
Abstract
There is known to be a decrease in quality of life and perceived occupational performance and satisfaction following total knee arthroplasty (TKA). This study was planned to examine the effectiveness of a client-centered (CC) intervention with the telerehabilitation (TR) method on the quality of life, perceived occupational performance, and satisfaction after TKA. A total of 38 patients who had undergone TKA were randomly assigned to the CC and control groups. A 12-day intervention program was applied to the CC group. The Nottingham Health Profile (NHP) and Canadian Occupational Performance Measure (COPM) were applied before and after intervention. The 12-day intervention showed a strong effect on all parameters in the CC group (p<.001). In the postintervention comparisons, a significant difference was found in favor of the CC group (p < .001). CC interventions with the TR method can be used in post-TKA interventions.
Keywords
Introduction
Total knee arthroplasty (TKA) is an effective treatment for patients with knee osteoarthritis as it aims to reduce pain and improve disability, functional outcomes, and physical activity (Softness et al., 2017). In the acute postoperative period, problems are observed in many parameters such as pain, sleep, physical activity, psychological state, and activities of daily living (ADL), and these problems negatively affect the quality of life (Canovas & Dagneaux, 2018; Dorsey & Bradshaw, 2017; Hiraga et al., 2019). These situations experienced in the acute period cause occupational performance problems and make it difficult for individuals to adapt to ADL (Dorsey & Bradshaw, 2017; Hiraga et al., 2019). To prevent such difficulties, an interdisciplinary approach is taken to various postoperative treatments (Dorsey & Bradshaw, 2017; Feng et al., 2018). Occupational therapy interventions have an important place in these treatment approaches (Dorsey & Bradshaw, 2017).
Occupational therapy interventions used in rehabilitation approaches for lower extremity musculoskeletal disorders focus on training, increasing ADL performance, using compensatory strategies for functional limitations, using joint energy conservation strategies, activity pacing training, and providing functional mobility training through intervention approaches implemented by an interdisciplinary team (Dorsey & Bradshaw, 2017; Feng et al., 2018; Hiraga et al., 2019). A systematic review focused on the importance of investigating the effects of client-centered (CC) approaches and the effects of occupational therapy interventions (American Occupational Therapy Association [AOTA], 2020; Dorsey & Bradshaw, 2017). The systematic review results showed a strong role for occupational therapy in treating clients with lower extremity musculoskeletal disorders. However, it has also been stated that it is important to apply cost-effective approaches in rehabilitation services and to find solutions for accessibility problems (Hung & Fong, 2019). The COVID-19 pandemic necessitated the development of alternative treatment methods because of the problems in accessibility to rehabilitation services caused by the various measures taken to address health concerns and prevent infection transmission (Negrini et al., 2020).
Telerehabilitation (TR), which can be delivered with information and communication technology, represents an innovative approach to overcome the barriers associated with face-to-face interventions (Hung & Fong, 2019; Negrini et al., 2020). TR technologies provide access to health care services by allowing remote service provision in the patient’s home or in other settings (Hung & Fong, 2019; Proffitt et al., 2021). In a recent study, researchers used TR methods to promote the occupational balance of university students (Pekçetin & Günal, 2021). Rehabilitation services in the natural environment of the home have the added advantage of making the treatment more realistic and more applicable in ADL (Hung & Fong, 2019; Proffitt et al., 2021). Furthermore, following the onset of the COVID-19 pandemic at the end of 2019 and the implementation of restrictions to daily life in March 2020, problems arose in accessing rehabilitation services (Negrini et al., 2020). It has been indicated by researchers in this field that TR applications can be used as an alternative method to overcome these problems (Negrini et al., 2020). However, there are various TR methods that can be applied, and no clinical consensus has yet been reached about the content design of TR interventions for TKA (Petersen et al., 2021). In addition, the TR method has problems such as insufficient internet infrastructure, the inability of the participants to adapt, and not knowing the applicability of assessment and interventions (Hung & Fong, 2019; Petersen et al., 2021).
The current study examines the effectiveness of CC intervention applied with the TR method on the quality of life, perceived occupational performance, and satisfaction of adults following TKA.
Method
This single-blinded, randomized controlled trial (RCT) was conducted to examine the effectiveness of CC intervention with the TR method for adults who had undergone TKA surgery. The study was designed according to the CONSORT statement, which provides a standardized method for RCT design (Schulz et al., 2010). Approval for the study was granted by the local ethics committee. Written informed consent was obtained from all participants prior to the study.
Participants
A total of 46 adults admitted to the occupational therapy department of a public university between January 2021 and March 2021 were screened. Patients who were eligible according to the evaluation and inclusion and exclusion criteria on the third day after TKA were included in the study. The study inclusion criteria were (a) age between 18 and 65 years; (b) Mini-Mental State Examination (MMSE) score of ≥24; (c) education level of at least completion of elementary school; (d) having undergone unilateral TKA surgery; (e) access to technological equipment; and (f) ability to understand and follow verbal instructions. The exclusion criteria were defined as (a) revision surgery; (b) having any chronic disease that will affect the rehabilitation process; (c) auditory and visual problems that may affect rehabilitation implementation and communication; (d) postoperative complications (e.g., nerve injury and deep vein thrombosis); and (e) attendance of any rehabilitation program (physiotherapy, speech therapy, psychotherapy, and so on) during the study period. According to the inclusion and exclusion criteria, five participants were excluded from participating in another program. The remaining 41 participants were randomized to either the control group or the CC intervention group using a computer-generated randomization technique. The allocation process was carried out by the second author of this study (Ö.K.). Further exclusions were made of one from the control group and two from the CC group, who did not complete the program, and thus the analysis was made of a sample of 38 adults (Figure 1).
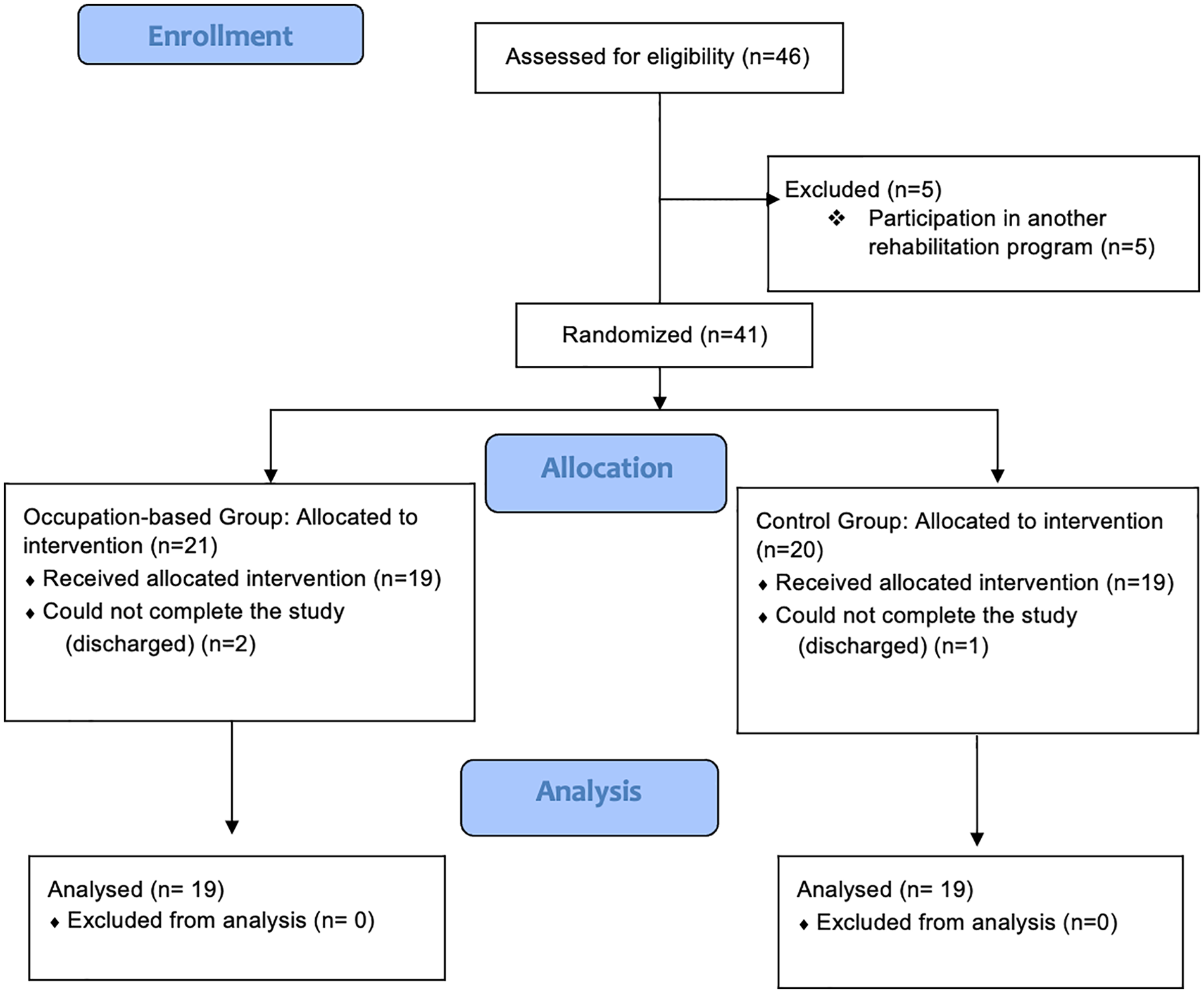
Consort diagram.
Measurement
The demographic characteristics of the participants were recorded, including age, sex, education level, body mass index (BMI), other people in the house where they lived, and marital status. The MMSE was used to determine the cognitive status included in the inclusion criteria. The Canadian Occupational Performance Measure (COPM) and the Nottingham Health Profile (NHP) were applied to all the participants twice, once before the intervention and again after the 12-day intervention. All assessments were made by a researcher (S.P.) who has 15 years of experience in the field and was blinded to the design of the study and group allocation. All the patients were assessed in occupational therapy clinical practice units (first and last sessions).
Assessments
Mini-Mental State Examination
This test, which was used in the inclusion criteria of the study, was used to determine the cognitive state of the participants. The MMSE assesses various cognitive functions, including memory, attention, and language. From a maximum total of 30 points, a score of 24 is accepted as the threshold value, with scores below this value indicating problems in cognitive functions (Folstein et al., 1983). Turkish validity and reliability studies of the test have been conducted (Güngen et al., 2002), and the researcher found the MMSE positive and negative predictive values of .90 and .95, respectively, and kappa score .86 (Güngen et al., 2002).
Canadian Occupational Performance Measure
This scale is a measure that determines the problems faced by individuals in the field of occupational performance through a semi-structured interview. Occupational performance problems are evaluated with self-reported performance and satisfaction scores. In the first step, ADL problems experienced by individuals in the areas of self-care, productivity, and leisure are determined, and each occupation is scored according to importance. The subject then selects a maximum of five occupations according to their importance scores and gives performance and satisfaction scores in a Likert-type system of 1 to 10 for each occupation. The overall performance and satisfaction scores are obtained as the total of the performance and satisfaction scores of each occupation divided by the number of occupations (Law et al., 2014). The Turkish COPM was used to evaluate the perceived occupational performance and satisfaction levels of the study participants and to create the CC intervention program (Torpil, 2021). The Turkish adaptation was performed, and the test–retest reliability of the Turkish version of COPM performance was .988 and satisfaction .986, indicating excellent reliability (Torpil, 2021).
Nottingham Health Profile
The NHP is a general quality-of-life questionnaire that measures perceived health problems and the level of these problems affecting normal ADL. The questionnaire consists of 38 items in six dimensions related to health status: energy (3 items), pain (8 items), emotional reactions (9 items), sleep (5 items), social isolation (5 items), and physical activity (8 items). Each item is answered as yes or no, and each section is scored between 0 and 100, with 0 indicating the best health status and 100 the worst health status (Hunt et al., 1981). In the Turkish adaptation study, the test–retest reliability of the subscales (dimensions) of the scale varied between .70 and .92, and internal consistency values ranged between 0.56 and 0.87, confirming its validity and reliability (Küçükdeveci et al., 2000).
Interventions
The intervention program consisted of one 45-min session every day for 12 consecutive days. The first 2 days of intervention in both the groups were home modifications training and transfer training. These training sessions were given using presentations and videos. For the remaining 10 days, the program was created and the CC method was used for the occupations specified in the COPM. The caregiver actively participated in the treatment to prevent any possible injuries and to perform the applications more smoothly during the entire intervention process. The TR interventions were delivered through programs such as Zoom, Skype, WhatsApp video call, or Microsoft Teams, according to the preference of the patient.
Home modifications training
Home modifications training was applied to eliminate problems in areas of the home that would be difficult for mobilization and could lead to injuries, such as the living room, bathroom, toilet, kitchen, bedroom, corridors, and stairs. Based on previous studies, training was given on home modifications, the use of adaptive equipment, the recommendation of assistive technology tools, the causes of falls in the house, and what should be considered to prevent falls (Sanford et al., 2006; Breeden, 2016). This training included information on the mobilization of individuals in ADL and how to increase mobilization and prevent various injuries, such as the use of grab bars, arranging furniture, using adequate lighting, how to prevent slipping on wet ground, arranging corridors to help transfer processes, using photocell lamps in corridors, having sufficient lighting in other areas, removing door thresholds, moving carpets and cables, using ramps, and rearranging armchairs/chairs/beds to facilitate the transfer process.
Transfer training
A transfer training program was created in accordance with the needs of the individuals and as specified in the literature (Singh & Lewallen, 2014). This training included how to safely transfer on wet floors, such as toilets and bathrooms; transfer to beds, chairs, and sofas; transfer from one room to another; and climbing the stairs.
CC intervention
The CC intervention developed according to the literature and based on a systematic therapy process, characterized by an active participatory attitude of both the participants after TKA process and the therapist, consisted of four phases (AOTA, 2020; De Vriendt et al., 2016; Enemark Larsen et al., 2018): (a) CC goal-setting, (b) negotiating a therapy plan, (c) the actual intervention, and (d) an evaluation of the outcome and finally reporting to relevant others. The key aspect of this intervention was the client-centered approach in which the therapist is trained to clarify the prioritized goals of the patient. The therapy procedure was implemented according to the prioritized goals determined in the COPM. The four stages are explained below:
First stage: Setting a measurable, realistic, and achievable goal for the solution of occupations involving performance problems.
Second stage: Considering and studying the pros and cons of possible solutions by brainstorming through the Canadian Model of Occupational Performance.
Third stage: After deciding on a possible solution, making a plan, and taking action: Adaptation of the occupation and making alterations to one or more of the following: who (involving another person), where (making a change in the place), when (changing the time), how (altering the way of application), and what (adding up new steps at the beginning or end of the occupation). Determining the new occupation, Planning the steps of the occupation (in accordance with priority), Bringing together occupation-related information and resources
Fourth stage: Revising the therapy process which has been activated with the CC training, receiving feedback about the experience of the patient, and making alterations to the course of action when necessary.
Statistical Analysis
Data were analyzed with SPSS version 25.0 statistical software. Data were presented as mean ± standard deviation values. The conformity of the data to normal distribution was analyzed using the Kolmogorov–Smirnov test. The data were seen not to be distributed normally, so nonparametric statistical methods were used. Differences between groups were analyzed with the chi-square test for nominal data. Comparisons between the groups were made using the Mann–Whitney U test. Pre- to postintervention changes within the groups were analyzed with the Wilcoxon signed-rank test. Statistical significance was evaluated at levels of 0.05.
The power of the study and effect sizes were analyzed using G*Power software, version 3.1.9.2. Power analysis was performed to calculate the sample size. It was determined that 17 participants were needed in each group to ensure a power of 80%, assuming a two-tailed test for α = .05. The effect size was calculated using the means and standard deviations of the groups. Effect size benchmarks were determined as <0.30, 0.30 to 0.80, and >0.80, interpreted as small, moderate, and strong, respectively (Cohen, 1992).
Results
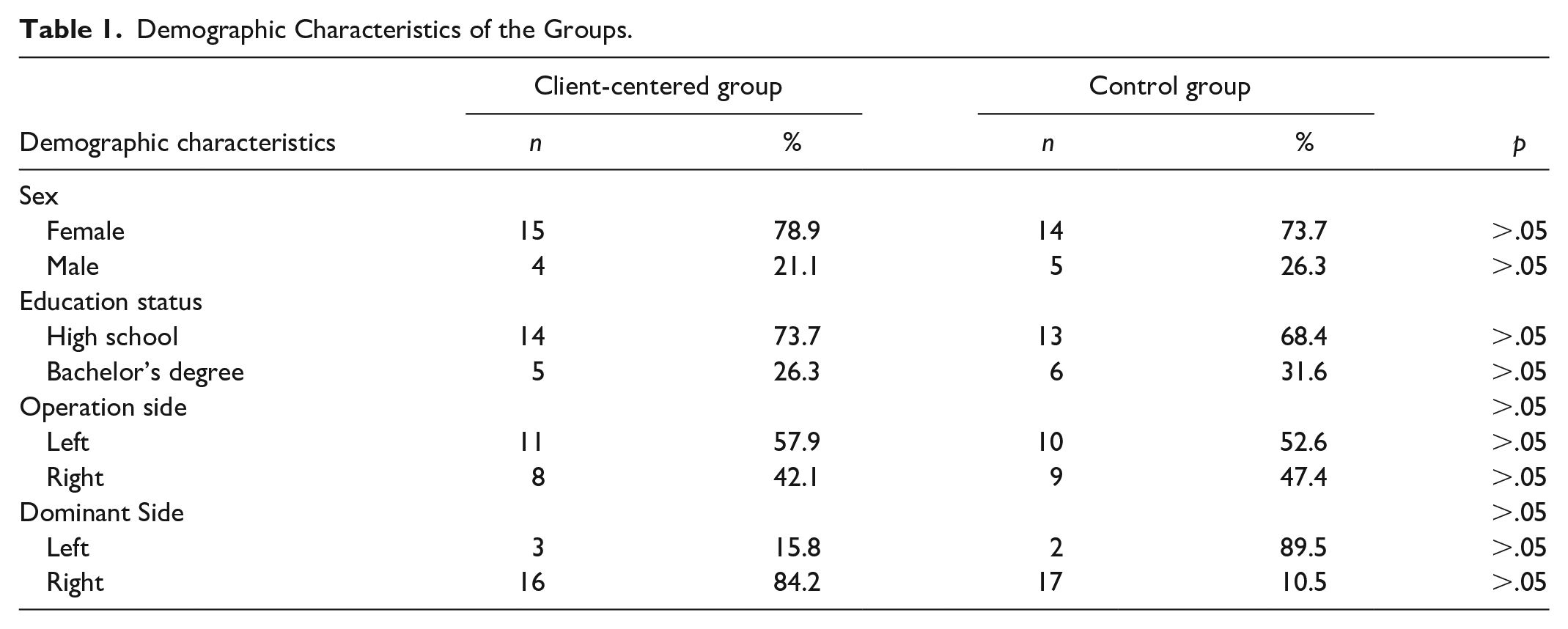
The mean age of the study participants was 55.10 ± 5.95 years (range, 44–64 years) in the CC group (n = 19) and 55.31 ± 5.45 years (range, 46–64 years) in the control group (n = 19) (p > .05). The mean BMI of the study participants was 30.62 ± 2.12 kg/m2 (range, 27.46–35.35) in the CC group (n = 19) and 30.60 ± 1.48 kg/m2 (range, 28.98–33.59) in the control group (n = 19) (p > .05). In both the groups, three participants smoked, and cigarette consumption was one pack per week on average. None of the participants drank alcohol. All of the participants were married and lived with their families. The other demographic characteristics of the study groups are shown in Table 1. There were no significant differences between the groups in terms of all the demographic parameters (p > .05; Table 1).
Demographic Characteristics of the Groups.
Before the intervention, no significant difference was determined between the groups in respect of all the parameters of the COPM scores and the NHP scores (p > .05; Table 2).
Comparisons of Preintervention Scores Between the Groups.
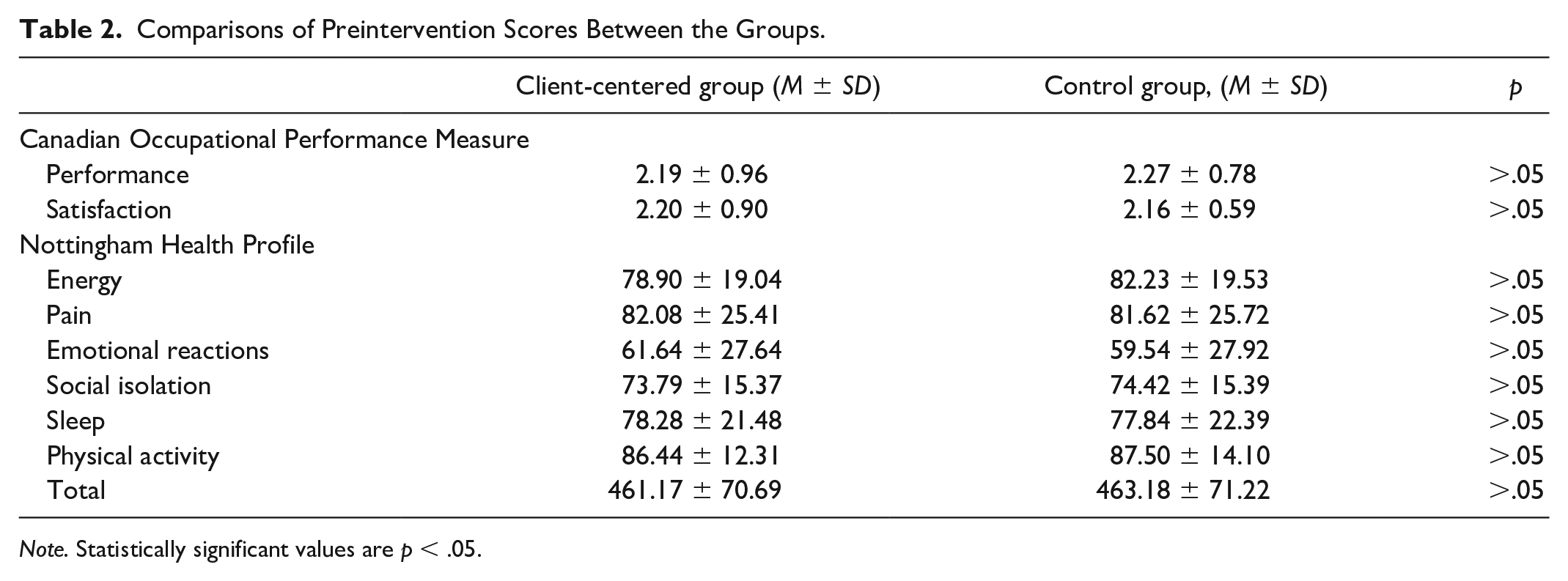
Note. Statistically significant values are p < .05.
In the comparisons of the groups, strong effect sizes were seen in all parameters in the CC group (p < .001). In the control group pre–post comparisons of energy, pain, and sleep parameters, the total scores of NHP had a medium effect size, and the physical activity parameter of NHP had a strong effect size (p < .05). In the control group, there was no significant difference within the group in the performance and satisfaction scores of the COPM and the emotional reaction and social isolation scores of the NHP (p < .05). The comparisons of the changes over time for all parameters of the COPM scores and the NHP scores within and between the groups, and the effect sizes, are shown in Table 3.
Comparisons of Baseline and Final Assessment Scores of the Canadian Occupational Performance Measure and Nottingham Health Profile Within and Between the Study Groups.
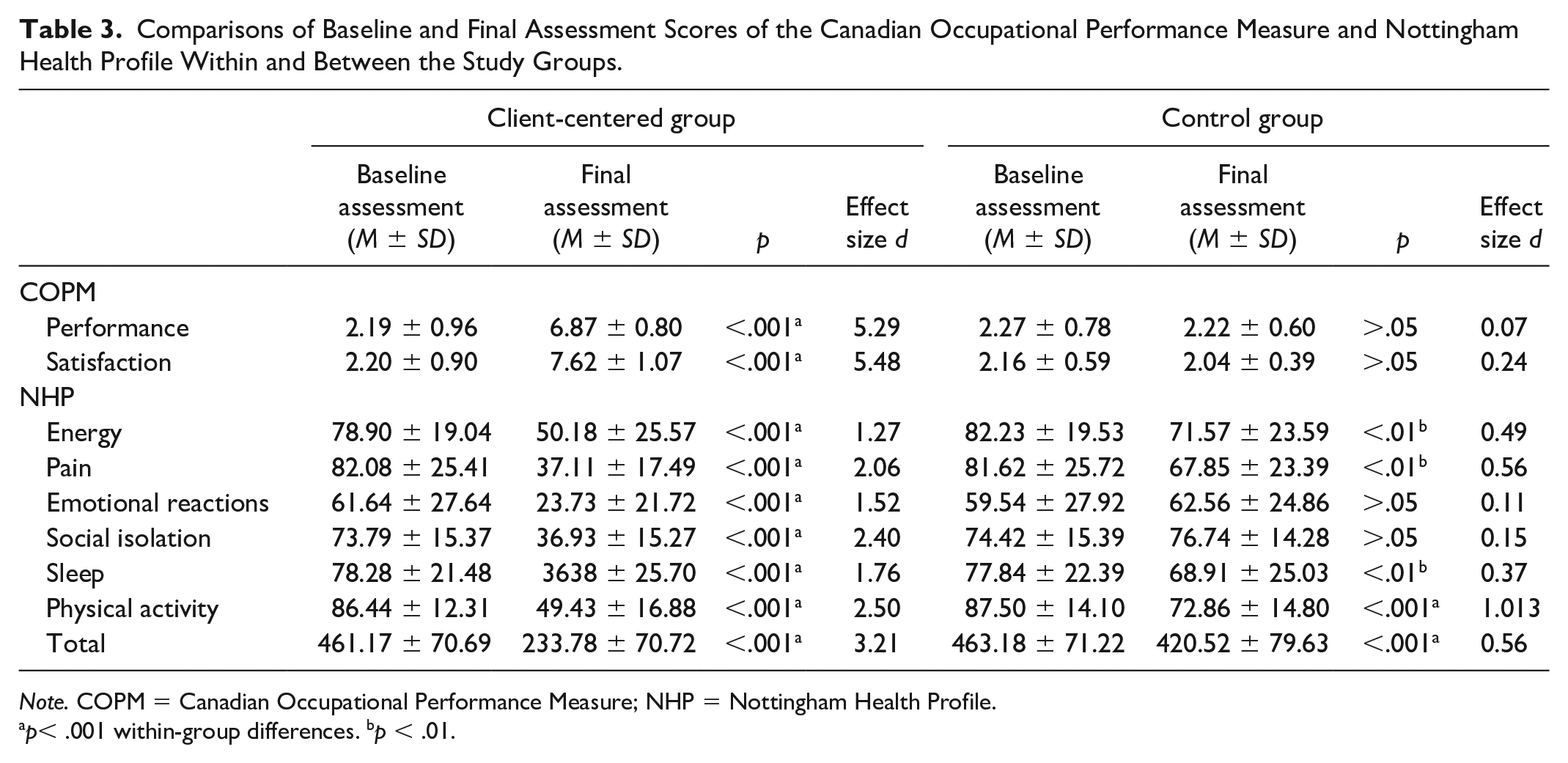
Note. COPM = Canadian Occupational Performance Measure; NHP = Nottingham Health Profile.
p< .001 within-group differences. bp < .01.
After the intervention, a significant difference was determined between the study groups in all parameters of the COPM and the NHP scores (p <.001; Table 4).
Comparisons of Postintervention Scores Between the Groups.
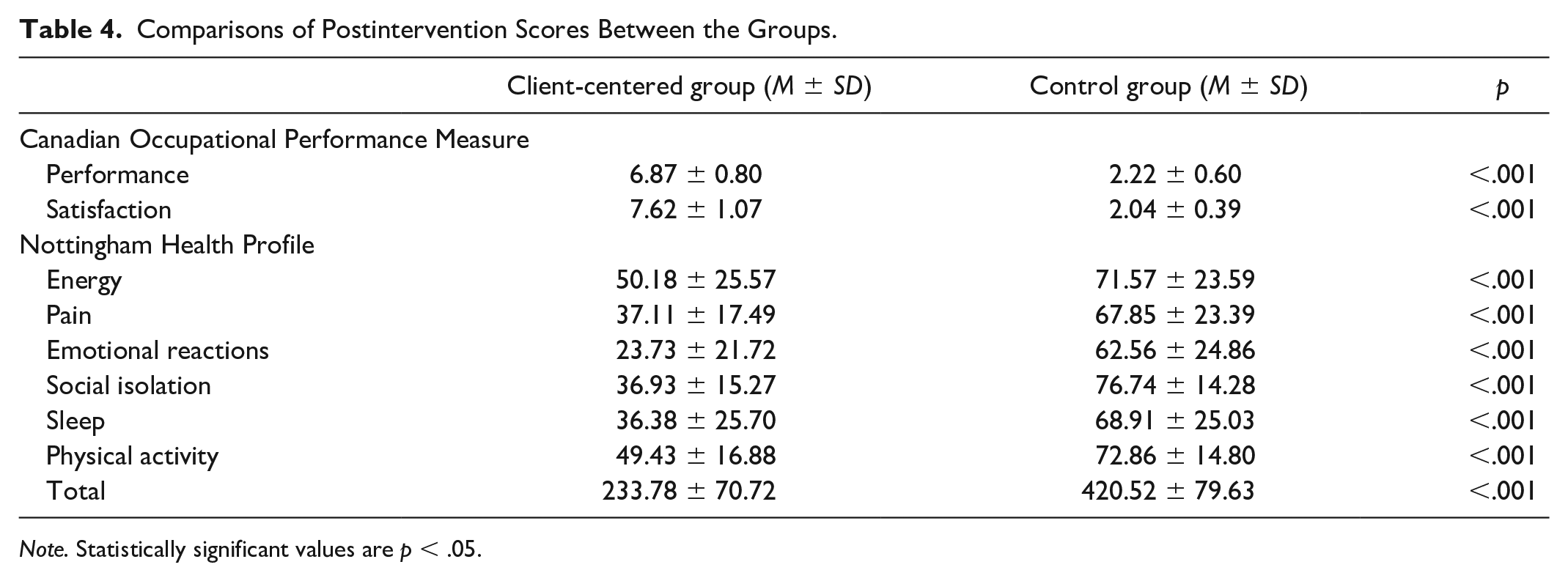
Note. Statistically significant values are p < .05.
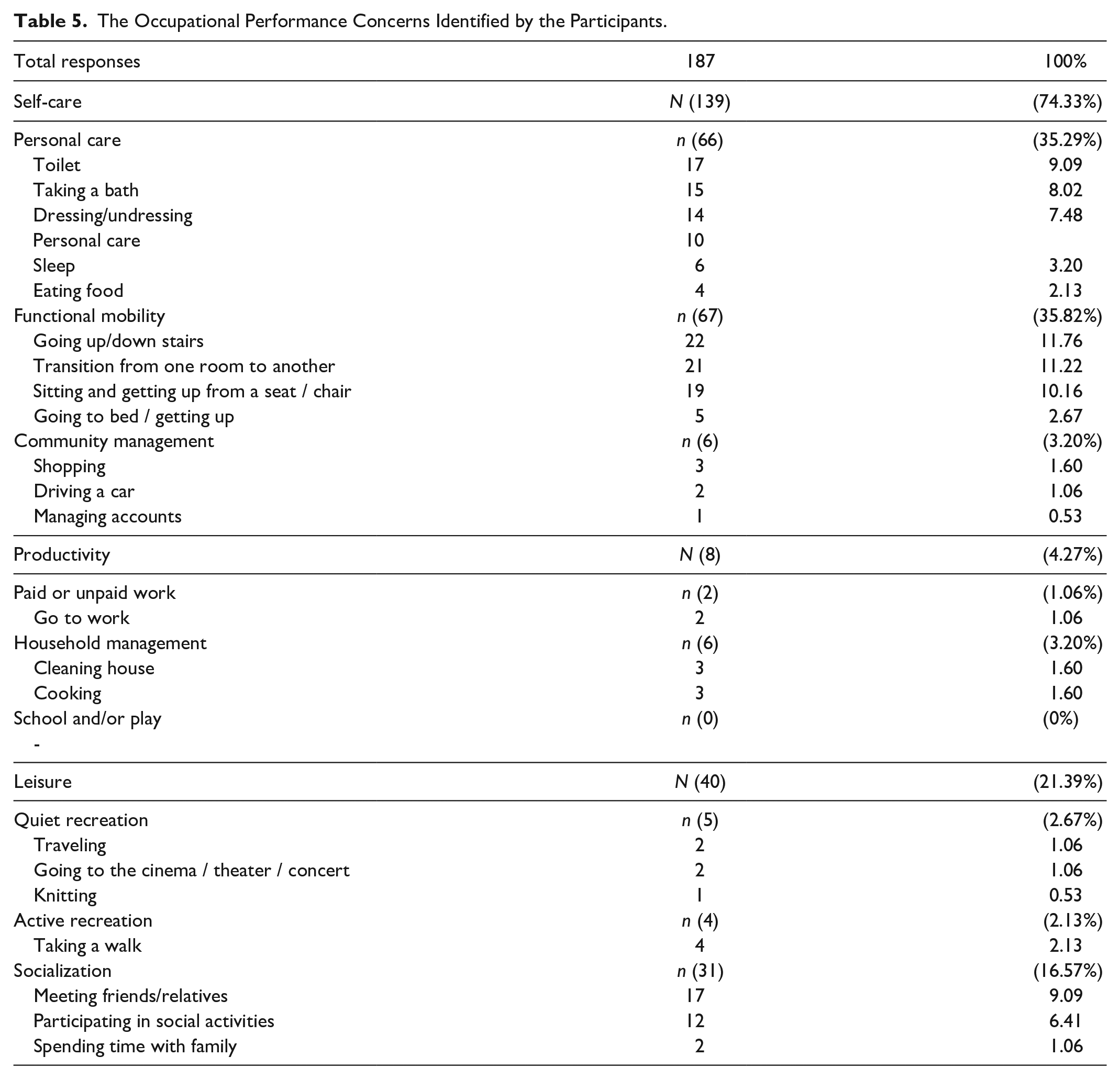
Of the occupational problem areas of greatest concern identified by the participants, the most common were going up and down stairs (n = 22) among the self-care occupations, and transition from one room to another (n = 21) and sitting and getting up from a chair (n = 19) among the self-care occupations. In the leisure category, the most common problem areas were meeting friends/relatives (n=17) from the socialization area. The occupational performance concerns identified by the patients are shown in Table 5.
The Occupational Performance Concerns Identified by the Participants.
Discussion
The current study examined the effectiveness of the OT intervention applied with the 12-day TR method on the quality of life, perceived occupational performance, and satisfaction of adults who had undergone TKA. The results of the study demonstrated that the tested program in the CC group demonstrated positive effects on the quality of life, perceived occupational performance, and satisfaction of adults following TKA. When the control group was examined, no significant improvement was found in emotional reaction, social isolation, or perceived occupational performance, although positive improvements were observed in energy use, pain reduction, and sleep and physical activity.
A previous randomized controlled study of TKA emphasized the importance of occupational therapy in ADL training as part of a multidisciplinary treatment approach (Nunez et al., 2006). Occupational therapy interventions have been reported to cause a decrease in pain intensity and disability and an increase in general physical and mental health, self-efficacy, and quality of life (Ackerman et al., 2012; Nunez et al., 2006). In another RCT, it was determined that in addition to standard preoperative clinical visits, individually tailored preoperative training that focuses on self-care, adaptive equipment, and home modifications resulted in a shorter hospital stay for TKA patients (Crowe & Henderson, 2003). In addition, it has been determined that an activity diary program created following the COPM at 1 to 2 weeks postoperatively increased perceived occupational performance and satisfaction level of TKA patients, findings shown to reduce pain and increase physical activity and psychological factors (Hiraga et al., 2019). In the current study, it was determined that the CC intervention applied in the early postoperative period increased the quality of life, perceived occupational performance, and satisfaction level in adults following TKA. It can be considered that CC interventions applied in the acute period will accelerate the adaptation to ADL following TKA and will positively affect the quality of life of patients due to adaptation to ADL. This study can also be considered important in respect of demonstrating the importance of applying occupational therapy interventions in early postoperative approaches to TKA. When the control group was examined, there were seen to be negative developments in perceived occupational performance and satisfaction levels, and in the emotional aspects in quality of life. This can be interpreted as difficulty adapting to ADL due to acute problems postoperatively and the inability to provide solutions for the problems experienced in ADL, as well as the presence of acute problems (such as the presence of stitches, wounds, and pain) and factors that cause social isolation such as the COVID-19 pandemic. When the other parameters examined in the control group were seen, which may be due to improvements in energy, pain, sleep and physical health. The reason for these findings was thought to be the increase in functionality as the operation site healed.
The use of TR was shown to have positive therapeutic effects (Hung & Fong, 2019). The authors suggested that TR offers an alternative service delivery model, and by Hung and Fong, studies with large samples should be developed (Hung & Fong, 2019). It was also emphasized that the TR method is important in terms of cost, time, and accessibility (Hung & Fong, 2019). The problems of accessing rehabilitation services that arose with the implementation of restrictions in the COVID-19 pandemic can be overcome with TR application (Negrini et al., 2020). In a systematic review of intervention approaches applied with the TR method for orthopedics, it was concluded that TR can be used for orthopedic consultations and rehabilitation (Petersen et al., 2021). In addition, it was stated in that review that there is a need for further RCT studies, and the effectiveness of various rehabilitation practices should be examined (Petersen et al., 2021). The results of the current study demonstrated that TKA patients treated with the TR method from the postoperative third day had increased quality of life and perceived occupational performance and satisfaction. This study can be considered to make a significant contribution to the literature in respect of the application of the CC intervention with the TR method in the acute period after TKA. The results of this study will be important in terms of generating solutions to cost, time, and accessibility problems in rehabilitation. One of the starting points of this study was the implementation of restrictions to prevent infection during the COVID-19 pandemic, thereby restricting access to rehabilitation services and creating a need for alternative rehabilitation methods. The intervention procedure determined with this study demonstrates the applicability of TR in the acute postoperative period of TKA and contributes to overcoming the problems of access to services during the pandemic.
It has been stated that patients have problems in various occupations of ADL after TKA (Dorsey & Bradshaw, 2017). These problems have been shown to significantly affect mobilization skills due to factors such as pain, joint limitation, and sleep problems, and this situation negatively affects the occupations in ADL (Dorsey & Bradshaw, 2017). Furthermore, TKA patients have also been reported to have psychosocial problems such as depression in ADL (Dorsey & Bradshaw, 2017). A previous cohort study found that after TKA, patients had problems going up and downstairs, walking, and sitting and rising from a chair, and that these problems can continue in the long term (Singh & Lewallen, 2014). In the current study, when the problematic occupations were examined in terms of occupational performance, there were problems in areas that require mobility skills such as going up and downstairs, going from one room to another, sitting and rising from a chair, and meeting toilet and bathroom needs. The patients mostly experienced problems in functional mobility, which can be considered to be typical pain and joint limitation, as previously stated in the literature. Additional problems reported were meeting friends/relatives and participating in social occupations in areas related to socialization in leisure time. Pain, sleep problems, and mobilization deficits may be the cause of this condition. However, the COVID-19 pandemic measures may have caused negative effects. The results of this study demonstrated that the 12-session intervention program applied via the TR method can be a solution for the problems experienced in postoperative TKA, will increase the quality of life, and positively affect perceived occupational performance and satisfaction level. When the control group was examined, there was no improvement in emotional skills, social isolation, perceived occupational performance, and satisfaction with a perhaps coming inability to gain the expected functionality or psychosocial issues created by the preventive measures during the COVID-19 pandemic. Despite the barriers, improvements were found in quality of life, energy, pain, sleep, and physical activity in the control group. This may be due to the increase in functionality with greater awareness of the two-session home modifications and transfer training.
This study had some limitations. First, the work could not be sustained effectively due to Internet infrastructure problems. Second, it could be difficult for patients to adapt to the TR method. The third limitation was that the therapist could not make any physical intervention, and only verbal guidance for the patient to perform the tasks could cause problems in the effective continuation of the treatment. Another limitation was that the long-term effects of the study were not known.
There is a need to further study the long-term effects of CC interventions with the TR method and to comprehensively evaluate the effects of parameters such as pain, sleep, and emotional state on ADL occupations in TKA patients. Further studies should also investigate immediate outcomes that include readmission to hospitals, falls, medication compliance, and cost-effectiveness of TR and also be conducted to determine the effectiveness of OT in meeting the more immediate client and organizational needs.
Conclusion
The current study is important in demonstrating the importance of occupational therapy in the acute period after TKA via the TR method. In addition, this study shows the importance in terms of early adaptation of individuals to ADL after TKA to increase their quality of life. On the contrary, this study sheds light on problems of time, cost, and accessibility (situations that make rehabilitation difficult such as COVID-19 pandemic) in TKA rehabilitation with the TR method.
The results of this study have numerous implications for both researchers and clinicians. First, occupational therapists should work in lower extremity musculoskeletal disorders rehabilitation practices when necessary, such as after acute TKA. Second, occupational therapy intervention approaches for lower extremity musculoskeletal disorders can be applied via the TR method. Third, the more active role of occupational therapists in rehabilitation for lower extremity musculoskeletal disorders is important for providing clients’ occupational performance and quality of life.
Footnotes
Acknowledgements
The authors are grateful to Serkan Pekçetin (PhD) for evaluating the patients in the study.
Author Contribution
All authors contributed to the methodology, analysis, and writing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical Approval was obtained from Lokman Hekim University (Ref: Go 2021/2).