
Abstract
Women treated for breast cancer often experience decreases in executive functioning, including goal maintenance, which interferes with daily living. The objective of this study was to conduct a preliminary comparison of cognitive neuroscience assessment performance with neuropsychological, self-report, and performance-based assessments of goal maintenance in women with breast cancer. Women treated for breast cancer in the preceding 3 years completed a battery of cognitive assessments. Relationships between assessment methods were evaluated using Spearman rho correlations. Consistent with prior literature, the AY condition of the Dot Pattern Expectancy (DPX) assessment had the highest error rate. No consistent relationships between the DPX and other methods of assessment were identified; however, some moderate correlations were identified between assessments. Women treated for breast cancer present with DPX performance patterns similar to that of healthy controls in past literature. A larger study is required to confirm relationships between measures of goal maintenance across disciplines.
Keywords
Introduction
Although the cognitive impact of treatment for breast cancer is now widely acknowledged (de Ruiter et al., 2011; Janelsins et al., 2017; McDonald et al., 2012), the severity and duration of the cognitive effects are ill understood. These cognitive impairments, known as cancer-related cognitive impairment (CRCI), occur in up to 78% of women with breast cancer (Janelsins et al., 2011, 2014; Koppelmans et al., 2012; Myers, 2009; Wefel & Schagen, 2012). CRCI continues well after the end of treatment and has been documented as far as 20 years posttreatment (Janelsins et al., 2011, 2014; Koppelmans et al., 2012; Myers, 2009; Wefel & Schagen, 2012). CRCI impacts functional cognition as it limits the ability to return to work at a previous capacity and thus has detrimental financial consequences for the individual and the economy (Bradley et al., 2005; Wefel et al., 2004). In addition, CRCI has substantial effects on return to driving, productivity, quality of life, social participation, and community engagement (Reid-Arndt et al., 2009, 2010; Ronis et al., 2008; Schou et al., 2005; Tobias et al., 2010). Currently, the literature indicates there are several discipline-specific understandings regarding CRCI due to a lack of precise measurement and a lack of a transdisciplinary approach to assessment.
As treatment approaches for women with breast cancer are evolving from traditional chemotherapy agents toward adjuvant chemotherapy and molecularly targeted treatments, additional research is required to understand what cognitive functions are impacted by these agents, when they begin, and for how long they persist. The National Cancer Institute (NCI, 2018) acknowledges that current literature is limited by data from multiple, distinct fields related to CRCI with little to no consensus. Existing knowledge of CRCI is also limited by imprecise measurement tools and a lack of longitudinal data. A transdisciplinary approach to the short-term and long-term assessment of CRCI is necessary to inform clinical assessment procedures and care plans. To establish a strategic, transdisciplinary assessment plan, it is first necessary to understand the relationships among different methods of assessment employed by varying professions. To evaluate these relationships, a specific cognitive construct needs to be evaluated across disciplines; for persons with CRCI, goal maintenance deficits tend to be prevalent and often addressed by multiple disciplines (Barch et al., 2012; Boone & Wolf, 2021; Lenartowicz et al., 2021; Unsworth et al., 2012).
Goal maintenance is a component of working memory (Paxton et al., 2007) and a key element of CRCI (de Ruiter et al., 2011; McDonald et al., 2012) which is poorly understood. Humans rely on goal maintenance for productive everyday behavior (Baddeley & Hitch, 1974). Goal maintenance refers to the identification of task-related goals and rules and the holding of this information for a period of time so that it can be used to guide attention and selection of appropriate behaviors to accomplish the identified goal (Carter et al., 2008). It follows that goal maintenance is essential for instrumental activities of daily living and should be considered a component of functional cognition.
A wealth of neuroimaging literature has demonstrated associations between performance on goal maintenance tasks with decreased activation in cognitive control networks (Simó et al., 2013). The Dot Pattern Expectancy Task (DPX) was developed as a part of the Cognitive Neuroscience Treatment to Improve Cognition in Schizophrenia initiative. The DPX was developed using a cognitive neuroscience paradigm to develop a measure of goal maintenance that could be used to identify specific underlying neural mechanisms to improve the identification of impairments and measurement of treatment effects to link neural circuitry and behavior. Performance on the DPX has been evaluated in healthy individuals and individuals with schizophrenia, but it has not yet been used in individuals with CRCI. A recent call for a cognitive neuroscience approach to evaluating CRCI has been made due to a reported lack of precision in neuropsychological assessments that may not be sensitive enough to detect the subtle but clinically meaningful effects of CRCI (Horowitz et al., 2018). The use of more precise measurement tools with direct links to structural and functional neurologic changes could lay the foundation for elucidating the causal pathway of CRCI spanning neurophysiology to everyday life function.
Several disciplines evaluate goal maintenance from various perspectives. Cognitive neuroscientists, occupational therapists, speech therapists, and health psychologists measure goal maintenance using tools that are sometimes discipline-specific but often overlap between disciplines. Existing research suggests that neuropsychological measures have only weak relationships with self-report measures of CRCI (Debess et al., 2010; Ganz et al., 2013; Hermelink et al., 2010). This may be due to the measurement of different constructs or the measurement time periods as self-report measures cover long periods of time and neuropsychological measures assess a singular point in time. Self-report measures of perceived cognitive abilities, as opposed to negatively worded items that inquire about perceived impairment, may have stronger relationships with neuropsychological measures (Van Dyk et al., 2017; Von Ah & Tallman, 2015). Individuals with CRCI present with reduced white matter integrity, overall reduced gray and white matter volume, and hypoactivation in prefrontal and parietal cortices (Deprez et al., 2012; McDonald & Saykin, 2013). These neural changes may be compensatory in nature (Lange et al., 2019). It is essential to understand the relationships between these variables to increase our knowledge of CRCI assessment to inform treatment and outcome measurement selection.
Importantly, there are no studies that have bridged different methods of assessment of goal maintenance (cognitive neuroscience, neuropsychological, self-report, and performance-based) to establish relationships and provide a more comprehensive understanding of goal maintenance. Therefore, the research question for this exploratory study was the following:
Method
Research Design
This was a cross-sectional study with women who had completed treatment for breast cancer (n = 22). All participants completed 2.5 hr of cognitive testing: cognitive neuroscience, neuropsychological, self-report, and performance-based testing (PBT) over the course of two separate visits. The second visit was completed within 2 weeks of the first visit. This study was approved by the University of Missouri Institutional Review Board, and all participants provided written informed consent. All study procedures were performed in accordance with the revised Helsinki Declaration (“World Medical Association Declaration of Helsinki,” 2000).
Participants
A sample of women (n = 22) who had been diagnosed with and treated for breast cancer were recruited from the Ellis Fischel Cancer Center in Columbia, Missouri. Women were recruited who met the following inclusion criteria: (a) 18 years of age and older; (b) history of primary breast cancer diagnosis; (c) history of cancer treatment (3 years or less posttreatment); (d) Montreal Cognitive Assessment (MoCA) score ≥ 23; (e) normal estimated intelligence indicated by a Wechsler Test of Adult Reading score ≥ 85; (f) able to read, write, and speak English fluently; (g) knowledge of how to use a check register as self-reported on the participant information questionnaire; and (h) community-dwelling.
Participants were excluded if any of the following criteria were present: (a) colorblind per self-report; (b) severe depressive symptoms as indicated on the Patient Health Questionnaire (PHQ-9 score > 19); (c) any thoughts of harming themselves or others as indicated on the PHQ-9; and (d) history of neurological or severe mental health condition.
Study Procedures
Women were recruited who had been treated for breast cancer within the previous 3 years at the ————– Cancer Center. Potential participants were asked to complete a prescreening survey. Those meeting initial eligibility criteria were asked to come into a University of Missouri research laboratory to complete additional screening measures. Those meeting inclusion criteria began a battery of cognitive assessments at the same visit. To minimize the participant burden, a second visit was scheduled at a later date to complete the assessment battery (see Table 1).
Assessments.
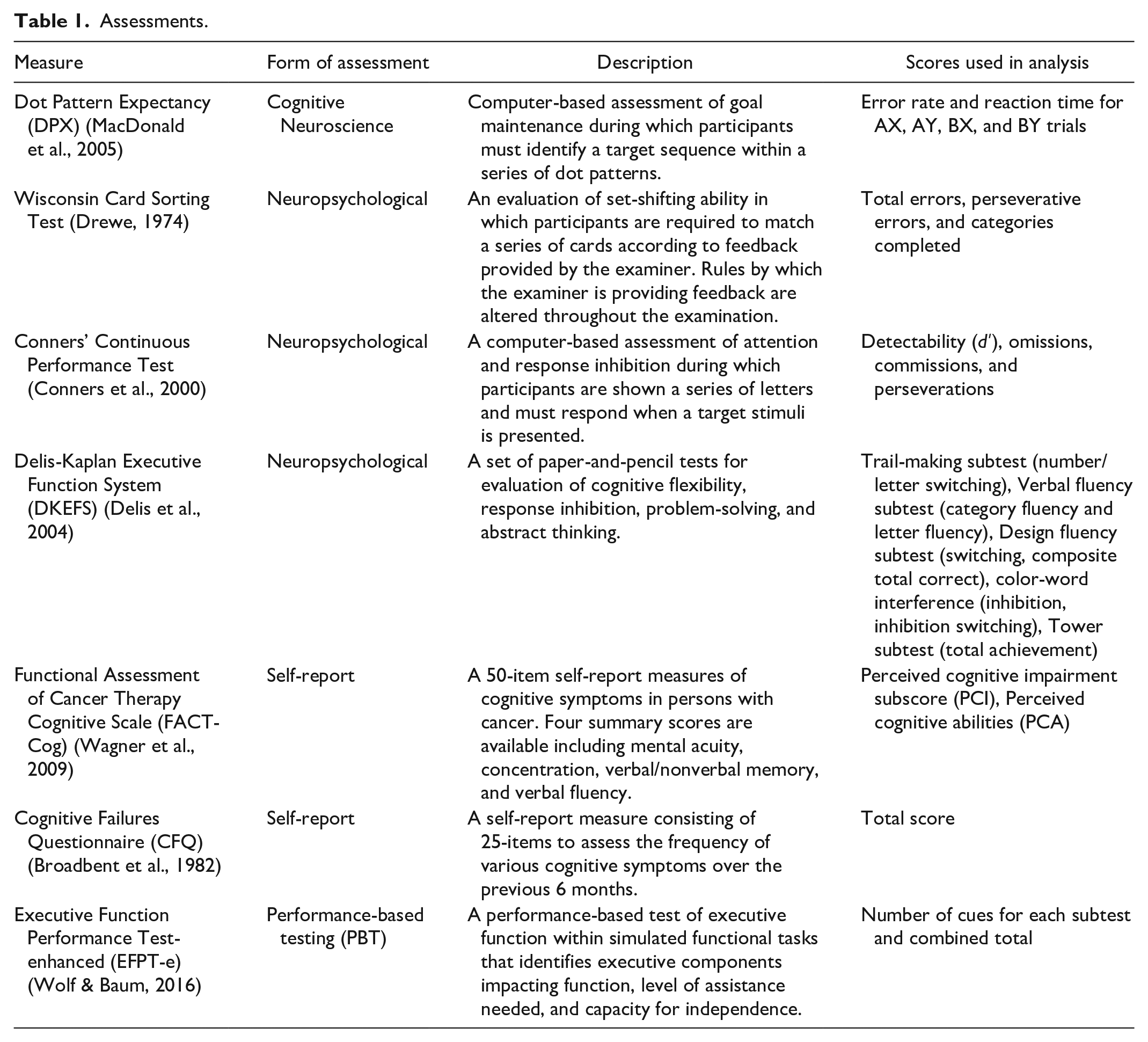
DPX
The DPX uses a series of visual dot patterns presented one at a time that are alternating cues and probes resulting in one of four types of trials: AX, AY, BX, BY (Barch et al., 2009; Henderson et al., 2012). The target response occurs when the A cue is followed by the X probe; all other trials are nontarget responses. The highest proportion of trials is AX (i.e., target response) leading to an expectation that an A cue will be followed by an X probe. Because of this expectation, AY trials tend to be the most difficult with more errors and longer response time due to the increased time needed to inhibit the prepotent response. In contrast, those with very poor goal maintenance abilities will make more errors on the BX condition as they are less able to use the accurate A cue as a signal that a target response may be coming. Each participant completed a practice block of 18 trials with 80% accuracy required prior to continuing on to testing trials. The DPX consisted of 4 blocks of 36 trials with 72% AX, 11% AY, 11%BX, and 8% BY. The interstimulus interval (i.e., time between cue offset and probe onset) was approximately 2,000 ms.
Data Analysis
All behavioral assessment data were first cleaned and checked for accuracy. IBM SPSS Statistics (Version 28; IBM Corp., Armonk, NY, USA) was used for all analyses. Descriptive statistics were calculated for all demographic variables and for the performance of the sample on each clinical assessment. Data were then checked for a normal distribution using the Shapiro–Wilks test. The majority of variables did not conform to a normal distribution; therefore, nonparametric statistics were used. To examine relationships between performance on cognitive neuroscience assessment (e.g., DPX) and each of the other methods of assessment, Spearman’s rho correlations with a Bonferroni correction (α = .0003) were calculated.
Results
Participant Demographics
Descriptive data for participant demographics and performance on clinical tests are located in Table 2. Overall, the sample consisted of middle age (M = 53.6 years), White, with a moderate level of education (M = 14.7 years). The majority of the sample received chemotherapy treatment and underwent radiation. As a whole, the sample presented with mild depressive symptoms and scored within the cognitively intact range on the MoCA, although the mean is on the border of mild cognitive impairment. No correlations among measures were significant following the use of the Bonferroni correction.
Sample Demographics (n = 19) and Performance on Clinical Assessments.
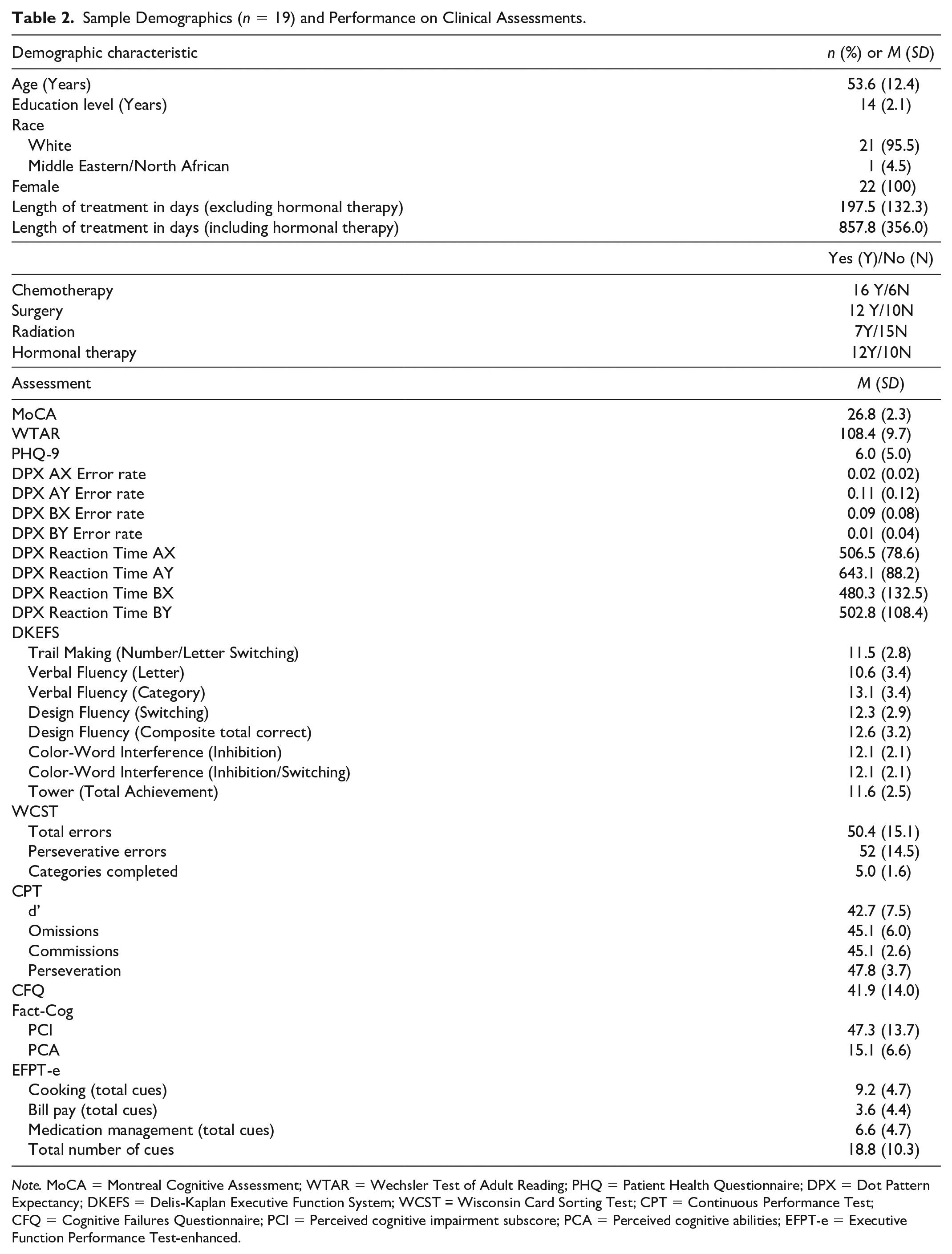
Note. MoCA = Montreal Cognitive Assessment; WTAR = Wechsler Test of Adult Reading; PHQ = Patient Health Questionnaire; DPX = Dot Pattern Expectancy; DKEFS = Delis-Kaplan Executive Function System; WCST = Wisconsin Card Sorting Test; CPT = Continuous Performance Test; CFQ = Cognitive Failures Questionnaire; PCI = Perceived cognitive impairment subscore; PCA = Perceived cognitive abilities; EFPT-e = Executive Function Performance Test-enhanced.
DPX Relationships With Neuropsychological Measures
Spearman’s rho correlation values between DPX performance and Delis-Kaplan Executive Function System (DKEFS) performance are shown in Table 3 and between DPX performance and Wisconsin Card Sorting Test (WCST) and Continuous Performance Test (CPT) in Table 4. Spearman’s rho values were interpreted as 0.1 = weak relationship, 0.4 = moderate relationship, and 0.7 = strong relationship (Dancey & Reidy, 2007). Evaluation of the relationship between DPX Accuracy and DKEFS demonstrated a moderate relationship with the DKEFS Tower Total Achievement (rs = −.55). A moderate effect was also demonstrated between DPX Probe Reaction Time and DKEFS Letter Fluency performance (rs = .41).
Correlations Between DPX and DKEFS Performance.
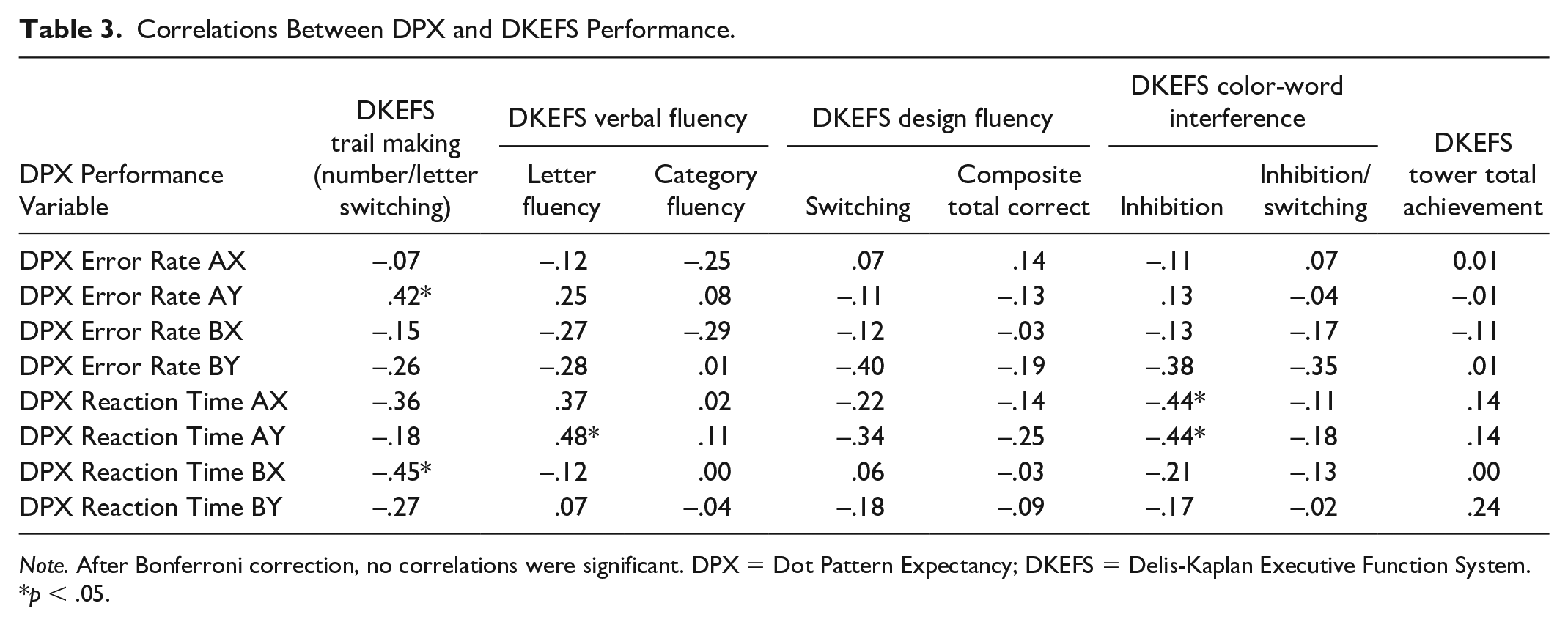
Note. After Bonferroni correction, no correlations were significant. DPX = Dot Pattern Expectancy; DKEFS = Delis-Kaplan Executive Function System.
p < .05.
Correlations Between DPX and Other Neuropsychological Measures.
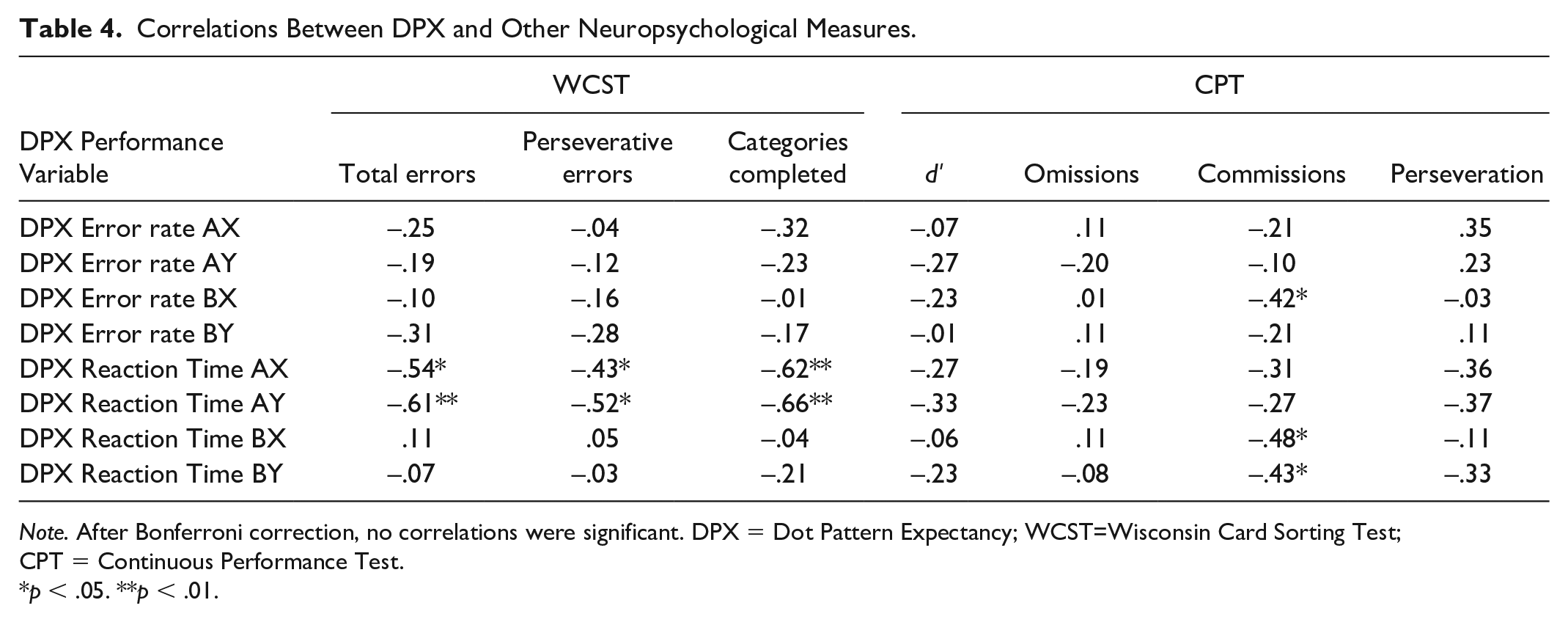
Note. After Bonferroni correction, no correlations were significant. DPX = Dot Pattern Expectancy; WCST=Wisconsin Card Sorting Test; CPT = Continuous Performance Test.
p < .05. **p < .01.
Evaluation of the relationship between DPX AY Accuracy and DKEFS demonstrated a moderate relationship with the DKEFS Trailmaking (rs = .42). A moderate effect was also demonstrated between DPX BY Accuracy and DKEFS Design Fluency Switching (rs = −.40). Additional moderate effects were identified between the DPX AX Reaction Time and DKEFS Color-Word Interference-Inhibition (rs = .44*) and between DPX AY Reaction Time and DKEFS Verbal Fluency-Letter Fluency (rs = .48*) and DKEFS Color-Word Interference-Inhibition (rs = .44*). Finally, a moderate correlation was demonstrated between DPX BX Reaction Time and DKEFS Trailmaking (rs = −.45).
The only moderate or greater relationship identified between DPX Accuracy and the WCST or CPT was noted between the DPX BX Accuracy and CPT Commissions (Table 4). However, several moderate effects were demonstrated for DPX Reaction Times and the WCST including between DPX AX Response Time and WCST Total Errors (rs = −.54*), WCST Perseverative Errors (rs = −.43*), and WCST Categories Completed (rs = −.62**). Several moderate correlations were also present between DPX AY Response Time and WCST including WCST Total Errors (rs = −.61**), WCST Perseverative Errors (rs = −.52*), and WCST Categories Completed (−.66**). Finally, moderate correlations were demonstrated between DPX BX Response Time and CPT Commissions (rs = −.48*) and between DPX BY Response Time and CPT Commissions (rs = −.43*).
DPX Relationships With Self-Report and Objective Measures of Functional Cognition
The strongest relationship between DPX performance and self-report measures was a moderate relationship between DPX BX Accuracy and the Cognitive Failures Questionnaire (CFQ; rs = .44*; Table 5). Furthermore, moderate relationships were observed between DPX BX Accuracy and Functional Assessment of Cancer Therapy-Cognitive Function (FACT-Cog) Perceived Cognitive Impairment subscale (PCI) (rs = .42), between DPX AX Reaction Time and Executive Function Performance Test–Enhanced (EFPT-e) Total Cues (rs = .40) and Bill Pay Total Cues (rs = .42).
Correlations Between the DPX and Functional Cognitive Measures.
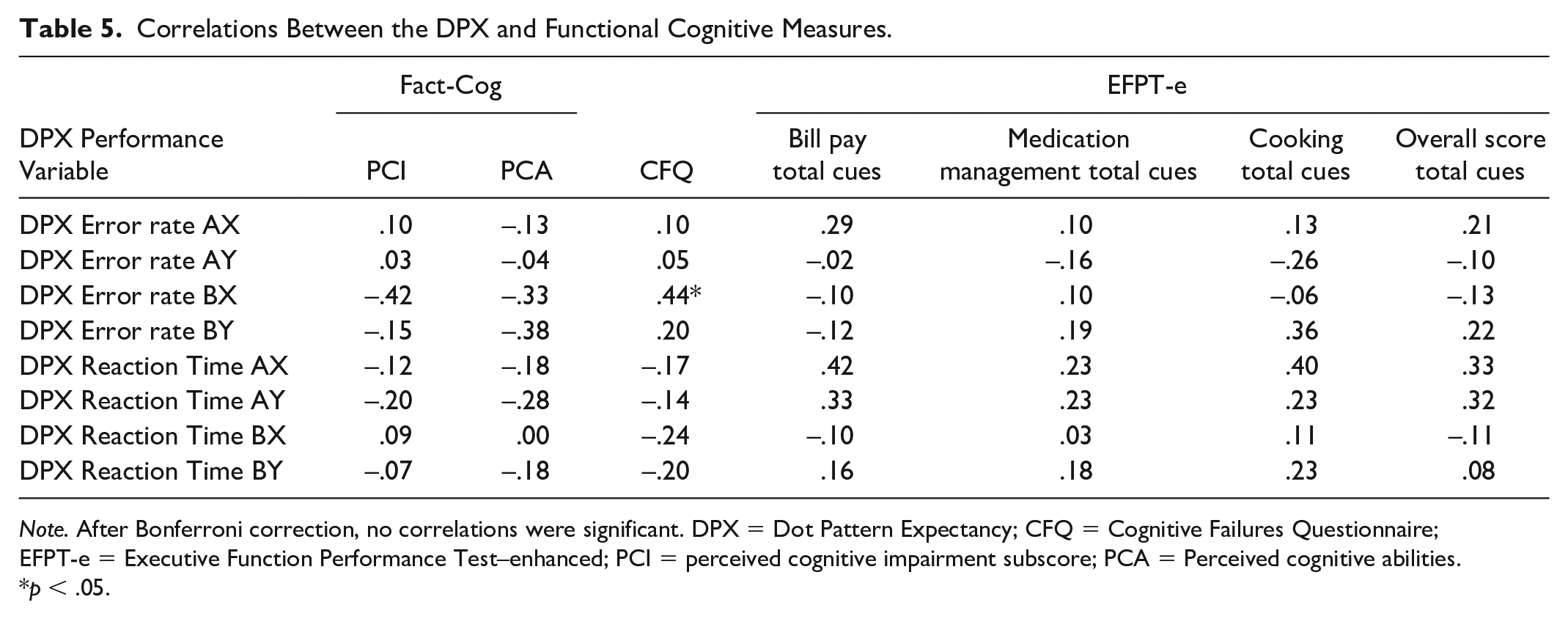
Note. After Bonferroni correction, no correlations were significant. DPX = Dot Pattern Expectancy; CFQ = Cognitive Failures Questionnaire; EFPT-e = Executive Function Performance Test–enhanced; PCI = perceived cognitive impairment subscore; PCA = Perceived cognitive abilities.
p < .05.
Discussion
The goal of this study was to conduct a preliminary evaluation of the performance of a sample of women treated for breast cancer on a cognitive neuroscience measure of goal maintenance, the DPX, and to compare to performance on validated neuropsychological, self-report, and performance-based tests of goal maintenance. This study was conducted in response to calls from the NCI for renewed efforts in the assessment of CRCI. Specifically, NCI noted the disparate understandings of CRCI resulting from past research in which assessment was conducted in disciplinary silos (NCI, 2018). A comprehensive understanding of CRCI requires a transdisciplinary evaluation that not only includes multiple disciplines working independently toward the same goal but more specifically working across disciplines to integrate expertise (Choi & Pak, 2007). DPX performance pattern in women treated for breast cancer in the current study reflects that of the prior literature in healthy controls with the greatest rate of errors in the AY condition followed by the BX condition (Jones et al., 2010; Lopez-Garcia et al., 2016). While no consistent relationships were present between the DPX and other methods of assessment, patterns that did emerge from the data will be discussed below.
Results in the study demonstrated highest error rates for the AY followed by the BX conditions. Higher levels of goal maintenance are associated with this pattern of errors and lower levels of goal maintenance are associated with more errors on AX and BX trials and few errors on AY trials (Henderson et al., 2012; Lopez-Garcia et al., 2016). A correct cue (A) serves as an indicator that the probe to follow may complete the sequence (AX). This can lead to individuals with relatively intact goal maintenance being predisposed to respond positively for whatever probe that follows, thus leading to more AY errors. In contrast, individuals with poorer goal maintenance may not use the correct cue (A) or incorrect cue (B) as indicators that a higher level or lower level of alertness, respectively, is needed for the probe that follows (Boudewyn et al., 2019; Lopez-Garcia et al., 2016).
DPX error rates predominately had absent to weak relationships with neuropsychological measures in the current study. There were three notable exceptions to this. AY error rates demonstrated a moderate relationship with DKEFS Trail-making (rs = .42*). This direction of the relationship is logical as individuals with higher scores in cognitive flexibility may very well have more errors on the AY condition. Individuals with higher cognition and higher levels of goal maintenance are able to use the A cue to prepare an appropriate response to the subsequent probe; because A cues are most frequently followed an X probe, clients with higher levels of goal maintenance make the most errors in the more infrequent AY condition (Jones et al., 2010; Lopez-Garcia et al., 2016). Second, a negative moderate relationship between CPT Commissions and BX error rate emerged from the data (rs = −.42); in other words, individuals with poor attention also may have been less likely to utilize the inaccurate cue (probe) as a signal for predicting an overall inaccurate cue sequence (BX). It is possible that individuals with inattention would also present with lower levels of goal maintenance as allocation of attentional resources is necessary to maintain a goal in working memory (Paxton et al., 2008). Finally, an unexpected relationship between BY error rate and DKEFS Design Fluency scores, indicating that higher levels of visual perception and cognitive flexibility are associated with increased BY error rates. The reason for this finding is unclear as BY is intended to serve as a control condition within DPX (Boudewyn et al., 2019).
Individuals with schizophrenia, in whom the majority of DPX evaluation has occurred, have generally slower reaction times than healthy controls across each of the conditions (Calvin & Redish, 2021). Interestingly, current findings suggest a pattern of relationships between reaction time speed in women with CRCI and performance on neuropsychological tests. Reaction times in the A cue conditions (AX, AY) demonstrated moderate negative relationships with WCST total number of errors and perseverative errors and for DKEFS Color-Word Interference Inhibition scores. In other words, slower reaction times were associated with lower levels of cognitive flexibility and inhibition or vice versa. Furthermore, B cue responses demonstrated moderate negative relationships with CPT commission errors and DKEFS Trail Making performance such that slower response times were associated with an increased number of errors (i.e., higher levels of inattention) and worse cognitive flexibility.
Relationships between DPX error rate and self-report and PBT’s of executive function are largely absent to weak. BX error rates were an exception to this with moderate relationships between the Fact-Cog and (rs = −.42) and CFQ (rs = .44), both self-report measures of everyday cognitive functioning. This relationship indicates that individuals who made more BX errors were more prone to self-reporting higher levels of cognitive impairment in daily life. Furthermore, DPX reaction times had few substantial relationships with either self-report or PBT measures; however, individuals with slower reaction times in the AX DPX condition required more cues for performance in the bill pay (rs = .42) and cooking tasks (rs = .40) of the EFPT-e.
This study performed a preliminary exploration of relationships across assessment levels of cognition in women with CRCI in an effort to create a broader but more detailed perspective of CRCI in women treated for breast cancer. Future studies in this area should consider the use of a larger sample size and a sample more diverse demographically. This study may have been limited by the heterogeneity in the sample’s treatment history for breast cancer. Further research in this area is warranted to meaningfully bridge findings across disciplines.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
University of Missouri IRB: 2010735