
Abstract
In pediatric occupational therapy, there is insufficient evidence examining assessment tool selection by occupational therapists and how assessment tools contribute to occupation-based practice. To examine the perceptions of occupation-based assessment tool selection by pediatric occupational therapists, a phenomenological research study was conducted with six pediatric occupational therapy practitioners. Three themes emerged from participants’ perspectives: the centrality of occupation, selecting the just right tool, and practice implications. Participants recognized the need to integrate occupation-based assessments into practice but reported decreased opportunities secondary to training, available supplies, lack of awareness of foundational constructs, and organizational expectations. The use of occupation-based assessments positively enhances pediatric occupational therapists’ clinical practice by upholding the core occupational beliefs of the profession throughout all phases of service delivery.
Introduction
Occupational therapy practitioners aim to facilitate participation in everyday occupations or meaningful life activities with their clients (American Occupational Therapy Association [AOTA], 2020). While approaches to meet that aim vary considerably, the core beliefs of the profession remain constant and include an understanding of the reciprocal relationship between occupation and health and the therapeutic benefits of occupation in clinical practice (AOTA, 2020; Wilcock & Hocking, 2015). The application of these beliefs in pediatric occupational therapy practice involves the habilitation of children’s skills to attain age-expected milestones through engagement in occupations (Cronin & Mandich, 2016; Kuhaneck & Case-Smith, 2020).
When selecting assessment tools during the initial evaluation, pediatric occupational therapists are responsible for collaborating with caregivers to determine supports and barriers to occupational performance and holistically assessing the client (AOTA, 2020; Chang & Richardson, 2020; Kolehmainen et al., 2013). Commonly, therapists prioritize assessment tools reflective of psychometric properties (Streiner et al., 2015) and make assessment tool decisions based on availability; policies and systems; fiscal implications; and practitioner training and comfort (Kuhaneck & Case-Smith, 2020). Resultantly, the focus of assessment selection has deviated from the profession’s foundational principle of analyzing occupational performance as pediatric occupational therapists report minimal utilization of top-down or occupation-based tools despite the profession’s movement toward occupation-centered practice (Bagatell et al., 2013; Kiraly-Alvarez, 2015; Mulligan, 2014; Skuthan & Stav, 2023). Limitations in children’s body functions or structures do not confirm or determine challenges within their occupations or promote occupation-based interventions (AOTA, 2020). Best practice recommends the incorporation of occupation-based assessments to address children’s engagement in occupations (Cahill & Beisbier, 2020; Chang & Richardson, 2020).
A few studies explore assessment tools in pediatric occupational therapy practice. Lee et al. (2018) examined assessment tools categorized into 10 occupational therapy practice domains. Commonly selected assessment tools by occupational therapists in South Korea were indicated (N = 105); however, assessment tools were not classified as occupation-based or skill-based (Lee et al., 2018). Peters and colleagues (2019) conducted a similar study, concentrating on children with cerebral palsy. Selected assessment tools did not include additional diagnoses or classification as occupation-based or skill-based (Peters et al., 2019). Recently, Skuthan and Stav (2023) indicated incorrect classification of assessment tools as occupation-based by pediatric occupational therapists and an overwhelming selection of skill-based assessments in practice. Despite occupational therapy’s focus on prioritizing occupation, there is a lack of evidence identifying the use of occupation-based assessments in pediatric occupational therapy practice.
Despite the profession’s intended focus on occupation, the use of occupation-based assessments in practice and the resultant implications on subsequent therapeutic interactions with clients is limited. This study explored pediatric occupational therapists’ use of occupation-based assessments in clinical practice. The research question is, how do occupation-based assessments shape clinical practice for practicing pediatric occupational therapists?
Method
A phenomenological design was selected, following Moustakas’ (1994) approach to identify the experiences of others and their perceptions regarding a particular situation or event. The qualitative research design described pediatric occupational therapists’ use of occupation-based assessment tools and the application of tools throughout service delivery. In the context of this study, occupation-based assessments were defined as assessment tools that measure a client through a top-down approach, beginning with an analysis of the client’s interest and ability to perform occupations; these assessment tools may specifically target occupations that are meaningful to the individual and/or caregivers. Conversely, skill-based assessments were defined as assessment tools that measure the body functions and/or performance skills of a client using a bottom-up approach, beginning with an analysis of the client’s impairments and/or specific skills. Institutional Review Board approval was obtained.
The participants for this study were selected through purposive sampling to select a specific population of pediatric occupational therapists who volunteered to participate at the conclusion of the preliminary quantitative study. Purposive sampling divulges information-rich material from specific individuals to explore the phenomena at hand (Richards & Morse, 2013). Initial sampling for the preliminary quantitative study used an infographic research invitation posted to pediatric occupational therapy groups on social media at the beginning of 2021 including two separate Facebook groups titled Pediatric Occupational Therapists with over 44,400 members and 9,400 members, respectively; the School-Based Occupational and Physical Therapists groups with roughly 25,300 members, and Research4OT with over 6,800 members (Facebook, 2020). Participants in the quantitative study were pediatric occupational therapists who have provided therapeutic services to children between the ages of birth to 21 throughout their careers. For the follow-up qualitative study, participants who participated in the quantitative inventory and elected to participate in the qualitative collection through the provision of their email addresses were included. Excluded participants in the quantitative phase included occupational therapists who do not practice in pediatrics, and certified occupational therapy assistants as the assessment tool selection process is determined by the supervising occupational therapist. Excluded participants in the qualitative phase included pediatric occupational therapists who do not use at least one occupation-based assessment tool as identified by Mulligan (2014). Out of the available pediatric occupational therapy assessments, participants who indicated the use of the greatest number of occupation-based assessments as categorized by Mulligan (2014) were contacted first to provide the richest possible evidence. The contacted participants indicated the use of six to 16 occupation-based assessment tools in clinical practice. Participants were contacted in the order of their response to participate with initial contact of the participants indicating the use of 16 occupation-based assessment tools. A total of 19 participants were solicited with a total of six included in the qualitative study. The participants were contacted simultaneously and included in the study one at a time in the order in which they responded until the data reached saturation. To determine the appropriate sample size for the study, qualitative samples must be large enough to uncover “new and richly textured understanding” and small enough to promote “deep, case-oriented analysis” (Sandelowski, 1996, p. 183). Interviewing continued until the researcher deemed that data saturation had been reached and no new codes were presented from subsequent interviews, occurring at the conclusion of the sixth interview.
The qualitative data were collected using semi-structured interviews over Zoom and transcribed using the software’s transcription feature (Zoom Video Communications, 2021). Data were collected through the creation of a semi-structured interview included in Figure 1 by the researcher with the utilization of questions that prompted information sharing without bias or integration of leading questions (Moustakas, 1994). The semi-structured interview acquired background information for each participant, including years of practice, entry-level degree, and primary practice setting. The remainder of the interview consisted of questions generated following a review of the literature pertaining to occupation-based practice including barriers and facilitators. In addition, questions reflected clinical practice as outlined in the Occupational Therapy Practice Framework: Domain and Process, 4th ed. (AOTA, 2020), the Standards of Occupational Therapy Practice (AOTA, 2021), and Occupational Therapy Practice Guideslines for Ages 5 – 21 years (Cahill & Beisbier, 2020). A draft and final version of the interview questions were reviewed and edited by three occupational therapy researchers; one of whom is experienced in pediatric practice, two of whom have expertise in occupation-based practice, and all three with experience in qualitative research. The participants were asked to define occupation-based practice, provide examples of occupation-based assessment tools, and identify strengths and barriers to the application of occupation-based assessment tools.
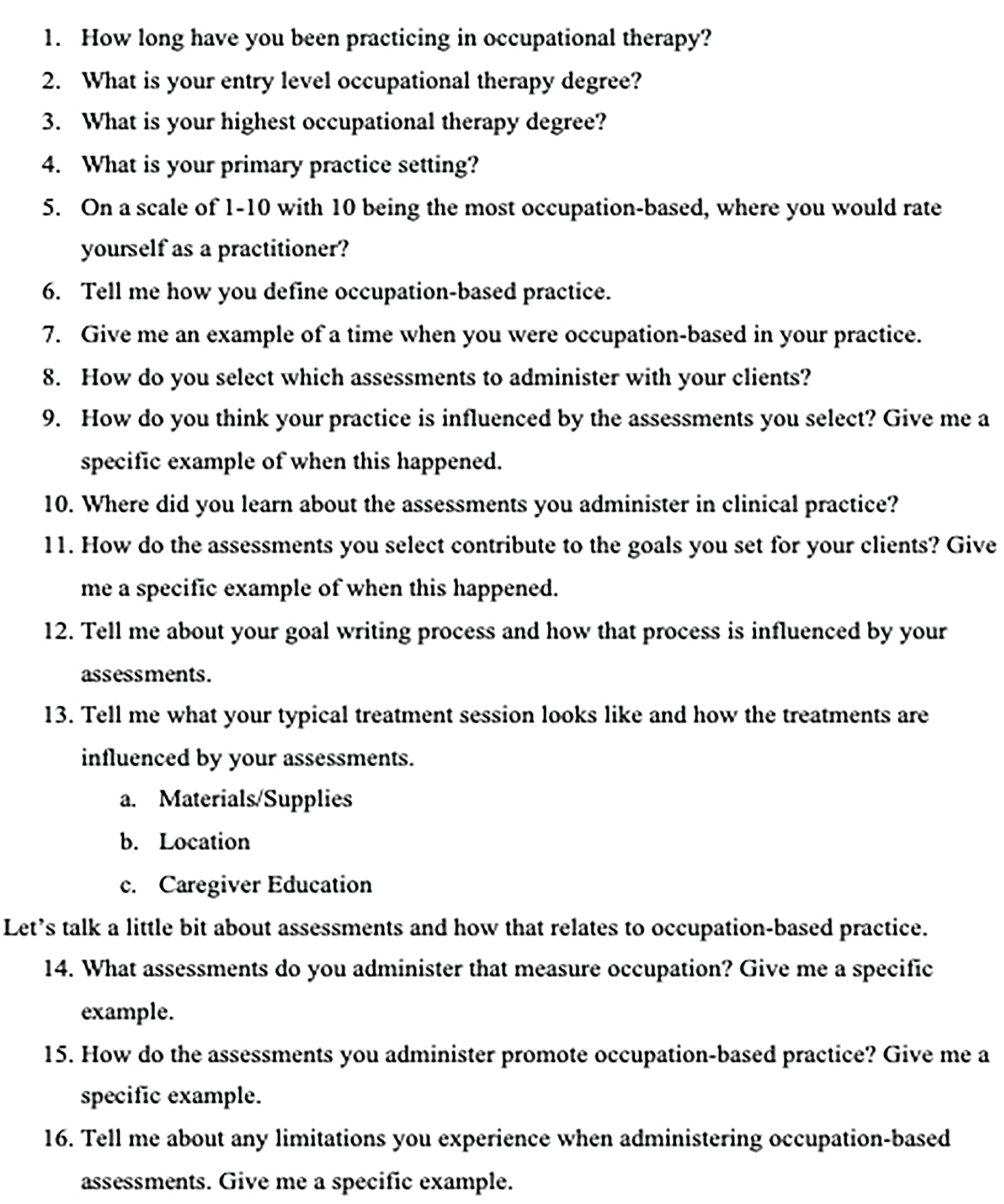
Interview Guide for Semi-Structures Interviews.
The Zoom (Zoom Video Communications, 2021) recordings were reviewed using the Zoom-generated transcripts. The researcher listened to the recordings to correct any errors and ensure accuracy. The participants were sent the transcriptions to confirm for accuracy and/or correct any errors with no changes required. Next, the researcher followed Moustakas’ (1994) six-step approach to the phenomenological model using phenomenological reduction and QDA Miner Lite software (Provalis Research, 2016).
To allow for bracketing to occur, the researcher kept a written journal throughout data collection to include biases such as the importance of occupation-based assessment tools and the importance of occupation to promote the view of the participants instead of the researcher. For horizontalization, the researcher repeatedly reviewed the articles, kept a well-loved list of significant statements, and re-watched the recordings through the lens of the person-environment-occupation model (Law et al., 1996). Aspects related to the person included therapist training, years of experience, comfort level of occupation-based practice, value of occupation within practice, and the level of occupation-centeredness of the participant. Aspects related to the occupation included the development of treatment plans, the administration of assessments, billing process, and family education. Finally, aspects of the environment included the clinical setting of the participants, the selected assessment tools, and the culture of the setting of the participants. For the textural description, the list of significant statements was condensed to reflect how clinical practice is influenced by occupation-based assessment tools. Finally, in textural–structural synthesis, the researcher linked the selection of occupation-based assessments and resultant influences on clinical practice to the list of significant statements for final thematic selection.
To confirm the trustworthiness of the study and enhance the methodological rigor, member checking was performed during the data review process of the semi-structured interviews. After the researcher identified themes and descriptions within the data, the researchers reviewed themes and descriptions to finalize the data analysis. The triangulation of data occurred through multiple methods as the researcher collected the data through audio recording, transcription, and note-taking during the semi-structured interview process prior to analysis (Creswell & Plano, 2007). In addition, there was sufficient information described in the study to allow for replicability.
The positionality statement was developed through reference to Tong and colleagues (2007) consolidated criteria for reporting qualitative research (COREQ) and Wainstein and colleagues (2023) establishment of positionality through self-reflexivity. As such, the researchers identify as occupation-based, occupational therapy practitioners with experience in academic instruction and both pediatric and adult clinical practice. Their clinical experiences support the acquisition and integration of occupation-based assessments to promote evidence-based, occupation-centered clinical practice. The researchers are passionate and committed to infusing occupation into occupational therapy practice via education to their students and application to their clients and are continuing to work toward this goal. The interviewees were informed before and at the time of the interview that the researchers are occupational therapists with the primary researcher performing interviews as part of doctoral work. The participants provided feedback on the accuracy of completed transcripts. Through the use of bracketing and member checking, the researchers hope this manuscript can serve as a helpful reminder of the importance of occupation-based assessment tools and their resultant implications for clinical practice.
Results
In total, six pediatric occupational therapists participated in semi-structured interviews with the researcher. The participants varied in experience ranging from 3 to 40 years of practice, with four obtaining their Master of Science and two obtaining their Bachelors in Science upon entering clinical practice. In addition, three of the participants indicated school-based practice as their primary setting, two indicated outpatient practice, and the final participant indicated home health/assistive technology provision. In total, five of the six participants identified as female, and the remaining participant identified as male. The included participants indicated frequent utilization of at least six 11-based assessment tools as indicated on the inventory, with some using as many as eleven occupation-based assessment tools. Finally, the participants represented a geographically diverse representation of practice including practitioners in the Northeast, Southeast, Midwest, West, and Southwest.
Pseudonyms were utilized to protect confidentiality. The therapists participated in interviews lasting approximately 1 hr and shared their perspectives and experiences about their professional engagement specific to occupation-centered practice and the utilization of occupation-based assessments. The likenesses of their perspectives are presented as themes that emerged from the data. The three themes that emerged from the data were the centrality of occupation, selecting the just right tool, and practice implications, and collectively depicted as the bridge of occupation-based assessment.
The Centrality of Occupation
The centrality of occupation theme is defined as the incorporation of occupation into the center of practice and includes subthemes of therapist background, value of occupation, and out of my control. It elucidates the philosophical foundations of the profession whereby practitioners utilize occupation as the means and ends to service delivery, beginning with theoretical underpinnings. The practitioners’ core beliefs informed the inherent value for occupation through occupation-based assessments and the meaning associated with occupational engagement. Therapists acknowledged factors that influenced the inclusion of occupation in practice that they do and do not have control over.
When reflecting on training and preparation to practice as pediatric occupational therapists, there were differences identified by participants. Erin stated, “When I started, there was no such thing as standardized occupational therapy assessments, when I was in school, not even a thing. The only one I think was the Ayres Sensory Integration test . . . assessing was very informal.” Brian, a newer graduate, indicated that school prepared him for practice, “In class we got to practice a lot on actual kids which was really cool and OT school was really powerful and then we practiced on each other . . . and have trainings at work about certain assessments.” Although both participants are currently practicing, education and exposure to assessment tools varied considerably. Experience and exposure were commonly indicated to affect the selection of assessments by pediatric occupational therapists. Lauren stated, “I have school psychologists telling me that they [students] need to have a score to qualify for services, which is not true, but if you’re a new therapist you think it is true, then you do it.” She continued, I don’t know if the new therapists quite get that [assessment selection] because they don’t really have an understanding of our history, like from the beginning to the mid-century, when we jumped into medicine, we just ruined ourselves. And we have never been able to get out back from that I don’t think I think we rallied and we’ve never gotten back . . . I think that’s part of the reason why we can’t get school-based therapists to stop using impairment-based assessments, because they don’t understand theory and if you don’t understand the theory they are working under, then you can’t name and frame what you do, or why you do it, and if you don’t know why you’re doing what you’re doing, then of course you don’t know if they qualify, you know they need your services or not right.
Occupation was indicated as beneficial for professional practice when incorporated into the assessment process by selecting occupation-based assessments instead of skill-based assessments. Heather commented, Those occupation-based tools that are looking from more of a top-down approach, kind of takes a little bit more clinical reasoning. So, they [kids] can thrive in those occupations that are identified through those more top-down assessments, so I think at times, using a more occupation-based assessment process can be a little more work for the practitioner itself or themselves, but I do feel like the work is warranted because it provides more of a holistic perspective of the child, or the student as an occupational being.
Finally, Allie reviewed the why behind occupation-based practice. She emphasized the need to set a standard greater than what must be billed for insurance reimbursement. She emphasized that the care is dictated by the therapist’s focus and this focus must be occupation, commencing during the assessment process: Providing that high quality care, I’m not about just meeting the standard, you have to be above that standard, because that standard bar is set very low okay and I know when I have families coming in here that are paying a $3,000 deductible . . . so that’s part of my mission, I don’t have to put those things in to get paid, right? I get paid the same for 97530 as anyone else. I get paid the same for the codes as anybody else but that’s not what I’m trying to do, I’m trying to change the fabric of our community.
When reflecting on materials, Lauren indicated that the assessments selected simply result from the concept of, “you just do what your fieldwork therapist does.” Allie reflected, “I think people should do standardized testing I understand it’s expensive and we don’t like to do that.” Lauren also stated, “They’re [therapists are] using impairment-based assessments and they don’t have a theory then you’re going to do what they [fieldwork educators] do and then, when you get out in practice, you’re going to do what they [fieldwork educators] do so yeah . . . there has to be something that switches.”
Practice Implications
The practice implications theme is defined as the direction, tone, and concentration of occupation in the practice process as influenced by the use of occupation-based assessments at the initiation of services. This theme includes subthemes practice confusion and what progress should be depicting stakeholder misunderstandings of occupation in practice and the disparity between how occupation should be infused in practice compared to the actual presence of occupation in practice. Participants emotively explained how practice is influenced by the selection of assessment tools and the resultant importance of selecting occupation-based assessment tools to integrate occupation into all facets of pediatric occupational therapy clinical practice. Participants expressed frustration, exasperation, and even anger with the inconsistent use of occupation-based assessment tools by fellow pediatric occupational therapists. Furthermore, participants described the misalignment between the profession’s foundational roots in occupation and current practice that deviates from occupation. Lauren began by reviewing the philosophical roots of the profession, explaining how the selection of skill-based assessments are hindering the understanding of occupation and the application of occupation-based practice: Our teams do not assess what they treat and we don’t know what they do and that’s a problem in our profession. Assessments and theory and all of that becomes a problem in our profession, like we’re not important, because it doesn’t make sense that I look at your fine motor and then you go in and make a sandwich . . . But we hitched our wagon to medicine, we did a really huge disservice to ourselves, you know, we were holistic and Meyer and everybody . . . [but] we just jumped right the hell on to medicine and reimbursement and the minute we did that . . . I mean if Meyer was talking holistic and he was talking purposeful activity, he was talking temporal adaptation and he was talking, you know healthy populations back then. And here we are, we still haven’t done it.
Erin echoed her common challenges within clinical practice stemming from the lack of understanding of occupation, affirming, “unfortunately, you know, we became known as the handwriting teachers and it’s like no, I’m not a handwriting teacher . . . that’s not really what I do unless a student has a true deficit . . . I’m an occupational therapist.”
The participants alluded to the benefit and unique scope of pediatric occupational therapy that can be provided when appropriately assessed through the selection of occupation-based assessments. Allie reviewed that occupation-based assessments allow her to focus on function throughout practice and without the appropriate selection assessment, this can negatively affect her service delivery. She stated, “I think especially with the Autism population is it sometimes the tests are not a good assessment of skills, that’s why I have gone to purchasing things like the M-FUN and the GOAL, because it’s got that function.” In summary, participants identified that the selection of occupation-based assessments allows them to provide occupation-based practice. They indicated the current misalignment in practice where therapists are commonly selecting skill-based assessments instead of aligning with historical roots and occupation.
To begin the goal-writing process, participants identified the need to review completed assessments and collaborate with the recipients of services to guide treatment through an occupation lens. Allie referred to her utilization of occupation-based assessments but indicated the priority of her goals to be reflective of what is most important to the client and his or her family: When I’m writing a goal, I will, I’m always going to ask family and the client what areas do you want to address, I can take testing and I can say, well, I really believe there’s a problem with some ADL, right, and they may come and say to me, you know what, that ADL isn’t important . . . it doesn’t matter if it’s important to me, it matters if it’s important to them.
Allie commented, “My philosophy is that you never write a goal to an assessment, ever ever ever and if I audit and find it, you’re going to have to change it . . . our goals here are measurable and function based. We don’t say you can now stand on one foot.”
Heather positively commented on her unique perspective on goal writing. She does not focus on specific skills or common impairment-focused goals but rather uses the information from her occupation-based tools to create goals that are holistic. Heather stated, “I write completely different than other practitioners in my setting. I’m not someone that writes a lot of baseline alignment or letter sizing goals.” Lauren also indicated the need to write goals that are occupation-based. She detailed that although the assessment and score on the assessment are important, it is about the client’s needs and keeping the focus on occupation: We are under the impression that we have to have a number and assessment and . . . they have to be all independent, like instead of us just saying you know he wants to be able to get up and make a damn sandwich, so that’s your goal.
Conclusively, the participants echoed the influence of occupation-based assessments to create occupation-based goals with the awareness of external influences to promote occupation-based practice.
Selecting the Just Right Tool
The selecting the just right tool theme reiterates the importance and value of using occupation-based assessment tools within pediatric occupational therapy practice. Participants exposed the assessment tool selection process, identified the reasoning behind their commonly selected assessment tools, and how they learned about the occupation-based assessment tools they commonly administer in clinical practice. All participants referenced the benefits of occupation-based assessment tools and seek opportunities to build their assessment collections.
To begin the assessment selection process, participants indicated using skilled clinical observations, reviewing referral information, and/or collaborating with other members of the team. Lauren specified, “I can observe a classroom and observe a kid and then that’s how I usually start as I do an observation and then I get an idea.” Erin referenced the value of collaboration with members of the interdisciplinary team stating, “I have talked to the teacher, I’ve talked to the case manager, we have team meetings every week and we’ll discuss the students so I’ll get a good idea of what I’m looking for with that kiddo and that’s what I base [for] my assessment.” Brian referenced the need to remember the referral information, “I usually like to look at what they’re being referred for and then kind of match that up with what we have available.” No two therapists identified selecting assessment tools in the same manner.
When reviewing the specific assessment tools selected in clinical practice, participant answers varied but focused on an awareness of occupation-based assessment tools. Kim stated, “I avoid any skill, like I’ve moved away from the Beery VMI, I’ve moved away from any of those really like non-occupation-based assessments . . . and I’ve been purchasing assessments.” She further indicated a need to transition away from skill-based assessments, “I recently purchased the REAL, or the Roll Evaluation of Activities of Life, and that is what I’m using now . . . it wasn’t really an assessment that I found to be something I liked, but I needed, something that was going to give me that quantity that data that insurance companies want.”
Conclusively, when labeling assessment tools as occupation-based, participants most commonly recalled and referenced the Print Tool, The Jordan Left/Right Reversal Test, The Weekly Calendar Planning Activity, the GOAL, the REAL, the COSA, the PEDI, the COPM, and the Test of Handwriting Skill Revised.
To identify how participants learn about the occupation-based assessment tools they commonly select, the majority of participants indicated proactive measures to build their assessment toolkits. Allie stated, “I’m always researching,” and Erin incorporates research, Facebook groups, and professional organization membership benefits.
The thematic analysis can be visualized through the concept of a bridge located in Figure 2. The bridge of occupation-based assessments is comprised on one side of the theme centrality of occupation with its subthemes therapist background, the value of occupation, and out of my control while the other side consists of the theme practice implications and its subthemes practice confusion and what progress should be. Connecting the two sides of occupation and clinical practice, sits the final theme selecting the just right tool as the keystone, allowing the philosophical foundations of occupation to be applied to practice. Without the utilization of occupation-based assessment tools, the bridge will collapse as the unique scope of the profession of occupational therapy—occupation is lost and skilled intervention becomes mastery of developmental milestones instead of occupational performance and participation.
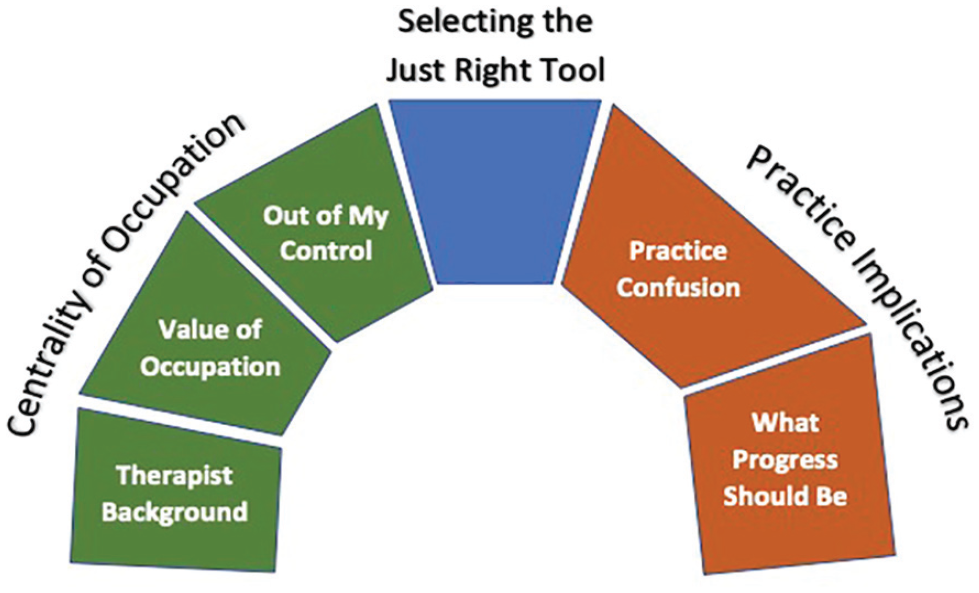
Concept Image of the Bridge of Occupation-Based Assessment.
Discussion
The findings are consistent with the literature in identifying the benefits and usefulness of occupation-based assessment tools in shaping clinical practice. The participants’ professional experiences reflect the best practice identified in the literature (Bagatell et al., 2013; Chang & Richardson, 2020; Kiraly-Alvarez, 2015; Kolehmainen et al., 2013) in prioritizing the use of occupation-based assessments defined by the centrality of occupation theme. The participants noted significant benefits for clinical practice from caregiver understanding/support, goal attainment, and volition within treatment sessions when integrating occupation into all aspects of service delivery. The participants additionally emphasized the importance of didactic learning and clinical experiences to promote the integration of occupation-based assessment tools within occupational therapy training for the focus of service delivery to seamlessly integrate occupation and to aid in minimizing practice confusion. Participants also concluded that intentional occupational therapy practice reflects true occupation through the selection of occupation-based tools as the assessment shapes many of the logistics of practice to include chosen interventions, the context of interventions, the extent of family/caregiver involvement, and how documentation is completed. Through the selection of occupation-based assessment tools, occupation remains the focal point to prioritize goals and practice decisions. Conclusively, by selecting occupation-based assessment tools, occupation is placed at the center of all future interactions.
The findings explored occupation-based assessments within pediatric occupational therapy practice by inquiring how the use of occupation-based assessment tools shape clinical practice through the theme practice implications. The interviewed therapists indicated selection of occupation-based assessments due to perceived insurance expectations, facility resources, exposure by fieldwork educators, and even to acquire a numerical score for service eligibility. Interviewed participants indicated greatest clinical utility when selecting assessments based on occupation constructs as opposed to standards of tests and measurements which suggests selecting assessments based on strong psychometric properties. Caregivers, members of the interdisciplinary team, and therapists will continue to present with confusion regarding the scope of occupational therapy practice when children are assessed on specific skills without the tie and/or application to occupation.
Furthermore, the findings of this study inform both direct clinical practice and systematic change. Specific to direct clinical practice, measurement of client progress, documentation, and goals should all incorporate occupation. Current goals vary among practitioners and oftentimes reflect assessment skill mastery or policy-level expectations (Kolehmainen et al., 2013). If a standard in goal writing could occur within the profession through consistencies in electronic documentation software and/or through requirements dictated by reimbursement organizations to reflect occupation with the achievement of goals only through occupational performance, this shift would realign practitioners to an occupation-based perspective. The documentation systems could reflect the Occupational Therapy Practice Framework (AOTA, 2020) outlined occupations to further link the purview of professional practice to clinical application. Progress could then be measured through occupation instead of attainment of “normal” scores on a standardized assessment.
These findings also inform systematic change in support of occupation-based practice. Given that the use of occupation-based assessments influences the use of occupation in practice, and thus solidifies a unique approach when working with children, it is paramount that practitioners take on the role of educator and advocate to promote the use of occupation-based assessments. In these roles, occupational therapy practitioners should inform administrators, third-party reimbursors, policy makers, and families of the importance of occupation-based assessments. The goal of education and advocacy efforts is to use occupation-based tools, establish service eligibility guidelines based on occupation, evolve documentation systems to reflect occupation and transition reimbursement expectations toward occupation.
The interviewed therapists also highlighted the importance of the theoretical application to clinical practice for best assessment tool selection as evidenced through the selecting the just right tool theme. When therapists select the developmental frame of reference (Creek, 2014), occupation is no longer the focus, and instead developmental milestones and/or assessment skill mastery take precedence. Therapists may simply be practicing within the developmental frame of reference (Creek, 2014) as they administer the available assessment tools to recipients of their services with automaticity. Pediatric occupational therapy practitioners may be in need of a new theoretical framework such as the Dynamic Model of Occupation-Based Practice (Psillas & Stav, 2021) that supports professional reasoning around the constructs of occupation, meaningful and purposeful value, therapeutic intent, and engaged participation to depict occupation-based practice. In addition, the associated Occupation-Based Practice Assessment (Stav et al., 2022) includes a scale to measure the occupation-centeredness of assessment tools. By reframing the theoretical alignment and focusing on occupation, progress can be measured through occupational function/dysfunction, and approaches to intervention can be provided along an occupation-guided continuum including adaptations needed for occupational performance. Within the realm of pediatric occupational therapy practice, it is also pivotal that therapists incorporate the family into all facets of service delivery to incorporate meaningful occupations and co-occupations of the child and the family (Fingerhut, 2013; Kolehmainen et al., 2013). Pediatric occupational therapists must synthesize occupation into all facets of service delivery and must be mindful of the type of assessment tool selected to remain holistic, client-centered, and occupation-based.
Conclusion
The findings of this research study provide insight into how occupation-based assessments affect clinical practice. Future collaboration between didactic and fieldwork educators may be beneficial to enhance the integration of occupation within all aspects of service delivery. Further study is recommended to examine the influence of occupation-based assessment tools on length of care, duration to implementation, how goals are created, and materials and contexts of practice.
Footnotes
Acknowledgements
This work was based on a dissertation completed in partial fulfillment of the requirements for the PhD in Occupational Therapy at Nova Southeastern University. The authors would like to acknowledge the other committee members for their contribution to the study: Dr. Elise Bloch and Dr. Donna Colaianni.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics Section and Patient Consent
Nova Southeastern University Institutional Review Board (IRB) at (954) 262-5369 or toll free at 1-866-499-0790 or email at