
Abstract
Powered wheelchair standing devices (PWSDs) allow supported standing for activity; however, little is known about their use. To understand factors affecting use of supported standing for participation among boys with Duchenne muscular dystrophy (DMD) and characteristics of successful users, we gathered data over 7 days from boys who had used PWSDs for 24 months, using a smartphone application. We used descriptive statistics to identify factors that affected their participation. Physical/social engagement and independence were motivators for standing in PWSDs. Enablers included positive attitudinal/social environments. Barriers included pain during supported standing and lack of physical environment accessibility. The characteristics of successful users were identified. Supported standing via PWSDs has potential to improve participation for boys with DMD. The disease stage, individual personal factors and environmental supports impact on use. Therapists should carefully consider and manage factors that impact on uptake and sustainability of use.
Introduction
Duchenne Muscular Dystrophy (DMD) is the most common inherited neuromuscular disease affecting boys, with progressive loss of mobility in childhood (Mah et al., 2014). Medical and rehabilitative management have extended life expectancy (Birnkrant et al., 2018), but boys experience social and community disengagement due to declining physical ability (Andrews & Wahl, 2018; Bendixen et al., 2013; Bray et al., 2011; Fee & Hinton, 2011; Pangalila et al., 2015).
The role for allied health professionals is to provide assessment and intervention to maximize independence, function and participation in daily life and prevent unnecessary secondary disability (Birnkrant et al., 2018; Case et al., 2018). The window for intervention needs careful anticipatory planning to minimize the impact of physical deterioration and social isolation. This will enable continued development and optimization of daily function. Enabling interventions such as assistive technology, activities, and community engagement overcome the impact of declining physical status on participation (Bendixen et al., 2012, 2013; Bray et al., 2010, 2011; Lue et al., 2017). Participation refers to involvement in life situations (World Health Organisation, 2007), which involves motivation, feeling competent, self-efficacy, self-determination (Baum, 2011; Deci & Ryan, 2000) and individual personal factors (Egilson & Traustadóttir, 2009). Interventions that maximize enablers and minimize personal and environmental barriers to participation are important (Christiansen et al., 2015; Colver, 2009; Gudgeon & Kirk, 2015; Raghavendra, 2013).
While a conventional power wheelchair (PWC) is a primary enabling intervention for boys with DMD aged 8 to 14 years (Birnkrant et al., 2018; Case et al., 2018; Muscular Dystrophy Campaign, 2011), prolonged sitting and wheelchair dependency leads to problems such as genitourinary problems (Backhouse & Harding, 2006), chronic pain and orthopedic complications (Engel et al., 2009; Richardson & Frank, 2009; Silva et al., 2016). Equipment such as standing frames are often recommended for physiological benefits for boys with DMD but poor adherence to static standing devices prevents optimum use (Pandya et al., 2016; Pedlow et al., 2019; Townsend et al., 2016).
Supported standing in a powered wheelchair standing device (PWSD; also known as a sit-to-stand wheelchair) provides mobility and independence for moving from sitting to standing and has attracted increasing interest for boys with DMD (Case et al., 2018; Mannlein & Pangilinan, 2008; Pedlow et al., 2019; Schofield et al., 2020; Townsend et al., 2016). It is important to understand the use of the supported standing feature and prevent its abandonment since, without it, the PWSD merely performs the function of a seated PWC which could have been provided at lower cost. Supported standing in PWSDs by boys with DMD has potential to enable participation in everyday activities (Vorster et al., 2019), maintain musculoskeletal status and mental health benefits (Bayley et al., 2020). According to consensus guidelines on prescription of PWSDs for boys with DMD (Schofield et al., 2020), therapists and users agree on necessary considerations. However, peer-reviewed literature is limited (Pedlow et al., 2019). Research remains limited despite numerous recommendations for studies of functional, behavioral, cognitive, and participation outcomes of supported standing (Craig et al., 2016; Dicianno et al., 2016; Lukersmith, 2012; Nordstrom, Naslund, et al., 2014; Paleg et al., 2013; Townsend et al., 2016).
The gap in understanding how boys with DMD use supported standing in PWSDs is partly attributable to a lack of responsive and sensitive outcome measures. Electronic diary methods offer a potential solution by capturing in-the-moment participation. The experience sampling method (ESM) (Hektner et al., 2007), using personal electronic devices, has been found to be valid and reliable for providing details of everyday experience in the DMD population (Bray et al., 2010, 2017). The aim of this article is to explore participation by boys with DMD using supported standing by addressing the following research questions: (a) What typical activities do boys engage in using supported standing? (b) What intrinsic and extrinsic barriers, enablers, and motivators impact on the use of standing and PWSDs? (c) What are the characteristics of boys who most successfully use supported standing?
Methods
We conducted a clinician-led descriptive study with boys with DMD and their parents/carers. ENABLE NSW (NSW state equipment supplier), Mitech (NSW supplier), and charities provided grants to purchase LEVO C3 PWSDs for participants between April 2014 and September 2015. The LEVO C3 is a model of PWSD imported into Australia, manufactured by LEVO in Wohlen, Switzerland.
Participants
We recruited participants from two pediatric neuromuscular clinics in Sydney NSW Australia via convenience sampling through usual clinical care. All the boys lived in metropolitan Sydney, NSW Australia. Inclusion criteria were a confirmed DMD diagnosis according to standard diagnostic criteria, supply of a PWSD via the aforementioned grants and access to a smartphone.
Nine boys and guardians/parents provided written consent to participate in the study. This study was approved by the Human Research Ethics Committee at the Sydney Children’s Hospitals Network. Table 1 presents individual characteristics and summarizes information about the boys, including Egen Klassifikation (EK) Scale scores (Steffensen et al., 2001, 2002) and stages of DMD as described by the DMD Care Considerations Guidelines (Birnkrant et al., 2018). The EK scale measures functional abilities in people with neuromuscular diseases on a 30-point scale. Higher scores indicate a higher level of disability. The EK scale has been found to produce reliable and valid data for monitoring functional capacity (e.g., wheelchair use, ability to turn in bed, and ability with upper limbs) and can guide anticipatory clinical management. The DMD Care Considerations Guidelines recognize five stages in the progression of DMD: 1. At diagnosis; 2. Early ambulatory; 3. Late ambulatory; 4. Early nonambulatory; and 5. Late nonambulatory.
Participant Information.

Notes. PWSD = powered wheelchair standing device; CALD = culturally and linguistically diverse; Y = Yes; N = No; NC = no complications; C = complications; AFO = ankle-foot orthosis; EK2 = Egen Klassifikation 2 (Steffensen et al., 2001) measures change in functional abilities over time in neuromuscular diseases. Scores on this ordinal scale range from 0 to 30 points where 0 represents the highest level of independent function and 30 the lowest level; DMD stage = refers to the Duchenne muscular dystrophy stage according to DMD Care Considerations guidelines (Birnkrant et al., 2018). The five stages in the progression of DMD: 1. At diagnosis; 2. Early ambulatory; 3. Late ambulatory; 4. Early nonambulatory; and 5. Late nonambulatory.
Participants were representative across the ambulatory and nonambulatory stages 2 to 5 of DMD when power wheelchairs are prescribed. One boy (
Two boys (
Five boys
Outcome Measure
We used a purpose-built smartphone-app-based standing survey to collect information about (a) activities in which the boys used supported standing, (b) initiation of standing, (c) reasons for using standing, (d) physical and (e) social environments in which boys used standing, and (f) reports of pain. The surveys were delivered using the Participation in Everyday Life Application (PIEL) app https://pielsurvey.org/ (Blue Jay Ventures Pty Ltd, 2017; Jessup et al., 2012).
The standing survey consisted of 11 potential questions, the number depending on the responses selected for previous questions (e.g., if a participant answered “Do you have pain in standing?” with a “Yes” response, the next question would be, “Please tell me where the pain is.”). A summary of the standing survey questions is provided as Supplementary Material.
Procedures
We introduced the standing survey after the boys had used PWSDs for 24 months. We considered 24 months of experience adequate to ensure boys had incorporated the device into everyday life and that standing surveys reflected typical use. The primary investigator introduced the standing survey and provided training in person. The participants downloaded the PIEL app on their smartphones and imported the emailed standing survey. Boys completed a survey each time they used supported standing over a 7-day period. Each survey took 2 to 3 minutes to complete. Parents or teacher aides completed the survey when a boy was unable to do so due to task requirements. After 7 days, results were emailed to the primary investigator in the form of a Microsoft Excel (2017 version) spreadsheet.
Data Analysis
The PIEL app generated a spreadsheet for each boy recording total number of standing surveys and coded question responses. No surveys were excluded from analysis. We grouped responses into fewer categories to allow analysis. Tasks and physical/social environmental contexts were grouped into meaningful categories (e.g., occasions of toileting [urination] were identified as when alone or with a carer). We analyzed responses using descriptive statistics (see Figure 1 and Table 2).
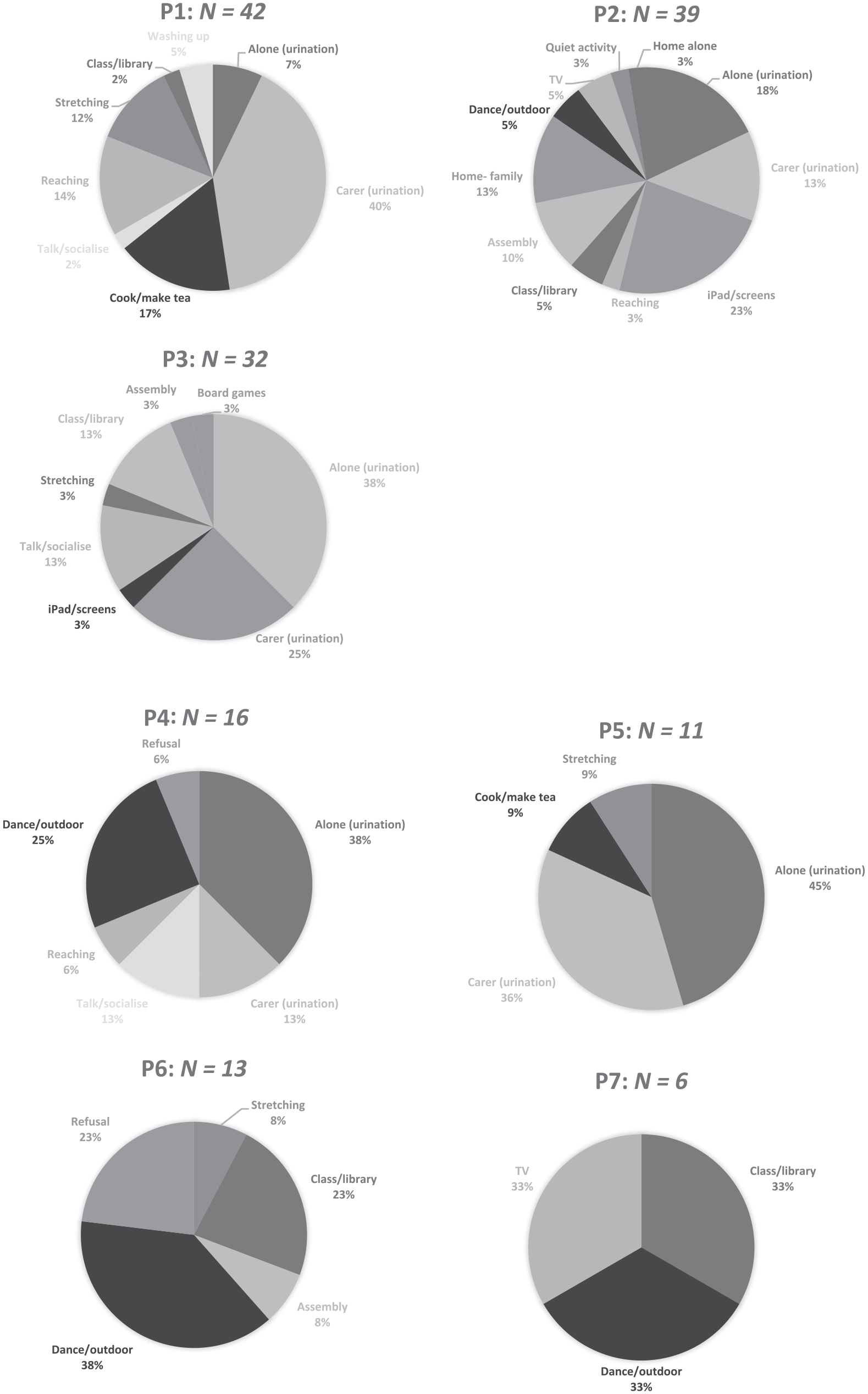
Individual participant responses to the question “What are you doing in supported standing?”
Supported Standing (SS) Survey Data From 7-Day Monitoring Period.

Note. * Denotes unknown (P7 had malfunction of his PIEL survey). Results are unrecorded for “who with SS,” but we know from “where” question that he was in the playground × 2, at home watching movie × 2 and in class × 2.
Results
P1 to P7 regularly used the supported standing function and completed the PIEL app standing surveys. The app recorded 159 standing surveys in total (Table 3).
Number of Surveys Completed in 7-Day Standing Survey.

Everyday Tasks and Frequency of Supported Standing in PWSDs
P1, P2, and P3 used supported standing at least twice as often as the other boys. All five nonambulatory boys reported toileting (urination) as the most frequent activity in supported standing; 33 out of a total of 69 reports were of independent toileting. Other than toileting, nonambulatory boys participated in a variety of learning, social, leisure and physical activities (e.g., sport), and productivity tasks (e.g., cooking and countertop activities). Ambulatory boys (P6 and P7) used standing in the PWSDs most frequently in classroom activities and in active pursuits (i.e., sports, dance, outdoors) at school. Ambulatory boys never used PWSDs for toileting urination. Figure 1 details the type and frequency of tasks for individual boys.
Initiation and Reasons for Supported Standing in PWSDs
Both nonambulatory and ambulatory boys self-initiated standing on the majority of occasions, M = 78% of occasions (range 46%–100%). Two nonambulatory boys (P2 and P4) and one ambulatory boy (P6) needed frequent reminders from adult carers to initiate standing at home and school. Occasionally, P4 (once) and P6 (three times) refused to use supported standing when requested by carers. Reasons for refusals were given as “fatigue” and “pain.”
We designed the “why stand” question to learn boys’ motivations for using supported standing. Nonambulatory boys reported “stretching,” “need for standing,” and “easier to do the task”; and P6 (ambulatory) reported “stretching” and “being with others” as main reasons.
Environment
Other than toileting, nonambulatory boys used the PWSDs in both home and school environments. P1 (35.5%) and P2 (49%) reported most occasions of standing at home, with P3 standing more often at school. P4 was not able to use the PWSD at home indoors due to lack of ramp access. Other than toileting, P5 reported standing on two occasions at home. Ambulatory boys used supported standing in the PWSDs most often in school environments of classroom, hall, and playground. P6 did not use PWSD at home due to lack of accessible transport. P7 used standing twice at home (watching TV).
Adults were present for occasions of supported standing in PWSDs, either in one-to-one or group situations. This included counts of refusals when adults were recording the refusals. Being alone was possible for toileting urination for nonambulatory boys, but these boys were seldom alone in other activities.
Pain Reports in Supported Standing
P1, P2, and P3 reported little or no pain. P4 and P5 reported pain in 44% and 36% of standing events, respectively, in ankles, knees, and calves. Ambulatory boys reported pain in spine, knees, and calves when standing (P6, 15% of the time and P7, 33% of the time).
Discussion
Our study provided details on what boys with DMD do in supported standing. The PIEL Survey app https://pielsurvey.org/ (Blue Jay Ventures Pty Ltd, 2017) was easy to use and the standing survey yielded detailed information about the real-life context and frequency of use of supported standing in PWSDs in natural environments. We identified factors that enabled or hindered participation. Understanding the characteristics of boys who successfully use PWSDs in daily life can help clinicians identify boys most suited to using them. This will assist decision-making about, and prescription of, this high-cost equipment (Lukersmith, 2012; Schofield et al., 2020). Identifying the subset of “high frequency users” is also important for researchers. Recruiting successful users for future studies on DMD and PWSDs would power studies more effectively and strengthen any conclusions made on the outcomes of the PWSD intervention, especially in view of inconclusive evidence on physiological changes such as bone mineral density and range of motion (Bayley et al., 2020; Pedlow et al., 2019; Townsend et al., 2016).
Importantly, supported standing in a PWSD for urination was a powerful motivator for nonambulatory boys because they could complete this self-care task easily. PWSDs enabled the boys to achieve an important participation goal by facilitating independence in toileting at a time when they usually become dependent on others. PWSDs have the potential to support genitourinary health of young men with DMD by counteracting negative perceptions of dependency and overcoming problems of voiding postponement and reduced fluid intake (Backhouse & Harding, 2006; Zhu et al., 2015). The possibility for ease in toileting helped boys overcome ambivalence often associated with supported standing (Nordstrom, Naslund, et al., 2014).
While we were not able to measure durations of standing events, boys who used supported standing most often (P1–P3) reported engaging in a variety of activities. Our data support the effectiveness of standing for short periods in a variety of meaningful and purposeful activities (Nordstrom, Nyberg, et al., 2014). P1 made a smooth transition from ambulatory stage 3 to nonambulatory stage 4 during the 24-month study period and used standing most frequently of all the boys. Supported standing in PWSDs allowed social and physical engagement despite declining physical and functional abilities (Vorster et al., 2019). This contrasts with the commonly-cited abandonment of static standing devices (Pandya et al., 2016). Supported standing in PWSDs can help counteract low engagement in everyday activities of boys with DMD as they age (Bendixen et al., 2013). However, the low frequency use by the ambulatory boys and some non-ambulatory boys in our study, indicates that PWSDs need to be carefully prescribed and supplied at an optimal stage of disease progression, under certain environmental conditions, to boys with particular personal characteristics.
Among nonambulatory boys, pain was a barrier to using supported standing in PWSDs. P1, P2, and P3, likely benefited from successful lower limb management (orthotics, complication-free surgery), making standing pain-free to allow frequent and easy use for a wide variety of participation tasks and stretching. P4 and P5 experienced pain in supported standing and were less likely to stand. However, they considered it worthwhile to persevere with supported standing for independent toileting. Pain reports were mostly episodic and subsided with return to sitting or perching positions (i.e., release of stretch). We suspect that the ambulatory boys, P6 and P7, reported discomfort during dance and sport with able-bodied peers due to sustained end-of-range stretches in PWSD stand postures for long periods during these activities. Pain is known to affect boys and young men with DMD, often worsening with progression of disease (Engel et al., 2009; Silva et al., 2016; Zebracki & Drotar, 2008). Pain was a reported barrier for P9 who ceased standing in his PWSD.
Opportunity alone is not enough to enhance participation. Personal factors can impact greatly on engagement and participation of school age children (Egilson & Traustadóttir, 2009). Individual factors—abilities, motivation, and preference—often decided whether and how opportunities were used, and these factors changed over time, supporting the findings of Egilson and Traustadóttir (2009). Ambulatory boys (P6 and P7) did not always choose to use their PWSDs. Supported standing was least used at home as they reported walking indoors at home and standing on the floor independently for daily tasks. P6 had an accessible home environment but chose to use his PWSD at school only. However, the desire for social engagement appeared an important motivator for supported standing in the ambulatory boys to “keep up” with peers in active physical activities. With disease progression, supported standing in PWSDs for non-ambulatory boys might allow equality and connection to peers, as indicated by comments from P3 such as,
Occasional refusals to follow adult requests to use supported standing were not surprising in ambulatory boys. Feeling self-conscious and not wishing to draw attention affected personal choice regarding the use of standing in PWSDs in social situations. This was reported by both ambulatory and nonambulatory boys who stood less often (P4–P9), consistent with previous PWSD research (Vorster et al., 2019). Positive attitudinal and social environments facilitated and motivated boys to use supported standing in PWSD for engagement in activity. Adult presence (i.e., expectations and attitudinal environment support) seemed an important enabler, suggesting that boys needed support to learn to use the device and develop self-motivation.
Lack of wheelchair-access vans and home access prevented some boys from full-time use of PWSDs. This almost certainly contributed to lower frequency of supported standing. Four boys did not have wheelchair-accessible vans. P4 did not have ramp access to his home and therefore could not use his PWSD indoors. Ambulatory boys (P6 and P7) reported use of a manual wheelchair for outings due to ease of transport. Limitations in access to the physical environment are known to affect participation and quality of life of pediatric power wheelchair users (Gudgeon & Kirk, 2015).
There appears to be an optimum “window” of stage of disease progression (late stage 3 and stage 4 DMD) when supply of PWSDs for boys with optimal personal and environmental characteristics, allows effective and sustainable use. P1, P2, and P3 used supported standing at least twice as often as their counterparts. By examining personal and environmental factors for this subset of boys who used PWSDs frequently and effectively, we were able to identify likely characteristics of boys best suited to being supplied with them: little or no pain on supported standing; consistent lower limb physical therapy management; personal choice and motivation for standing in PWSDs; supportive physical environments and transport allowing full-time use; supportive social and attitudinal environments facilitated by adult caregivers.
Limitations
The number of participants was limited by the number of supplier and subsidy grants offered to fund PWSDs. Thus, our sample size was small. However, the sample included boys representative across the ambulatory and nonambulatory stages 2 to 5 of DMD when power wheelchairs are prescribed, and different patterns of use provided data to answer our research questions.
Future Research Directions
Enrolling participants who are high-frequency users of supported standing in PWSDs is important when it comes to powering recommended future studies on participation and physiological changes. Furthermore, research to identify specific intervention strategies that enable effective use of supported standing in PWSDs would be worthwhile, aiming to minimize the barriers experienced by low-frequency users.
Smartphone application technology may provide valuable tools for use in both clinical practice and further research. Apps using smart devices and Bluetooth for PWSD models are now available to monitor inclinometry (angle of stance) and exact standing duration but were unavailable at the time of our data collection. Combining apps would enhance data collection on outcomes of interest to researchers.
Longitudinal studies should improve our understanding of the longevity and sustainability of use of supported standing in PWSDs for individuals with a progressive disease such as DMD. Analysis of possible cost savings from use of PWSDs by nonambulatory boys for independence in maintaining toileting and other aspects of everyday life deserves further investigation.
Implications for Occupational Therapy Practice
Boys with DMD can use supported standing in PWSDs to facilitate participation, potentially reducing the impact of progressive loss of function on daily life.
Therapists should consider anticipatory planning (including funding time frames); maximizing enablers and minimizing barriers for successful use of supported standing in PWSDs; and the characteristics of boys best suited to using them; as these issues impact uptake and sustainability of use.
Researchers and clinicians can use smartphone apps to monitor and collect data on participation.
Conclusions
Supported standing via PWSDs has the potential to improve participation for boys with DMD. The disease stage, individual personal factors and environmental supports impact on use of the supported standing function. Therapists should carefully consider and manage the barriers and enabling factors when prescribing PWSDs as they impact on uptake and sustainability of use.
Supplemental Material
sj-pdf-1-otj-10.1177_15394492211004844 – Supplemental material for Everyday Life Participation Using Powered Wheelchair Standing Devices by Boys With DMD
Supplemental material, sj-pdf-1-otj-10.1177_15394492211004844 for Everyday Life Participation Using Powered Wheelchair Standing Devices by Boys With DMD by Helena Young, Paula Bray, Kausik McKinnon, Joshua Burns and Anita Bundy in OTJR: Occupation, Participation and Health
Footnotes
Acknowledgements
The authors wish to thank K.M. for his invaluable assistance with data management and analysis. The authors wish to thank our participants and their carers for their time and cooperation over the study period.
Authorship
Author affiliations are named. All the named authors have contributed to the work and agree to the presented findings. H.Y. designed the study with input from P.B., J.B., and A.C.B. H.Y. coordinated the ethics approval processes and designed the study survey questions with input from P.B. and A.C.B. H.Y. and K.M. managed the collection of data and designed, implemented, and executed the statistical analysis. H.Y., A.C.B., and P.B. led the interpretation of findings with input from J.B. H.Y. drafted the manuscript. All the authors reviewed the manuscript and approved the decision to submit for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The authors are grateful for financial support to supply the powered wheelchair standing devices from Mitech NSW, and individual top-up grants from registered charities MDNSW and Variety the Children’s Charity Freedom program. Mitech NSW also provided 3 years of service and maintenance plans for the participants. Save our Sons (registered charity) provided a grant to the project for travel expenses for boys and parents.
Research Ethics and Patient Consent
Approval for the study was received from Sydney Children’s Hospitals Network Human Research Ethics Committee for two participating sites: The Children’s Hospital at Westmead and the Sydney Children’s Hospital (HREC Reference LNR/13/SCHN/222). Procedures were carried out in accordance with relevant institutional or national bodies and consistent with revised (2013) Helsinki Declaration (![]() ), including obtaining informed written consent from participants to collect and use data for stated research purposes.
), including obtaining informed written consent from participants to collect and use data for stated research purposes.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.