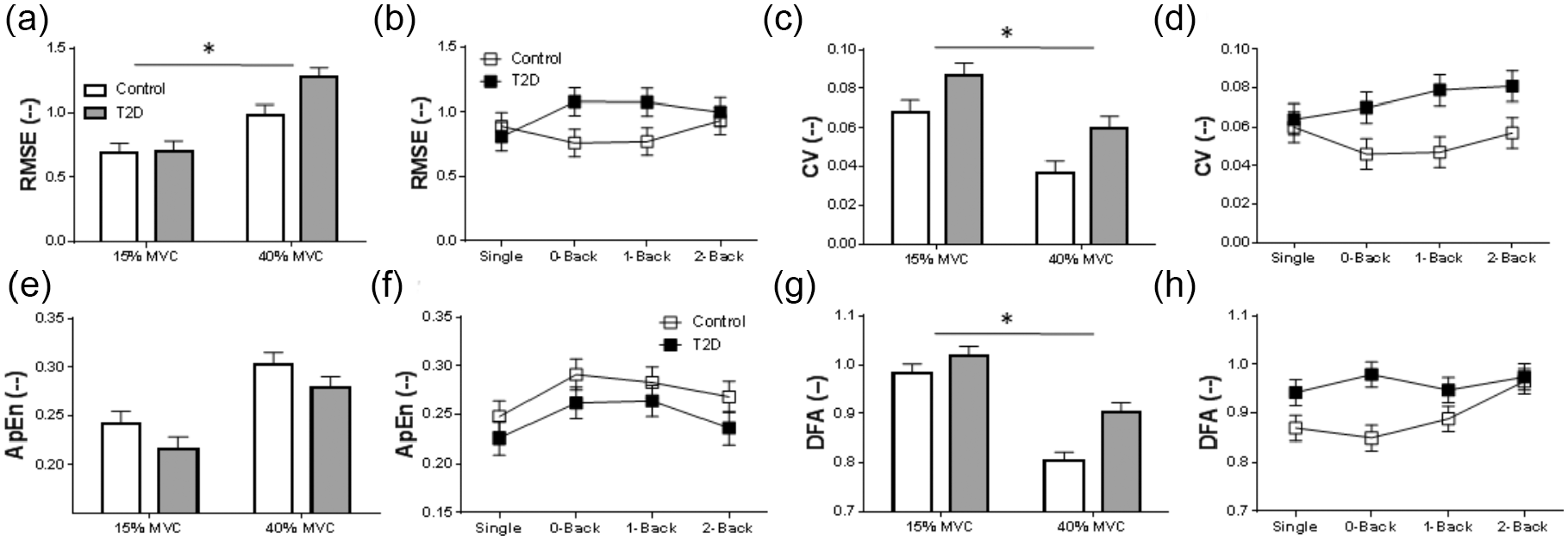
Mean and standard error of motor function data.
CV values were higher for the T2D Group, F(1, 133) = 14.1, p < .001, via RM-ANOVA (Figure 3c and 3d). ANCOVA indicated that CV values decreased with increased %MVC Level, F(1, 133) = 26.96, p < .001 (Figure 3c). PN status, F(1, 128) = 21.57, p < .001, and Diastole, F(1, 128) = 6.15, p < .05, presented with significant effects on CV, with the Group effect remaining intact. Subsequent bivariate correlations indicated a positive correlation between CV and Diastole (r158 = .2, p < .05).
Nonlinear analyses of the kinetic data also pointed to Group differences, F(1, 133) = 4.78, p < .05, via RM-ANOVA, such that the T2D group exhibited lower ApEn values as compared with controls (Figure 3e and 3f). Covariates Diastole, F(1, 128) = 36.44, p < .001; PN status, F(1, 128) = 31.40, p < .001; HbA1c, F(1, 128) = 10.92, p < .001; and Duration, F(1, 128) = 6.21, p < .05, were all also found to contribute significantly to ApEn values, all enhancing the Group effect in follow-up ANCOVA. DFA also exhibited a significant Group effect, F(1, 133) = 13.26, p < .001, via RM-ANOVA, such that T2D patients exhibited larger DFA values as compared with controls. DFA values were found to be higher with lower %MVC Level, F(1, 133) = 62.05, p < .001, via RM-ANOVA (Figure 2g and 2h). ANCOVA did not yield any significant results for DFA.
Discussion
The purpose of this study was to explore the effects of T2D on basic cognitive–motor activities during working memory evaluation and a motor task involving the upper extremity. This study is a first step toward understanding the specific challenges in CMI with respect to hand/finger function of persons with T2D. More work is needed in this specific area. We hypothesized that (a) persons with T2D would demonstrate impairment in baseline evaluations and in cognitive, tactile, and motor single tasks compared with controls, and (b) persons with T2D would demonstrate further impairment in one or both the cognitive and motor domains during dual tasks as compared with controls. Our findings on all of the baseline and single task evaluations support the first hypothesis, such that persons with T2D demonstrate impairment in baseline evaluations and in each of the cognitive, tactile, and motor single tasks evaluated in this study compared with controls. The data do not support the second hypothesis, such that persons with T2D demonstrate impairment in the cognitive and motor domains during dual tasks compared with controls; however, these impairments were consistent with single task losses. These losses may impact the ability for persons with T2D to perform activities of daily living. In the following paragraphs, we discuss the results of this study in regard to the published literature as it relates to impaired self-care and implications for occupational therapists as well as possible mechanisms responsible for behaviors exhibited.
T2D-Induced Cognitive–Manual Motor Deficits, Self-Care, and Occupational Therapy
Baseline evaluation of tactile function, motor function, and cognitive function (via MoCA) all revealed significant losses in tactile, motor, and cognitive functions in the T2D group. Consistent with previous publications, tactile detection thresholds in the hands of the T2D group were in the range of diminished light touch to diminished protective sensation (Gorniak et al., 2014; Ochoa et al., 2016; Ochoa & Gorniak, 2014). Maximal pinch strength was reduced in the T2D group in this study as compared with the control group, despite previous reports of preserved pinch strength in T2D patients (Gorniak et al., 2014; Ochoa et al., 2016; Ochoa & Gorniak, 2014). Significant differences in force production error rates and signal predictability in the T2D group in motor only tasks were consistent with previous literature (Gorniak et al., 2014; Ochoa et al., 2016; Ochoa & Gorniak, 2014). Baseline cognitive function, assessed via MoCA, was reduced in the T2D group, particularly in the domain of recall/working memory, consistent with recent reports of MCI and working memory deficits in T2D (Christman et al., 2009; Creavin et al., 2011; Gorniak et al., 2019).
Deficits in both motor and cognitive functions in adults with T2D persisted in evaluation of single tasks, in which the tested task was either predominantly motor or cognitive (recall) in nature. Motor deficits in the T2D group manifested as increases in RMSE, CV, DFA, and a decrease in ApEn. Cognitive deficits in the T2D group manifested in increased reaction times and reduced correct response rates per trial during the N-back tasks. Each of these forms of deficits persisted in dual task evaluations in the T2D group, with no additional statistically significant deficits noted due to dual tasking. We do note that the 4 s windows between working memory stimuli in the N-back (cognitive) task may have contributed to the lack of group differences in the response rate findings. It is possible that additional cognitive deficits may have emerged if the time interval between cognitive stimuli was decreased or if the duration of each trial had been longer than 30 s, thereby further taxing the central nervous system (e.g., by taxing a limited channel capacity), as found in Gorniak et al. (2019). All single task evaluations were performed prior to any dual tasks, which may have induced a learning effect in our study population, and thus a reduction in reaction time in the dual task. Although this is possible, this particular order of testing is the standard in evaluating dual task loss for working memory tasks (Frankemolle et al., 2010).
Although baseline tactile, motor, and cognitive functions were impaired in all tasks in the T2D group, it is important to note that this decline was not exacerbated by the performance of dual tasks. This may mean that while patients living with T2D may exhibit functional decline in cognitive and motor functions separately, their ability to perform activities of daily living that require the coupling of cognitive and motor tasks may not be as significantly impaired as other patients with CVD-induced neural damage (e.g., stroke). However, these losses still likely impact the ability for persons with T2D to perform activities of daily living. Given the length of time for T2D to develop in most patients, the slow metabolic changes experienced by the nervous system may permit the patient to develop coping strategies in the performance of activities of daily living concurrently with the development of the disease, unlike the acute neurological deficits found in patients after stroke. Despite the possibility of developing coping mechanisms, the significant tactile, motor, and cognitive deficits in T2D patients should not be downplayed.
In particular, clinicians should take the confluence of these deficits into account when developing medical management and rehabilitation strategies, including physical activity interventions and modifications of self-care activities related to activities of daily living. Given that the deficits exhibited have roots both in the central and peripheral nervous systems, it is recommended that clinicians consider the use of low stimulation environments and devices with sensory augmentation in one or more modalities to assist in rehabilitation in T2D. Low stimulation environments may assist with recall and memory functions, whereas multimodal sensory augmentation may be used to overcome tactile detection deficits in persons with T2D.
In addition, the severity of cognitive, sensory, and motor deficits should be considered when designing occupational therapy interventions for persons with T2D. It is likely that these deficits have led to individualized maladaptive coping mechanisms that may interfere with functional hand use in activities of daily living. This may further complicate occupational therapy rehabilitation in persons with T2D in which significant comorbid conditions are also present (e.g., stroke). Accordingly, it is appropriate for occupational therapy to occur early on in the disease process to minimize the effects of cognitive, sensory, and motor deficits in persons with T2D.
Potential Mechanisms
In our covariate evaluations, several disease state markers were found to magnify the group effects found in the data. In the working memory data, the covariate analyses signaled subtle working memory changes due to deterioration of health state markers, not the specific diagnosis of T2D. Blood pressure measures were found to significantly contribute to the variability in working memory measures included in this study. Blood pressure measures indicate the pressure exerted on the cardiovascular system during contraction and relaxation (“The Facts About High Blood Pressure,” n.d.). Increased blood pressure is associated with vascular damage, increased cardiovascular workload, and a high likelihood of reduced tissue oxygenation resulting in tissue and organ damage (“The Facts About High Blood Pressure,” n.d.). Given the association between tissue damage and high blood pressure, the functional results of this study are logical. Both cognitive function and motor function measures were generally worsened with increased blood pressure measures. In particular, males had worsened blood pressure measures as well as larger pinch force values. Although males do generally produce larger maximal force values, it is possible that increased blood pressure may be associated with excessive manual force production leading to reduced ability to modulate manual forces (e.g., ApEn, RMSE, and CV results) when required due to the development of vascular damage.
The magnification of significant differences in both cognitive and motor functions between the two groups given the covariates is likely due to slow systemic cardiovascular and neurological damage caused by the presence of metabolic disease. This suggests that multiple functions of the body may be directly affected by T2D. As a result and contrary to traditional clinical opinion, reduced motor function in the T2D group is thus not due solely to peripheral nerve damage, but to multi-system changes in the body (Ochoa et al., 2016).
Between-group differences in the motor function data were magnified when the incidence of PN was controlled for in the data, suggesting that clinical diagnosis of peripheral nerve damage does not simply account for between-group differences. Consistent with our previous work, this suggests that global CVD may directly impact the corticospinal tracts and/or cerebral cortex and thus is responsible for the tactile and motor function deficits exhibited in this and previous studies (Gorniak et al., 2014, Gorniak et al., 2019; Ochoa et al., 2016; Ochoa & Gorniak, 2014). Additional work in this area may elucidate how self-care is impacted by systemic subtle cardiovascular and neurological impairment in T2D patients.
Limitations
We acknowledge the small sample size used in this particular project despite the indication that the sample should provide enough power for detecting between-group differences. Our findings are consistent with previous assessments of upper extremity function in persons with T2D. They are also consistent with preliminary data from our follow-up neuroimaging study evaluating manual and cognitive dysfunction in persons with T2D in a larger sample.
Footnotes
Acknowledgements
We are thankful for the help with data collection from our team of research interns: Sahifah Ansari, Beatriz Thames, Lena Younes, Neryeda Ochoa, Taft Knowles, Zahrah Mohamed, Reka Kovacs, Yoshimi (Fangmei) Lu, Taylor Peabody, and Aisha Khan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by American Heart Association Grant Number 16BGIA27250047 (Gorniak).
Ethical Approval
Institutional Review Boards of the University of Houston (FWA 00005994) and University of Texas Health Science Center at Houston (FWA00000667) approved this study.