
Abstract
We used a community-based participatory research (CBPR) approach to develop and conduct a mixed-methods needs assessment with a sample of 36 veterans. We gathered data using the Short-Form 36 Health Survey (SF-36), focus groups, and individual interviews. The sample SF-36 mean scores were significantly higher than the general population average for general health, but lower for role limitations due to emotional problems, vitality, and social functioning. The qualitative data revealed three significant health needs for the veterans: (a) access to mental health services, (b) barriers to social participation, and (c) the importance of nature-based occupations. Findings suggest that occupation-based interventions, administered in the natural environment, targeting rural veterans’ mental health and social participation, could help improve their access to needed mental health care.
Plain Language Summary
We assessed rural Montana Veterans on a Short Form (SF-36) health survey. They also participated in focus groups and interviews about their health needs. The veterans in the sample reported better overall health than the average person, but they struggled more with emotional challenges, energy levels, and social connections. Interviews revealed three main needs: (a) better access to mental health services, (b) help with staying socially connected, and (c) opportunities for outdoor activities. This suggests that offering activities in nature that support mental health and social engagement could help rural veterans get the mental health care they need.
Introduction
Occupational therapy (OT) research has shown engaging in occupations specific to military service can have lifelong effects on veterans’ trajectories of health and well-being throughout the life course (Carroll & Bailliard, 2024; Eakman et al., 2016; Kinney, Graham et al., 2020). Given this, U.S. military veterans have diverse and unique health care needs as they are more at risk than civilians of experiencing mental health disorders, post-traumatic stress, traumatic brain injuries, and other conditions associated with their time in service (Olenick et al., 2015). To date, research on the health of U.S. military veterans has mainly focused on veterans who live in urban areas and have easier access to Department of Veterans Affairs health care services (O’Shea et al., 2019). However, much less is known regarding the impact of military service on rural veterans’ health, especially how this varies based on social determinants of health (SDOH).
The World Health Organization (WHO, 2019) defines SDOH as nonmedical factors influencing health outcomes, including the conditions in which people are born, grow, work, live, and age. Within OT, scholars have argued that SDOH shape the opportunities for and access to health-promoting occupations (Bailliard et al., 2024). In the context of Montana, SDOH are a useful perspective for examining how veterans’ health is shaped by the places in which they live. A focus on local communities is needed to understand veterans’ health better as these places provide the context for resources, opportunities, and barriers inextricably linked to health and well-being. To illustrate, compared with the national veteran population, veterans in Montana overall have less access to health care resources (U.S. Census Bureau, 2021) given the rurality of the state. This is of concern as Montana has the second largest veteran population in the United States, with an estimated one out of every 10 residents identifying as a veteran (U.S. Census Bureau, 2021). Of these veterans, almost 72% live in rural areas in the state. Rural residents historically have been overrepresented in military service which is reflected in the higher concentrations of veterans who live in rural versus nonrural counties in the United States (Jameson & Curtin, 2012). While no differences in the likelihood of developing health conditions between rural and urban veterans have been found rural veterans experience challenges accessing the health care services they need (Turvey et al., 2019).
Research has estimated that up to 75% of veterans in rural areas receive health care services outside the U.S. Department of Veterans Affairs (VA) health care system due to geographical distances to the nearest VA and satisfaction with non-VA health care providers (Nayar et al., 2013). In Montana, less than 40% of veterans in the state utilize VA health care (U.S. Census Bureau, 2021). In addition to limited access, rural veterans also do not receive the same quality of care or the same types of health care as their urban counterparts (O’Shea et al., 2019). For example, rural veterans are 70% less likely to receive care for mental health and 64% less likely to receive outpatient services or medication for mental health conditions (Teich et al., 2017).
The veterans’ community in Montana has some clear and pressing health needs. The ability to address these needs with evidence from the current literature is limited as dominant understandings of the impact of military service on health and well-being are mainly based on veterans who receive health care services from the VA and live in urban areas. Extrapolating these understandings to veterans in Montana is problematic as many veterans do not use the VA for health care services and most live in rural areas.
There is a need then in Montana for a collaborative research approach focused on veterans’ health that seeks to understand the unique health needs of veterans from their perspectives and how local community contexts shape access to and participation in health-promoting occupations.
To address this need, the purpose of this study was to conduct a veteran-centered health needs assessment using a CBPR approach (Israel et al., 2012) to define priority health needs to be addressed by OT interventions. This study was guided by the following research question: What are the unmet health needs of veterans in Montana that OT programming can address?
Method
Research Design and Theoretical Framework
A needs assessment is applied research that gathers and analyzes data to identify and describe gaps in service. In OT, needs assessments are used to identify the needs of groups of people to develop occupation-based services, programs, and policies that can address those needs (Finlayson, 2017). To develop the veteran-centered health needs assessment, the first author used established collaborative partnerships from previous research and community-based OT practice with the local veteran’s community to establish a community advisory board (CAB). Before this study, the first author obtained initial grant funding for a pilot planning project in the previous year that supported her in learning more about the veterans’ community in Montana and creating collaborative and equitable research partnerships with the veterans’ community in Montana. The first author spent over a year volunteering and attending local veterans’ nonprofit events and meetings to build trust and working relationships with key stakeholders in the veterans’ community. She educated the local veteran community on the role of OT in addressing community health and, in turn, learned more about how nonprofits in Montana were addressing veterans’ needs in community settings.
In line with a CBPR approach as a variation of participatory action research, potential partners and veteran service nonprofits whose work aligned with OT principles were identified, and these community stakeholders were approached about becoming CAB members. They all agreed to participate. The CAB comprised five veteran community stakeholders and established operating norms and principles to ensure equity and power sharing in the research process (Israel et al., 2012). The CAB and the first author collaboratively developed the veteran-specific needs assessment, including the paper-based survey and the individual and focus group interview question guide. The CAB was involved in the needs assessment process and associated decision-making. CAB meetings were held every 3 months between January 2023 and March 2024. This study was approved by the Rocky Mountain College Institutional Review Board (IRB).
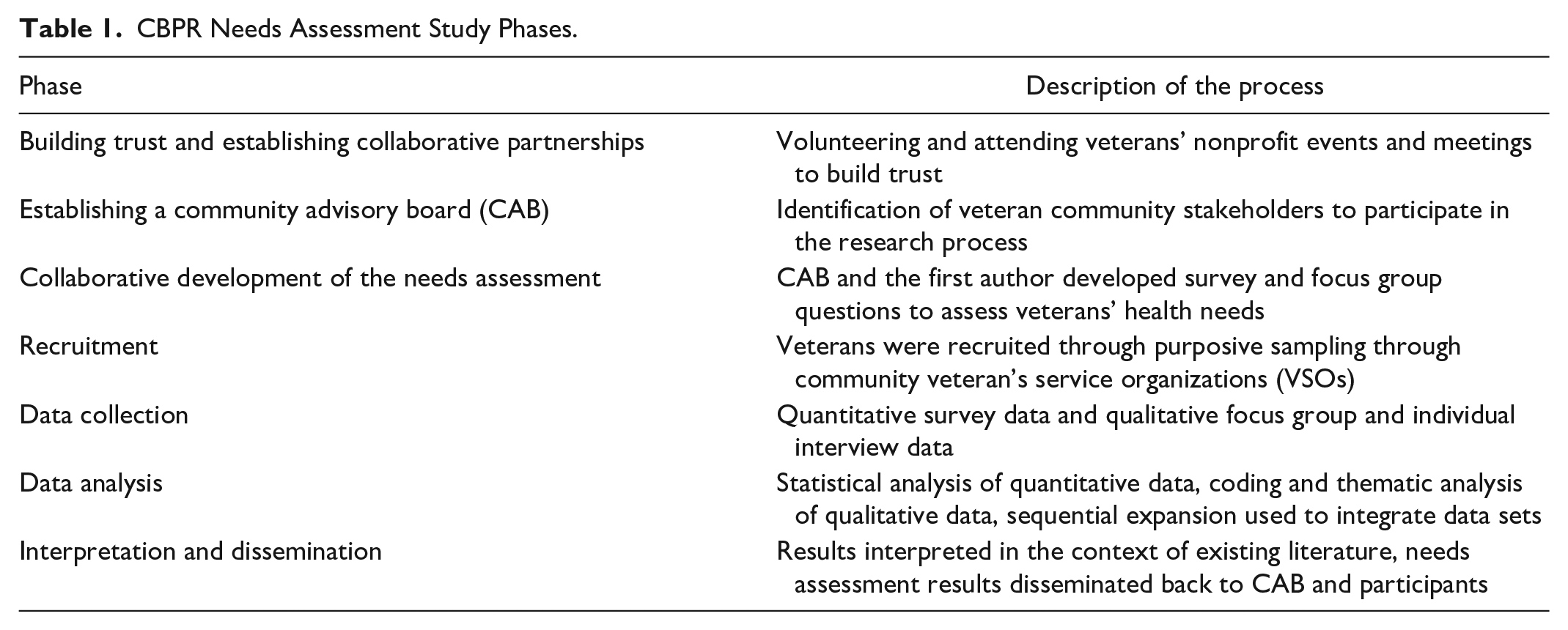
This project used a CBPR approach to needs assessment that equitably involved the veterans’ community in Montana in the research process. There is increasing recognition in the literature of the need for participatory approaches to research and interventions focused on reducing health disparities (Israel et al., 2012). CBPR is a useful research design for investigation of veterans’ health, given its emphasis on empowering veterans as active and engaged partners in the research process and attunement to the role of SDOH. In line with methodological recommendations for high-quality needs assessments (Finlayson, 2017), this study used a cross-sectional emergent quantitative and qualitative mixed-methods needs assessment (see Table 1 for Study Phases).
CBPR Needs Assessment Study Phases.
Participants and Recruitment
In 2023, Montana veterans were recruited through purposive sampling of four community veteran’s service organizations (VSOs) in Montana within a 1-hr drive of the university location. Eligible participants were at least 18 years old, communicated in English, were residents of Montana, and self-identified as U.S. military veterans. The authors volunteered at the VSOs’ local community events between January and May 2023 to develop trust and rapport with the local veteran community. Veterans were informed about the study and invited to participate after IRB approval. In addition, community stakeholders distributed research flyers through VSO email listservs and social media.
Data Gathering Instruments
Demographic Questionnaire
Basic demographic information and military demographics, including age, gender, branch of service, years served in the military, and service era, were gathered from the participants.
The RAND SF-36
The SF-36 (Ware et al., 2005) is a standardized measure assessing health-related quality of life. The SF-36 consists of 36 questions, with four health-related subscales comprising physical health (Physical Functioning, Role Physical, Bodily Pain, and General Health) and four health-related subscales comprising mental health (Vitality, Social Functioning, Role Emotional, and Mental Health). Scores on each SF-36 domain subscale and the total physical and mental health score range from 0 to 100, with higher scores indicating better functional health and well-being. Item responses are rated on Likert-type scales ranging from 2 to 6 points, and respondents must consider the past month when providing answers. The SF-36 has been used extensively in health-related research and has demonstrated reliability and validity in the adult population (Jason et al., 2011).
Focus Group Interview Guide
The focus group questions were based on an extensive literature review and developed in collaboration with the CAB. The researchers developed the focus group questions to elicit discussion of veterans’ specific health needs, occupations they engage in for their health, barriers to being healthy, and community resources and services they utilize to be healthy. Sample questions included: (a) What do you do to stay healthy? (b) What types of activities do you engage in, or what are some things you do daily/weekly for your health? (c) Do you experience any barriers or challenges that impact your health? (d) Who and what helps you be healthy? (e) Do you use any community resources or services to support your health? Are there any that don’t exist in our community but you would use?
Procedures
Participants completed a demographic questionnaire and the SF-36 health survey before participating in the interviews so that the focus group discussions would not bias their ratings. Qualitative data were obtained through in-person focus groups and audio-recorded interviews to gain first-person perspectives from veterans. Participants provided verbal and written informed consent at the beginning of each individual or focus group interview. Focus groups involved three to six participants simultaneously, with two researchers leading the group using the semi-structured interview guide. Four focus groups were conducted in the community at two local veteran service organizations. Focus groups were intentionally held at VSO locations familiar to the veterans to promote their comfort in line with best practice recommendations for engaging veterans in the research process (Barker et al., 2022). Six veterans were uncomfortable participating in the focus groups but agreed to individual interviews via Zoom. The same interview guide was used for the individual interviews. Focus groups occurred from June through November 2023. Focus group interviews averaged 120 min, and individual interviews averaged 45 min.
Data Analysis
Quantitative Analysis
We used the IBM Statistical Package for Social Sciences (SPSS) for Windows Version 29.0 to analyze the quantitative data. We computed means and standard deviations for the SF-36 variables. The SF-36 subscale scores of the 36 veterans were compared with the normative general civilian population (Mariush, 2011) data using one-sample t-tests. For the one-sample t-test, a two-tailed 5% significance level was used to interpret p values.
Qualitative Analysis
The researchers verbatim transcribed qualitative interviews. Transcript coding began inductively and included a combination of descriptive, in vivo, and process codes (Saldana, 2016), resulting in a codebook with codes grouped into categories and emerging themes. Subsequently, the authors met to discuss codes to establish inter-coder reliability, determined by double-coding one shared transcript and comparing coding patterns, which were 90% in agreement. The remaining transcripts were then independently coded. Meetings were held weekly to discuss the coding process and emerging themes. A matrix display containing summary demographic information, emergent themes, illustrative quotes, and other observations was created for the analysis.
Researchers kept a reflexive journal to develop an ongoing awareness of their positionality, identity, and interpretations surrounding the data. In line with a CBPR approach (Israel et al., 2012), preliminary findings were shared with the CAB and participants as a form of member checking to validate the emerging findings, establish rigor and trustworthiness, and enhance research participation. CAB members and participants provided helpful commentary that further confirmed the findings.
Mixed-Methods Integration
The researchers used sequential expansion as an integration strategy (Bazeley, 2018) to combine the two data sets meaningfully. Sequential expansion builds on the insights gained from initial data collection to ensure consistency across different data sets. For this study, information from the qualitative interviews was used to better understand and expand upon the survey results. The integration of the data is interpreted in the discussion section.
Results
Quantitative Results
Demographics
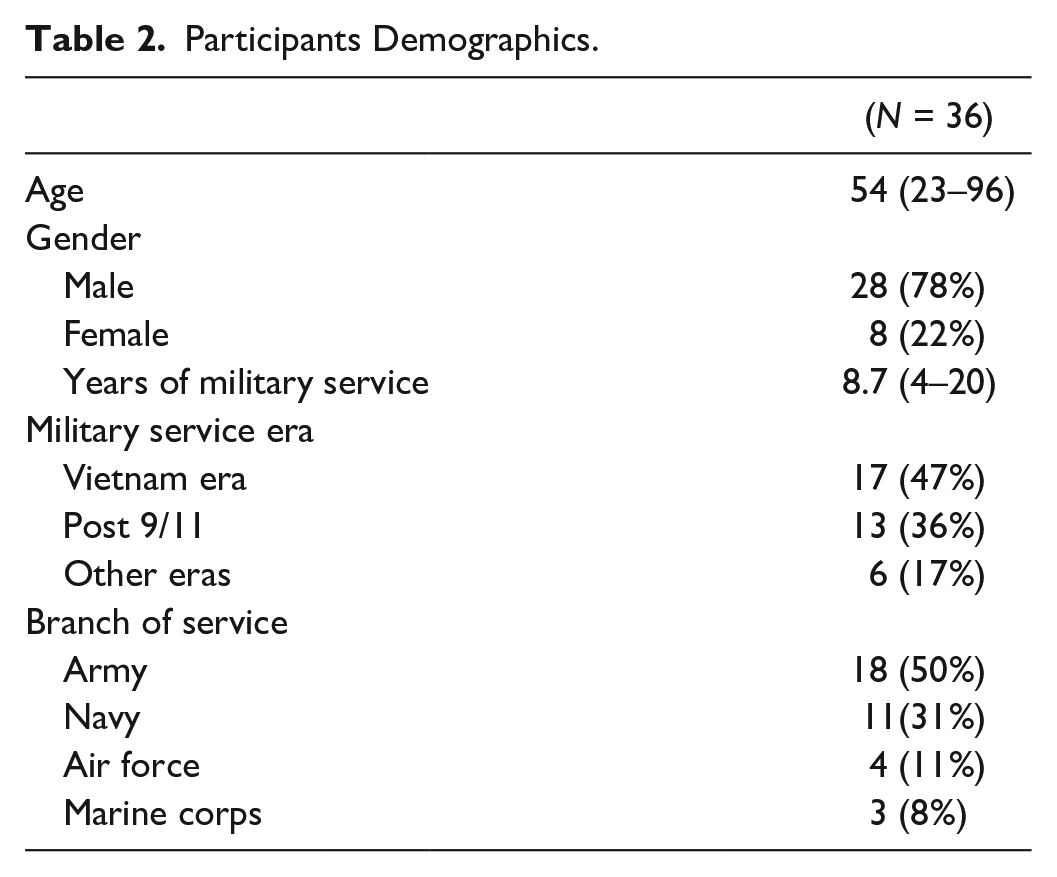
Thirty-six veterans provided informed consent and participated in the needs assessment. The majority of participants were male (n = 28). Participants’ ages ranged from 23 to 96 years, with an average age of 54. Fifty percent served in the U.S. Army, and 47% served during the Vietnam Era (see Table 2 for key participant demographic characteristics).
Participants Demographics.
SF-36 Health Survey Results for Veteran and Comparison Group
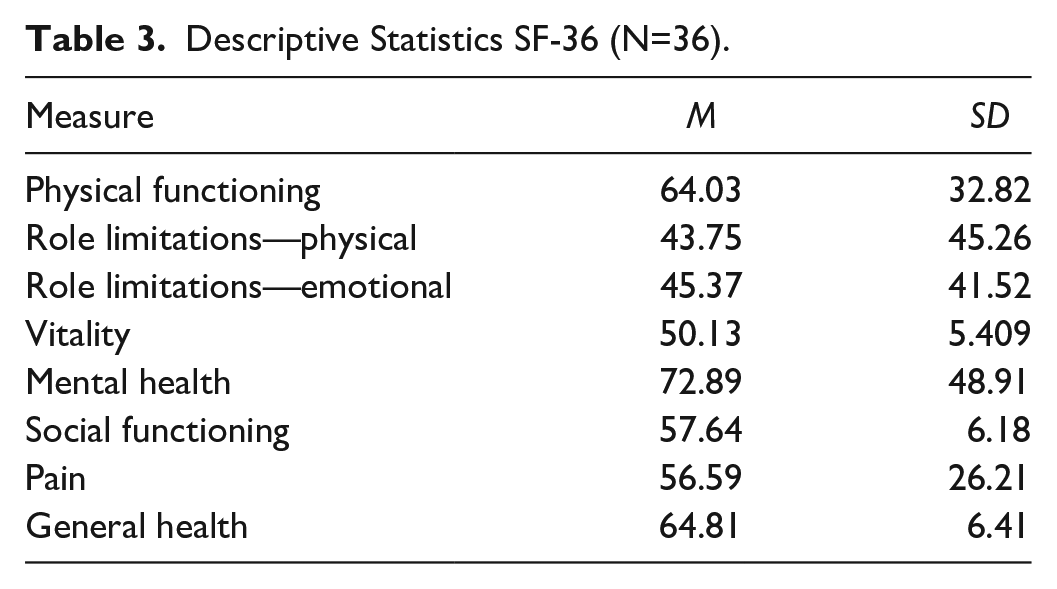
SF-36 descriptive statistics showed that for the eight health-related subscales, the veteran sample scored the highest mean (M = 72.88) for Mental Health and the lowest mean for Role Emotional (M = 45.37). The U.S. adult population norm mean score (theoretical mean with which the sample psychometrics were compared) for each domain is M = 50 (SD = 10) (Maruish, 2011; see Table 3).
Descriptive Statistics SF-36 (N=36).
The veteran sample group mean was significantly lower than the theoretical mean for Role Emotional, Vitality, and Social Functioning and significantly higher for General Health. No statistically significant differences were found between the veteran sample group mean and the theoretical mean for Physical Function, Role Physical, Pain, and Mental Health (see Table 4).
Distribution of SF-36 Subscale Scores in Veteran and Comparison Group.
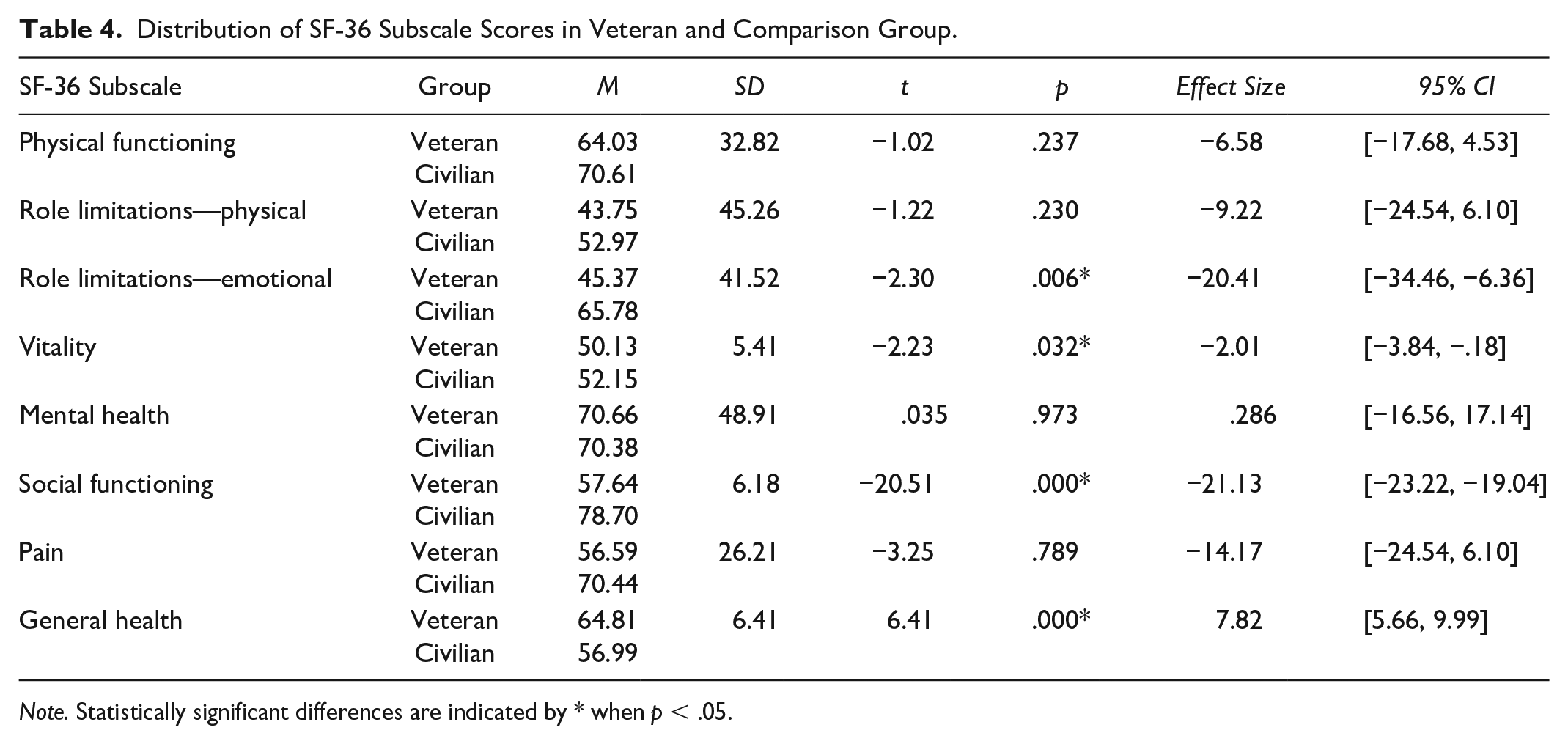
Note. Statistically significant differences are indicated by * when p < .05.
Qualitative Findings
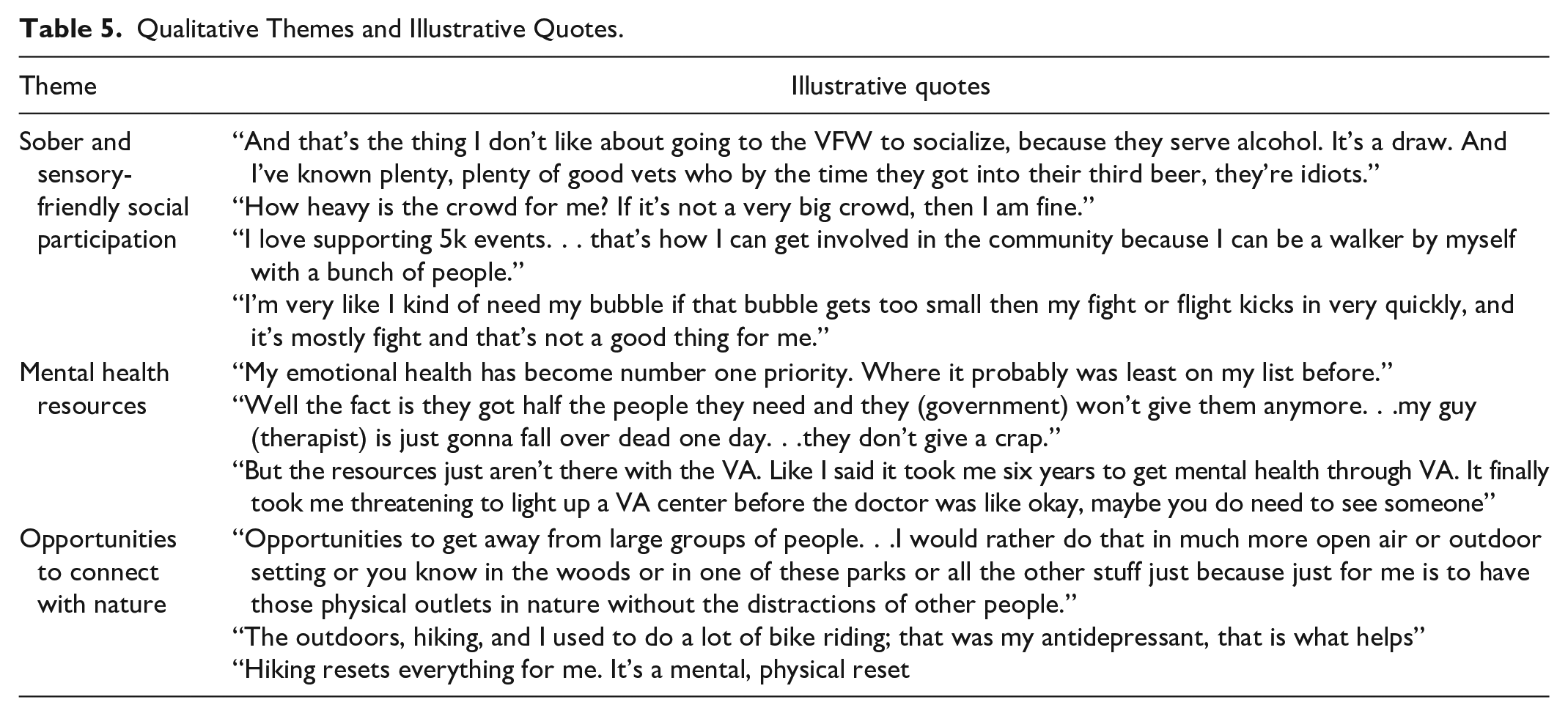
Three themes describing veterans’ health needs emerged from the qualitative data and are presented in the following sections: (a) mental health services, (b) sober and sensory-friendly social participation, and (c) nature-based occupations. While participants expressed many needs, only the most salient themes from the needs assessment are presented in this article. A summary of each theme, with illustrative quotes, is presented in Table 5.
Qualitative Themes and Illustrative Quotes.
Theme #1: Mental Health Services
The most frequent and important health need expressed by the veterans in this study was the need for access to consistent mental health services in the local community. Across the board, veterans identified the need for “more mental health resources” as a top priority. One veteran stressed the importance of mental health stating, “My mental and emotional health has become number one priority. Where it probably was least on my list before.” Veterans shared stories of their struggles accessing mental health services through the VA and community health clinics including distance to local VA facilities and a lack of resources and trained mental health providers. Many veterans described living in rural areas and commuting long distances to come to an urban area to receive services. The VA told one veteran he needed to come in for sessions 3 days a week and shared how this wasn’t feasible explaining, “I live in Lewistown its 130 miles one way. I can’t afford to drive that every day or every other day . . . so it was oh veteran refused treatment.” Another veteran described the extreme action he had to take to receive mental health services through the VA for post-traumatic stress disorder (PTSD) and anxiety sharing, But the resources just aren’t there with the VA. Like I said it took me six years to get mental health through VA. It finally took me threatening to light up a VA center before the doctor was like okay, maybe you do need to see someone.
Veterans shared that waiting times for mental health services were another barrier. A veteran shared that even though he lives in a city where there is a VA clinic offering mental health services, he waited months to see a provider stating, “Time is one of the biggest ones (barriers), I mean, you go in for something. Well, then it takes 30 days and somebody sits on it . . . finally calls you to schedule something two or three months later.” “Even if veterans were able to access services, many expressed frustration at the turnover in mental health providers.” One veteran illustrated this point stating, “The VA . . . I haven’t had the same provider twice in eight years.” Another veteran echoed a similar experience with provider turnover and the devastating effect this had on his mental health describing, “I’d have another provider and start the process over again. And I did that six different times and I gave up, which actually did lead to suicide. So I attempted suicide twice.”
Along with access and consistency of mental health services, veterans also shared their concerns about mental health providers having a lack of understanding of their military experiences and the impact on their mental health. Many described their experiences of feeling misunderstood by mental health providers. For example, a veteran expressed his feelings of being stigmatized by a provider stating, “That’s a lot of the problem with people in the mental health field. They have no idea what you’ve experienced. There’s things that I had to do to survive.” Others shared that they felt more comfortable when their providers were actually veterans who had similar experiences. One explained, “The people they hire at the VA should be veterans. They should hire people there who understand the people who are coming through the door.”
Theme #2: Sober and Sensory-Friendly Social Participation
When asked what supports their health, veterans discussed the value of participating in social occupations that gave them opportunities to connect and spend time with their family, friends, and other veterans. For instance, one veteran described, “It’s my close friends, my family, or wife that help me the most when I’m struggling because those are the people that I enjoy spending my time with.” Another stated how important it was for him to motivate himself to spend time with others for his mental health, stating, “You have to for your mental health, you have to get up and you have to at least make an attempt to get out and see people.”
While the veterans described the importance of social participation for their health, they also expressed the desire for opportunities to participate socially with others that did not revolve around alcohol. Veterans shared how in the local community most activities where veterans had a chance to connect with other veterans centered around alcohol. One veteran stated he spent a lot of time at a local veterans-focused gym because “There is no alcohol there, and that is huge.” Veterans expressed their dislike of socializing at traditional veteran gathering places, such as Veterans of Foreign Wars (VFW) or American Legion, due to the alcohol and bar-like atmosphere. One veteran explained, “I don’t like going to the VFW to socialize, because they serve alcohol. It’s a draw. And I’ve known plenty, plenty of good vets who by the time they got into their third beer, they’re idiots.” Likewise, another veteran had stopped attending social events at the American Legion stating, “There’s the American Legion where you sip your drink and you tell war stories. I don’t need that in my life.” A younger veteran noted it’s harder for him to socialize sober stating, “I’ve been sober for 8 months now, and I’ve had to throw away a lot of relationships because it’s more of a negative bias now that I don’t drink.”
Along with sober social activities, veterans also expressed the need for sensory-friendly social opportunities. Veterans shared they often wanted to engage in social activities with friends and families but experienced barriers due to sensory sensitivity. One veteran described his sensory challenges stating, “I know that I’m not deployed anymore and I’m not dealing with things like that (combat) but it’s kind of hard to turn that switch off.” Another veteran described the impact of “being on edge” on his occupations stating, A lot of us (veterans) have been taught and trained to do things most people haven’t done, puts a lot of us on edge. I know for me specifically like it puts me on really edge and I can’t really enjoy what I’m doing/
Veterans shared the challenges they faced when going to social activities where a crowd of people was likely. For example, one veteran expressed his discomfort with crowds describing how when he is asked to attend a social event he thinks, “How heavy is the crowd for me? If it’s not a very big crowd, then I am fine.” Another veteran described his need for personal space and hypervigilance whenever he eats with his family. He described, “I kind of need my bubble. If that bubble gets too small then my fight or flight kicks in very quickly, and it’s mostly fight and that’s not a good thing for me.” Stories of attending a social event, such as a sporting event or going out to eat and having to leave due to sensory challenges, were frequently shared by the veterans.
Theme #3: Nature-Based Occupations
When asked what resources in their local community helped promote their health, veterans expressed an appreciation for access to nature and the outdoors as a way to improve their mental health and overall well-being. Veterans shared stories of how spending time in nature allowed them to mentally reset, decrease their PTSD, anxiety, and depressive symptoms, and had a positive impact on their quality of life. One veteran discussed how nature provided solitude for him. He expressed his need to get away from crowds stating a preference for outdoor settings, “you know in the woods or in one of these parks or all the other stuff just because just for me is to have those physical outlets in nature without the distractions of other people.” Another veteran similarly shared that when he was feeling stressed he chose to engage in nature-based occupations by himself, “getting up to the mountains and hiking resets everything for me. It’s a mental and physical reset.”
Veterans shared the different nature-based occupations they engaged in solely and with others. One shared how engaging in these occupations impacted his mental health stating, “the outdoors, hiking, and I used to do a lot of bike riding; that was my antidepressant.” Veterans also expressed a desire for more opportunities to engage in nature-based activities in the community. For example, one veteran expressed he wished there were more opportunities socially for veterans to engage in nature-based occupations such as “Groups that go hiking, golfing, fly fishing activities, groups getting out there like living life because a lot of people they don’t know how to live, they have no idea how to live, they’re stuck in their ways.”
Integration of Quantitative and Qualitative Findings
The integration of quantitative and qualitative findings provided a comprehensive understanding of the health needs of rural veterans. Quantitatively, the SF-36 scores indicated lower-than-average scores in emotional role limitations, vitality, and social functioning, while general health scored above average. These results were contextualized by qualitative insights revealing barriers such as limited access to mental health services, challenges in finding sober and sensory-friendly social environments, and the therapeutic value of nature-based activities. Veterans’ first-person perspectives further highlighted how these factors impact their health and resilience.
Discussion
This study aimed to explore the health needs of rural veterans in Montana using quantitative and qualitative data. We aimed to understand the challenges faced by rural veterans and highlight areas in which OT intervention could be helpful. The quantitative results obtained from the SF-36 showed that the performance of Montana veterans for overall general health was higher than the general population average. This finding may be attributed to the impact of resilience veterans’ developed during their military service on their overall health. Resilience refers to the ability to adapt and recover from adversity, trauma, or significant sources of stress (American Psychological Association, 2019). Veterans often develop resilience during their military service and experiences, which can help them cope with the challenges they face post-service (Pietrzak & Cook, 2013). Research has shown that resilience is associated with better overall health and well-being for veterans (Georgescu et al., 2023).
For the rural veterans in this study, resilience may be particularly important in managing stressors associated with rural living, such as social isolation, travel times, and limited access to health care services and resources. Existing occupation-based literature has confirmed that occupational participation is associated with increased resilience among the veteran population (Carroll & Bailliard, 2024; Eakman et al., 2016; Kinney, Schmid, et al., 2020). Findings from the qualitative phase of the study help to bring more into focus the relationships between occupation and resilience, especially the potential impact of nature-based occupations for veterans’ overall health. Nature-based occupations and outdoor activities have been shown to decrease symptoms of depression and PTSD, improve mood, and enhance overall health and well-being (Bettmann et al., 2021). The natural environment in Montana offers many opportunities for such activities, which may contribute to the higher overall general health scores observed in the veteran sample.
However, despite higher general health scores, the veteran sample also reported significantly lower scores for role limitations due to emotional issues, decreased vitality, and decreased social functioning. Veterans often face higher rates of PTSD, depression, and anxiety, compared with civilians which can significantly impact their ability to participate in meaningful occupations (Vogt et al., 2020). These mental health challenges can also contribute to decreased vitality and energy levels. These barriers may lead to poorer mental health outcomes and lower scores in emotional well-being and social functioning.
In their interviews, the veterans highlighted a significant need for addressing mental health in the community, with many participants expressing that they had to be in crisis before they could get support. Barriers such as distance to VA facilities, long wait times, and turnover of mental health providers were highlighted, underscoring the challenges veterans face in accessing timely and continuous care. These findings echo the results of previous studies that show rural veterans face barriers to receiving mental health care, including decreased service availability and quality and culturally sensitive services (Koenig et al., 2016). Travel distance has also been identified as a major barrier for rural veterans seeking health care services (Buzza et al., 2011).
In addition to the need for mental health resources, the qualitative findings shed light on why the veteran sample reported significantly lower social functioning, often due to PTSD symptoms. Veterans expressed the need for sober and sensory-friendly social participation opportunities. This study substantiates previous research identifying the importance of social participation for veterans’ health (Carroll & Bailliard, 2024; Kinney, Graham, & Eakman, 2020) and emphasizes particular types of social participation identified as important by veterans. Participants expressed discomfort with traditional veteran gatherings centered around alcohol consumption. Sensory sensitivities, stemming from PTSD and anxiety, further complicated social interactions, highlighting the need for inclusive and accommodating social environments.
Overall, findings from this study underscore the multifaceted nature of veterans’ health needs and the need for a comprehensive approach that encompasses accessible mental health services, inclusive social environments, and opportunities for nature-based interventions to address these needs. A limitation of this study was the small and homogeneous sample. The data were limited to self-reported data, and there may be potential for selection bias. The cross-sectional design of this study also limits assertions of causality. In addition, the majority of study participants were recruited from one VSO, and the use of convenience and snowball sampling may have restricted participation to veterans particularly interested in sharing their health experiences. The sample was also homogeneous in terms of gender, race, education, and income levels. These demographic differences could all have been confounding variables given the variability in military experiences and cultural values across different services. This may have led to a lack of diverse perspectives being shared.
Implications for OT
Findings from this study highlight the need for targeted OT interventions that support mental health, social engagement, and nature-based activities tailored to veterans’ unique experiences. Rural veterans face significant barriers to consistent mental health care. OT practitioners can address these gaps by advocating for telehealth and mobile mental health services, community programs that offer veterans supportive, controlled environments for socializing, encouraging regular engagement in therapeutic outdoor activities. Finally, integrating OT services into community-based settings and non-VA facilities commonly used by rural veterans can increase accessibility.
Conclusion
This study sheds light on the distinctive health challenges and needs of rural veterans, identifying key opportunities for OT interventions. The CBPR approach used in this study was essential in amplifying rural veterans’ perspectives, ensuring that their insights directly informed the identification of priority health needs and relevant intervention approaches. By prioritizing veterans’ voices and lived experiences, CBPR-driven research can strengthen the relevance and impact of OT services in addressing veterans’ health and well-being.
Footnotes
Authors’ Note
This study received ethical approval by the Rocky Mountain College Institutional Review Board (IRB) Protocol #: IRB-SP23-021
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.