
Abstract
There is a relationship between sitting balance and self-care functioning, but no occupation-based sitting balance assessment. The objective of this study was to determine whether the Sock Test for Sitting Balance (STSB) is a valid balance assessment for use by therapists in acute care. Results of the STSB were compared with those of the Adapted Functional Reach (AFR), the Functional Independence Measure (FIM™) chair transfer, and the Kansas University Sitting Balance Scale (KUSBS), in both hospitalized and healthy participants. There is a significant relationship between STSB results and AFR results for all participants (rs = −.382, p = .012). Relationships between STSB results and score on the FIM™ Chair Transfer subscale (p = .001), and score on the KUSBS (p = .003) are significant. The STSB can differentiate between a hospitalized population and healthy population (p = .017). Criterion and known-groups validity are demonstrated, but should be confirmed with further testing.
Numerous everyday tasks, such as working at the computer, reaching for the television remote, toileting, or buckling a favorite pair of sandals, each require adequate sitting balance to complete successfully. Balance is a complex phenomenon that entails the interaction of multiple body systems to accomplish the basic task of remaining upright. There is a strong correlation between sitting balance and level of self-care functioning (Gorman et al., 2014; Hama et al., 2007; Oh et al., 2012), yet there is no purposeful activity-based sitting balance assessment grounded in occupation-based theory. A function-based assessment, utilizing the task of sock donning and doffing, is proposed as a method of measuring sitting balance in the acute care setting.
The acute care practice environment requires therapists to make discharge placement recommendations after an initial, 30-min evaluation session, and is marked by high patient caseloads, short lengths of stay, and the pressure of productivity expectations (McKelvey, 2004). In addition, occupational therapists’ expertise in providing discharge recommendations to prevent costly hospital readmissions is now being recognized (Roberts & Robinson, 2014; Rogers et al., 2017). Occupational therapists, currently, use few standardized assessments in the acute care setting (Craig et al., 2004) to base their goals and recommendations.
The Sock Test for Sitting Balance (STSB) is a performance-based test that assesses active sitting balance during a functional task, specifically, doffing and donning socks. The patient is assessed in an unsupported sitting position on the edge of their hospital bed as they don and then doff a pair of hospital-issue slipper socks. The theory and framework used for the development of STSB include occupational adaptation (OA) theory (Schkade & Schultz, 1992) and the Systems Framework of Postural Control (SFPC; Horak, 2006). The task of sock donning and doffing is a purposeful activity with an end-product that is appropriate for assessment of a client’s ability to adapt, and could be a pragmatic application of the OA theory. The SFPC states that no single body system is responsible for postural control, but rather that postural control is the result of the interaction of multiple systems in a continuously changing environment (Woollacott & Shumway-Cook, 1990). Five of the six major components of postural control identified by the SFPC can be observed in the STSB.
The purpose of this study was to test the validity of the STSB by comparing results with validated assessment tools, and to determine whether the STSB can differentiate between a hospitalized and healthy population. In addition, the data from the healthy population provide normative standards for client comparison and judging of future treatment effectiveness.
Research Questions
As suggested by Portney and Watkins (2009), the process of validating a measure typically includes exploration of criterion validity as well as some forms of predictive or “known-groups” validity. This study sought to answer the following research questions:
Method
Study Design
This methodological study utilized reference-standard comparison, purposeful sampling, and case matching. The design and number of participants for this study were based upon the results of a pilot study. The pilot study was completed in December 2016, and post hoc analysis using G*Power showed that 20 participants were needed for each group. To answer the research questions, the STSB was administered along with the following three instruments: Adapted Functional Reach (AFR) Test, a validated sitting balance assessment tool; the Kansas University Sitting Balance Scale (KUSBS), a quantitative descriptor of balance; and the Functional Independence Measure (FIM™) Chair Transfer subscale, a measure of function.
Participants
A total of 21 adults, of age 21 years and above, who were hospitalized at Ochsner Medical Center in New Orleans, LA, were age-, gender-, and weight-matched to 21 apparently healthy adults living independently in the community. Matching was conducted to control for the effect of body habitus and age on results. The community dwelling participants were age-matched to the hospitalized participants by ±5 years, and were weight-matched by ±50 lbs. Ochsner Medical Center is a 473 bed, research-based, acute care hospital.
The hospitalized participants’ inclusion criteria were as follows: ability to follow verbal instruction, a prior independent level of functioning in self-care activities of daily living (ADLs), and the ability to maintain static sitting balance on the edge of the bed without physical assistance. Exclusion criteria were medical instability, current or past range of motion or weight bearing precautions, and any person that was under the influence of immediate postoperative pain medications or sedation. There was a wide variety of admission diagnoses and length of stay among the hospitalized participants.
The inclusion criteria for the community cohort were the same as for the hospitalized, with the addition of “apparently healthy”; defined by a lack of history of procedures or disease that affect range of motion and/or balance.
Sampling Procedures
Participant recruitment and testing took place between August 16, 2017 and October 7, 2017. Appropriate hospitalized participants were identified from chart reviews of current patients on the occupational therapy caseload. Five patients were recruited from each of the following three distinct patient units: stroke, neuro, and oncology, and six from the general medicine unit.
The community participants were recruited from acquaintances of the principal investigator (PI), and by snowball sampling. Inclusion criteria were confirmed by phone interview, and testing conducted in their home.
Instruments
The STSB
The initial publication of a version of the Sock Test was done by Strand and Wie in 1999, and consists of reaching for the foot in unsupported sitting (Strand & Wie 1999). In 2002, timed donning of one sock was included in a performance battery with significant correlations found between the sock donning time and six other tasks (Simmonds, 2002). Two currently unpublished thesis studies were completed with sock donning and doffing at Texas Woman’s University in 2011 and 2012. This unpublished work includes normative data (Nicholson, 2012) and timed data with a cerebrovascular accident (CVA) population (Parker, 2011). Stepwise multiple regression analysis in the study by Parker (2011) showed that sitting balance and attention could predict STSB time. Interrater reliability of the STSB was .99 and test–retest reliability was .92.
The AFR test
The AFR is an assessment of sitting balance in which the distance a participant is able to reach forward and laterally while seated is measured using a yard stick. It is a modification of the functional reach (FR) test, (Duncan et al., 1990), and the modified functional reach test (MFRT; Lynch et al., 1998). In 2007, normative data were collected for forward and lateral reach in sitting (Thompson & Medley, 2007). Although the authors did not specifically name this modification of the MFRT, for the purposes of this project, it will be referred to as the AFR test. The AFR has been determined to have excellent intrarater reliability when measuring forward and lateral reach (intraclass correlation coefficient [ICC] = .98 and .96, respectively; Thompson & Medley, 2007).
FIM™
The FIM™ is an established outcomes tool in a wide variety of medical settings, including acute care (Chumney et al., 2010). The transfer item of the FIM™ was chosen for criterion validation as it has been used to determine validity with other balance scales, including The Postural Assessment Scale for stroke patients (Benaim et al., 1999), and the Kansas University Sitting and Standing Balance Scales (KUSSBS) (Kluding et al., 2006). A review of the literature in 2009 by Glenny and Stolee summarized psychometric properties of the FIM™ from multiple studies, and found that the motor subscale has high internal consistency (α = .68–.96), very high intrarater reliability (r = .90–.97), and high interrater reliability (ICC = .91–.99). Use of the motor subscale and individual items of the FIM™, have been shown to be more relevant than using the FIM™ total score (Ravaud et al., 1999).
The KUSSBS
The KUSSBS were developed in 2006 at the University of Kansas Medical Center (Kluding et al., 2006). The sitting scale was chosen for criterion validation as it provides an objective description of balance and is appropriate for use in the acute care setting. The KUSSBS consists of an ordinal rating system (0–5 grades with plus values), which provides 10 levels (Geriatric Examination Toolkit, 2017). The Kansas University Standing Balance Scale has been determined to have good intrarater reliability (ICC = .893) and moderate interrater reliability (ICC = .728). Concurrent validity has been established against the FIM™ transfer score (rs = .486, p = .014; Kluding et al., 2006).
Procedures
Institutional Review Board approval was obtained from Ochsner Clinic Foundation and an Institutional Authorization Agreement was established with Texas Woman’s University on 19 July, 2017. Informed consent was obtained prior to commencement of any testing, including the study’s risks and benefits, the voluntary nature of their participation, and the non-disclosure of their identity. All participants were assigned a code, and the informed consents were filed in a separate secure location from the coded study results.
All testing was conducted by the PI. After ensuring that the participant’s feet were on the floor while sitting on the edge of the hospital bed, the PI administered the AFR and the STSB. To avoid a practice effect, the PI alternated which of the two assessments was administered first with each participant. During administration of the STSB, the PI applied the relevant KUSBS score. Following administration of the STSB and the AFR, the PI had the participant transfer on to a bedside chair and then back to the bed.
The community participants were contacted either in person or by telephone and an appointment was scheduled. To match hospital bed height between 23 and 27 in. tall, a few of the home-based participants were assessed on the edge of a guest bed or child’s bed instead of their primary bed. The PI then administered the three assessments in the same manner as described for the hospitalized participants.
AFR
The AFR test was administered according to the procedures described by Thompson and Medley (2007), with one alteration. The measurement took place along the edge of an adjustable height bedside table as a yardstick could not be affixed to the walls of the participants’ room.
STSB
For testing, the participant was seated on the edge of the bed, barefoot, with both feet on the floor. The participant was instructed to put the socks on and take them off at a pace that was normal for them. The PI stood directly in front of the participant, and held a pair of hospital-issue slipper socks within reach of the participant. The PI simultaneously started the stopwatch and gave a verbal “Go” command. The PI measured the amount of time required to don and then doff both slipper socks, in seconds. Time, method of sock donning/doffing, and clinical observations related to the SFPC were recorded on the data collection sheet. For the hospitalized participants, a rehab tech was near the participant for balance safety.
FIM™ Chair Transfer
The chair transfer was administered as per FIM™ guidelines. If the scores for the two transfers differed, the lowest score was used, as per FIM™ guidelines (Keith et al., 1987).
KUSBS
The KUSBS was printed on to the data collection sheet, directly below the STSB section. Based on balance observed during the STSB, the appropriate KUSBS level was applied and recorded on the data collection sheet.
Results
Data analysis was conducted with International Business Machines Corporation Released (IBM 2016, 2017) SPSS Statistics 24 and 25. Both research questions were answered using nonparametric data analysis, as the STSB data did not have a normal distribution (Field, 2013). Spearman’s rho was used to correlate the STSB results to the AFR test, the KUSBS, and the FIM™ Chair Transfer subscore. Degrees of freedom were calculated with the formula, n−2 (McDonald, 2014).
Mann–Whitney U independent samples testing was used to differentiate between the two cohorts. Effect sizes for the Mann–Whitney analyses were calculated by converting the z score to the effect size estimation r. Results for all effect sizes were interpreted as follows: .10 = small effect size; .30 = medium effect size; .50 = large effect size (Field, 2013, p. 82).
Participants
The average age and weight of the hospitalized participants were not significantly different than the community participants. There were 15 women and 6 men in each group. See Table 1 for details.
Demographic Information..
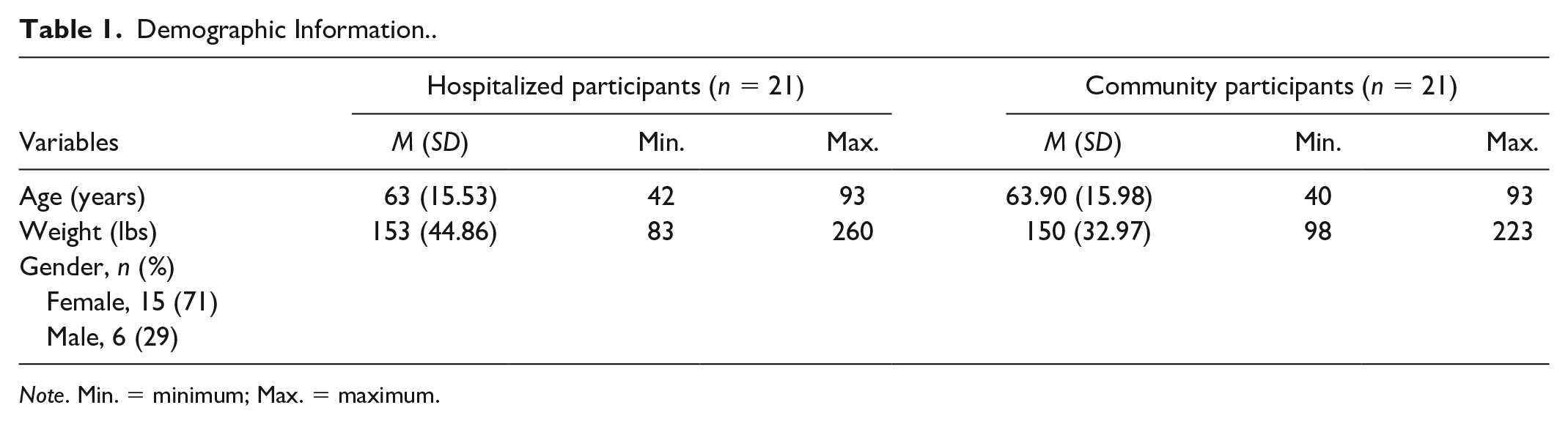
Note. Min. = minimum; Max. = maximum.
Construct Validity
The primary method chosen to establish validity of the STSB as an assessment of sitting balance was using criterion validation to correlate the scores obtained on the STSB to scores obtained on other balance and mobility instruments. Spearman’s rho correlation showed that there was a significant relationship between ranked time to complete the STSB and centimeters of reach on the AFR-forward reach, rs (40) = −.382, p = .012, and lateral reach, rs (40) = −.393, p = .010, for all participants. Longer time to complete the STSB was associated with a shorter reach forward and laterally, and faster time to complete the STSB was associated with a longer reach forward and laterally. However, neither the relationship between STSB and forward reach, rs (19) = −.178, p = .440, nor between STSB and lateral reach, rs (19) = −.199, p = .388, were significant for the hospitalized cohort alone.
Spearman’s rho correlation showed that there was a significant relationship between ranked time to complete the STSB and score on the FIM™ Chair Transfer subscale, rs (19) = −.677, p =.001, for the hospitalized cohort. Faster time to complete the STSB was associated with a higher (more independent) transfer score, and longer time to complete the STSB was associated with a lower, more dependent transfer score.
Correlation to the KUSBS showed that there was a significant relationship between ranked time to complete the STSB and score on the KUSBS, rs (19) = −.614, p = .003, for the hospitalized cohort. Faster time on the STSB was associated with a higher (more normal) KUSBS balance score, and longer time to complete the STSB was associated with a lower (more impaired) KUSBS balance score. For a summary of the correlation data, see Table 2.
Summary of Correlations for the Scores on the STSB, AFR-forward, AFR-lateral, FIM chair transfer, KUSBS-hospitalized participants, and all participants.
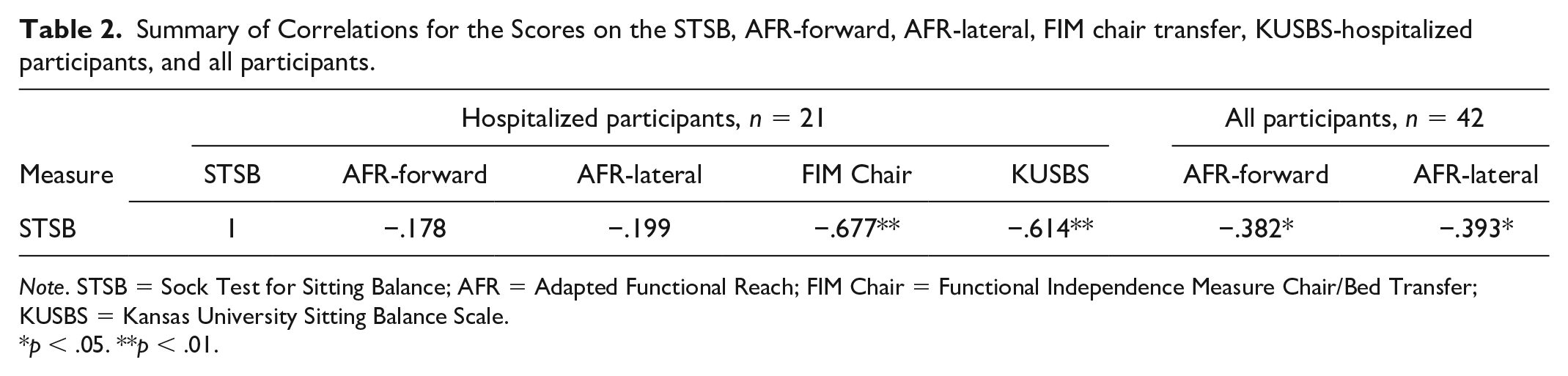
Note. STSB = Sock Test for Sitting Balance; AFR = Adapted Functional Reach; FIM Chair = Functional Independence Measure Chair/Bed Transfer; KUSBS = Kansas University Sitting Balance Scale.
p < .05. **p < .01.
Known-Groups Validity
Overall, the community participants completed the STSB faster, and reached further forward and laterally on the AFR test, than the hospitalized participants. See Table 3 (descriptive statistics) for details.
Descriptive Statistics and Outcome Comparisons Between Hospitalized and Community Participants—Research Question 2.
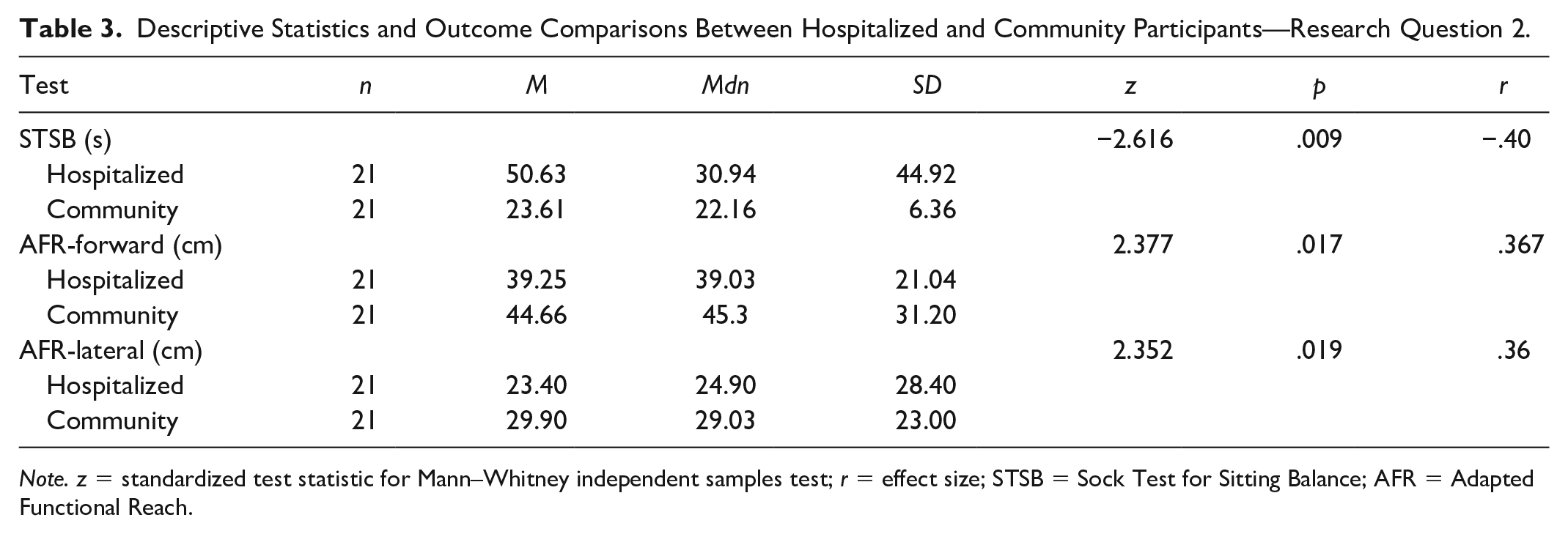
Note. z = standardized test statistic for Mann–Whitney independent samples test; r = effect size; STSB = Sock Test for Sitting Balance; AFR = Adapted Functional Reach.
Results for Research Question 2 showed that the STSB could differentiate between the two cohorts, with the community population (Mdn = 22.16) completing the STSB an average of 27.02 s faster than the hospitalized (Mdn = 30.94) population. The ranked differences between the two cohorts was significant, z = −2.616, p = .009, and represents a medium effect size, r = −.40. The AFR forward and lateral were also able to differentiate between the two populations (p = .017, p = .019; see Table 3).
Discussion
This study sought to determine construct validity of the STSB for use as a sitting balance assessment tool in the acute care setting, using criterion and known-groups testing. The hypothesis that the STSB would be able to differentiate between a hospitalized and an apparently healthy population was confirmed. The hypothesis that there would be a significant relationship between results on the STSB and the three assessment tools used in the study was partially confirmed. There was a significant relationship in the hospitalized cohort between the STSB and both the FIM™ chair transfer and the KUSBS. There was a significant relationship between STSB and the AFR test for the community cohort and all participants, but not hospitalized participants alone.
The results of this study support other studies that have correlated timed balance assessment tools (like the STSB) to that of functional reach in healthy subjects. Newton found a significant correlation between distance reached on the functional reach test and time on the Timed Up and Go (TUG) in community dwelling older adults (Newton, 2001). In a study of healthy women aged 63 years and above, Franchignoni (1998) found significant correlation between the distance reached in the functional reach test and time required on the Five Times Sit to Stand. Simmonds (2002) found significant correlation between the timed needed to don one sock and functional reach in both a group with cancer and a healthy control group.
As a timed assessment, the STSB can be used to objectively measure patient progress. The use of time is easily understood by patients and therapists alike, as demonstrated by the prevalence of the Timed Up and Go, Nine Hole Peg Test, 30-second Sit to Stand, and more (Gervais et al., 2014; Grice et al., 2003). The community sample size from this study is small, but the results are consistent (no statistically significant difference) with the healthy community norms of Nicholson’s (2012) 60-participant study. Thus, these norms might be used to evaluate client performance.
The structure of the STSB facilitates the assessment of a client’s adaptive response behavior. As per the OA framework, to observe and assess a client’s adaptive response, a task must be chosen that has a beginning and an end, has an end product, is process-oriented, and is meaningful to the client (Schkade & Schultz, 1992). By requiring the client to complete a functional task from beginning to end, rather than simulating or only partially completing it, the STSB meets these criteria. The acute hospital environment requires the use of slipper socks as part of modern fall prevention programs, thus adding context and further meaning to the task of sock donning and doffing for the patient. Finally, the STSB provides an opportunity for occupational therapists to observe and assess a patient’s level of adaptive behavior in their first session with the patient, establishing a baseline for this important aspect of occupational therapy evaluation and treatment.
Clinical utility plays a role in the decision to use a standardized instrument, and the importance of clinical utility in an assessment tool has been gaining prominence in the literature (Kluding et al., 2006; McGinnis et al., 2009). The STSB addresses these concerns with its quick administration time and utilization of equipment (slipper socks) that is readily available to occupational therapists working in acute care settings. The time required to set up and conduct the STSB for each participant in our study was below 5 min, suggesting the STSB is a realistic balance assessment tool choice in the acute care setting. Although minimal training to administer the STSB is required, analysis would be enhanced by closely observing the client using the SFPC. Finally, the use of a timed result from the STSB combined with the standardized description of balance provided by the KUSBS, could facilitate objective documentation of balance, an improvement over many current descriptors such as “good” or “fair.”
Limitations
A larger sample size would improve generalizability of the results. The study also excluded those with a history of range of motion impairment and this could have impacted the results.
Future Research
The control of dynamics and biomechanics required to perform the STSB are greater than that required for the AFR. Therefore, to further validate the STSB, a future study should be conducted comparing results on the STSB to a different sitting balance assessment tool, preferably one that challenges control of dynamics in a similar fashion to the STSB. To improve interpretation and utility of results, a study in which a cut-off score is established that indicates a higher chance of falling or that correlates with a discharge setting, should be conducted. Observations from this study also show that a study that includes regression analysis to determine the impact of the adaptive response and anticipatory movement strategies on balance and STSB time is indicated.
Conclusion
This study sought to determine construct validity of the STSB by correlating the results to those of an already-validated sitting balance assessment tool, the AFR test, to a functional measure, the FIM™ Chair Transfer subscale, and to a quantitative descriptor of balance, the KUSBS. The study results advance the use of the task of sock donning and doffing as a sitting balance measurement tool, helping to establish the STSB for use by occupational therapists in the acute care setting. The STSB could contribute to the future evidence base of occupational therapy practice, as occupation-based outcome measures are currently needed in studies of the efficacy of occupational therapy (Lesher et al., 2017). As a timed, occupation-based test, the STSB could eventually be used in efficacy studies, similar to the TUG. Finally, the STSB consists of an appropriate task in which to observe and assess a patient’s level of adaptive functioning, thus providing information on this important component of occupational therapy evaluation, and serving as a pragmatic application of OA theory.
Footnotes
Acknowledgements
I thank the entire PhD in Occupational Therapy program at Texas Woman’s University, and especially Dr. Mary F. Baxter and Dr. Sally Schultz for their support and guidance. Dr. Katy Mitchell’s feedback was invaluable. I also thank Ochsner Medical Center of New Orleans, LA, and all of the participants that agreed to give their time and effort for this study.
Author’s Note
This material was presented at the 2019 American Occupational Therapy Association Annual Conference as a Scientific Research Panel presentation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approved by the Ochsner Clinic Foundation Institutional Review Board on July 13, 2017; IRB#: 2016.174.C. The study protocol was approved by the Ochsner Clinic IRB and all procedures followed were consistent with the revised Helsinki Declaration, and the ethical standards of Ochsner Clinic, Texas Woman’s University, and the American Occupational Therapy Association.