
Abstract
The neonatal intensive care unit (NICU) is a dynamic system with multiple stakeholders and contextual factors impacting the implementation of novel practices. This qualitative study aimed to (a) define health care professionals’ perceptions on the feasibility of implementing a sensory intervention to study its efficacy, and (b) elaborate on transactions occurring between NICU health care professionals and the proposed research. Eleven NICU professionals participated in one of three focus groups that were audio-recorded, transcribed, and analyzed thematically in NVivo first descriptively and then interpretively through a transactionalism lens. The health care professionals implied the intervention was feasible, but provided multiple suggestions to enhance implementation. The modification of familiar occupational practices, ingrained habits, and the potential impact on the collective occupational performance of NICU community members arose. Understanding occupations within the NICU as transactional allows for a broader view of occupational engagement and enhances knowledge of the nuances related to implementing clinical changes.
Keywords
Introduction
As an advanced area of practice, occupational therapy in the neonatal intensive care unit (NICU) necessitates excellent clinical knowledge about the complex interplay of the NICU environment and the infants’ developmental process as well as medical and social factors that require dynamic assessment and interventions (American Occupational Therapy Association [AOTA], 2018). Occupational therapists in the NICU focus on individualized treatment of infant and family factors to enhance outcomes (AOTA, 2018). However, for interventions to benefit those they are intended for, they must be feasible within the NICU context. Feasibility considers intricate factors (such as acceptability to stakeholders, practicality, and suggested adaptations) that can impact successful implementation (Bowen et al., 2009). Furthermore, the setting, habits, routines, and occupations of health care professionals may impact feasibility (AOTA, 2018).
Recent advances in NICU clinical research have focused on understanding the effect of the NICU environment and the development of interventions to optimize infant outcomes (Pineda et al., 2020). This research group developed an innovative sensory-based guideline, the Supporting and Enhancing NICU Sensory Experiences (SENSE) program. It consists of parent-led sensory interventions with age-appropriate dosages and timing of sensory exposures for preterm infants in the NICU (Pineda et al., 2020). It was systematically developed by integrating existing evidence, obtaining stakeholder feedback, and conducting clinical feasibility studies. The health care professionals’ perspectives (reported here) formed part of the program development process and were integrated into the SENSE program prior to testing its feasibility and efficacy.
When developing clinical innovations, such as the SENSE program, researchers often gather stakeholder input to determine perceptions about feasibility and to identify potential barriers to implementation (Hogan & Logan, 2004). This is important, as the NICU is a complex adaptive system with multiple stakeholders (nurses, therapists, physicians, parents, etc.) working through collective occupations toward a common goal of optimal infant and family outcomes. Lavalley (2017) asserts that “the communication, meaning-making, and systemic co-existence of humans acting in association with one another form living communities” (p. 462). Per this transactional stance, a NICU can be conceptualized as a functional community. As with different communities that have shared space, values, customs, and cultures, different NICUs have their own cultures (Ohlinger et al., 2003). The training and clinical approach of different NICU professionals may vary, and conducting clinical research adds another layer of complexity within the dynamic landscape of multidisciplinary work under overarching organizational and political systems (Braithwaite et al., 2018). The roles, values, beliefs, experiences, strengths, and resources of NICU staff should therefore be factored into the implementation of interventions (AOTA, 2018).
By understanding the NICU setting as a complex system, researchers may anticipate barriers and facilitators to the implementation and research of innovative practices (Braithwaite et al., 2018; Ohlinger et al., 2003). Transactionalism posits that occupation facilitates coordination of intertwined person- and contextual-transactions and shapes and is shaped by the interaction (Dickie et al., 2006). Furthermore, framing occupations as collective allows for analysis of participation within complex systems (Dickie et al., 2006; Lavalley, 2017). Therefore, NICU occupations are co-constructive to the adaptive system, influenced by the collective role players and the context, and this view allows for a broader consideration of the systemic effect that novel practices may have.
Lavalley (2017) calls occupational scientists to “identify moments when traditions, policies, environments, and relationships change among people and their situations” (p. 463). When suggesting engagement in novel practices, such as the SENSE program, researchers introduce a new set of task demands into a dynamic environment, which could change traditions of care and the relationships between people and their context. Traditionally, the research outcome is narrowly defined with tangible outcome measures, yet the effect that research may have on the functioning of the system that supports it is often neglected. In defining occupation as situated at the contextual level of which an individual is a part (Dickie et al., 2006), researchers may consider the broader effects of suggesting new practices (changes in current occupations) within a NICU community. Asking health care professionals to deviate from existing practices impacts their habits and routines, which could impact their occupational performance and satisfaction with their roles (Law et al., 1996). Therefore, it is imperative to understand if a proposed clinical or research intervention is practical, possible, and suitable to implement from the perspective of the health care professionals, to determine perceived feasibility.
This qualitative study aimed to (a) define health care professionals’ perceptions on the feasibility of implementing a sensory intervention to study its efficacy, and (b) elaborate on transactions occurring between NICU health care professionals and the proposed research.
Methods
Data Collection
This study was approved by the study site institutional review board. Participants were NICU health care professionals employed at the anticipated implementation site (a level IV NICU) and were recruited via email invitation to attend one of three focus groups (based on the participants’ availability). A multidisciplinary group with representation from neonatologists, nurses, and neonatal therapists was sought to elicit multiple perspectives from people with different roles and responsibilities. Other stakeholders impacted by NICU interventions include parents; however, parents were not invited to participate in these focus groups, as the intent of this study was to gather perspectives from health care professionals. Separate interviews were conducted to gather parental input on the SENSE program (Lisle et al., 2022). Focus groups for health care professionals were specifically selected above individual interviews, as focus groups are particularly helpful in the early stages of research (Smithson, 2000), and participants can dynamically co-construct ideas during an interactive discussion.
Three, 90-minute, focus groups were held in 2016 in a conference room near the NICU where the participants were employed. Focus groups were audio-recorded and were led by two researchers trained in probing techniques. The researchers were familiar with work in the NICU through more than 20 years of clinical experience in this setting. The groups started with a brief report on literature related to sensory-based interventions in the NICU (Pineda et al., 2017), a description of the proposed SENSE protocol, and an introduction to the proposed pilot research (which included enrolling 30 preterm infants born <32 weeks within the first week of life and providing them with the SENSE program each day of NICU hospitalization). The brief report was followed by a semi-structured group discussion using the following prompts:
Is the sensory-based intervention (SENSE program) feasible? (Feasibility was not formally defined but left open-ended to encourage participants to share any aspects that they regarded as important.) When individualized to the needs of the infant, will infants tolerate the intervention? (Tolerance was not defined, but in this context, it typically refers to infant stress or physiological changes in response to overwhelming stimuli). How will health care professionals support or impede the intervention plan? Will the use of volunteers/surrogates be feasible when parents are not present? (The researchers explained that volunteers/surrogates could include graduate occupational therapy students, family members of infants, or other volunteers who may conduct sensory interventions when parents were unable).
Are there reasons why sensory experiences (defined in the program) might not be used?
What are some unknowns that will affect the ability to implement sensory-based interventions and test the program’s efficacy?
Data Analysis
Transcripts of the audio-recorded focus groups were uploaded to NVivo v.12 software for analysis. First, a descriptive analysis was conducted to understand feedback related to the discussion prompts. Second, the data were re-analyzed interpretively using transactionalism as a frame of reference. Two independent coders (familiar with NICU practice and guided by the principal investigator with substantial NICU experience) developed the codebook and conducted the descriptive analysis. The coders employed a case-oriented strategy to independently code each transcript by engaging in open coding where each line of text was read and assigned to corresponding themes (nodes) (Siccama & Penna, 2008). To enhance rigor and trustworthiness, the coders compared their nodes and resolved discrepancies through discussion. Following the coding process, the first author analyzed NVivo text and matrix queries to review the content and logically connect overlapping themes (Siccama & Penna, 2008). Multiple themes could be assigned to quotes, as many of them had multiple meanings. After the initial descriptive analysis, the interpretive analysis was undertaken (using transactionalism as a frame of reference), as multiple codes highlighted the transactional nature of interactions that occur between stakeholders and the proposed research with a specific focus on interpersonal interactions and interactions between people and their occupations. An audit trail documenting the coding decisions and interpretive analysis was maintained.
Results
Eleven health care professionals (4 neonatologists, 4 neonatal nurses, 1 occupational therapist, 1 physical therapist, and 1 neonatal nurse practitioner) participated in one of three focus groups.
Descriptive Analysis
The descriptive analysis centered around the practical aspects related to the implementation of the proposed sensory-based intervention. Table 1 lists the themes, the number of references per theme, and a representative quote. Below we organize quotes related to the discussion guide.
Themes From the Descriptive Analysis.
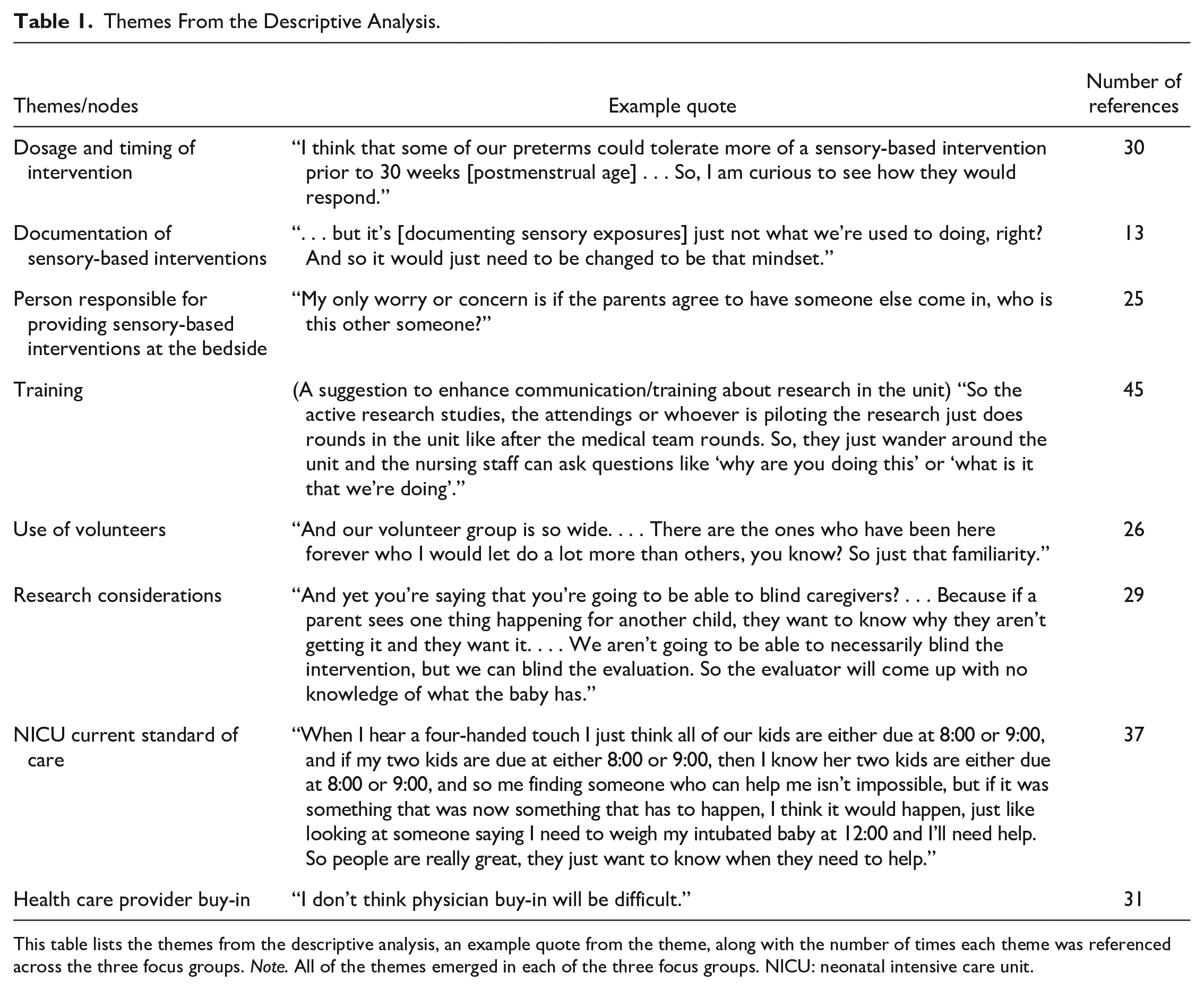
This table lists the themes from the descriptive analysis, an example quote from the theme, along with the number of times each theme was referenced across the three focus groups. Note. All of the themes emerged in each of the three focus groups. NICU: neonatal intensive care unit.
Feasibility
The health care professionals implied the sensory-based guideline would be feasible to implement and would be accepted.
. . . we’ve spoken to the experts. I think most of us would feel supportive of it.
Infant tolerance
Individualizing the intervention based on medical acuity and postmenstrual age of infants seemed important to positive perceptions about infant tolerance and the use of the interventions listed in the SENSE program.
A big part of that is making sure that each baby is individualized, that you’re looking at parameters to tell you they are tolerating it, and they are benefitting from it at this time.
Health care professional support
To enhance health care professional support for the program, participants suggested having specific protocols to guide parent and staff participation.
So will the parents have these guidelines as well as like the medical staff, to have something to go by each day? Like this is a 23 weeker, so today we need to do this.
Further suggestions to promote effective health care professional engagement highlighted the need for staff training through short workshops, checklists, and documentation reminders.
Scheduling and a concise, “this is what we want to happen” is going to make it the best for nursing.
To confirm that the sensory-based intervention listed in the protocol was acceptable and would be implemented, the health care professionals asked about the evidence supporting the intervention and asked to review the intervention materials prior to implementation.
But the frequency (of the sensory interventions) was designed based on studies? Do you feel like once you create your protocol for each gestational age (it would be okay) for us to just look at it and give feedback?
Volunteers
In response to the prompt on volunteer use, health care professionals raised the potential challenge of inconsistent parental presence and affirmed the need for volunteers.
I’m kind of stuck on the parental involvement. I don’t find that we have families who are consistent with care.
Additional results related to this construct of volunteers and parental engagement in the NICU are discussed in the following sections.
Interpretive Analysis
Interpretive analysis using transactionalism as a frame of reference resulted in two themes: NICU community and familiar NICU occupations. This incorporated the discussions on volunteer use (prompt 1 c) and elaborated on additional challenges related to implementation and the proposed study to determine SENSE efficacy (prompt 3).
NICU community
On interpretive analysis, a strong connection to the concept of community was identified. In addition to the physical layout of the NICU environment (termed “neighborhoods,” “pods,” or “gardens” by participants), sociocultural aspects around community membership and responsibilities emerged. While discussing the feasibility and buy-in to the SENSE program, accountability for implementation and the interconnected roles of different people in the NICU were discussed (training of parents, volunteers, and health care professionals). Challenges related to training health care professionals who were not permanently stationed in specific sections of the NICU arose.
. . . because we are so busy and our staff is kind of situated funny, we have a lot of travelers, we have a lot of flex team, we have a lot of people that consistently work outside their pod or garden. . . . I think you will still have days where even if you educated everyone in that area, other people (who have not been trained on the proposed intervention) are going to consistently be in there.
The NICU community had specific personnel who identified designated roles to safeguard infants with the ability to disallow access if they were uncomfortable with procedures.
The nurses are the gatekeepers. They allow access to the child . . .
The role and responsibilities of parents were described. They were viewed as part/not part of the community, based on their presence in the NICU and participation in care. Parents who were able to be present more often were viewed more favorably.
The families who are there consistently all the time . . . are so rare, but those are like the perfect people . . . because they could do all those interventions themselves.
The health care professionals listed some parental challenges such as transportation, living far from the hospital, and having other children at home as reasons for lower parental presence.
How their lives are . . . Can (they) get out of the house on time and be here when they need to be, and do they have reliable transportation, do they have to worry about care for their other kids?
The health care professionals suggested collaborative efforts between themselves and parents to provide positive sensory interventions to infants.
Something that could be a nurse, therapy, and parent intervention coming together, it could work a lot better.
Assigning specific roles to parents and enhancing their understanding of concrete tasks to engage in during their time in the NICU was recommended to boost participation. Having a specified role in the community could enhance parental engagement. This was seen as a potential program benefit If you give parents a job, they have more motivation to show up.
The health care professionals mentioned that parents “loved” knowing what to do with their infants, identified how parents could do the interventions in the NICU, and felt that parents would support SENSE implementation.
. . . we show [parents] you can give them [infants] containment, the parents love that, because it’s something that they know they are allowed to do that’s safe for their baby. So, it would be received well.
The sensory support team was introduced as trained volunteers/surrogates who would augment sensory interventions with the infants if parents were unable to complete the suggested daily dosages of sensory exposures. This feature of the SENSE program was directly connected to the descriptive analysis, but on interpretive analysis it took on additional meaning when considered in tandem with aspects of this NICU community’s experiences. The health care professionals had contrasting reactions related to volunteer training with some participants noting enthusiasm while others expressed hesitancy. The supportive statements illustrated the perceived feasibility of the proposed use of trained volunteers.
If they’re trained! If they know what they’re doing, then I won’t have a problem. We have the Cuddler Program that is getting started, and there’s a lot of interest.
However, the following statements indicated some uncertainty.
Volunteers come in and hold our babies all the time. I don’t know how I would feel about them transitioning them (from the bed) if they had any piece of a respiratory component or even IVs.
Some previous encounters with volunteers were described as chaotic, and poor communication about the volunteer role, their skill, competence, and training seemed to influence views about future NICU volunteer engagement.
We are doing a lot more of an educational rollout . . . so people will have . . . recognition that this person took the time to learn more, so hopefully, the bedside nurse will feel more comfortable with letting that person provide intervention.
The need for adequate training, familiarity, and understanding reasons for volunteering, as well as volunteers’ dedication to understanding and working cautiously in the NICU, seemed to trigger or minimize “gatekeeping” responses. Suggestions of limiting the number of volunteers to a familiar group of people, having volunteers wear special clothing/badges to promote visibility, setting guidelines for volunteer activities with medically stable infants, making staff aware of the level of volunteer training, and ensuring that the volunteers were health care students seemed to enhance the sense of comfort among health care professionals who would allow/disallow the volunteers in the unit.
Familiar NICU occupations
Familiar NICU occupations refer to challenges in merging the proposed changes to daily occupations inherent in the SENSE program with the current habits and routines and day-to-day practices of the health care professionals in the NICU community. The health care professionals raised several points about the proposed SENSE program as it related to current occupations, such as current sensory intervention-related practices, documentation, scheduling, and research in the NICU.
Engaging in research was a familiar occupation within the study site NICU and was spontaneously brought into the discussion by the participants. The health care professionals seemed open to research, yet asked numerous questions about the proposed study design, methodology, recruitment, blinding, and measures. The following quote illustrated concerns about treatment impacting the control group, and it also highlighted the health care professionals’ familiarity with the limitations of other intervention studies within this context.
You still get some spill-over. All the developmental interventions, that’s something they are criticized for, is the spill-over.
The health care professionals suggested that the researchers carefully consider which nurses (community members) to train and focus on certain sections of the NICU to avoid contamination. Established weekly research rounds were mentioned defined as opportunities for transactions between researchers and NICU staff. Past research experience, along with the current workload, may have influenced some perceptions about feasibility. The health care professionals stated that other interventions were not as time-intensive as the SENSE program and that the proposed research might be burdensome in comparison.
For nursing, because they are over-worked, and (current research intervention) is really quick, so this [SENSE program] is going to be more time-consuming.
The health care professionals desired formal scheduling and timeliness from parents. Conversely, flexibility in protocol implementation was requested to accommodate unpredictable workloads.
We love schedules . . . When moms call us and say ‘I can come in at 3:00 and I would love to hold’, awesome, we can plan and make that happen.
Finally, the health care professionals encouraged researchers to communicate expectations effectively. They pointed out that additional documentation in charts should be explicitly requested, as charting is a routine or habitual activity, which may require specific instruction and reminders to adapt practices to include sensory interventions.
. . . but it’s just not what we’re used to doing, right? So, it would just need to be changed to be that mindset.
Furthermore, compiling clear guidelines about intervention expectations was suggested.
Having a list of all the things you want accomplished, that’s going to be helpful. Even if it’s ‘do it when you can,’ but when you can, here’s what we want to happen.
The buy-in of health care professionals appeared to be engrained in suggestions that would enhance implementation. Physician buy-in was perceived to be high if the supportive evidence and the safety of the intervention could be emphasized during training. Buy-in from other staff was more complex and impacted by workload, health care professional responsibilities during implementation, ambiguity about whether parents would engage, and volunteer assistance.
It would be great if everyone was on board, I just know that with recent general unit education bits, everybody is just resistant to new things . . .
However, several health care professionals conceded that the proposed intervention was necessary to improve care and conveyed a high level of excitement about the program.
I think it’s super exciting, and it’s well-needed. I think it’s awesome.
Discussion
Thematic analysis of focus group discussions revealed that implementation of a novel sensory-based program for infants to test its efficacy in the NICU was largely perceived as feasible, but perceptions on implementation were impacted by multiple factors. The descriptive analysis highlighted the practical concerns (such as staff training and tailoring the intervention to individual infants), while interpretive analysis underscored deeper concerns around the NICU community, modification of clinical practices, and the potential impact on the collective occupational performance of the stakeholders. This provided important insights during the SENSE program development, which has now been finalized and studied (Pineda et al., 2021).
Although the discussion guide was formulated around the practical facilitators and barriers to implementation, the focus group elicited rich discussion that allowed for deeper analysis through a transactional lens to illustrate the interconnected nature of NICU occupations. The complexities around intervention implementation, which would require multifaceted transactions such as the coordination of staff, families, and volunteers within a highly complex setting, were apparent. When framing occupations as transactional and dependent on the complexities of the situation (Dickie et al., 2006), this outcome was not surprising. The multi-layered implementation challenges identified strengthen the notion that occupation is a collective endeavor affected by the norms, structures, situations, and other people within the context (Lavalley, 2017). Implementation strategies that recognize and address these complexities likely have a higher chance of success.
The health care professionals shared valuable information about their current occupations and their NICU’s culture. As occupational transactions occur over time, it is important to consider the impact of previous experiences, such as health care professionals’ historical engagement in other research studies. The health care professionals asked to review the optimized protocol, possibly as a technique to verify that their input was understood and implemented and to exercise a level of control over the proposed intervention, which would impact their daily routines. Having control over occupations adds to engagement and satisfaction among health care professionals (de Jonge et al., 2008). Also, the health care professionals contemplated whether the research would disrupt their habits and routines in the NICU before voicing their acceptance of it. Health care professionals also stressed the importance of individualizing the intervention and clustering care as is in line with current NICU best practices (Altimier & Phillips, 2013). As part of the transactions occurring in the focus group, and in negotiating the responses to the health care professionals’ questions, researchers had the opportunity to increase confidence in the intervention and to build trust for future collaboration. Establishing confidence and credibility is essential when implementing complex interventions into clinical settings (May et al., 2007). These transactions may be viewed as purposeful coordination, which enhances understanding of the proposed intervention and promotes meaning for the stakeholders (Dickie et al., 2006). Despite this potential positive outcome of the focus groups, it is noteworthy that our participants repeatedly engaged with the researchers during the discussion, and therefore, the influence of the group moderators on the evolving participant perspective is unclear (Smithson, 2000).
Practical concerns on novel intervention execution are important considerations for implementation (May et al., 2007). Within the current study, several practical concerns were raised. One highlighted the interconnected nature of the physical and social environment. Health care professionals mentioned that frequent NICU staff rotation through various physical areas of the NICU may result in team communication challenges and pointed out that this may affect research implementation. Frequent NICU staff rotation has previously been described as a challenge to effective communication and the forming of relationships between staff (Kraemer, 2006), thereby affecting everyday occupations. To enhance work efficiency, the health care professionals highlighted the need for good communication between team members and having well-defined research protocols. The need for clear scheduling of tasks, which is also in line with other daily NICU practices such as the clustering of infant care, was emphasized. The health care professionals’ high regard for checklists and schedules could be interpreted as part of the habitual structured practices within the NICU that aid job performance.
Dickie and colleagues (2006) highlight that the context within which transactions occur goes beyond just the physical environment to also include the social and cultural environments. Within our data, the sociocultural dimensions were more prevalent in the discussion than the physical environment. The sociocultural world of the NICU community and the interconnectedness of the members (health professionals) and others (parents, researchers, and volunteers) may have impacted the perceptions of the feasibility of SENSE.
Within the current study, health care professionals highlighted the importance of parents and their crucial role in the implementation of the proposed intervention. The health care professionals emphasized that parents may function in various arenas during their infant’s hospitalization, with multiple daily transactions influencing their engagement in the NICU. For example, participants discussed that parents may need to actively coordinate child care and transportation in addition to their expected engagement in the NICU. These factors are not only influenced by family-level preferences and routines, but also by the broader community and societal systems that regulate the availability of transportation, child care, and parental leave. It is therefore important to consider parental participation beyond just the individual level. Broader perspectives on the coordination of occupations related to parental participation in the implementation of the SENSE program were highlighted as areas of concern. It was noted that some parents could navigate these transactions and would be able to coordinate the additional demands that participation in a research study may introduce. On the individual level of occupation, health care professionals identified that many parents may need a role to encourage their active engagement in the NICU, and participating in the SENSE program could assist with this. Aiding parents in developing their parental role and confidence is important to decrease parental stress and enhance engagement in the NICU (Harris et al., 2018) and could be crucial to the successful implementation of the SENSE program.
Within this NICU community, volunteers were viewed as outsiders, yet were acknowledged as persons who could fill a need within the system. While many NICUs across the United States have implemented “Cuddler” programs, where volunteers engage in therapeutic touch with infants, there is a lack of standardized training and health care involvement in these programs (Milanaik et al., 2019). Before the proposed SENSE implementation, health care professionals expressed the importance of adequate volunteer training and ensuring NICU staff buy-in. This is consistent with other reports related to volunteers in the NICU (Insley et al., 2021). Furthermore, our findings related to concerns about the need for health care professionals to supervise engagement by volunteers is consistent with another article that identified that nurses acknowledge the benefits of a volunteer program but highlight the additional responsibility that they bear to assist the volunteers (Hignell et al., 2020). Through the introduction of volunteers into the NICU, the range of daily transactions occurring in the NICU would broaden. The health care professionals within our study seemed willing to accept this, contingent upon antecedent transactions between the researchers and volunteers during which training and vetting of volunteer capacities could occur. It is unclear how relational hierarchies between health care professionals and volunteers may further impact the implementation of interventions where volunteers have a predefined role, and additional attention could be directed at practical environmental aspects (such as workspace, dress code, etc.) prior to volunteer introduction into the NICU environment. Developing initial working relationships in this way may enhance trust between health care professionals and other stakeholders in the community.
Cohesive social communities are important for occupational engagement of health care professionals and can mitigate the stress associated with complex hospital work (Fiabane et al., 2013). Introducing new people (role players) into the NICU environment can impact the “person-place-whole” and could be regarded as potential “undetermined situations” in which creative avenues are sought to uphold occupational performance (Cutchin, 2007). As such, the introduction of new role players into the NICU should be carefully considered in terms of the emotional and practical toll. If staff are already experiencing high levels of burnout, the creative capacity to problem solve and uphold occupational performance may not be optimal (Fiabane et al., 2013), and the additional stressors brought about by changes in the person-place-whole could potentially have unintended consequences on the NICU community which may confound the research outcomes. Health care professional workload has been described in the literature and can lead to burnout (Fiabane et al., 2013). Appropriate timing of introduction of new role players may decrease staff workload, decrease burnout, and potentially strengthen the community. As defined by health care professionals in this study, opportunities for cohesive training, communication, and relationship-building can aid in the introduction of volunteers in the NICU.
The impact of changes to the sociocultural landscape of a NICU may be larger than the seemingly “small” changes to individual daily tasks or habits that the researchers suggested. Habits are organizing units within occupational transactions (Dickie et al., 2006). For example, the suggested changes to documentation and implementation of sensory experiences would require changes to existing habits. While imagining the future feasibility of the SENSE program, the health care professionals suggested numerous practical ways of coordinating action through clear communication of researcher expectations and encouraging shared habits related to scheduling and timeliness of parents and providers. Allowing for reframing or redistributing task demands across multiple role-players within the community as time and workload permits may aid in buy-in and enhance community cohesion. Ensuring the congruence of proposed practices within the current systems can enhance the implementation of complex interventions (May et al., 2007). Occupation is constantly influenced by norms, structures, situations, and other people (Lavalley, 2017). If the proposed change to practice is experienced as co-constructed and there is a perception of shared meaning and positive consequences, engaging in the process of change could be incorporated into future “habits of action,” leading to a willingness to engage in practice change endeavors (Lavalley, 2017). Yet, if the required change is seen as incongruent with current habits, routines, or skill level, or if the consequence of the action is undesirable in terms of the shared intention of the community, it may potentially disrupt occupational performance and challenge occupational engagement (Law et al., 1996). In this instance, the proposed change can be perceived as a threat to occupational performance. In the case of the NICU environment where optimal performance is required, it could lead to hesitancy in changing habits and care practices and slowing down the process of translational research for evidence-based practice. Shared habits developed by solving these types of practical challenges can enhance understanding among stakeholders and contribute to the meaning of the co-constructed occupations (Lavalley, 2017). Therefore, through engaging in a process where the feasibility of implementing change within communities is negotiated, an understanding of the shared goals of researchers and clinicians can be enhanced. Transactions could be viewed as purposeful re-organization of relations and habits to optimize outcomes for all involved (Cutchin, 2007).
Understanding the habits and routines nestled within daily transactions occurring during the occupations of health care workers and designing research protocols that complement and integrate seamlessly within these existing performance patterns are important considerations during the planning and implementation of clinical research. Therefore, researchers can benefit from investigating the community culture within a specific NICU, to garner a broader understanding of the intersubjective view of occupations performed by the role players before suggesting multifaceted changes to clinical practice. This study provided valuable information to the research team, including perceived feasibility and suggestions to overcome the identified barriers, to enable the successful implementation of the SENSE program.
This study had limitations including small sample size (11 participants) at a single site. The first author only had access to transcribed, aggregated copies of the data, limiting the ability to assign pseudonyms, untangle perspectives of individual participants from different disciplines, or discern the presence of dominant voices (Smithson, 2000). Hierarchy associated with different professions in the NICU along with the presence of seasoned NICU professionals as group moderators may have subconsciously influenced the discussion, and heterogeneity of participants within the focus groups may also be a limitation (Smithson, 2000). In addition, apart from the participants’ disciplines, no other characteristics were included in the analysis. Furthermore, triangulation was limited and member checking of the data could not be done, as the researchers were no longer actively engaged at the research site. Although field notes were not available, all quotes and descriptions were reviewed by a research team member who conducted the groups to ensure accuracy of reporting. The themes were organized from coded data and could be organized and/or collapsed in a multitude of different ways to establish meaning. Here we have chosen to report the descriptive analysis related to the discussion guide followed by interpretive themes related to transactionalism. Finally, discussion and questions that were immersed in the brief report were not well-captured on audio-recordings.
Conclusion
The NICU is a complex adaptive system. Health care professionals within this system indicated that although implementation of novel practices (such as the SENSE program) are perceived as feasible, underlying concerns around the co-constructed occupations within the sociocultural NICU environment and their ingrained habits and familiar practices may impact their perceptions. The SENSE program was perceived to be feasible to implement and study, and information gained from the health care professionals was incorporated into the program prior to its implementation. Understanding occupations within the NICU as transactional allows for a broader view of occupational engagement and enhances knowledge of the nuances inherent in implementing clinical changes in this setting.
Footnotes
Acknowledgements
The authors thank Dr. Mary Lawlor for her intellectual contribution to the development of this manuscript, Julia Lisle for her role as the second coder, and Sarah Tenbarge for organization of the data. We also thank Jessica Roussin, Polly Kellner, and Kylie Buma for their assistance with the project.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Two authors (R.P. and J.S.) are authors of the SENSE program. It is available “at cost” to clinicians and researchers, with no financial benefit to the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Washington University Research Strategic Alliance and the Gordon and Betty Moore Foundation.
Ethical Approval
This study was approved by the Washington University Human Research Protection Office IRB number: 201502093.