
Abstract
Adequate sleep tailored to children’s age is important for their well-being. This study aimed to examine the association between adequate sleep and children’s participation in occupational areas. This study was a retrospective cross-sectional analysis of secondary data obtained from the 2020 National Survey of Children’s Health in the United States. This study included 6,818 children aged 6 to 11 years. The mean age was 8.48 years (standard deviation = 1.72). Multivariate regression models revealed that adequate sleep was significantly associated with increased participation in occupational areas (17% more in leisure, 95% confidence interval [CI]: 1.11–1.23; 15% more in play, 95% CI: 1.07–1.22; 11% more in education, 95% CI: 1.01–1.22) in school-age children, but not with participation in work and social participation. Adequate sleep is associated with increased participation of school-age children in occupational areas.
Plain Language Summary
Occupation refers to an individual’s activities of daily living and all activities in which children participate. Occupational areas are divisions encompassing various activities in which children participate, such as leisure, play, education, social participation, or work. In this study, we analyzed the association between adequate sleep (age-appropriate sleep duration) and participation in various occupational areas among school-age children between 6 and 11 years old. Data from the 2020 National Survey of Children’s Health were analyzed. Adequate sleep in children was associated with increased participation in leisure, play, and education. Encouraging children’s participation in activities within occupational areas is associated to adequate sleep.
Introduction
Occupational therapy primarily focuses on sleep to enhance rest and recuperation, enabling individuals to actively participate in meaningful occupations and activities (Ho & Siu, 2018; Howell & Pierce, 2000). Occupational areas have been reported to be associated with children’s sleep (American Occupational Therapy Association [AOTA], 2020; Case-Smith & O’Brien, 2014). Sleep has been reported as an associated factor with children’s activities of daily living (ADLs) and instrumental activities of daily living (IADLs; Desjardins, 2015; Rosenberg et al., 2019), health management (Fadzil, 2021; Waters et al., 2013), education (Paavonen et al., 2010; Ribeiro & Stickgold, 2014), work (Knutson & Lauderdale, 2009; Sadeh, 2007), play (Jacquier et al., 2020; Lin et al., 2018), leisure (Dalene et al., 2018; Sexton-Radek, 2013), and social participation (Hoedlmoser et al., 2010).
In children, adequate sleep (i.e., age-appropriate sleep duration) enables balanced participation in various occupational areas and enhances their overall well-being (Backman, 2004; Chaput et al., 2018; Ho & Siu, 2018). However, sleep difficulties in children have a negative impact on their overall well-being, deteriorating their quality of life, and leading to physical or psychological issues (Mindell & Owens, 2015). Factors influencing of children’s sleep include sleep behaviors, sleep satisfaction, sleep alertness, sleep timing, sleep efficiency, and sleep duration (Meltzer & Montgomery-Downs, 2011). Inadequate sleep duration can lead to imbalances in occupational performance (Backman, 2004; Fadzil, 2021; Ho & Siu, 2018).
Sleep difficulties have detrimental effects on various aspects of human functioning, including attention, emotional control, cognitive function, task performance, perceptual function, working memory, communication, and learning (Accardo, 2018; Durmer & Dinges, 2005; Meltzer & Mindell, 2006; Wiseman-Hakes et al., 2009). Furthermore, sleep difficulties in school-age children are associated with various health issues, such as hypertension, injuries, obesity, and depression (Child and Adolescent Health Measurement Initiative [CAHMI], 2022). Moreover, the sleep quality of a child has been reported to be interconnected with that of their family (Meltzer & Montgomery-Downs, 2011). Although many studies have emphasized the significance of children’s sleep, there is limited research on its relationship with participation in occupational areas.
Occupational therapists help achieve adequate sleep by providing interventions or assisting clients in managing their participation in various occupational areas (Case-Smith & O’Brien, 2014; Tester & Foss, 2018; Wagman et al., 2012). Although approximately 90% of occupational therapists acknowledge the significance of addressing sleep-related issues in occupational areas, only 30% of them actively incorporate sleep interventions into their practice (Ludwig et al., 2022). Lack of sleep education has been found to contribute to the absence of evaluation or intervention for sleep-related issues (Ludwig et al., 2022). Therefore, the need for establishing evidence-based interventions to ensure adequate sleep delivered by occupational therapists is increasing (Faulkner, 2022; Ludwig et al., 2022; Tester & Foss, 2018). This study aimed to analyze the association between adequate sleep and participation in occupational areas in a large sample of school-age children.
Methods
This study was a retrospective cross-sectional analysis of secondary data. The study protocol was reviewed and approved by the Yonsei University institutional review board (IRB). This study received IRB exemption approval.
Data and Sample
This study used the most recent wave of the 2020 National Survey of Children’s Health (NSCH), a comprehensive nationwide survey designed to assess various aspects of children’s health in the United States. Data were collected with the support of the Health Resources and Services Administration’s Maternal and Child Health Bureau. The NSCH collects information on physical and mental health, schools, social environments, caregiver health, and families (CAHMI, 2022). The 2020 NSCH data were collected from June 2020 to January 2021 using different methods: online (web instrument), on paper (paper-and-pencil interviewing screener instrument), or over the phone (telephone questionnaire assistance). One of the parents or other caregivers with a comprehensive understanding of their child’s health status was requested to complete the questionnaires (U.S. Census Bureau, 2021). During the sampling process, 240,000 addresses of children in the United States were initially selected. Subsequently, one child from each household belonging to these addresses was included in the study sample through subsampling (U.S. Census Bureau, 2023). Information on the NSCH and its associated data can be accessed through the official NSCH website, available at http://www.childhealthdata.org.
Data on 42,777 children originally included in the 2020 NSCH dataset were analyzed. The inclusion criteria included (a) children without any diseases or disabilities, (b) those aged between 6 and 11 years, and (c) observations without any missing values in the study variables. The exclusion criterion was the presence of missing values. Figure 1 shows the process of selecting the study sample. Finally, 6,818 children were included in the analysis.
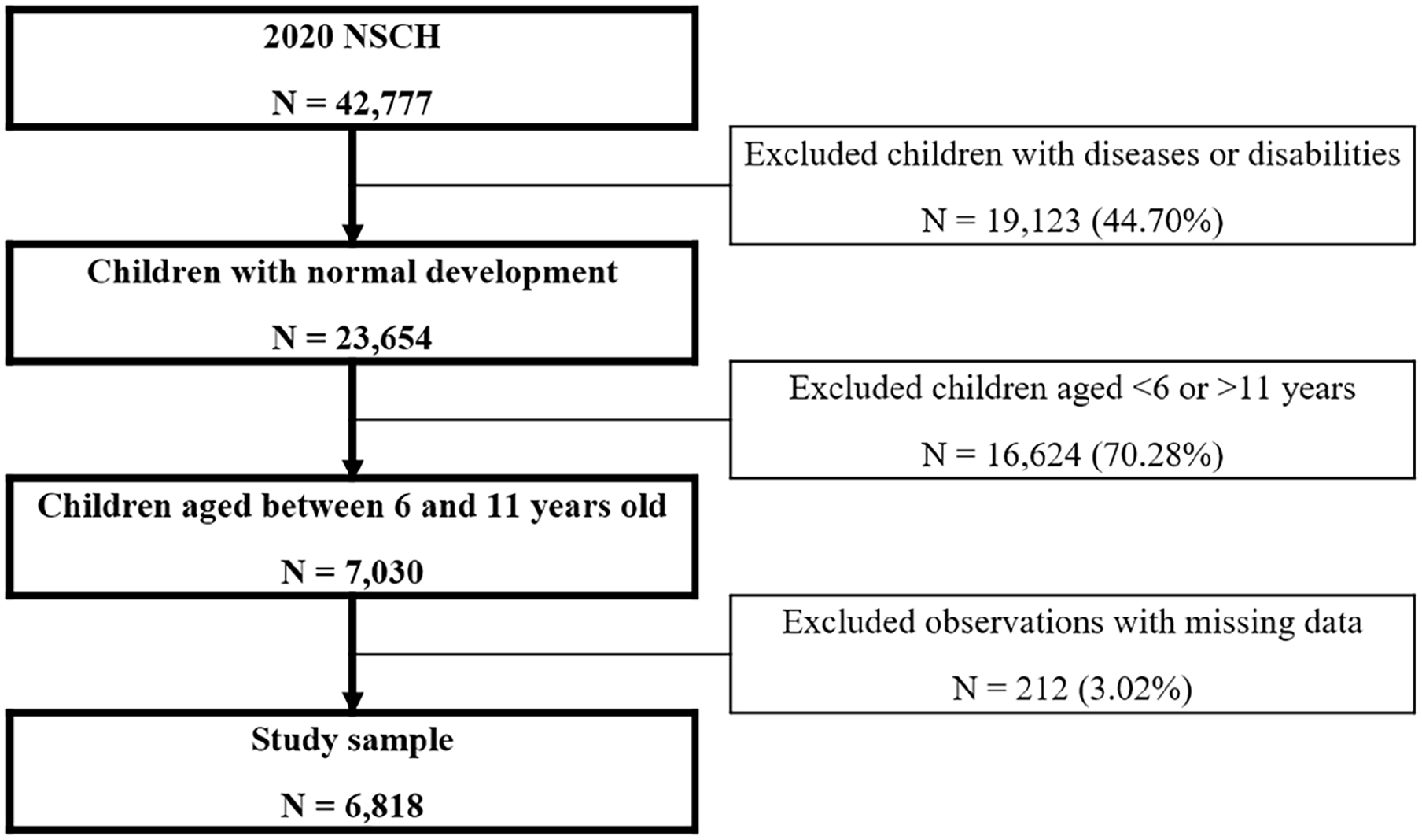
Flow Diagram of the Sample Selection Procedure.
Study Variables
Dependent Variable
The dependent variable was adequate sleep, which was measured using a dichotomous scale (1 = adequate sleep and 0 = inadequate sleep). These two options refer to the options provided by the NSCH data (i.e., good sleep and poor sleep). In the NSCH data, based on the American Academy of Sleep Medicine (AASM) guidelines, obtaining 9 to 12 hours of sleep per day, including nighttime sleep and napping, was considered adequate sleep. Therefore, children sleeping 9 or more hours were considered to have adequate sleep, and those sleeping less than 8 hours were considered to have inadequate sleep in the NSCH data (Chaput et al., 2018; CAHMI, 2022).
Independent Variables
The independent variables were participation levels of children in five occupational areas (education, work, play, leisure, and social participation). Participation of children in education was assessed by inquiring about their frequency of concern for achieving good grades at school using a 3-point rating scale (2 = always, 1 = usually, and 0 = sometimes and never). Although “sometimes” and “never” were initially considered separate options, in this study, both options were merged as “sometimes and never” owing to the extremely small number of responses (i.e., <1% of the total number of responses). Participation of children in work was assessed by inquiring about their engagement in volunteer work at school, places of worship, and the community using a dichotomous scale (1 = yes and 0 = no). In general, “work” for school-age children refers to academic activities or studies at school (Lewis, 2004). However, in this study, variables aligning with the definition of “work” as per Occupational Therapy Practice Framework (OTPF-4; AOTA, 2020) were selected. According to the OTPF-4, “work” for children aged 6 to 11 years refers to volunteer work at school, places of worship, and the community (AOTA, 2020). Participation of children in play was assessed by inquiring about their frequency of engagement in physical activities lasting >60 minutes within the past week. The responses were assessed using a 4-point rating scale (4 = every day, 3 = 4–6 days, 2 = 1–3 days, and 1 = 0 day). Participation of children in leisure involved a question regarding their frequency of engagement in leisure activities (watching programs, playing games, accessing the internet, or using social media on TV, computers, cellphones, or other electronic devices) within the past week. The responses were assessed using a 5-point rating scale (4 = ≥ 4 hours, 3 = 3 hours, 2 = 2 hours, 1 = 1 hour, and 0 = <1 hour). Social participation of children was assessed by inquiring about their frequency of attending social activities (after-school or weekend activities such as sports teams, clubs, organized lessons [e.g., sports, music, dance, language, and arts], and other group engagements) along with their caregiver within the past 12 months. The responses were assessed using a 4-point rating scale (3 = always, 2 = usually, 1 = sometimes, and 0 = rarely or never). This study utilized the scales of each variable as they were collected by the NSCH.
Covariates
Child-related covariates included age, sex, race (Hispanic, non-Hispanic White, non-Hispanic Black, or non-Hispanic others), language (English or other than English), number of family members (two or less, three, four, or five or more people), and parent’s marital status (currently married two parents, not currently married two parents, single parent, or others). Since children and their caregivers share an interdependent relationship, and the personal attributes of caregivers are associated with children’s adequate sleep (Boergers et al., 2007; Mindell et al., 2010; Sadeh et al., 2009), caregiver-related covariates were included in statistical analyses. Caregiver-related covariates included age, sex, educational level (college degree or higher, some college or technical school, high school or general educational development, or less than high school), income level (≥400% federal poverty level [FPL], 200%–399% FPL, 100%–199% FPL, or 0%–99% FPL), mental health status (good or poor), and physical health status (good or poor).
Statistical Analysis
The sociodemographic characteristics of the children and their caregivers included in the study were analyzed using descriptive statistics. The association between adequate sleep and children’s participation in the five occupational areas was investigated using multivariate logistic regression analysis while controlling for covariates. In Model 1, the dependent variable was adequate sleep, and the independent variables were occupational areas (education, work, play, leisure, and social participation). In Model 2, the dependent variable was adequate sleep, and the independent variables were occupational areas, controlling for child-related covariates. In Model 3, the dependent variable was adequate sleep, and the independent variables were occupational areas, controlling for both child- and caregiver-related covariates. The results were presented as odds ratios with 95% confidence intervals (CIs). Data management and statistical analysis were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
A total of 6,818 children were included in the analysis. Table 1 shows the sociodemographic characteristics of the participants. Their mean age was 8.48 years (standard deviation = 1.72), and 3,696 (54.21%) of children were females.
Sociodemographic Characteristics of the Sample (N = 6,818).
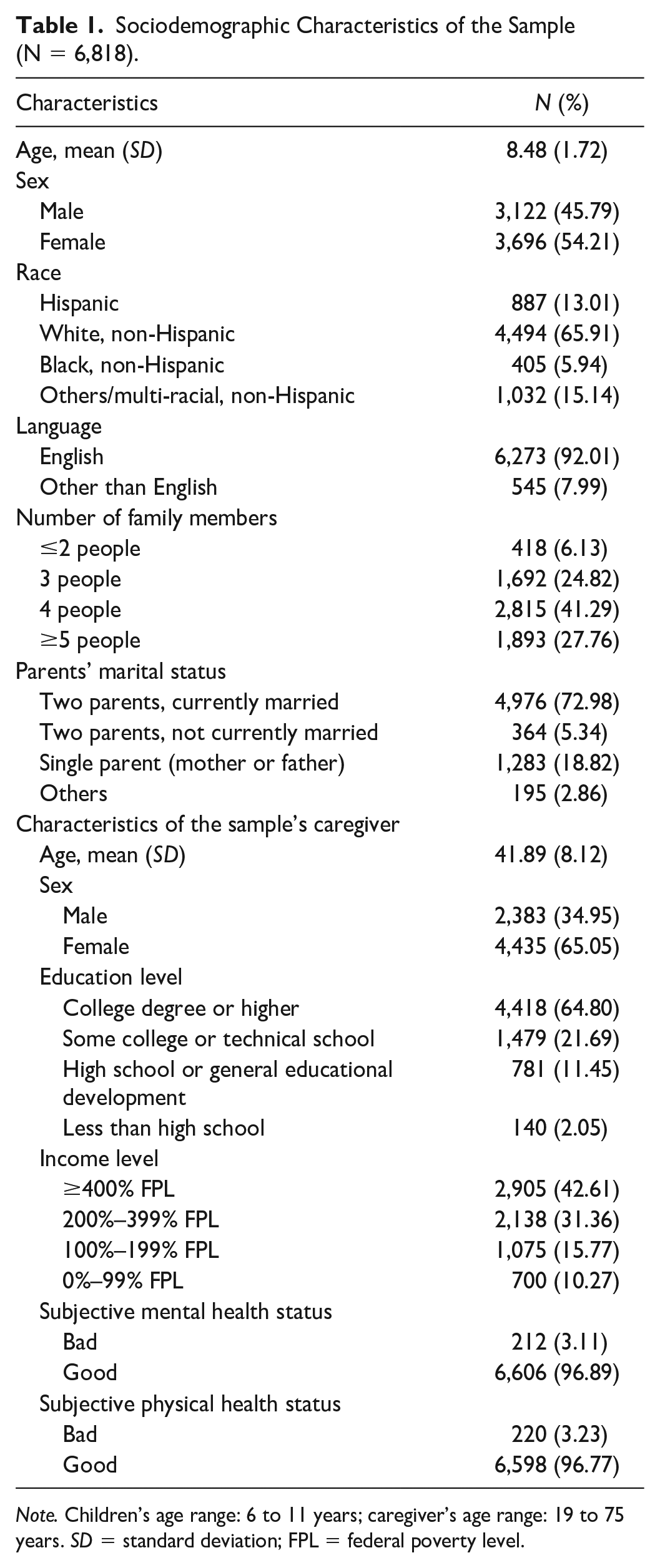
Note. Children’s age range: 6 to 11 years; caregiver’s age range: 19 to 75 years. SD = standard deviation; FPL = federal poverty level.
Table 2 shows the results of multivariate logistic regression analysis. Model 1 (unadjusted) was used to analyze the participation of children in occupational areas, including education, work, play, leisure, and social participation. Model 1 revealed statistically significant associations between adequate sleep and increased participation in four occupational areas (27% increased participation in leisure, 95% CI: 1.21–1.33; 22% increased participation in play, 95% CI: 1.15–1.30; 18% increased participation in work, 95% CI: 1.04–1.32; 9% increased participation in social participation, 95% CI: 1.01–1.18). However, the associations between adequate sleep and increased participation in education were not statistically significant (95% CI: 0.95–1.14).
Association Between Adequate Sleep and Occupational Areas in School-Age Children.
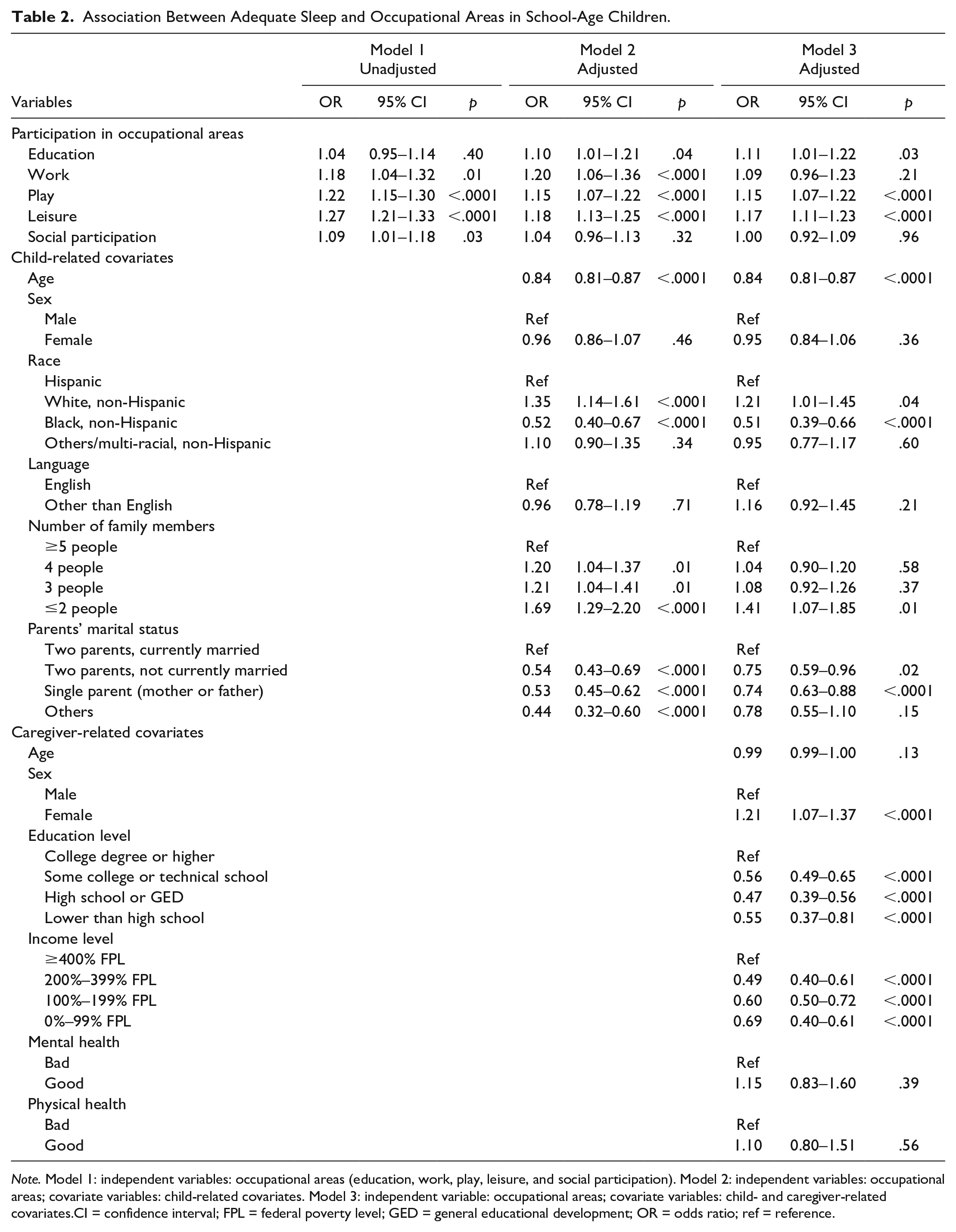
Note. Model 1: independent variables: occupational areas (education, work, play, leisure, and social participation). Model 2: independent variables: occupational areas; covariate variables: child-related covariates. Model 3: independent variable: occupational areas; covariate variables: child- and caregiver-related covariates.CI = confidence interval; FPL = federal poverty level; GED = general educational development; OR = odds ratio; ref = reference.
Model 2 was adjusted for child-related covariates. It revealed statistically significant associations between adequate sleep and increased participation in four occupational areas (20% increased participation in work, 95% CI: 1.06–1.36; 18% increased participation in leisure, 95% CI: 1.13–1.25; 15% increased participation in play, 95% CI: 1.07–1.22; and 10% increased participation in education, 95% CI: 1.01–1.21). However, the associations between adequate sleep and increased participation in social participation were not statistically significant (95% CI: 0.96–1.13).
Model 3 was adjusted for both child- and caregiver-related covariates. It revealed statistically significant associations between adequate sleep and increased participation in three occupational areas (17% increased participation in leisure, 95% CI: 1.11–1.23; 15% increased participation in play, 95% CI: 1.07–1.22; and 11% increased participation in education, 95% CI: 1.01–1.22). However, the associations between adequate sleep and increased participation in work (95% CI: 0.96–1.23) and social participation (95% CI: 0.92–1.09) were not statistically significant. Covariates positively associated with adequate sleep included non-Hispanic White, smaller number of family members, female caregivers, caregiver’s good mental health status, and caregiver’s good physical health status. Conversely, negative associations with adequate sleep were observed for covariates such as older age of children, non-Hispanic Black, parent’s marital status other than being currently married, caregiver’s educational level of below college degree, and caregiver’s income level of <400% FPL.
Discussion
In this study, the associations between adequate sleep and participation in five occupational areas (i.e., education, work, play, leisure, and social participation) were analyzed in school-age children using the NSCH data. The results from the final model (i.e., Model 3) indicated that adequate sleep (9–12 hours, according to the AASM) was associated with increased participation in three occupational areas (i.e., leisure, play, and education). The study findings provide valuable information for occupational therapists to emphasize the importance of children’s participation in various occupational areas for achieving adequate sleep.
The results showed that adequate sleep was associated with increased participation in leisure. This finding is consistent with that of previous studies showing that sleep is positively associated with participation in leisure activities (Amiri et al., 2022; Brand et al., 2009; Dursun et al., 2015; Rosa et al., 2021). In previous studies, adequate sleep duration was found to be strongly associated with leisure activities, particularly physical activity, such as sports (Brand et al., 2009; Dursun et al., 2015; Rosa et al., 2021). Although leisure, as defined by the OTPF-4, refers to intrinsically motivated and engaged activities during any period, including variety of activities (AOTA, 2020), the leisure activities surveyed in the NSCH included watching TV, using computer/social media, using cell phones/electronic devices, and playing games (CAHMI, 2022; Lenhart et al., 2015). Other studies have revealed that adequate sleep is inversely associated with sedentary leisure activities, such as screen time (Dalene et al., 2018; Xu et al., 2016). This study evaluated the frequency of screen time, whereas other studies evaluated the time spent on it. Therefore, future research is needed to investigate leisure activities with various characteristics, considering both frequency and duration for adequate sleep. In addition, it may be beneficial to consider and adjust for the influence of children’s living environments on their leisure activities.
Furthermore, this study revealed a significant association between adequate sleep and increased participation of children in play, a finding consistent with that of previous studies (Ekstedt et al., 2013; Sorić et al., 2015; Xu et al., 2016). The most common type of play among school-age children is physical activity. Previous studies have reported that regular participation in intense physical activity is beneficial for establishing healthy sleep patterns and enhancing sleep efficiency in school-age children (Dworak et al., 2008; Foti et al., 2011; Iwata et al., 2011; Matricciani et al., 2020). Caregivers can encourage children to engage in at least 60 minutes of moderate-intensity physical activity play each day, in accordance with the international physical activity guidelines (World Health Organization, 2010). However, engaging in vigorous physical activities before bedtime is not recommended, as it is negatively associated with sleep quality (Driver & Taylor, 2000). Therefore, providing guidance for children to avoid engaging in vigorous physical activities before bedtime might be good. Parents are also encouraged to guide their children in choosing the type of play, the method of play, and the place for play, as these factors may influence children’s sleep quality and can lead to elevated fatigue levels (Abraham & Scaria, 2015; Gruber et al., 2016). Hence, parental support needs to be considered, although it was not adjusted for in the current study due to limitations in the variables available from the NSCH data.
This study showed that adequate sleep was positively associated with increased participation of children in education, which was evaluated by asking about their frequency of concern for achieving good grades at school. Children who make an effort to achieve good grades are more likely to be actively engaged in their education (Lee, 2014). Children’s participation in education is related to increased levels of daily activities. Elevated fatigue levels associated with increased daily activities are linked to adequate sleep among children (Abraham & Scaria, 2015; Gruber et al., 2016). Teachers have a substantial influence on children’s motivation to participate in educational activities (Koca, 2016). Therefore, further research is warranted, which includes controls for educational environment, encompassing factors such as the relationship between the child and teacher, teacher’s teaching style, or the school environment. Considering that previous studies have reported inadequate sleep duration resulting from difficulties in managing stress caused by participation in educational activities (Pascoe et al., 2020; Sadeh et al., 2000), guidance to maintain optimal levels of participation in education is necessary.
The current study revealed no significant association between adequate sleep and children’s social participation. This result is inconsistent with those of previous studies reporting a link between adequate sleep and social participation (Chien et al., 2019; Gordon et al., 2021). In this study, uncontrolled confounders, such as caregiver’s support or the community environment (Bedell et al., 2013; Hart, 2013), may contribute to the lack of a significant association between adequate sleep and social participation.
The association between adequate sleep and participation of children in work was not statistically significant in the current study. Since this is the first study to examine the association between adequate sleep and children’s work, which includes volunteer work at school, worship places, and the community (AOTA, 2020), additional research is warranted to validate this association. For example, factors influencing children’s volunteering, such as the residence areas of the caregiver or child and the financial support provided by the caregiver, are recommended to be included in the analysis (Perenboom & Chorus, 2003).
Implications for Occupational Therapy Practice
Inadequate sleep duration in children may result in occupational imbalance and their poor well-being (Backman, 2004; Chaput et al., 2018; Fadzil, 2021; Ho & Siu, 2018). Given the association between children’s adequate sleep and increased participation in occupational areas determined in the current study, it is recommended that occupational therapists may assist children in achieving adequate sleep by promoting participation in daily life activities (Case-Smith & O’Brien, 2014).
Occupational therapists play a crucial role in promoting children’s participation in various occupational areas (AOTA, 2020; Case-Smith & O’Brien, 2014; Rosenberg et al., 2019). For example, first, occupational therapists can focus on motivation, inspiring children to engage actively by offering guidance on a diverse range of activities in their daily lives. Second, occupational therapists can contribute to efficient time management by assisting in the planning and organization of children’s schedule, ensuring meaningful engagement in occupational areas. Third, occupational therapists can use environmental modification approaches to mitigate barriers that may hinder participation in activities. Fourth, imbalanced participation of children in occupational areas can be monitored to achieve occupational balance. Finally, occupational therapists can collaborate with caregivers or teachers to provide education and coaching, providing a holistic environment for increasing the participation of school-age children.
Limitations
Secondary data analysis has the advantage of using large samples to derive and check results. However, this study may have some limitations due to variable constraints. In this study, adequate sleep duration was a binary variable, indicating whether or not the recommended sleep duration for the corresponding age was achieved. Thus, the results cannot explain the associations between sleep and participation in terms of a linear association framework. Among the occupational areas, ADLs, IADLs, and health management were not available from the NSCH data. Nonetheless, participation in occupational areas applied in this study was measured using the most relevant items available in the NSCH data, items that narrowly addressed participation compared with the broader definitions in the OTPF. For instance, the leisure variable analyzed in this study included activities involving screen time. Therefore, information on leisure activities with other characteristics is lacking. Further studies are warranted to analyze leisure activities with various characteristics to obtain information about activities strongly related to good sleep. Furthermore, the play variable primarily focused on physical activity, excluding table-top play activities such as board games or crafts from the analysis. The results of this study can only be applied to children without disabilities, as the study sample typically comprised developing children. Therefore, further research is warranted to examine the association between adequate sleep and occupational participation in children with disabilities.
Conclusions
The study findings suggest an association between children’s adequate sleep and increased participation in occupational areas, including leisure, play, and education. Therefore, it is recommended for occupational therapists working with children to understand that increased participation in occupational activities is associated with adequate sleep.
Footnotes
Acknowledgements
This work was supported by the VA Pittsburgh Healthcare System. The contents do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (grant number: NRF-2021S1A3A2A02096338).
Ethical Approval and Patient Consent
This study protocol was reviewed by the Institutional Review Board of Yonsei University Mirae Campus and granted an exemption from requiring written informed consent (approval number: 1041849-202211-SB-197-01).