
Abstract
The COVID-19 pandemic exacerbated social isolation among people with traumatic brain injury (TBI). Yet, little is known about how changes in personal factors, environmental factors, or the characteristics of activities affected social participation. We examined experiences with social isolation and barriers to social participation using the person–environment–occupation–performance model as a framework. Twelve adults with TBI participated in a series of three focus groups. Data were analyzed using thematic analysis. We identified two primary themes with sub-themes: (1) social isolation experiences: (1a) emotional impact and (1b) managing personal risk; and (2) greater barriers but a lack of strategies to address them: (2a) access and opportunities and (2b) social and societal factors. New environmental barriers and task demands affected occupational performance, and participants identified few successful strategies to overcome these barriers. Occupational therapy can develop new strategies to re-balance the person–environment fit and enhance social participation.
Plain Language Summary
People with traumatic brain injury (TBI) have experienced increased social isolation because of the COVID-19 pandemic. There has been limited research to describe how social isolation has been experienced beyond the initial pandemic lockdowns, what limits people from participating in more social activities, and how occupational therapy can help people overcome these new challenges. We interviewed 12 people with TBI to understand their experiences of social isolation using the person–environment–occupation–performance model as a framework. We found that people with TBI have continued to experience worse social isolation, which has affected their emotional well-being. They continue to worry about their risk of exposure and illness. We found that limited opportunities for social activities, inaccessibility of activities, and a lack of social support have contributed to social isolation. Occupational therapy practitioners can help people with TBI develop new strategies to overcome barriers to social participation so they may safely return to important social activities.
Introduction
During the COVID-19 pandemic, people with disabilities experienced greater social isolation than those without disabilities (Goggin & Ellis, 2020; Lund et al., 2020; Morrow et al., 2021). People with disabilities have experienced higher risk of severe COVID-19 or death and reduced access to health care, making social participation riskier than for the general population (Annaswamy et al., 2020; Sabatello et al., 2020). Furthermore, people with disabilities have experienced discrimination, unemployment, and lack of access to critical activities, services, and supports that contributed to fewer opportunities for social participation (Goggin & Ellis, 2020; Lund et al., 2020). Together, these new challenges resulted in fewer social contacts and lower social support, contributing to worsened social isolation (Goggin & Ellis, 2020; Morrow et al., 2021). There is little evidence to suggest that these new pandemic-related challenges have improved even in the later stages of the pandemic.
Among people with disabilities, people with traumatic brain injury (TBI) are particularly vulnerable to social isolation. Social isolation is prevalent after TBI and has been identified as a highly prioritized issue, both for individuals with TBI, and for the broader public health (Hammel et al., 2008; Holt-Lunstad et al., 2017). The person–environment–occupation–performance (PEOP) model (Baum et al., 2015) provides a framework for examining the factors that have contributed to social isolation among people with TBI. The PEOP model posits that personal factors (e.g., physical and cognitive function), environmental factors (e.g., physical and social environment), and characteristics of occupations can each contribute to successful performance of occupations (Baum et al., 2015). A strong fit between the person, the environment, and the occupation enables participation, while the lack of a strong fit leads to problems with participation (Baum et al., 2015). Prior to the pandemic, there was evidence to suggest that each of the PEOP model’s domains contributed to social isolation among people with TBI. Personal factors associated with TBI, including changes in cognition, communication, and social interaction skills, are associated with fewer close relationships and lower social participation (Kersel et al., 2001; Kersey et al., 2019; Milders, 2019). Environmental factors—including lack of social support, discrimination, lack of physical and cognitive accessibility of public spaces, and fewer financial resources—result in fewer opportunities for social participation, contributing to social isolation (Hammel et al., 2015). Finally, social occupations may be difficult for people with TBI, which may affect occupational performance and preclude greater social participation.
Components of the person, environment, and occupation domains continue to influence the performance of social occupations, and thereby, influence social isolation for individuals with TBI following the onset of the COVID-19 pandemic; however, the factors in each domain and the interactions among them have likely changed. Understanding changes in factors that facilitate social participation is critical to determining the most appropriate intervention approaches to support people with persistent social isolation, including people with TBI. Although some research examined the experiences of social isolation among people with TBI during the early stages of the pandemic (Bellon et al., 2023; Goverover et al., 2022; Morrow et al., 2021), little research has examined the ongoing pandemic-related challenges that people with TBI continue to face. Furthermore, little research has examined the specific barriers to greater social participation related to the pandemic or strategies to overcome persistent barriers. This gap in research leaves occupational therapy practitioners without adequate tools to address the critical, long-term problem of severe social isolation in a world of new challenges. Therefore, the purpose of this study was to examine the experiences of social isolation throughout the COVID-19 pandemic up to the time of data collection (July-October, 2022), including barriers to social participation, and possible strategies to achieve social participation goals.
Method
In this descriptive qualitative study, we conducted focus groups using a community-based participatory research approach (Israel et al., 1998; Mohatt et al., 2021). This study was conducted in collaboration with a community-based day program serving diverse people with TBI. The program provides member-driven services to enhance community living and participation, wellness, and social connection. Members are racially diverse, many of whom live in low-income households in under-resourced areas of Chicago. This program served as a community partner throughout this project to address a problem—social isolation—their members wanted to improve. This study grew from multiple conversations about rehabilitation and community participation priorities between the research team and members and staff at the community program. Two people with TBI were active members of the study team, both to support participants and to strengthen the credibility of this study through its design and analysis. These peer leaders were involved in designing the interview guide, facilitating focus groups, and interpreting results. Cognitive supports were provided to the peer leaders, including written meeting agendas and notes, frequent reminders about study objectives and methods, structured meeting times and procedures, and use of plain language. The design and reporting of this study were guided by the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Supplemental Materials).
Between July and October of 2022, two cohorts of six participants each completed a series of three 2-hr focus groups. During this timeframe, mask mandates and vaccination mandates had been lifted in the city of Chicago and many pandemic-related policies had been ended. The peer leaders with TBI and a staff member from the community program participated in the development of the question routes and helped ensure the use of plain language. Focus groups were co-facilitated by the first author and the two peer leaders. We provided accommodations to ensure cognitive accessibility (Mohatt et al., 2021), including advance provision of questions to allow participants to prepare, written questions available for participants to follow during each session, slow speaking and repetition when needed, written notes on a whiteboard in large print to annotate important discussion points, and a mid-point break to reduce cognitive fatigue.
Participants were recruited through the community-based program and were eligible if they had experienced a TBI more than 6 months prior to enrollment and spoke English. Participants were excluded if they had a severe cognitive or communication impairment limiting their ability to participate in focus groups. Staff at the community program helped us purposively recruit a sample with diverse social and cognitive needs, who would provide a broad range of experiences to enhance the transferability of findings. All participants were recruited in person at the community program and provided informed consent prior to participating in any research activities. Study activities were approved by the University of Illinois Chicago Institutional Review Board.
The first focus group session focused on defining social participation and social isolation and describing experiences engaging in social activities throughout the pandemic. The second session focused on identifying social participation goals and needs related to the achievement of goals. The third session focused on identifying barriers and supports to achieving social participation goals and strategies to manage barriers and supports.
Focus groups were audio recorded, transcribed by the first author, checked by a research assistant, and de-identified for analysis. We used ATLAS.ti 22 (Scientific Software Development GmbH, 2022) to assist with coding and data management. Using a thematic analysis approach (Braun & Clarke, 2006, 2022), two coders analyzed transcripts and identified codes that represented concepts within the data. Then, we constructed themes to describe experiences with social isolation and participation. We reviewed and refined themes iteratively to ensure that the themes accurately represented the collective experiences of the participants. Our iterative theme development process included active participation from all members of the study team, including the peer leaders, which strengthened the credibility of our findings. We maintained an audit trail of analytic memos and meeting notes to track important decisions and rationale for analytical choices to enhance dependability and confirmability. We referred back to the audit trail at critical points throughout the analysis to inform our decision-making.
The researchers involved in conducting this study and analyzing the data are all White female occupational therapists with experience in clinical and community TBI rehabilitation, as well as TBI rehabilitation research. We all share a passion for supporting community and social participation among people with disabilities and are invested in seeing this project inform community-based rehabilitation services. Furthermore, we all have an interest in understanding how a broad range of environmental factors influence participation outcomes for people with disabilities. We see the environment as an important component of the PEOP model that is often under-studied in TBI rehabilitation research, and this perspective informed our use of the PEOP model as a comprehensive framework for our analysis. All members of our team have experience in conducting qualitative research and community-based participatory research with people with TBI. The first author had an existing relationship with many members at the community program, including many of the focus group participants, built through prolonged engagement with the community program.
Results
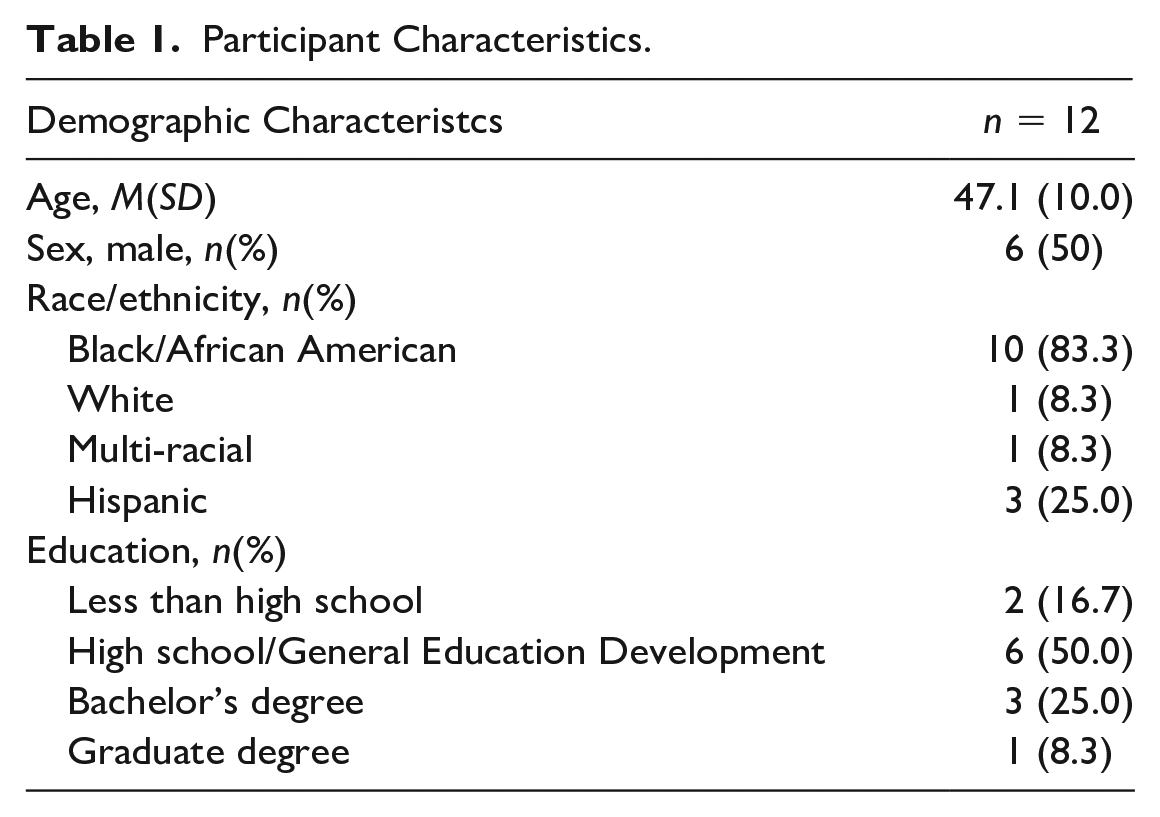
We enrolled 12 participants with chronic TBI in this study. Their characteristics are described in Table 1. Participants had an average age of 47.1 (SD = 10.0) years, were equally split between male and female, were predominantly Black or African American (83.3%), and had diverse educational backgrounds. Two participants attended only two of the three focus group sessions, while the remaining participants attended all sessions.
Participant Characteristics.
To describe participant experiences with social participation and social isolation since the start of the COVID-19 pandemic, we generated two themes: experience of social isolation and greater barriers but fewer strategies.
Theme 1: Experience of Social Isolation
Participants reported social isolation throughout the pandemic that continued to the time of the focus groups. We describe these experiences with two related sub-themes: (a) emotional impact and (b) managing personal risk.
Sub-Theme 1: Emotional Impact
Participants described feelings of loneliness at the start of the pandemic, which affected their mental health “It felt terrible . . . You couldn’t go nowhere, couldn’t do nothin.’ That was the hard part, just sittin’ in the house. You couldn’t go visit anybody cause they was sittin’ in the house, too” (ID10). They described few opportunities for socialization, worsened by a lack of access to their usual activities and environmental supports “I was going crazy. I like getting up and going out. And when it was closed, I didn’t have that option. So yeah, it was driving me nuts” (ID5). Furthermore, when they did get out and about for essential activities, mitigation plans and restrictions led to worse experiences and heightened occupational performance problems, “I had to go to the hospital by myself for my appointments. God” (ID10).
Remote socialization was identified as a lifeline to remain connected to others, but the quality of remote interactions was perceived to be worse than in-person interactions, “It’s much better in person. I mean it works when you do Zoom and things, but it’s not the same as being around someone” (ID4). Technology added a new environmental barrier that was difficult for participants to manage, and complicated the performance of previously easy and enjoyable occupations. Remote occupations represented a substantial performance change with significantly different task characteristics (finding technology, connecting to virtual services, managing remote social mechanics and dynamics) compared with usual in-person occupations. Thus, remote activities were not always pursued due to perceived complexity, nor were they always effective, for example, “I couldn’t go to school because they were doing it on Zoom. I tried to go to church on Zoom” (ID1). The challenges and lack of satisfaction related to remote social activities were insufficient to reduce the feelings of isolation participants experienced.
After the initial shutdown, participants described hesitancy returning to their usual activities, “[The] fear factor. Not wanting to be around people because you don’t know if they have [COVID] or not” (ID2). They also described lower satisfaction with social interactions because of social distancing, smaller groups participating in activities, fewer activity options, and masking and social distancing, “It was like, because it was a smaller group of people . . . and we couldn’t even sit with each other . . . we had to spread out, one here one over there” (ID6). At the community program specifically, participants reported feeling a sense of loss over long-time friends who have not returned to the program, “We had really good friends that used to come here. Well, I say really good friends, but I don’t know. How long have they been away now . . . we don’t even know if those people are alive or not alive” (ID12). Finally, participants reported that it was awkward and difficult to establish a new normal as they returned to some activities with their previous social contacts who they had not seen in a long time, “Seeing them after 2 years, it’s like ‘hi’—that awkward feeling” (ID6). Although opportunities for socialization have become more available than during initial shutdowns, participants identified a continued emotional impact and ongoing barriers to occupational performance.
Sub-Theme 2: Managing Personal Risk
Efforts to reduce personal risk not only enabled some socialization but also contributed to persistent social isolation. Participants placed a high value on masking, vaccination, and social distancing, which they felt enabled the return to some social activities safely. “Well with me, as I have four shots now, I feel much better for myself . . . It’s so important to stay up on the shots” (ID12). Some refused to interact with people who had not been vaccinated as a way of reducing their personal exposure risk, “They had to be vaccinated to come to the party. We had nobody who was not vaccinated” (ID10), which served to protect them, but also limited their options for social contact. Participants continue to actively rely on masking and expressed frustration that others have discontinued their masking practices, “I get so tired of telling people to pull their mask up. I say, I’m just going to let it be what it’s going to be. I’m going to protect myself. That’s all I can do” (ID4). Although efforts to manage personal risk were perceived as critical to protecting their safety, the lack of others’ embrace of these practices contributed to the negative emotional impact of the pandemic.
Hesitancy to return to social activities still persists. As participants have started to attempt social activities, they remain hesitant based on situations they perceived as unsafe. Participants reported an ongoing fear of exposure that continues to affect their social participation, “See I know what I been doing, I don’t know what they doing. Sitting down socializing with them, you gotta be kidding. You can’t socialize with them because you don’t know what they been doing. And they wanna get all up in your face. No, you gotta stand back” (ID10).
They report a persistent pattern of fewer social activities compared with before the pandemic “I was going to the health club like 3 or 4 times a week before, or walk in the park. I ain’t doin’ none of that now” (ID9). The prevailing perspective was that participants felt the need to think carefully about what they do and who they do it with, with a need to determine whether the risks are worth the benefit, “I need to think carefully about what I’m doing, where I’m at, who I’m around . . . I might say no to comin’ certain places, bein’ around 2 people, or any people who aren’t vaccinated yet . . . I don’t even wanna talk to em’” (ID7).
Overall, this has led to smaller social networks, fewer social activities, and lost relationships, “I deal with the ones who are important for me to deal with. The rest of em’, I just don’t deal with anymore” (ID10).
Theme 2: Greater Barriers But Fewer Strategies
Participants reported a range of barriers and supports to social participation, including many that were novel responses to the pandemic. It was notable that most of the strategies that participants identified for overcoming barriers to participation were those they had relied on prior to the pandemic; these did not adequately address new pandemic-related barriers. Barriers included new environmental barriers, loss of previously existing environmental supports, and changes to their occupations that limited their performance. The types of identified environmental barriers align with previously identified participation barriers for people with disabilities, including TBI, as reported by Hammel and colleagues prior to the onset of COVID-19: (a) economic and financial, (b) systems, services, and policies, (c) transportation, (d) physical (built and natural) environment, (e) assistive technology, (f) information and technology access, and (g) social supports and societal attitudes (Hammel et al., 2015). Both the ongoing and new challenges identified by our participants, and the strategies they identified to overcome them, are presented in Table 2. Here, we will discuss specifically those barriers that are new and resulting from the COVID-19 pandemic. We present these barriers as two sub-themes: (a) access and opportunities and (b) social and societal factors.
Environmental Barriers and Supports, Strategies.
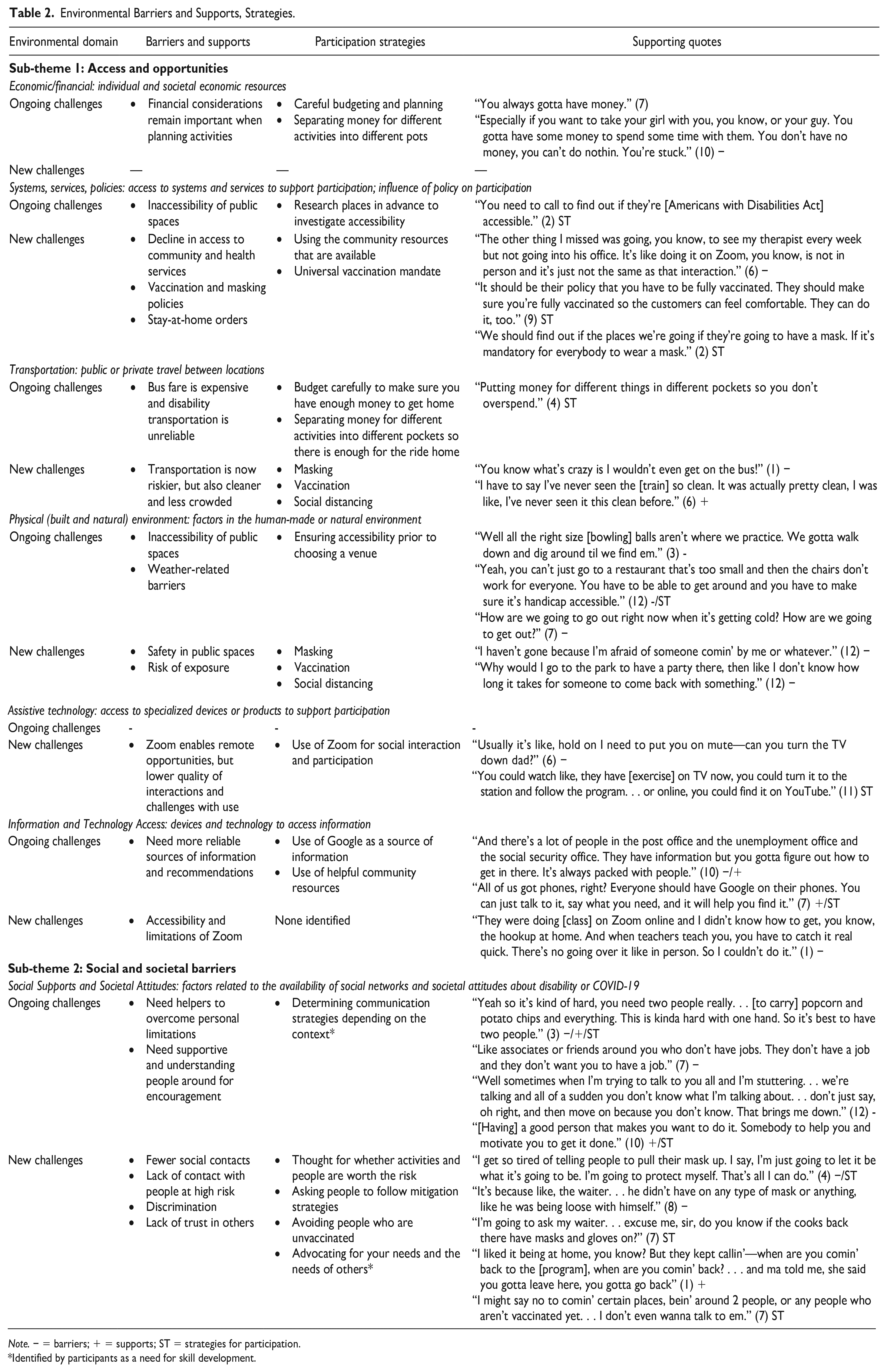
Note. − = barriers; + = supports; ST = strategies for participation.
*Identified by participants as a need for skill development.
Sub-Theme 1: Access and Opportunities
Participants reported a wide range of environmental barriers limiting their opportunities for social participation. These included:
a decline in access to community and health services that would support social participation or alleviate the effects of social isolation, “The other thing I missed was going, you know, to see my therapist every week but not going to his office. It’s like doing it on Zoom, you know, is not in person and it’s just not the same as that interaction.” (ID6)
stay-at-home and mitigation orders, and public or organizational policy that made participants feel unsafe in public places, “It should be their policy that you have to be fully vaccinated. They should make sure you’re fully vaccinated so the customers can feel comfortable. They can do it, too.” (ID9)
limited options for safe transportation to participate in social or community activities, “You know what’s crazy is I wouldn’t even get on the bus.” (ID1)
risk of exposure in public places or during social activities, “Why would I go to the park to have a party there, then like, I don’t know how long it takes for someone to come back with something.” (ID12)
inaccessibility and limitations of Zoom, “They were doing [class] on Zoom online and I didn’t know how to get, you know, the hookup at home. And when teachers teach you, you have to catch it real quick. There’s no going over it like in person. So I couldn’t do it.” (ID1)
Aside from masking, vaccination, and social distancing, participants identified few specific and effective strategies for managing these barriers. Strategies included researching masking rules in advance, “we should find out if the places we’re going to, if they’re going to have a mask, if it’s mandatory for everybody to wear a mask,” (ID2) and use of online opportunities for wellness activities, “you could watch like, they have [exercise] on the TV now, you could turn it to the station and follow the program. . . or online, you could find it on YouTube” (ID11). No strategies were identified for managing the challenges of online or remote opportunities. Furthermore, many of the identified strategies were discussed hypothetically, rather than identified as strategies that participants had implemented.
Sub-Theme 2: Social and Societal Barriers
Social support and broader societal attitudes were identified as both barriers and supports for social participation. Social support was identified as an important source of encouragement and information for participants, “I liked it being at home, you know? But they kept callin..’ . . when are you comin’ back [to the program]?. . . and ma told me, she said you gotta leave here, you gotta go back” (ID1). Still, participants suggested that they feel the need for more guidance to determine the best communication strategies to effectively use social support depending on the context of their situation.
Beyond individual social support, broader societal attitudes were among the most frequently identified barriers to participation. Frustrations with others who do not follow masking and social distancing recommendations in the community was prevalent, “It’s because like, the waiter . . . he didn’t have on any type of mask or anything, like he was being loose with himself” (ID8). Frequently, participants described a lack of trust in others to be truthful about the risk they brought to social situations, specifically their vaccination status. Participant 12 explains: “Let’s say you and I are in a room together. Neither of us have had any shots. I lie to you and say I had my shots, and you lie to me and say you had your shots. Neither of us had any shots at all,” (ID12). Reacting to this scenario, Participant 7 says, “it’s like playing Russian Roulette” (ID7). Participants identified few strategies for addressing societal barriers. Self-advocacy was occasionally identified, but participants suggested that they needed more skills to effectively advocate for their needs. Most often, the strategy to address societal barriers was to avoid others and limit activities and social contact.
Together, new environmental barriers have contributed to changes in performance of social occupations, and these occupational performance changes have contributed to the ongoing social isolation experienced by people with TBI.
Discussion
This study examined the experiences with social isolation and social participation among people with TBI since the start of the COVID-19 pandemic. We found that social isolation remains prevalent among our sample of people with chronic TBI in late 2022, even as pandemic-related policies had been relaxed and society had started to return to “normal.” Although social isolation is not a new problem for people with TBI, it is clear from this study that participants have not yet returned to their pre-pandemic levels of participation. Participants have not returned to many meaningful occupations, including school and exercise, limiting opportunities for personal advancement and health maintenance. They also continue to experience smaller social networks, fewer social activities, and reduced quality of relationships, furthering their social isolation.
Our findings support those of the few other studies examining social isolation among people with TBI during the pandemic, which also showed that social isolation was prevalent and problematic (Bellon et al., 2023; Goverover et al., 2022; Morrow et al., 2021). Our findings highlight that the experience of social isolation was not only heightened during the initial lockdowns but persisted even to a time when businesses had re-opened and masking and vaccination mandates had ended. Our study, in contrast to a study by Bellon and colleagues (2023), found that participants had not found effective strategies to overcome many of the new challenges. Bellon’s study included qualitative data from family members and care providers of people with TBI, while ours exclusively included people with TBI. It is possible that care providers identified and used their own strategies, while people with TBI did not. It is also possible that important demographic differences between the samples led to different results. Our sample was composed of people with low incomes and were predominantly from racial minority groups. It is possible that differences in environments, communities, available resources, and social and financial supports, generated differences in whether strategies were identified and effective.
Applying the PEOP model to these findings, our study suggests that this heightened level of social isolation may be tied to an increase in environmental barriers (safety concerns, limited access to information) a decrease in environmental supports (community resources, public transportation, social support), new values and priorities that affected their occupational performance, and added complexity to preferred occupations (management of technology and accessibility issues). Although many personal factors may not have changed, the changes in environmental factors and occupations appear to have affected the performance of social activities, and the reduced performance of social occupations contributed to greater social isolation. The mismatch between environmental barriers and the strategies that participants use to overcome those barriers appears to have widened during this time. Participants are facing greater environmental barriers without adequate strategies to overcome them, creating a greater imbalance in the person–environment fit and resulting in a change in occupational performance. In this study, participants were able to identify some strategies to achieve their social participation goals, but these were often out of their control (change airline policy), were unrealistic (personally monitor event attendees for vaccination status), or were identified hypothetically, rather than actively used as strategies. It was clear that participants had few effective strategies to enhance their social participation in the context of the ongoing pandemic.
Occupational therapy can play a role in addressing this new imbalance in the person–environment fit by guiding clients to develop or adapt strategies for goal achievement. Strategy training interventions have been found to enhance achievement of activity-based goals among people with acquired TBI (Dawson et al., 2013; McEwen et al., 2019; Skidmore et al., 2015). This approach focuses on iterative development and refinement of participation strategies, with guided application of strategies to specific meaningful occupations. Strategy training interventions provide the opportunity for people with TBI to develop practical, effective strategies for managing the environmental barriers related to social activities. Strategy training interventions are one tool that may contribute to improving the person–environment fit required for enhanced social participation.
Participants specifically identified two areas where they expressed a need for skill development: self-advocacy and communication skills. These skills could be leveraged to effectively use social support depending on the context. Based on these findings, rehabilitation interventions targeting social participation in the complex post-COVID environment should incorporate skill development in self-advocacy so clients can effectively ask for what they need, exert their rights, and request accommodations. Intervention may also need to focus on strategies to find, grow, and leverage social support.
Finally, Zoom was identified as an important means of safely staying connected with people and services. However, participants had low success and satisfaction with using Zoom. Clearer instructions, guidance, and support from videoconferencing platform services and internet service providers may improve accessibility and satisfaction with remote opportunities, which were generally perceived as safer. Rehabilitation intervention may also provide individualized training on the use of technology to enhance social participation. Although telehealth options have been growing rapidly since the start of the pandemic, people with TBI (in our study and others) have continued to express a preference for in-person interactions (Kringle et al., 2023; Rietdijk et al., 2022). Telehealth options offered to people with TBI must be specifically tailored to the person’s individual needs, resources, and capacity.
Limitations
All participants in this study were recruited from the same community-based program in Chicago and thus may share similar perspectives. Their perspectives were informed by their experiences in the Chicago area, which had more severe mitigation policies than some other regions. Furthermore, this study only included participants who had returned to activities at the community program. It is possible that experiences may be different among the group who have not re-connected with an important community support service and existing social network. This homogeneity of our sample limits the generalizability of our results to the broader population of people with TBI outside of this specific program and outside of Chicago.
That said, a strength of this study is the racially, educationally, and economically diverse sample. This study included participants with few resources and many barriers that may not have been identified by less diverse samples. This racially diverse sample was at a higher risk for severe COVID-19 or COVID-19-related death due to both race-based and disability-based discrimination and health inequities, which likely influenced their perspectives (Acosta et al., 2021; Johnston & Pollack, 2023). These are critical perspectives to examine, as they represent those who have the greatest risks and the most to gain from stronger community supports and rehabilitation intervention.
Conclusion
We examined experiences with social isolation among people with TBI in the late stages of the pandemic (July-October 2022) using the PEOP model as a framework. We found that people with TBI continued to experience heightened social isolation, with a detrimental emotional impact. They remained concerned about returning to social activities and continued to limit their social contacts. Furthermore, they reported greater environmental barriers to performance of social activities, including issues with access and opportunities, and social and societal barriers. These new barriers disrupted the person–environment fit, culminating in greater occupational performance problems and, thereby, greater social isolation. Participants had identified and used few strategies to effectively manage these new barriers, suggesting a need for greater occupational therapy services focused on strategy development for social participation.
Supplemental Material
sj-jpg-1-otj-10.1177_15394492241233260 – Supplemental material for Ongoing Challenges Related to the COVID-19 Pandemic Among People With Brain Injury
Supplemental material, sj-jpg-1-otj-10.1177_15394492241233260 for Ongoing Challenges Related to the COVID-19 Pandemic Among People With Brain Injury by Jessica Kersey, Amy R. McArthur and Joy Hammel in OTJR: Occupational Therapy Journal of Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved by the University of Illinois Chicago Institutional Review Board #2017-0797.
Research reported in this publication was supported by the National Institutes of Health under award number UL1 TR002003. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.