
Abstract
Illness-induced trauma (IIT) might cause a disruption in an individual’s occupational performance. To examine occupational therapy practitioners’ (OTPs) perspectives and role in addressing IIT. In this descriptive mixed-methods design, 24 OTPs completed an online survey and 10 OTPs participated in a semi-structured 1:1 interview. Survey questions asked about knowledge regarding IIT. Interviews addressed incorporation of IIT knowledge and trauma-informed care (TIC) into practice. Quantitative results showed most OTPs (64%) did not receive TIC training and believed training was inadequate. Qualitative results indicated three major themes: “Impact on Rehabilitation,” “Variety of OT Approaches for IIT,” and “Barriers to Providing Trauma-Informed Care.” Although OTPs report inconsistencies with incorporating TIC into practice, there are similarities with foundational OT skills and TIC. Findings suggest OTPs utilize a TIC approach to support clients with IIT to process and re-engage in meaningful occupations.
Plain Language Summary (PLS)
Researchers have shown that some individuals who have been hospitalized and diagnosed with a serious medical condition, also have illness-induced trauma (IIT). They developed symptoms of post-traumatic stress disorder, including mood changes, hyperarousal, and re-experiencing the event. In the criteria to be diagnosed with post-traumatic stress disorder, there are specific events that are considered traumatic and able to receive a diagnosis. IIT is not considered a traumatic event by the diagnosis criteria. Occupational therapy practitioners (OTPs) frequently work with clients who have potentially experienced IIT. This study aimed at learning about the perspective OTPs have while working with individuals who experienced IIT and their role to address this trauma. The researchers recruited 24 OTPs to complete an online survey and 10 OTPs to participate in a 1:1 interview. Survey questions asked the therapists about their knowledge of IIT. Interview questions asked how therapists incorporate knowledge about IIT and intervention strategies to support clients healing from trauma. Survey results showed the majority of OTPs did not receive formal training on ways to support clients processing trauma or believed their training was not enough when working with clients. Interview results indicated three major ideas: IIT has a negative impact on rehabilitation outcomes, there are a variety of approaches that OTPs use to support clients processing their trauma, and there are barriers to supporting clients with IIT. Even though there are inconsistencies to training and incorporating strategies, many of the foundational skills that OTPs are taught in their education align with the principles and approaches to provide supportive care and consideration of trauma. OTPs use these approaches to support clients processing their trauma from medical conditions and events and help re-engage them in meaningful activities.
Keywords
Introduction
Illness-induced trauma (IIT) is a distressing experience occurring with medical conditions and/or life-threatening illness (El-Gabalawy et al., 2018). IIT is often precipitated by: hospitalization, medical procedures, communication challenges, or reduced autonomy (Jackson et al., 2016). IIT symptoms include re-experiencing the event, avoidance, mood changes, and hyperarousal. During hospitalization, potential stressors may include pain, fear of dying, loss of control, and difficulties communicating with health care practitioners and family (Jackson et al., 2016).
Individuals experiencing IIT may be at high risk for developing post-traumatic stress disorder (PTSD). The Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR; American Psychiatric Association, 2022) acknowledges the threat of injury and death as trauma. The DSM-5 TR (2022) recognizes that a life-threatening illness or medical event could possibly be a traumatic event but is not an official PTSD criteria. It is estimated that 25% of patients with stroke, spinal cord injury, and amputation develop PTSD or clinically significant trauma-related symptoms (Edmondson et al., 2013; Kearns et al., 2019; Kunz et al., 2021).
PTSD has significant effects on performance in occupations and quality of life (QoL); for example, 40.3% of individuals with PTSD had more than one activity of daily living (ADL) impairment (Zatzick et al., 2008). Trauma and illness can disturb participation in meaningful occupations and cause maladaptive responses to occupational challenges (Lopez, 2011). Thus, symptoms associated with IIT might result in poorer outcomes in occupational performance and participation.
To our knowledge, no research has focused on occupational therapy practitioners’ (OTPs) role in identifying and managing IIT in practice. To address this gap in knowledge, the purpose of this study is to better understand occupational therapists’ perspectives on IIT and to describe their role in identifying and managing IIT during therapeutic encounters.
Methods
Study Design
A descriptive mixed methods design was used to collect quantitative data about IIT knowledge and qualitative data to understand OTPs role in addressing IIT. We utilized the qualitative data to explain the quantitative results (Creswell & Plano Clark, 2018). During the quantitative phase, 24 OTPs participated in an online survey to collect information about the participants’ knowledge and perspectives on IIT. Ten OTPs who completed the survey also participated in a 1:1 semi-structured interview to explore their role when working with clients with IIT. Both quantitative and qualitative data were collected to provide a rich insight into the research questions rather than obtaining each type of data separately (Creswell & Plano Clark, 2018). Quantitative and qualitative data were integrated throughout the discussion section. The study was approved by the Colorado State University Institutional Review Board.
Conceptual Framework
This study incorporated both an inductive and deductive approach guided by the Occupational Therapy Practice Framework (OTFP) and trauma-informed care (TIC) principles. Our study focused on OTPs perceptions; the OTPF uses language at an individual level and incorporates person factors, environment factors, and occupational participation. TIC principles were used to incorporate the standard approaches to support clients healing from trauma. The TIC six-core principles include (a) safety; (b) trustworthiness and transparency; (c) peer support and mutual self-help; (d) collaboration and mutuality; (e) empowerment, voice, and choice; and (f) cultural, historical, and gender issues (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014).
Participants
We purposively sampled OTPs for the online survey by recruiting through internet postings to occupational therapy websites, and we reached out to OTPs who had interest in trauma or who worked in settings where trauma may be common (i.e., acute or inpatient rehabilitation). Survey participants were asked about their interest in completing a 1:1 interview and were then contacted for interviews. For the 1:1 interview, we also recruited participants using snowball sampling to reach data saturation (Creswell & Plano Clark, 2018). Thus, not all interview participants completed the survey.
Participants were included if they met the inclusion criteria: be a licensed occupational therapist with at least 6 months of clinical experience working with clients who had sudden onset of disability or injury, including but not limited to stroke, spinal cord injury, brain injury, burns, amputations, intensive care unit stay, or other traumatic injury. All participants provided consent at the beginning of the survey and before the interviews. Data from the surveys and interviews were not linked.
Data Collection
Quantitative Data
The survey (Supplemental File 1) for the study was completed using Qualtrics and took approximately 10 to 15 minutes to complete. The survey included 11 demographic questions. We then provided a definition of “illness-induced trauma” and included 18 questions based on three content areas: (a) participants knowledge of IIT, (b) their perspectives on psychological trauma’s impact on rehabilitation, and (c) incorporation of TIC in therapeutic encounters. Content-based questions about IIT were answered using a 5-point Likert-type scale of either frequency (Never, Rarely, Sometime, Often, Always) or agreement (Strongly disagree, Disagree, Neutral, Agree, Strongly Agree). The 18 questions were developed through a literature review and peer discussions. The survey was pilot tested with an occupational therapist and two occupational therapy students and adjustments were made based on feedback.
Qualitative Data
A semi-structured interview guide was generated to ask questions addressing OTPs perceptions related to their: experiences when treating clients with IIT, the impact IIT has on the rehabilitation process, and intervention strategies utilized when working with clients experiencing IIT (Supplemental File 2). Additional questions were asked about the OTP’s practice setting, personal and professional perceptions of IIT, and how they incorporate TIC into their practice. One author (C.N.B.) conducted 10 semi-structured interviews. Interviews times ranged from 35 to 55 minutes, were conducted virtually on a secure platform, audio-recorded, and transcribed verbatim. Data collection ended when code saturation was reached. Code saturation was determined when no new codes were generated (Hennink et al., 2017).
Data Analyses
Quantitative Data Analysis
Survey data were exported from Qualtrics to Dedoose software for analysis (Dedoose Version 9.0.17, 2021). Descriptive statistics were used to examine data from the survey, including demographics, OTPs’ perceptions of TIC, PTSD, and IIT, and whether therapists considered trauma in treatment sessions.
Qualitative Data Analysis
Interview transcripts were de-identified, reviewed for accuracy, and uploaded to Dedoose. Data were analyzed using thematic analysis, an inductive approach, and framework analysis, a deductive approach (Colorafi & Evans, 2016; Hsieh & Shannon, 2016). First, two analysts (C.N.B. and C.M.H.) read each transcript at least 3 times. Second, the research team selected three of the transcripts that provided perspectives from different practice settings and included a variety of IIT approaches to generate a preliminary codebook. Independently the two analysts used a holistic, in vivo approach; where codes were derived using the participants’ words (Saldana, 2016). A holistic approach is when one paragraph can be coded to two separate ideas, also known as code co-occurrences (Saldana, 2016). Then, the analysts met to discuss the codes and discrepancies were resolved through conversation. Codes from the first three transcripts were defined and described in the preliminary codebook. The remaining transcripts were coded using these existing codes while remaining open for the possibility of generating new codes. Once all transcripts were coded, the final codebook was refined.
Codes in the final codebook were organized into categories. Because the research team was comprised of authors with a background in occupational therapy, the two analysts generated categories that were related to content from the OTPF and TIC principles. Codes and categories were inextricably linked to the data. Through an iterative process of analyzing the data, writing memos, and discussing the coding process during weekly team meetings, we generated themes and subthemes by combining more than one category. We reorganized the codebook using the categories and themes and appraised our analytic process by engaging in constant comparison analysis of the themes (Glaser, 1965). The constant comparison approach was also used to understand how code co-occurrences reflected the OTPF relation to the six TIC principles. Subthemes and themes are presented in the results, along with supporting quotes.
Reflexivity and Trustworthiness
The authors are aware that their knowledge on TIC, PTSD, IIT, and training in occupational therapy (including the OTPF model) are reflected in the codes. The authors were reflexive and met with the research team to discuss codes and themes. The two analysts wrote memos when collecting and analyzing data to bring awareness to their assumptions and feelings. To ensure trustworthiness of the data, member checking occurred through follow-up with participants to confirm data findings and an additional author not involved with study participants (JW) peer-reviewed the codes and themes (Shenton, 2004). The authors acknowledge the sample and research team being all-White and majority female impacts generalization. Even though our sample reflects the occupational therapy profession, it does not reflect the diversity of the national demographic (American Occupational Therapy Association [AOTA], 2021).
Integration of Mixed Methods
We integrated the qualitative and quantitative strands in the discussion section below to highlight how the qualitative results helped explain our quantitative findings.
Results
Participants
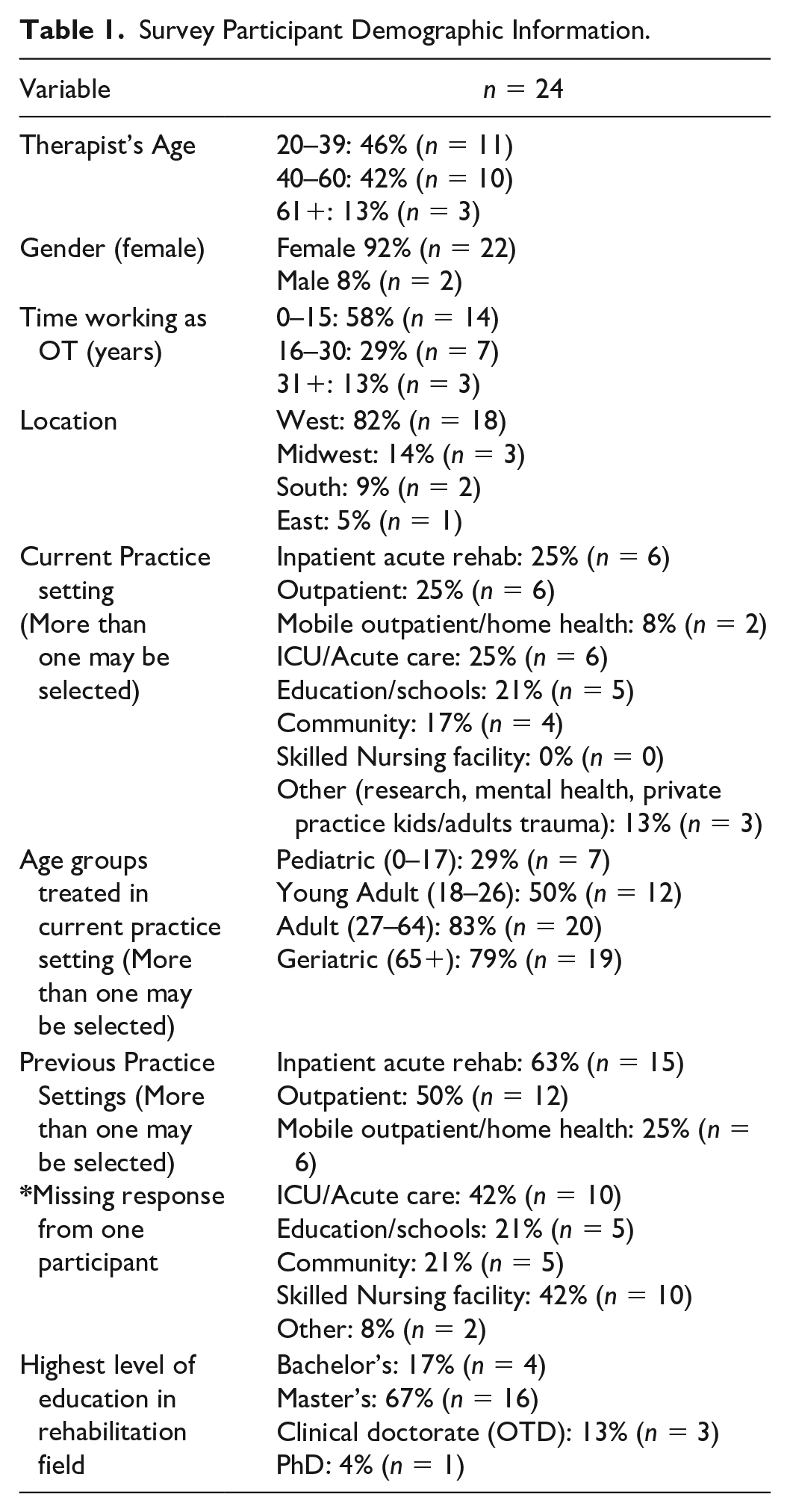
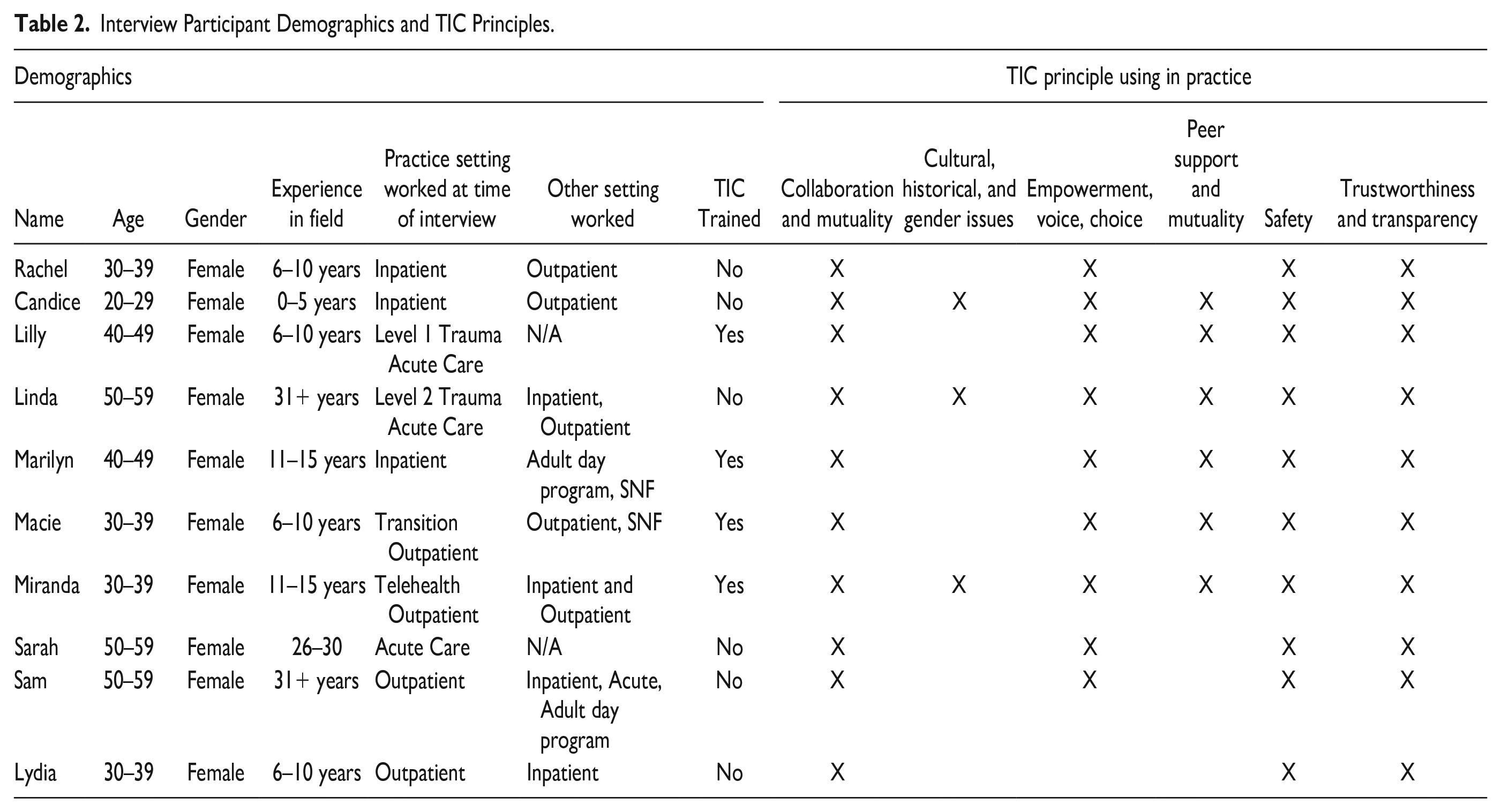
Most of the 24 survey participants (n = 22, 92%) were female; all were White and living in the United States (Table 1). OTPs practiced in a variety of settings, most commonly in inpatient acute inpatient rehabilitation (n = 6, 25%), outpatient rehabilitation (n = 6, 25%), and ICU/acute care (n = 6, 25%). All ten interviewees were female, white, and living in the United States (Table 2).
Survey Participant Demographic Information.
Interview Participant Demographics and TIC Principles.
Quantitative Results
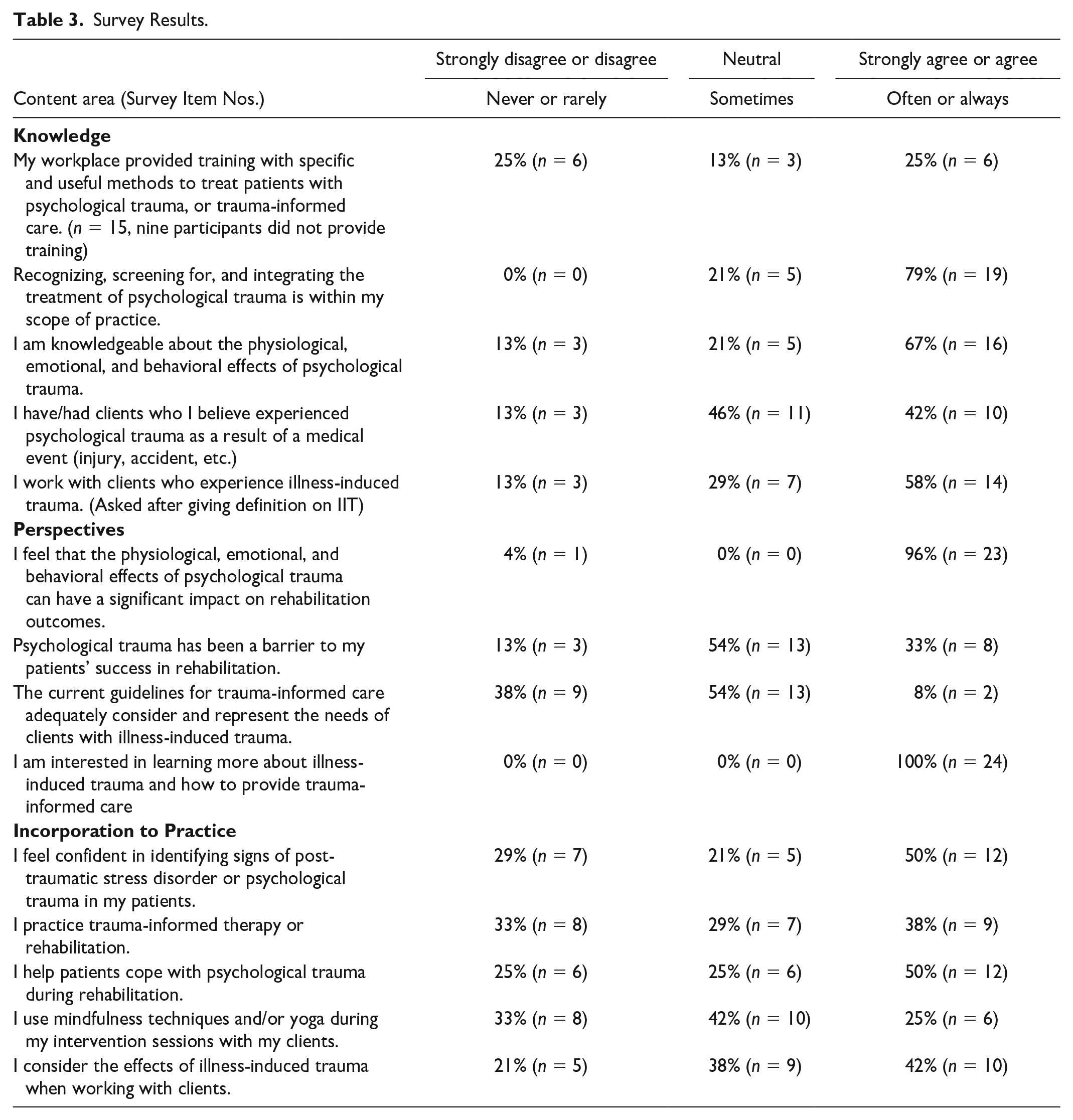
When asked if OTPs received formal training on best practice methods for treating patients with psychological trauma, 67% of participants (n = 16) reported no, 25% (n = 6) reported yes, and 8% (n = 2) were not sure (Table 3). The six OTPs who received TIC training were educated through their employer or continuing education courses, and training was not specific to OTPs. Survey results indicated that 96% of OTPs (n = 23) agreed or strongly agreed that effects of psychological trauma can have a significant impact on rehabilitation outcomes. In addition, 92% of participants (n = 22) were neutral, disagreed, or strongly disagreed when asked if the current guidelines for TIC adequately considered and represented the needs of clients with IIT. All OTPs agreed or strongly agreed when asked if they were interested in learning more about IIT and how to provide TIC.
Survey Results.
Qualitative Results
Three themes reflecting OTPs’ perspectives and role for addressing IIT were generated from the data, including 1) “IIT’s Impact on Rehabilitation,” 2) “Variety of Occupational Therapy Approaches for IIT,” and 3) “Barriers to Providing TIC for Clients with IIT.” Two subthemes were generated from the second theme: “Alignment of Occupational Therapy Approaches and TIC Principles” and “Approaches are Dependent of Therapist Factors” (Supplemental File 4).
Illness-Induced Trauma’s Impact on Rehabilitation
OTPs indicated that the trauma response associated with the event causing the illness/disability/medical event can have negative consequences on the client’s rehabilitation and healing progress. Most participants (n = 9, 90%) stated that they perceived their clients to be experiencing trauma from a medical event. There were 48-code co-occurrences between “trajectory of healing” and “trauma response,” indicating that aspects of healing could also be traumatic. OTPs noticed symptoms caused by trauma that occurred during their clinical sessions stating that “the first thing that we see is . . . anxiety and they don’t want to work with therapy because they’re afraid that they’re going to get even more hurt” (Linda).
Throughout the rehabilitation progress, many participants attempted to balance addressing trauma and reaching therapy goals to enhance occupational performance and participation. Macie discussed working with a client struggling with mental health because of the fear associated with a new stroke diagnosis; this resulted in limited carryover to home and family support: Having to kind of say . . . I need you (patient) to stop, we need to get something accomplished in therapy today . . . We really tried to use consistency with her, giving her time where she could be heard and validated by us, but also . . . give her something to focus so that she can get her mind off the same topics . . . she was one where her anxiety and then the trauma she’s experiencing after the stroke really were some of her biggest barriers for recovery . . . (Macie)
Participants mention how almost all their patients experience some trauma due to their hospitalization or medical event, stating “we don’t have a lot of patients that are formally diagnosed with PTSD. However . . . the majority of them have symptoms or experiences from their injury that are impacting their ability to complete rehab” (Miranda).
Variety of Occupational Therapy Approaches for Illness-Induced Trauma
When OTPs recognized their clients might be experiencing IIT in their sessions, they changed their approach to address their clients’ needs and potential trauma response. Participants reported using a variety of approaches while working with clients experiencing IIT (Table 4). In occupational therapy, building rapport establishes trusting therapeutic relationships to support the client’s ability to perform meaningful occupations (Schell & Gillen, 2018). The approach of “building rapport” was broken down into communication, supportive environment, and client-centered. Every participant reported using the following approaches: building rapport through communication, building rapport through supportive environment, and building rapport through client-centeredness.
Interview Participant Approaches Used to Manage Illness-Induced Trauma (n = 10).
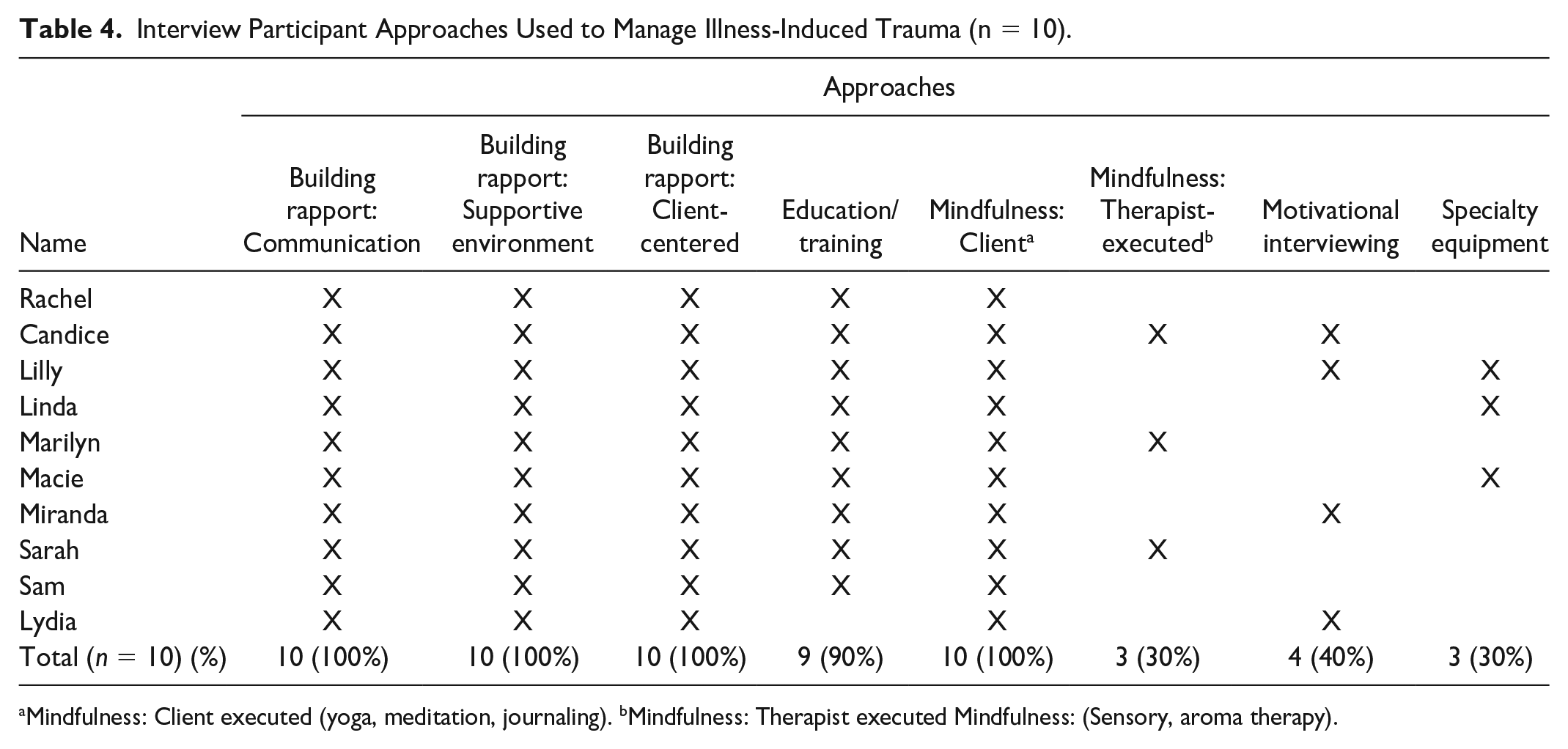
Mindfulness: Client executed (yoga, meditation, journaling). bMindfulness: Therapist executed Mindfulness: (Sensory, aroma therapy).
Communication consisted of participants discussing the following: speaking openly, shifting tone, asking questions, and recognizing potential. Participants described how they used communication strategies with their clients, for example: I will tell them everything that I know, and why I’m doing the things that I’m doing, to give them a sense of understanding . . . I try to put them in the driver’s seat as much as possible. (Lilly)
Here, Lilly incorporated clear communication to establish transparency, trust, and safety with her client because she explained what she was doing and why she was doing it. In addition, Lilly provided opportunities for her client to lead her own session, giving the client agency and autonomy, supporting TIC. These principles OTPs include in practice can elicit a supportive environment, which includes making space, trust, safety, and being present. Participants emphasized the importance of providing a supportive environment stating, to “create a safe space . . . It’s not just physical safety, that’s a mentally do they feel safe emotionally” (Miranda).
Therapists discussed being client-centered, including having clients lead sessions, meeting clients where they are, collaboration, client’s goals, and addressing the whole person. Participants explained how they considered the entire person: I think mostly trying to treat the whole person and pay attention to what is really important to them . . . what are the resources we have available to give them are? (Sam)
A variety of mindfulness strategies were used by every therapist. OTPs described using mindfulness strategies, which focus on the ability to brings one’s attention and awareness to the present-moment (Hardison & Roll, 2016). Mindfulness strategies are used in therapy to support clients in managing stress, pain, and anxiety to target QoL, health, and wellness outcomes (Hardison & Roll, 2016). Mindfulness was divided into: client-executed and therapist-executed. Client-executed mindfulness strategies are activities the client’s themselves initiated and actively participated in, such as meditation, yoga, journaling, deep breathing, and relaxation/calming techniques. A participant described their use of client-executed mindfulness strategies in treatment sessions: . . . the typical ways in yoga, feel your feet on the ground . . . all these things that are grounding . . . I just tried to reframe, and say, what in your body . . . is in control right now . . . drawing your attention to that. (Candice)
Participants also discussed using passive mindfulness strategies (i.e., aroma therapy), motivational interviewing, specialty equipment such as virtual reality and electrical muscle stimulation.
In addition, most interviewed OTPs (90%, n = 9) described education/training as an approach. Topics within education/training participants included the following: medical condition/diagnosis, recovery process, training on calming strategies and technology, benefits of rehabilitation, support groups, and recovery windows.
Alignment of Occupational Therapy Approaches and Trauma-Informed Care Principles
As OTPs reported approaches used within their practice, many of their rationales naturally incorporated OTPF and TIC principles. Specifically, the OTP skill of building rapport and the six TIC principles had 148 code co-occurrences. All ten participants discussed client-interactions regarding environment, performance, and participation that aligned with the TIC principles of collaboration, safety, and trustworthiness in their practice. Participants referred to client-centered and whole person approaches when addressing trauma: I think you have to address the whole person and what is either keeping them from progressing based on their injury or illness or the traumas that they’ve been through and what is helping them to have hope and work through it and be able to achieve their highest level of function. (Sam)
OTPs often grade activities to provide the “just right challenge” to build skills while still being manageable to perform. When OTPs noticed a trauma response, they adjusted the occupation or activity for their clients to feel supported to processes their emotions while still addressing therapy goals: I’m going to slowly start to incorporate those things that might trigger some PTSD, in a gentle, protected way. Once I’ve gained trust, I’ll start to add some of those things in knowing that those skills of losing your balance or being in an atmosphere where there’s a lot of noise, are necessary to being successful out in the community. (Lydia)
Approaches Are Dependent on Therapist Factors
Although all participants provided TIC with patients experiencing IIT, approaches selected for the client depended on therapist factors such as personal and professional experiences, clients, and practice setting. Some participants discussed how their personal experiences with trauma impacted how they treated their clients: I personally like having an interest in illness-induced trauma now because of my stroke . . . . I had this really bad headache in March, and the thought is that the stroke was kind of coming from that . . . as a result, a headache is never going to be the same for me. (Rachel)
With Rachel’s personal experience with stroke and IIT, she knows firsthand the psychological and rehabilitation impacts IIT can have on an individual and recovery. Her experience gave her a new perspective on IIT and the ability to connect and relate to clients about trauma responses they are experiencing throughout the rehabilitation process.
Participants discussed how their knowledge of diversity, equity, and inclusion (DEI), impacts relationships with clients and trust to engage in meaningful occupations: One of my patients came from a Muslim background, and the nurse nursing staff was saying that she’s refusing to do a bowel program . . . she wasn’t trying to be non-compliant . . . with that patient being so aware of the dynamic . . . she was much more comfortable with talking to me . . . She was not sharing that with a male nurse . . . I had specifically asked her at one point there was a holiday was coming up. I told her . . . what you shared with me that you’re Muslim, this holiday is coming up, would you like to celebrate it or is there something I can do . . . she said, yes and I want to be able to do my prayers. Her schedule had been so packed, she hadn’t been able to do her prayers. That opened a whole occupation we needed to work on with needing to be clean before your prayers . . . but also illuminated that’s why she had been late to all those sessions and not taking medication (Miranda).
Miranda was able to build a positive relationship with her client by learning more about her culture, personal factors, and values. By Miranda being accepting and acknowledging diversity, it gave her client the space and ability to engage in meaningful occupations while hospitalized.
Participants who worked in specific practice settings witnessed their clients with IIT in different stages of processing their trauma. Acute OTs focused on the initial reactions to a medical event and preventive measures to reduce traumatic symptoms early in their healing: We had her (client) look at her limb, and touch her limb, and start to move her limb a little bit just to kind of get a sense of what her body looks like in this moment because that’s something that’s also can be pretty traumatic. She hadn’t looked at it yet . . . a grieving process, that she’s still very much in denial until you look at it. (Lilly)
Inpatient OTs described their approach toward addressing how clients with IIT were processing their diagnosis and changes: When we see patients on the inpatient side . . . the biggest thing that they’re experiencing is that change . . . I’ve never put pants on for the first time, without being able to move my legs, or my hands, everything is new. (Candice)
Outpatient OTs addressed the potential re-traumatization that may occur with clients when they initially change environments, such as when returning home after their medical event: There have been many occasions where when somebody comes for their very first day with us for eval day, they may have a break down moment where they’re in tears, or they’re so frustrated, because . . . when they get home, it’s not a hospital environment. There’s not 24-hour nursing care, there is not the fully accessible bathroom. Maybe your equipment didn’t arrive on time . . . suddenly they’re having to face the reality that they aren’t the same person who had previously been in that environment. (Macie)
Barriers to Providing Trauma-Informed Care for Clients With Illness-Induced Trauma
Participants stated a variety of barriers to providing TIC and support for their clients who experience IIT. Barriers mentioned include hospital and medical model discrepancies, therapist emotional burn out, lack of formal TIC education, and need common language for IIT. Participants expressed the need for common education and language for IIT: Not having a shared language around it (IIT) would be one of the first or biggest barriers. As practitioners, we don’t have the same language for it, and how to recognize it and how to treat it . . . I will say we don’t talk about illness-induced trauma, that’s not a phrase that you hear. I think we talk about it. But it’s not part of a checklist or anything. (Rachel)
In addition, participants discussed how their practice settings and burn out could lead to potential barriers: Our productivity expectations have gone up quite a bit, where in a 10-hour day, I’m meant to see 10 patients . . . If I’m over here typing on the computer, rather than sitting next to you as I’m asking questions, that’s a difference in the way that I’m attempting to connect with you and give space to you and your feelings . . . You have to be introspective to figure out how much time do I have? Is this the best way to serve all of my patients? Am I keeping myself protected as well? (Lilly)
Lilly indicated that increased productivity standards affects her ability to make more meaningful connections with her clients, making it more difficult to establish safety and trustworthiness. While providing TIC, Lilly was challenged with balancing her intrinsic drive to support her clients through trauma and the burn out associated with taking on her client’s trauma.
Discussion
Currently, to the best of our knowledge, no other study has examined OTP’s perspectives on IIT and how therapists address IIT during interventions. Our findings highlight the variety of approaches OTP’s use when interacting with clients who experience symptoms of IIT, the impact of IIT on rehabilitation outcomes, and barriers within the health care system that limit OTP’s ability to practice TIC. Data integration between current evidence, quantitative results, and qualitative results connected the data as mixed findings. Mixed findings included the following: similarities in OTP skills and TIC principles, difficulties identifying and addressing trauma symptoms with IIT, OTPs potential to support healing from IIT, and need to incorporate DEI into TIC and addressing IIT (Figure 1).
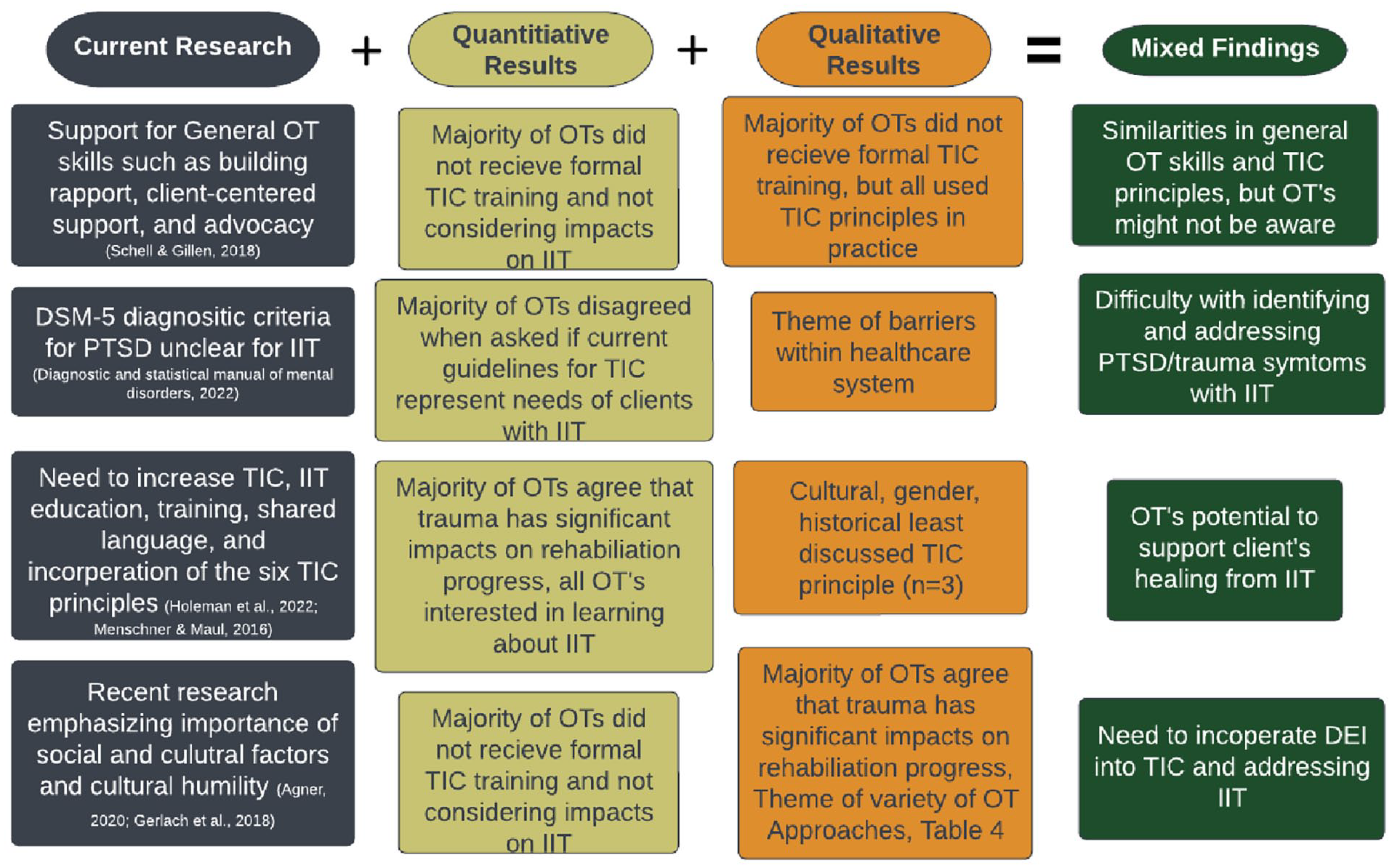
Mixed Findings Overview.
The data indicates a majority of OTPs did not receive formal training about the six TIC principles. However, the 10 interviewees described using TIC principles in treatment sessions. The inclusion of TIC principles might be due to general OTP skills, such as building rapport, client-centered approach, advocacy, and identifying personal and environmental factors (Schell & Gillen, 2018). OTP foundational skills and knowledge may lead OTP’s to naturally incorporate TIC principles into practice. However, as most survey participants did not report considering impacts of IIT or use of TIC, there is likely a need for additional education.
A majority of the survey participants disagreed when asked if current guidelines for TIC adequately consider and represent the needs of client’s with IIT. The DSM-5’s lack of clarity in defining which medical events and illness qualify as trauma might cause difficulty in identifying IIT as an event that could develop into PTSD. Being able to recognize trauma symptoms and providing early interventions such as TIC in an individual’s recovery decreases post-traumatic symptoms and PTSD severity (Kerbage et al., 2022; Oosterbaan et al., 2019). Perhaps embedding TIC into all therapy could minimize the negative impact of trauma on recovery.
OTPs who work with clients with IIT have the potential to play an integral role in supporting patients’ healing from trauma. Holman and colleagues (2022) found that 54% of OTPs identified TIC as applicable and important for their practice, and 44% either disagreed or strongly disagreed when asked whether TIC was adequately implemented into practice (Holman et al., 2022). The research findings indicate a lack of knowledge and practice with TIC. The researchers call for increased education and advocacy to ameliorate the gap of incorporation of TIC in current practice and to support best practice and holistic foundation of occupational therapy (Holman et al., 2022). In this study, most survey participants, and all interview participants, agreed that trauma can have significant impacts on rehabilitation progress and participants were interested in learning more about IIT. Increasing the awareness of IIT with a comprehensive and overarching program, including shared language, education, and training, could provide opportunities for OTPs to understand the alignment between the OTPF, ethics of care, and TIC. OTPs could incorporate knowledge on IIT into practice and could provide the support for clients to heal from IIT (Menschner & Maul, 2016).
The National Council for Behavioral Health (2017) established the “Trauma-Informed Primary Care: Fostering Resilience and Recovery” initiative which is pilot program intended to support primary care settings to best provide TIC (National Council for Behavioral Health, 2017). OTPs may benefit from this initiative to better incorporate TIC principles into OTP practice based on the client’s specific needs and strengths. OTPs indicate their approaches can be integrated into practice with additional training and are important to use with all clients.
From the 10 interview participants, three OTPs mentioned addressing cultural, historical, and gender issues, which was the least used TIC principle incorporated into practice. This could be potentially due to westernized society’s strong value of individualism. Recently, researchers have emphasized the importance of considering the social and cultural factors of the client and cultural humility (Gerlach et al., 2018). Cultural humility focuses on the learning-orientated approach when working with people with diverse backgrounds and consists of being self-aware, self-reflective, and fostering supportive interactions (Agner, 2020). Recent literature emphasizes addressing diversity, OTPs might not be educated on the importance of considering how different backgrounds or environments impact persons and occupational performance and their ability to process trauma. Although there is more research regarding DEI in the occupational therapy profession, OTPs might be unsure on how to translate their DEI education into their clinical practice (Hill, 2022).
In meeting with new clients, it is important for OTPs to assess their health and social background to understand their exposure to interpersonal and institutional trauma. Details about past interpersonal violence, abuse or silencing by health care systems, or being a member of a community that has experienced unethical medical treatment are essential in understanding the potential for medical mistrust. Through gathering education about the impact of historical medical trauma and health discriminatory practices OTPs can develop a healing-centered approach (Ragavan et al., 2023) and participate in preparatory empathy. Exploration of the unethical delivery of medical treatment could include learning about those who were enslaved, indigenous peoples, and those from historically marginalized communities. Some examples include the sterilization of Black and Indigenous women (Shreffler et al., 2015) and the erasure of human rights of sexual and gender minorities (Spurlin, 2023) in health care systems.
Limitations to this study include the small sample size, a larger sample size will increase the validity of the study. Interview participants volunteered to be a part of the study, indicating that the participants might have had a stronger interest in TIC and IIT than typical OTP population. Future researchers could focus more on how specific OTP practice settings address IIT or use of TIC. Interviews revealed approaches may differ by setting or time since injury. The all white, female sample and research team is a limitation to our study. Even with our qualitative reflexibility, this limitation may have influenced our analyses and may limit the generalizability of our data. Future studies could consider samples with more diversity (i.e., more variety of demographics, individuals with lived experiences with IIT). Learning more about IIT and TIC in specific settings may provide better insight in addressing trauma based on where a client is with processing their trauma. This study described approaches that OTPs have used in their practice, and further case studies and longitudinal studies could further evaluate the impact of IIT on clients and more specifically on how OTPs use approaches in practice. Learning about the different approaches that potentially reduce traumatic symptoms could provide OTPs more knowledge and guidance on how to incorporate TIC into their practice.
Conclusion
This mixed methods study explored occupational therapy practitioners’ roles and perspectives when addressing IIT in treatment. Findings suggest that OTPs use a variety of approaches to address IIT, trauma could negatively affect rehabilitation progress, and health care barriers could limit TIC with clients. OTPs have a unique perspective with addressing trauma and its relation to rehabilitation progress. OTP’s ability to approach IIT with TIC could significantly impact the client’s perceived support system and ability to process and heal after a traumatic medical event.
Supplemental Material
sj-docx-1-otj-10.1177_15394492241247735 – Supplemental material for Occupational Therapists’ Perspectives and Role With Illness-Induced Trauma From Medical Conditions
Supplemental material, sj-docx-1-otj-10.1177_15394492241247735 for Occupational Therapists’ Perspectives and Role With Illness-Induced Trauma From Medical Conditions by Camryn N. Beyers, Jennifer A. Weaver, Carly M. Huyber, Jennifer Currin-McCulloch and Arlene A. Schmid in OTJR: Occupational Therapy Journal of Research
Supplemental Material
sj-jpg-2-otj-10.1177_15394492241247735 – Supplemental material for Occupational Therapists’ Perspectives and Role With Illness-Induced Trauma From Medical Conditions
Supplemental material, sj-jpg-2-otj-10.1177_15394492241247735 for Occupational Therapists’ Perspectives and Role With Illness-Induced Trauma From Medical Conditions by Camryn N. Beyers, Jennifer A. Weaver, Carly M. Huyber, Jennifer Currin-McCulloch and Arlene A. Schmid in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
Extending a huge thank you to all the occupational therapy practitioners who shared their experiences and participated in this research. Thank you to Allegra McComb, who assisted with the survey and interview question development. In addition, thank you to all friends and family who supported throughout the research process. This research was accepted for AOTA INSPIRE 2024 and will be presented at this future conference.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics
All participants gave consent to be in the study and this study was approved by the Institutional Review Board at Colorado State University (3323).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.