
Abstract
Although many daily activities that require the upper extremity are performed in standing, arm motor function is generally measured in sitting. The purpose of this study was to examine the effect of standing on a measure of upper extremity function, the Jebsen Hand Function Test (JHFT). Twelve nondisabled adults (26.3 ± 3.1 years) completed the JHFT with the right and left arms under two conditions: sitting and standing. Total time to complete the JHFT increased when performed in standing compared with sitting in both arms (p = .005); mean increase was 4.4% and 5.6% for the right and left arms, respectively. Checker stacking was the only subtest that showed a significant increase in completion time in standing for both arms (p = .001); card turning showed an increase for the left arm only (p = .002). Measurement of upper extremity function in standing may provide insight into arm motor capacity within the context of standing postural control demands.
Introduction
Skilled movement of the arm and hand is important for completion of everyday functional activities. Although many functional tasks are performed in standing (e.g., meal preparation at the kitchen counter), most measurement of the upper extremity function in clinical and research settings occurs in sitting. Research suggests that the performance of skilled arm and hand movements in standing differs from the same movements in sitting (Berrigan et al., 2006; Cuisinier et al., 2005), requires precise coordination between upper extremity movement and postural control (Chen et al., 2016; Pozzo et al., 2002), and is associated with changes in corticomotor excitability for upper extremity muscles (Kantak et al., 2013; Runnalls et al., 2017). The impact of standing on the control of upper extremity tasks may be magnified in individuals with neurologic conditions such as stroke, who often present with postural control deficits (Belgen et al., 2006; Harris et al., 2005; Jorgensen et al., 2002; van de Port et al., 2006). Determining the effects of standing on upper extremity function effectively and efficiently, using a standardized outcome measure, could be useful to clinicians in understanding arm function in a manner that is better matched to how people move in real life and in determining if arm training activities in standing are warranted.
Standardized outcome measures are an important clinical and research tool to document upper extremity motor status in both nondisabled populations and individuals with a variety of clinical diagnoses. Scores on standardized measures are often used to determine level of function, degree of recovery, and improvement following an intervention (Lang et al., 2013). As the goal of outcome measures often is to define the level of motor capacity, most standardized measures of arm status are appropriately administered in a sitting position such that postural control requirements are minimal. However, many everyday functional tasks performed with the upper extremities are completed in a standing position. Compared with sitting, standing leads to an increase in postural control demands (e.g., decreased size of base of support and higher center of mass), a change in the number of degrees of freedom that have to be controlled (e.g., need to control the trunk and lower extremity joints), and requires some degree of attentional resources (Dierijck et al., 2020; Woollacott & Shumway-Cook, 2002), which may impact upper extremity movement. Therefore, measurement of skilled arm movements in standing as well as in sitting may be helpful in understanding arm motor capacity in a manner that reflects the challenges commonly faced in real-world function. To our knowledge, there have been no studies examining how performance on a standardized measure of arm function changes when completed in standing.
The Jebsen Hand Function Test (JHFT) is a valid and reliable standardized measure of arm and hand function (Jebsen et al., 1969) that is used in both healthy (Boggio et al., 2006; Convento et al., 2014) and clinical populations (Beebe & Lang, 2009; Mak et al., 2015; Weinstock-Zlotnick & Mehta, 2016). The JHFT includes seven items that require individuals to perform various functional hand and arm tasks while time to complete each item is recorded. The JHFT is relatively quick to administer, uses commonly available testing materials, and has published, normative data (Hackel et al., 1992; Jebsen et al., 1969). The standard way to administer the JHFT, per the instructions in the original paper, is in a sitting position (Jebsen et al., 1969). Currently, it is not known if completion of the JHFT in standing has an effect on test performance.
The purpose of this study was to examine the effect of standing on arm function as measured by performance on the JHFT. As a first step, this initial investigation was completed in a group of young, nondisabled adults to determine if the JHFT was sensitive to a change in position (i.e., standing). We hypothesized that time to complete the JHFT would increase when performed in standing compared with sitting. In addition, we expected the effect of standing on test performance to be greater on the nondominant, left arm than on the dominant, right arm. Center of pressure was measured during all standing trials to provide data for hypothesis generation in future studies.
Methods
This study used a within-subject, cross-over design where all participants completed the JHFT in sitting and standing with both the right and left arms in separate sessions. Testing sessions occurred on two separate days, one week apart; the arm tested on the first day was counterbalanced across participants.
Participants
Twelve nondisabled adults (mean age ± SD: 26.3 ± 3.1 years; 6 females) were recruited from the university student community. This sample size provided approximately 70% power in detecting a significant effect (G*Power 3.1.9; f = 0.4, α = 0.05). Participants were right-hand dominant (Oldfield, 1971), had no history of a neurological condition, and were free of arm and hand pain. All participants provided written informed consent prior to participation through a protocol approved by the Institutional Review Board at the University of South Carolina.
Jebsen Hand Function Test (JHFT)
The JHFT is a widely used objective test of arm and hand function during simulated activities of daily living that includes a variety of timed motor activities and is traditionally performed in a seated position (Jebsen et al., 1969). Clinically, the JHFT involves seven subtests, including turning over cards (Card Turning), picking up small objects (paper clips) and placing them in a can (Small Objects), picking up small objects (raw kidney beans) with a teaspoon and placing them in a can (Simulated Feeding), stacking four checkers (Checker Stacking), moving light cans (Light Cans), and moving heavy cans (Heavy Cans). The seventh JHFT subtest involves copying a written sentence that includes 24 letters at a 3rd grade reading difficulty. The writing subtest was not included in the present study because of its dependence on education level and hand dominance (Beebe & Lang, 2009; Hummel et al., 2005). Thus, in this study, our primary measure of JHFT performance was the total time to complete six of the seven subtests, excluding the writing test. We also used time on the six individual subtests as secondary measures of performance to identify which specific subtests, if any, were affected when performed in a standing position.
Center of Pressure Measurement During Standing
During all standing trials, participants stood on a force platform (AMTI, Watertown, MA) for the measurement of center of pressure (200 Hz). Center of pressure represents the center of the distribution of all forces acting on the support surface and is widely used as a measure of balance; center of pressure moves continuously to keep the center of mass within the base of support (i.e., the feet when standing) (Shumway-Cook & Woollacott, 2017). We expected an increase in center of pressure movement during the performance of the JHFT compared with static standing because of the weight shifts required to complete the items. The purpose of including this measurement was to describe the magnitude of center of pressure movements and to examine any differences between right and left arm JHFT performance if found.
Prior to performance of the JHFT in standing, a single measurement of static postural sway was measured. For this trial, individuals stood on the platform with the arms at the side and looked at a cross hanging 127 cm away for 10 s. Next, during each item of the JHFT performed in standing, center of pressure was measured for 10 s; the start of collection of center of pressure data coincided with a verbal “Go” signal to begin the JHFT item. After completion of each JHFT item, the participant was instructed to stand with the arms at the side and look at the cross similar to the static trial. Center of pressure movement was quantified as total path length (total distance traveled), a measure of the total amount of postural sway, and 95% ellipse area (size of spatial distribution), a measure of the total area of postural sway. In general, a higher value for total path length and 95% ellipse area represent a greater amount or area of postural sway. These measures have frequently been used to quantify postural sway in a variety of contexts and populations (Boisgontier et al., 2013; Bonnet et al., 2009; Kiers et al., 2013; Plummer et al., 2013).
Experimental Procedure
Data were collected during two sessions. During each session, the JHFT was completed with either the right or left hand; the order of the hand tested in the first session was counterbalanced across participants. The two sessions were separated by one week to provide a washout period between arms. In the first session, six practice trials of the JHFT were completed in sitting. The practice trials were provided to stabilize performance before the test trials as even healthy young adults can exhibit significant within-session practice effects; six trials were sufficient to stabilize JHFT performance in previous studies (Boggio et al., 2006; Hummel et al., 2005). Next, two test trials were completed: one in sitting and one in standing; the order of test position was counterbalanced across participants. In the second session, the experimental procedure was the same (six seated practice trials followed by two test trials) but was completed with the other hand. A standard set of verbal instructions was used for all JHFT trials. Table height was standardized across participants at 29 inches for sitting trials (consistent with standard table height) and 36 inches for standing trials (consistent with standard countertop height). For sitting trials, a standard chair height of 17 inches was used for all participants.
Statistical Analysis
All statistical tests were completed with SPSS 22.0 (IBM Corp., Armonk, NY). Data were checked for normality using the Shapiro–Wilk test (p > .05); normally distributed measures were analyzed with a repeated measures analysis of variance (ANOVA) while non-normally distributed measures were analyzed with a Wilcoxon Signed Rank test. The practice trials were analyzed and reported on previously (Schaefer et al., 2018). To determine the effect of standing on JHFT total time, a repeated measures ANOVA was performed on the test trials with factors for position (sitting, standing) and arm (right, left). To determine the effect of standing on individual items of the JHFT, a repeated measures ANOVA was performed separately for each task item with factors for position and arm; two items were not normally distributed (Card Turning and Small Objects) and were compared using a Wilcoxon Signed Rank test. Significant interactions or main effects were followed by a repeated measures ANOVA for each individual item or arm. Center of pressure measures were averaged across JHFT items and compared with static standing using a Wilcoxon Signed Rank test. Significance level was set at p < .05; for analyses of individual subtests, the significance level was set at a corrected p < .008 (0.05/6 total subtests). Partial eta squared (η2) was used to estimate the effect size of any differences in JHFT performance (η2 of 0.01–0.059 = small effect; 0.06–0.139 = medium effect; ≥0.14 = large effect) (Cohen, 1988).
Results
Total time to complete the JHFT in both the right and left arms improved within each session during the practice trials and was stable by the fourth trial (Schaefer et al., 2018). On the last practice trial, total time was similar between the right (26.7 ± 0.7 sec) and left (26.8 ± 0.7 sec) hands.
Effect of Standing on JHFT Total Time
For both hands, total time to complete the JHFT increased when performed in standing compared with sitting (Figure 1; main effect of position: F1,11 = 11.97, p = .005, η2 = 0.521). There was no difference in total time between arms (p = .982) and no interaction between arm and position (p = .711). On average, JHFT total time increased from sitting to standing by 4.4% in the right hand and by 5.6% in the left hand.
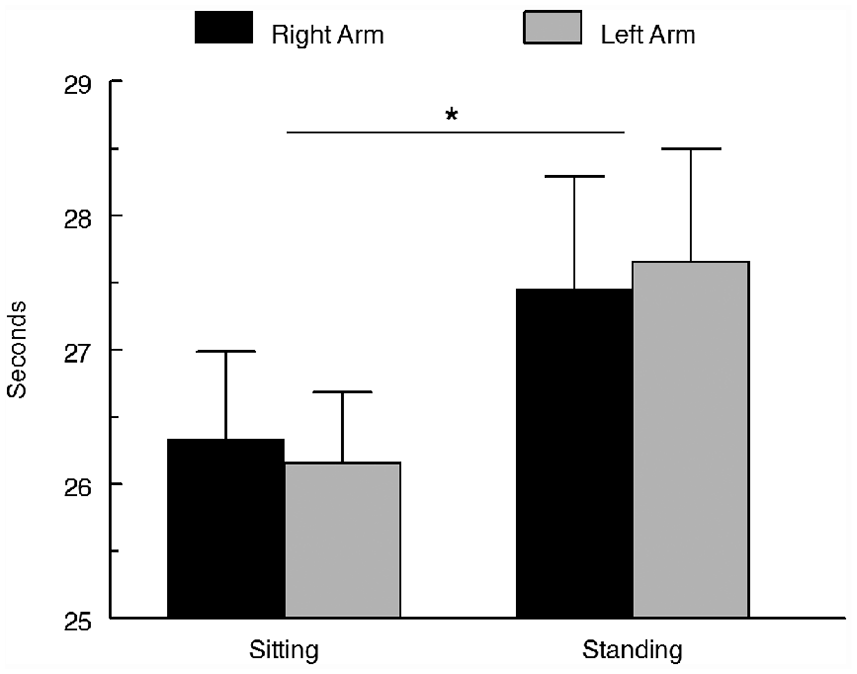
Total time to complete the JHFT by arm and position (mean ± standard error).
Effect of Standing on JHFT Subtest Times
Mean time to complete each subtest of the JHFT is shown in Figure 2 and Table 1. Most subtests showed an increase in performance time in standing compared with sitting. However, Checker Stacking was the only task that showed a statistically significant increase in completion time in standing in both arms (F1,11 = 18.81, p = .001, η2 = 0.631); there was a mean change of 760 ms for the right arm and a mean change of 750 ms for the left arm. Card Turning also showed a significant increase in completion time in standing, but only for the left arm (Z = 3.06, p = .002; mean difference 390 ms). A difference between arms was seen for Simulated Feeding (F1,11 = 6.91, p = .023, η2 = 0.386); although this difference did not meet the corrected significance level, a large effect size was present. For this item, individuals were faster with the right hand compared with the left hand (mean difference between arms: sitting 490 ms; standing 600 ms).
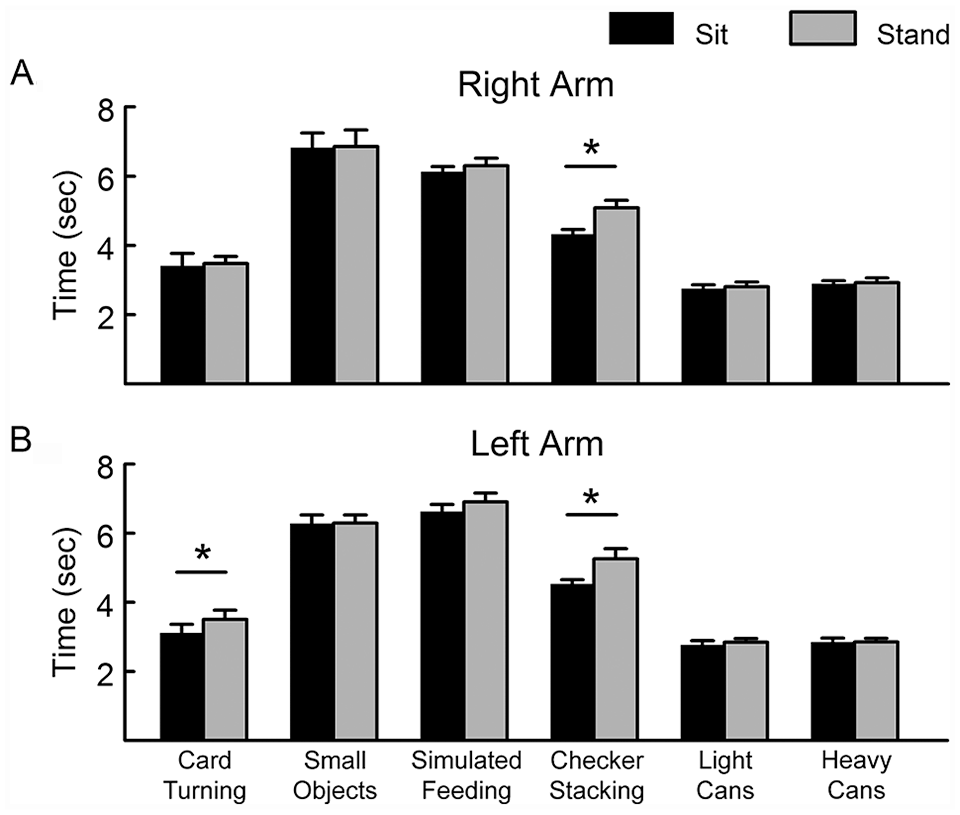
Mean time ± standard error to complete individual subtests of the JHFT by position (sitting, standing) for the right arm (A) and left arm (B).
Jebsen Subtest Performance Time.
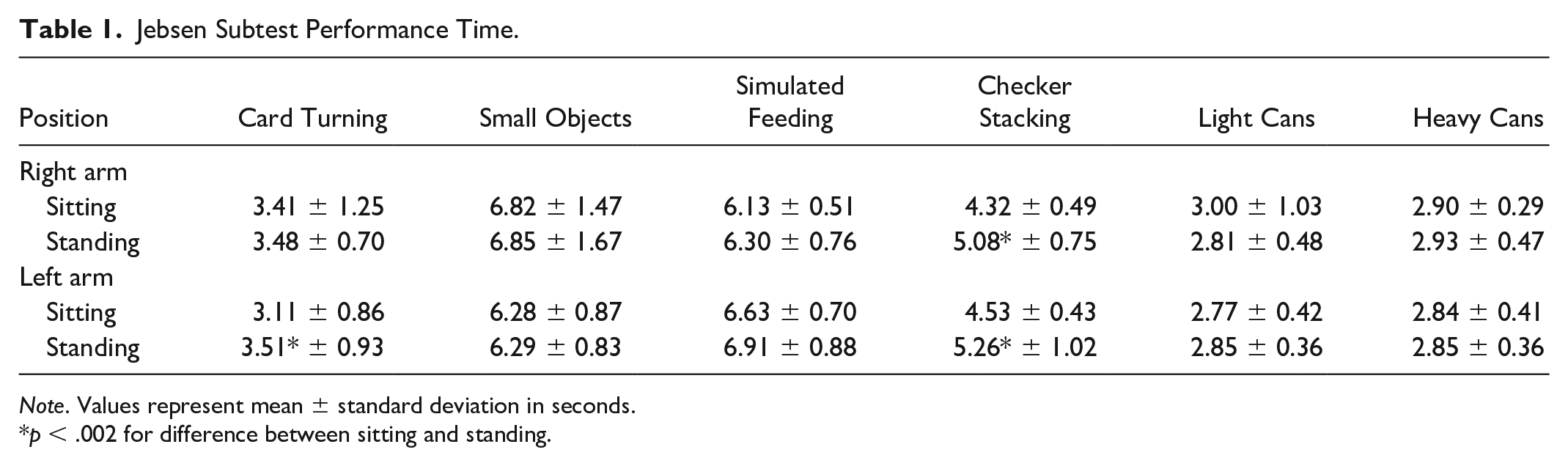
Note. Values represent mean ± standard deviation in seconds.
p < .002 for difference between sitting and standing.
Center of Pressure Movement During JHFT Performance in Standing
Path length and 95% ellipse area during static standing were similar to a previous study with comparable collection parameters (Melzer et al., 2001). As expected, there was an increase in center of pressure movement during the JHFT performance compared with static stance (Table 2, Figure 3). The magnitude of both path length and 95% ellipse area varied for each subtest item with the largest amount of postural sway tending to be during Card Turning and Simulated Feeding and the smallest amount during Checker Stacking. Mean center of pressure path length and 95% ellipse area across all subtests increased during the JHFT performance compared with static stance with the right arm (mean path length: 40.9 ± 19.0; mean 95% ellipse area: 17.9 ± 26.3) and left arm (mean path length: 43.3 ± 10.0; mean 95% ellipse area: 14.2 ± 11.6; Z > 2.82, p < .005 for all comparisons). There was no difference in mean center of pressure movement between the right and left arms (Z < 1.41, p > .158).
Center of Pressure Measures by Jebsen Subtest Item.
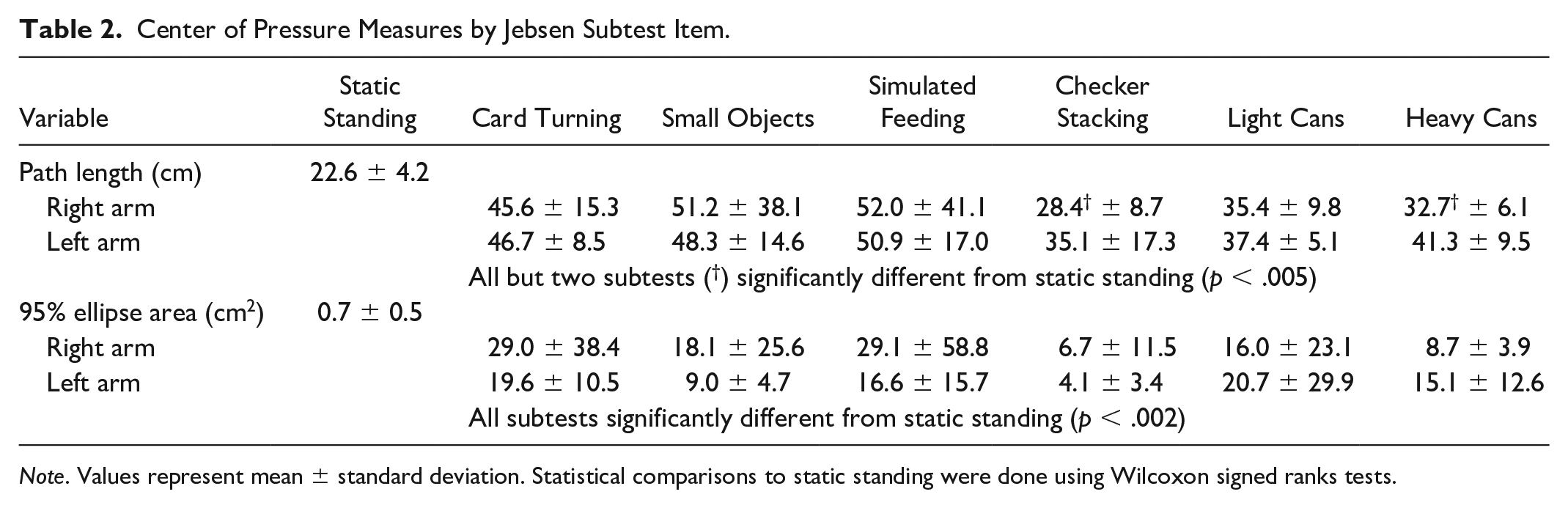
Note. Values represent mean ± standard deviation. Statistical comparisons to static standing were done using Wilcoxon signed ranks tests.
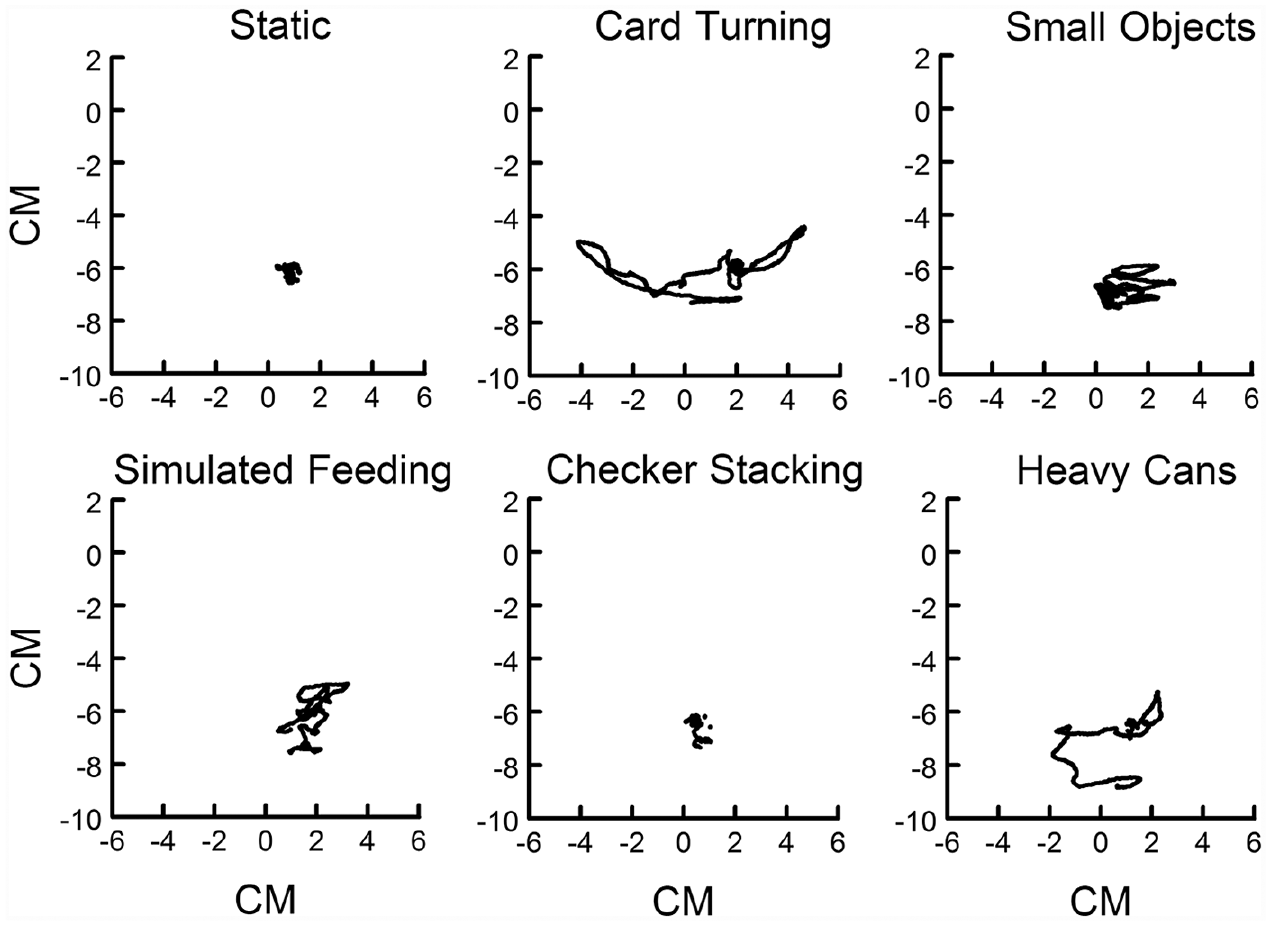
Center of pressure position data during static stance and the performance of JHFT subtest items in standing with the right hand for an individual participant.
Discussion
This study examined the effect of standing on a standardized measure of arm and hand function. Overall, total time to complete the JHFT increased when performed in standing compared with sitting, even in a young, nondisabled population. The effect of standing on JHFT performance was similar between the right, dominant and left, nondominant arms. The item that showed the strongest effect of standing was the Checker Stacking subtest, an item that requires precision during checker placement. The findings of the current study suggest that standing may impact the performance of this standardized measure of arm and hand function and should be investigated further in clinical populations.
To our knowledge, this is the first study to show an effect of standing on a standardized measure of upper extremity function. Several previous studies have suggested that the performance of skilled arm and hand movements is affected by the standing position. However, these studies have utilized laboratory-based tasks that required significant instrumentation, involved constrained, segmented upper extremity movement that required reaching alone or grasping alone (Berrigan et al., 2006; Chen et al., 2016; Cuisinier et al., 2005; Pozzo et al., 2002), or primarily focused on the effect of upper extremity movement on postural control (Aruin & Latash, 1995; Huang & Brown, 2015; McCombe Waller & Prettyman, 2012). The present study utilized the JHFT, a reliable, standardized measure of upper extremity function, which includes completion of functional tasks that require a combination of reach and grasp movements. The JHFT is accessible to researchers and clinicians with the purchase of a kit but without the need for instrumented equipment (e.g., motion capture system) and can be used in both healthy adults (Boggio et al., 2006; Convento et al., 2014) and clinical populations (Beebe & Lang, 2009; Mak et al., 2015; Weinstock-Zlotnick & Mehta, 2016). Our results suggest that the JHFT is sensitive to the effects of standing on upper extremity function and may be a useful tool in future studies investigating arm function in standing.
The performance of a skilled arm and hand task in standing could be viewed as a dual-task condition in which two tasks are performed at the same time. Completion of skilled upper extremity tasks in standing requires temporal and spatial coordination between movement of the arm and postural control (Aruin & Latash, 1995; Berrigan et al., 2006), with each component having its own attentional requirements (Goh et al., 2012; Schaefer & Lang, 2012; Woollacott & Shumway-Cook, 2002). Dual-task interference, defined as a decrease in one or both tasks’ performance relative to when it is performed by itself (Kinsbourne, 1981; Woollacott & Shumway-Cook, 2002), has been shown in a variety of tasks and clinical populations (Kelly et al., 2012; Plummer et al., 2013; Wajda & Sosnoff, 2015), including in young, nondisabled adults (Plummer et al., 2015; Schaefer et al., 2016). Alternatively, the performance of skilled upper extremity movements in standing could be viewed as a distinct task from the same movements in sitting, where the planning and execution of the arm movement and postural control are part of a single control strategy (Pozzo et al., 2002). In this case, the increase in completion time of the JHFT in standing would not represent a decrease in arm performance but instead performance of a distinct task. Although the present study cannot distinguish between these alternatives, future studies could explore the mechanisms behind the increase in performance time when the JHFT was completed in standing compared with sitting.
While performance time for most subtests increased when moving from sitting to standing, the individual item that showed the strongest effect of standing was the Checker Stacking subtest, suggesting this item made the largest contribution to the increase in JHFT total time in standing. This item requires an individual to carefully stack four checkers without knocking the stack over. While several subtests require fine motor coordination, Checker Stacking requires relatively greater precision and accuracy for object placement than other test items such as picking up small objects or simulated feeding (i.e., placing checker on another checker versus placing object in a large-mouth can). Previous studies have found that the level of dual-task interference can change based on changes in task demands (Hall et al., 2011; Wild et al., 2013). In addition, Berrigan et al. (2006) compared goal-directed reach movements in sitting and standing; decrements in reach performance were only seen when the accuracy demands of the reach task were high. Overall, this result suggests that arm and hand tasks with high accuracy demands may be more susceptible to the added demands of standing in young adults and should be investigated further.
There was no difference between the dominant and nondominant arms in the response to the standing position as hypothesized, except for a single subtest (Card Turning). We expected a greater effect in the nondominant left arm as this arm has been reported to have slower JHFT performance (Hackel et al., 1992; Jebsen et al., 1969; Mak et al., 2015), and, therefore, might be more susceptible to the effect of standing. Unlike these previous studies, the primary aim of the present study was to examine the effect of standing on JHFT performance. Therefore, our participants completed a set of practice trials prior to testing to achieve stable performance. At the end of practice, the JHFT total time (in sitting) did not differ between the two arms. This practice may have contributed to the consistent response to standing seen between the right and left arms.
Center of pressure movement during performance of the JHFT in standing varied for subtest items. Center of pressure is a measure of postural sway and moves continuously to keep the center of mass within the base of support. The movements of the center of pressure observed in the present study likely represent a combination of anticipatory postural adjustments (in anticipation of the postural disturbance caused by the movement of the arm) and reactive postural adjustments (in response to postural perturbation caused by movement of the arm) to successfully complete the upper extremity task (Shumway-Cook & Woollacott, 2017). Several studies have shown that task demands influence the postural adjustments seen during skilled upper extremity tasks in standing (Dierijck et al., 2020; Huang & Brown, 2015; Kennefick et al., 2018; Tijtgat et al., 2013). The center of pressure values found in the present study of young, nondisabled individuals provide a baseline for comparison in future studies in individuals with arm motor deficits, standing postural control deficits, or both.
There are a few limitations to consider when interpreting the results of this study. First, table height was held constant across all participants for both the sitting condition (29 inches) and standing condition (36 inches). We chose these heights as they represent standard desk and counter heights, respectively, and, therefore, represent a typical, real-world environment. This choice is consistent with our use of a standardized measure of upper extremity function (versus a laboratory task) that can be implemented efficiently in both the research and clinical environments. However, given that participant height varied, arm position in the sitting and standing positions varied between participants. Future studies could investigate the effect of standing on the performance of skilled arm tasks keeping the relative height of the surface to the individual and, therefore, arm position, constant. Second, several practice trials of the JHFT were completed in sitting prior to test trials (Schaefer et al., 2018). Practice trials were completed in sitting based on the suggested protocol for the JHFT. We cannot determine if practice trials completed in standing would lead to the same result found here. Future work could investigate this factor further. Third, while we found an increase in performance time to complete the JHFT in standing, we cannot determine if the magnitude of this increase is functionally meaningful. However, the results of the present study provide a reference point for the interpretation of changes in studies in clinical populations where determination of clinical meaningfulness will be important. Fourth, our sample size may not have been sufficient to find differences between sitting and standing for individual subtest items. Given the findings of the present study, future studies should include a larger population to specifically investigate differences on subtest items. Finally, the JHFT is a time-based measure of upper extremity function; it does not include an assessment of movement strategy or movement quality. The effect of standing on arm and hand function in clinical populations that have motor impairments may also be evident in measures of movement quality. Future studies on the effect of standing on arm and hand function should consider the effect of standing on measures of both performance time and movement quality.
How might these findings improve occupational therapy practice or treatment planning? Many functional tasks that include skilled arm and hand movements are frequently completed in standing (e.g., meal preparation in the kitchen). These tasks require an individual to maintain postural control while simultaneously performing the skilled arm task. Measurement of arm function in sitting provides important information on arm motor capacity; measurement of arm function in standing may provide insight into arm motor capacity within the context of standing postural control demands, a condition that has real-world, functional context, and may help determine whether training of arm function in standing (McCombe Waller & Prettyman, 2012) is appropriate. The results of the present study, while completed in a young, healthy population, suggest that the JHFT may be sensitive to the effects of standing and that further research in clinical populations is warranted.
Conclusions
JHFT performance decreased when completed in standing compared with sitting in young, nondisabled adults. Increased performance times in standing were seen in both the dominant, right arm and nondominant, left arm. These results may have implications for individuals with deficits in arm function and/or postural control and suggest that research in these clinical populations is warranted. Given the frequency with which functional arm tasks are completed in standing in everyday life, an improved understanding of how skilled arm and hand tasks are performed in a standing posture is needed.
Footnotes
Authors’ Note
This study was approved by the University of South Carolina Institutional Review Board (Pro00048852).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by grants 15SDG24970011 from the American Heart Association and K01AG047926 from the National Institutes of Health. This work was presented at the 2016 North American Society for the Psychology of Sport and Physical Activity Annual Conference, Montreal, Canada.