
Abstract
Limited literature exists investigating the relationship between sensory processing and complex regional pain syndrome (CRPS). This study aimed to identify and understand sensory processing patterns for people with CRPS. This study employs a cross-sectional survey design. Participants were a sample of convenience and completed two electronic surveys: a demographic survey and the Adolescent/Adult Sensory Profile (AASP). More than 90% of participants (n=62) were female and White or White in combination. Participants 18 to 64 perceived sensory experiences in subtypes of low registration, sensory sensitivity, and sensation avoiding, while they demonstrated lower perceived levels of sensation seeking. Participants above 65 reported experiencing sensory sensitivity and sensation avoiding “much more than most people.” There were patterns between sensory sensitivity to low registration and sensation avoiding, regardless of age. Above 65, low registration and sensation avoiding were significantly related. Patterns exist within sensory processing subtypes in people with CRPS.
Plain Language Summary
Little is known about how sensory systems may or may not increase someone’s likelihood to get complex regional pain syndrome (CRPS) after an injury. Likewise, it is unknown if sensory systems impact recovery. It is thought that there is a connection between people’s sensory systems and how CRPS looks in each person. We wanted to see what sensory patterns were reported by people diagnosed with CRPS. Two surveys were sent to people belonging to a CRPS support organization. Differences in sensory patterns were identified in people 18 to 64 and above 65. Possible ways this influences CRPS are discussed. Ideas for future research are talked about based on what was found.
Complex regional pain syndrome (CRPS) is a condition characterized by pain that is disproportionate to an inciting peripheral limb trauma (Harden et al., 2010; Veldman et al., 1993). CRPS is commonly thought of as a type of chronic pain, but this is an underrepresentation of the systemic changes throughout the body. People diagnosed with CRPS present with varied symptoms, including sensory and somatosensory changes (Di Pietro et al., 2013). People may experience various vasomotor, sudomotor, sensory, and autonomic abnormalities (Harden et al., 1999; Perez et al., 2010). Common symptoms include burning pain, edema, changes in skin temperature, changes in skin color, changes in skin appearance, trophic changes in hair and nail growth, tremors, decreased strength and range of motion, and/or dystonia of the affected region (Goebel et al., 2018; Harden et al., 2010).
The etiology of CRPS is multifaceted and not yet fully understood. Neurologic changes in the central and peripheral nervous systems occur as the nervous system adapts following an injury (Birklein & Dimova, 2017; De Schoenmacker et al., 2023). Central and peripheral sensitization causes an increase in responsiveness to pain, which may contribute to the varied presentation (Birklein & Dimova, 2017).
There is ample evidence to support that sensory changes occur with a CRPS diagnosis (De Schoenmacker et al., 2023; Huge et al., 2008, 2011; Rebhorn et al., 2022). According to the most common diagnostic criteria, experiencing hyperalgesia or allodynia is categorized as both a symptom and sign of CRPS and there is a gap in the literature on how this sensory input is processed (Birklein & Dimova, 2017; Goebel et al., 2021; Harden et al., 2010, 2022). Sensory processing and integration have not been extensively investigated in the CRPS population, despite varied sensory changes being included in the Budapest Criteria and Valencia Criteria for the diagnosis of CRPS (Goebel et al., 2021; Harden et al., 2010).
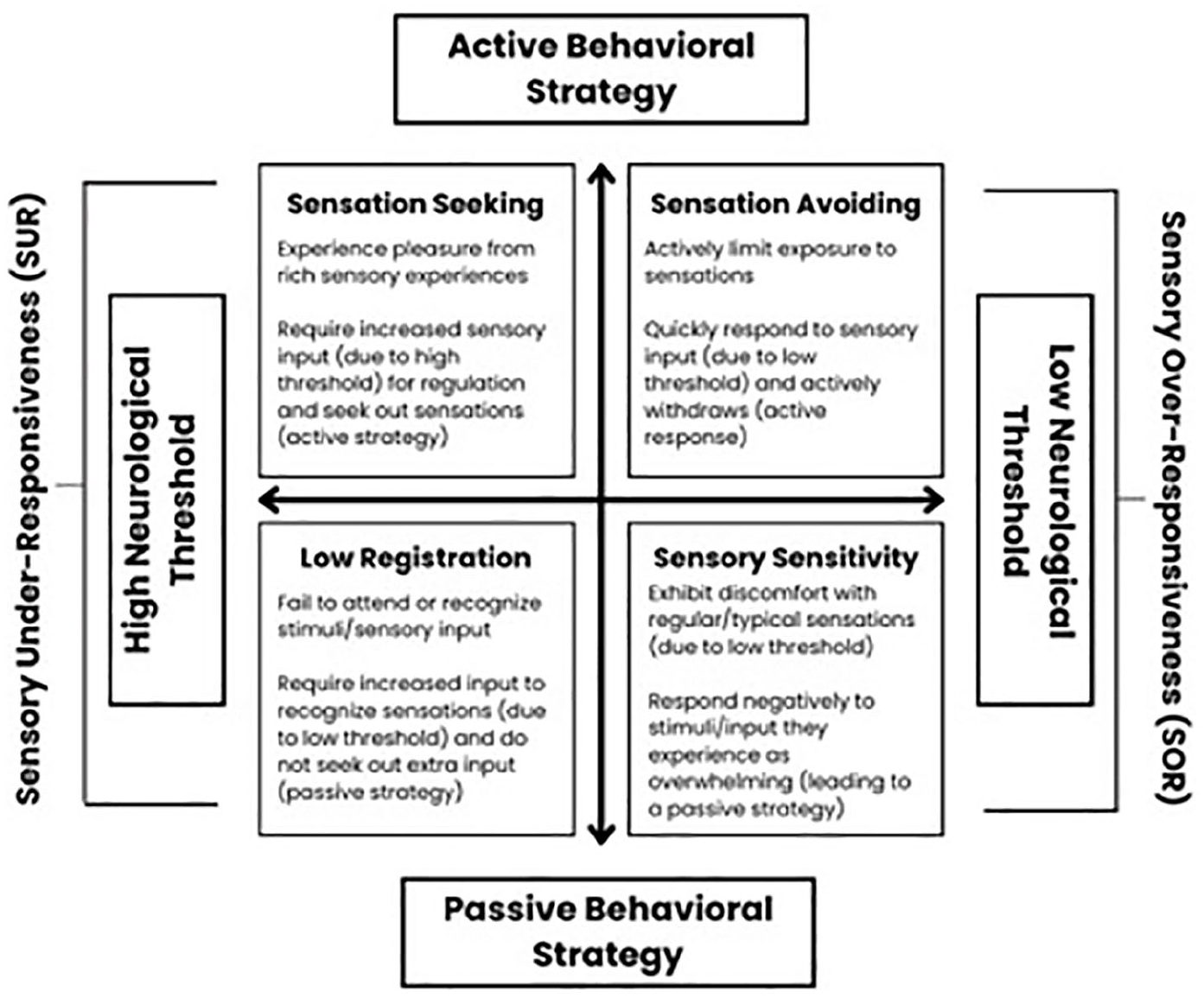
Sensory processing describes a person’s ability to register, modulate, and organize sensory information to create an adaptive response (Humphry, 2002). Individuals experience different neurological thresholds for sensory information and respond in varied behavioral strategies (Engel-Yeger & Dunn, 2011). The four subtypes (i.e., sensation avoiding, sensory sensitivity, sensation seeking, and low registration) are labeled from Dunn’s Model of Sensory Processing and fall under the category of sensory modulation disorder (SMD) (Dunn, 1997; Dunn & Westman, 1997). SMD is a subtype of sensory processing disorder (SPD) that interferes with sensory processing either through single or multiple sensory systems. People with sensory over-responsivity (SOR) experience abnormal sensations in response to an otherwise non-painful stimulus (Bar-Shalita et al., 2019). The subtypes of sensory sensitivity and sensation avoidance fall within the umbrella of SOR, whereas low registration and sensation seeking fall within sensory under-responsiveness (SUR) (Bar-Shalita et al., 2018). People with over-responsivity exhibit behavioral trends (e.g., avoidance of sensations) similar to those who are diagnosed with pain disorders (Engel-Yeger & Dunn, 2011). It is known that SMD can significantly impact a person’s occupational performance (Schoen et al., 2021). Dunn’s Model of Sensory Processing builds upon the sensory integration (SI) frame of reference and notes that sensory modulation lays the foundation for successful participation in occupations (Schaaf et al., 2010). Pain can also disrupt a person’s occupational participation (Nielsen et al., 2022).
There is limited research investigating the relationship between CRPS and sensory processing. Study findings by Bar-Shalita et al. (2018) found that 34% of participants with CRPS had scores associated with SMD, compared with 12.8% of healthy controls. Bar-Shalita et al. (2018) purport that SUR may be a potential risk factor in the development of CRPS, and screening for SMD after an injury may help identify those at risk. Research on other pain disorders has highlighted that for individuals with fibromyalgia, specifically the subdomains of smell, vision, and touch (Dorris et al., 2022).
Auditory perception (Tun & Wingfield, 1999), taste and smell (Schiffman, 1997), vision impairment (Branch et al., 1989), and proprioceptive changes occur as people age (Landelle et al., 2021; Saenen et al., 2023). These changes can influence alterations in the somatosensory cortex (Landelle et al., 2021). Alterations in the somatosensory cortex can influence responses to nociceptive input (Karunakaran et al., 2021). Given that the average age of diagnosis for CRPS is 46 (Sandroni et al., 2003), it is possible that age might be an additional confounding factor for sensory processing changes and CRPS.
Given the broad changes in sensory perception and sensory representation in the somatosensory cortex experienced with CRPS (Echalier et al., 2020; Sobeeh et al., 2023; Swart et al., 2009) and the theoretical foundations of the SI frame of reference (Dunn, 1997), it is hypothesized that there may be distinct patterns of sensory processing subtypes expressed in CRPS and these patterns may differ based on age. This study aims to identify and understand patterns of sensory processing subtypes for individuals with CRPS. The primary objective of this study is to understand sensory processing experiences in people diagnosed with CRPS to serve as a foundation for future research.
Method
This study employs a cross-sectional survey design. Ethics approval was obtained from Northern Arizona University, and informed consent was obtained from all participants. The Checklist for Reporting Results of Internet E-Surveys (CHERRIES) was adhered to in the methodology, with the exception of collecting response rates (Eysenbach, 2004).
Participants
Participants were a sample of convenience, recruited through email, newsletter, and Facebook post distributed by the Reflex Sympathetic Dystrophy Syndrome Association (RSDSA). Snowball sampling occurred when information about the study was shared. Inclusion criteria included being 18 and older, a self-identified diagnosis of CRPS, and upper extremity affected. This study included only upper extremities in hopes of capturing data more commonly seen in an occupational therapy clinical setting within the United States. Exclusion criteria included participants below 18, participants without a self-identified diagnosis of CRPS, and participants with self-reported CRPS of the lower extremity. Participants did not receive an incentive to participate.
Procedures
Two sequential surveys were sent to listserv members of the RSDSA. Both were electronic created using a secure Qualtrics Platform (see the appendix). The first survey collected demographic data, including length of diagnosis, details about their diagnosis to improve researchers’ confidence in a CRPS diagnosis, comorbidities, treatments participants had received in the past, sleep patterns, and perceived quality of life. No questions were mandatory or force-filled; all questions were voluntary. Participants were able to review or change their answers through a back button if needed. Face validity was established by reviewing the survey with therapists who have treated people with CRPS. Changes were made incorporating alternative language to minimize potential acquiescence bias, and clearer definitions were incorporated. Second, a psychometrician statistician was consulted to ensure clarity and minimize the likelihood of leading or confusing questions. The final iteration of this first survey in Qualtrics was reviewed by all researchers and the psychometrician statistician prior to distribution.
The second subsequent survey was the Adolescent/Adult Sensory Profile (AASP). The AASP has been used to identify the sensory profiles of individuals with chronic pain conditions and has appropriate internal consistency and construct validity (Gräper et al., 2022). Although the AASP has not yet been validated with individuals with CRPS, it was chosen for this study because pain is a hallmark symptom of CRPS and this is an association between both pain perception and sensory defensiveness and sensory processing and pain catastrophizing in adults (Engel-Yegar & Dunn, 2011; Kinnealey & Fuiek, 1999).
The AASP is a 60-item questionnaire with questions related to sensory information: auditory, touch, vision, taste and smell, and movement (Brown & Dunn, 2002). Each item is coded into four subtypes: sensation seeking, low registration, sensory sensitivity, and sensation avoiding (Brown & Dunn, 2002). Individuals are scored on scale from much less than most people to much more than most people for the four subtypes (Brown & Dunn, 2002). The AASP is a valid and reliable assessment for all four subtypes of SMD in adult populations (Brown et al., 2001).
The AASP is not available electronically, and all necessary permissions were granted from Pearson Assessments to proceed with the conversion to an electronic format in February 2022. No alterations were made to the original paper assessment when converted to the Qualtrics Platform. To control for the limited licenses granted by Pearson, the AASP was emailed to the participant’s designated email address given in the first survey. Participant email addresses were recorded from the first survey, and the AASP was sent directly to this recorded email. Multiple entries by the same individual were controlled by sending only the second survey to the primary email address, with responses being matched one-to-one to the first survey to create a complete data set unique to that particular individual. Both surveys were tested via computer and cell phone for usability, in accordance with the CHERRIES statement for online surveys (Eysenbach, 2004). Data collection took place from May 4, 2022, to June 1, 2022.
Data Analysis
Data were merged from both surveys and coded using participants’ individual identification numbers. After incomplete data sets were removed, participants who did not complete both surveys were removed, those who met exclusion criteria (e.g., self-report of a lower extremity injury) were eliminated, and the analytic procedures were based on 62 participants.
The scoring criteria for the AASP vary for ages 18 to 64 and above 65 years of age (Brown & Dunn, 2002), and data were stratified based on these age categories. Scoring criteria vary for these age categories because during instrument development, it was discovered that older adults scored higher for the subtype of low registration and scored lower for the subtype of sensation seeking when compared with 18- to 64-year-olds (Brown & Dunn, 2002). Following Brown et al. (2001), raw data were scored into the four subtype summary scores: low registration, sensation seeking, sensory sensitivity, and sensation avoiding. The subtype summary scores were compared with a scale of normal distribution and assigned a pattern of either: much less than most people, less than most people, similar to most people, more than most people, and/or much more than most people (Brown & Dunn, 2002). Independent variables obtained from the initial survey were age, self-identified gender, and race. Due to the majority of participants being women and White or White in combination, only age was used for analysis. The dependent variables were the AASP subscale summary scores. Means and standard deviations were calculated for continuous variables, while medians and interquartile ranges were constructed for categorical data. Due to the ordinal nature of the outcome variables, non-parametric analyses were employed. Spearman rho (rs) was calculated to determine the relationship between the subscale summary scores. Finally, Cronbach’s alpha (α) was used as an estimate of internal reliability for the items within each subscale. Results of .90 or greater are considered excellent reliability, .80 to .89 is good, .70 to .79 is acceptable, .60 to .69 is questionable, and .59 or below is poor (George & Mallery, 2003). Data merging and all statistical analyses were performed in SPSS 29.0 with an alpha level of .05.
Post Hoc Analysis
For this exploratory study, a post hoc analysis using G*Power 3.1 revealed with 62 participants, using a large effect size of 0.35, with .05 alpha error probability, this exploratory research was adequately powered at 83%.
Results
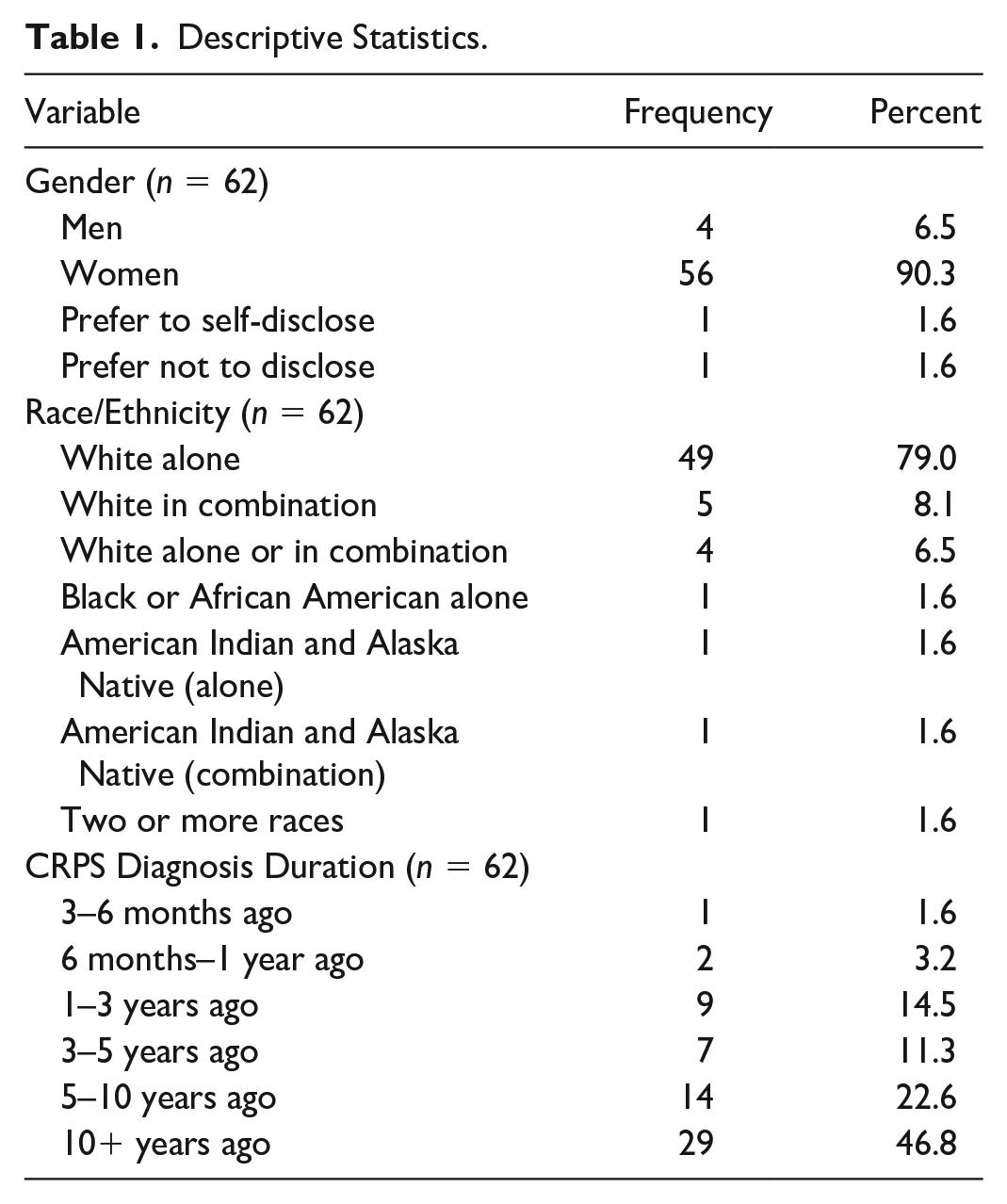
On average, participants were 53.5 ± 13.6 years of age. Participants who identified as female accounted for 90.3% of the sample, and participants identifying as White or White in combination with another race/ethnicity were 93.6% (Table 1).
Descriptive Statistics.
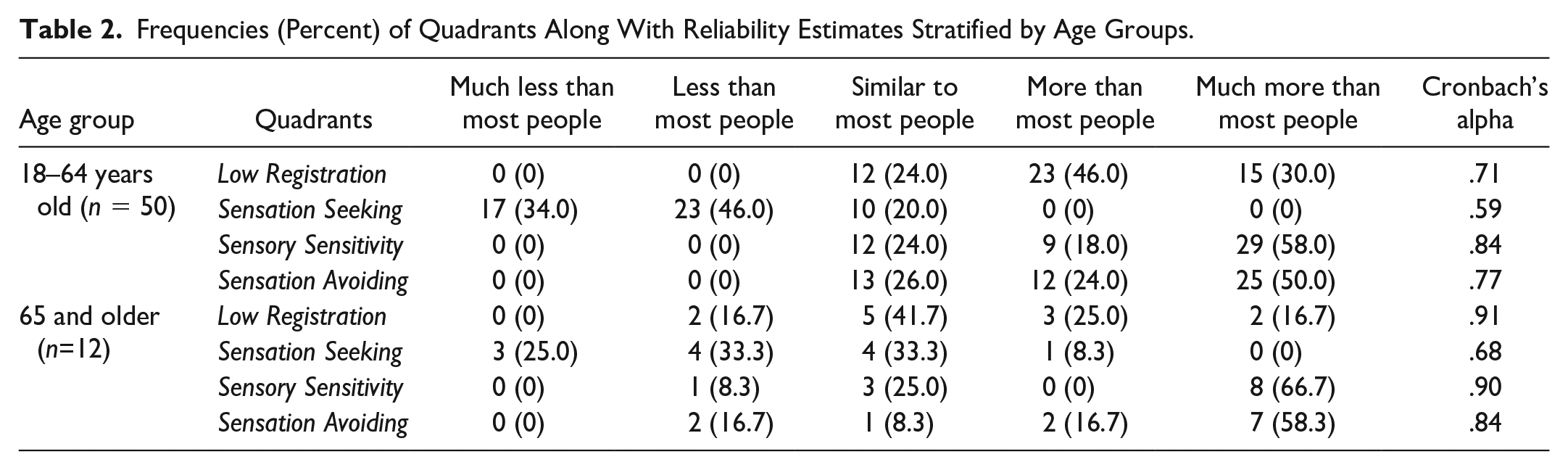
From the conversion of the raw scores to the subscales on the AASP, ranges start with “much less than most people” to “much more than most people” on a 5-point Likert-type scale. Participants’ responses were compared with each other to identify the frequency of scores. As seen in Table 2, those in the younger age category (18–64) more frequently endorsed “much more than most people” for low registration, sensory sensitivity, and sensation avoiding, whereas “less than most people” for the sensation seeking. For those 65 years of age and older, more frequently endorsed “much more than most people” for sensory sensitivity and sensation avoiding, while “similar to most people” for low registration and equally between “less than most people” and “similar to most people” for sensation seeking. Sensory sensitivity had the highest level of reliability for those 18 to 64 while low registration was for those 65 and older.
Frequencies (Percent) of Quadrants Along With Reliability Estimates Stratified by Age Groups.
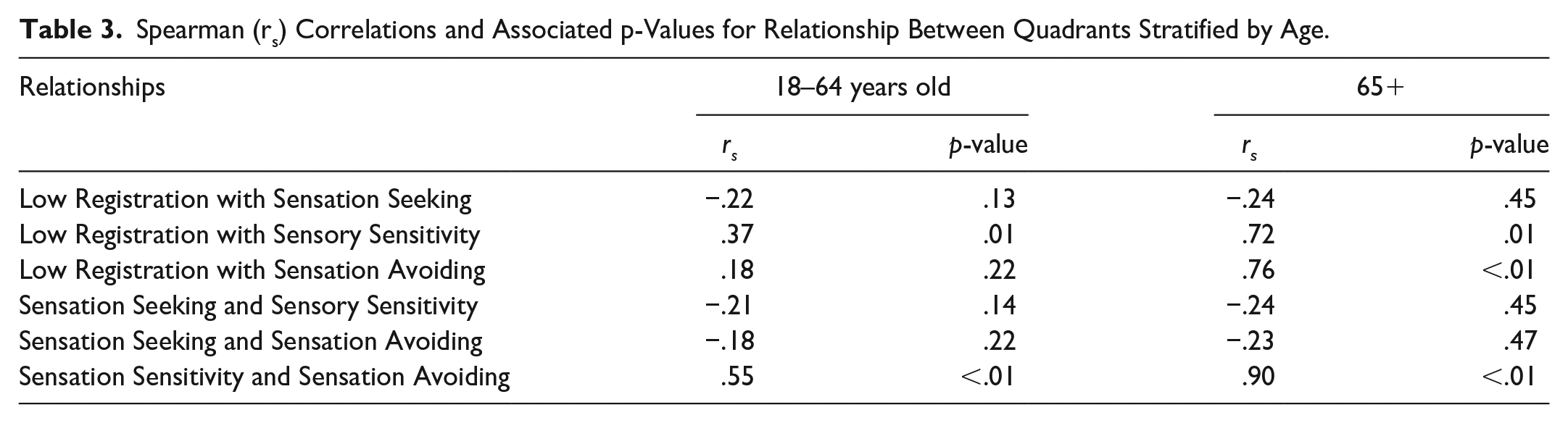
Results from the Spearman correlations show that statistically significant relationships exist between sensory sensitivity with both low registration along with sensation avoiding for the entire sample, regardless of age (Table 3). For the older population, low registration and sensation avoiding were significantly related (p = .01).
Spearman (rs) Correlations and Associated p-Values for Relationship Between Quadrants Stratified by Age.
Discussion
This study investigated sensory processing patterns in individuals with CRPS. The hypothesis for this study was that individuals with CRPS would record their sensory experiences in similar patterns and that these patterns may differ based on age. Results showed a trend toward SOR in this study population, including the following patterns: (a) individuals with self-identified CRPS aged 18 to 64 endorsed experiencing low registration, sensory sensitivity, and sensation avoiding “much more than most people” and sensation seeking “much less than most people,” and (b) individuals with self-identified CRPS 65 and older experienced sensory sensitivity and sensation avoiding “much more than most people” while they experienced low registration “similar to most people” and sensation seeking equally split between “less than most people” and “similar to most people.” Relationships were found between sensory sensitivity and low registration and between sensory sensitivity and sensation avoiding regardless of age. It is possible that these subtypes are associated, given the active behavior strategy and passive behavioral strategy used by the subtypes (Figure 1). In the older population, a relationship was identified between low registration and sensation avoiding.
Sensory Processing Patterns.
This study’s results demonstrate that individuals with CRPS may trend toward SOR. Given that one of the diagnostic criteria for CRPS involves pain disproportionate to an injury, it is not surprising that individuals who identify as having CRPS describe an over-responsive reaction to other types of sensory stimulation. Interestingly, Engel-Yeger et al. (2013) found that individuals with post-traumatic stress symptoms will fluctuate between sensory sensitivity, sensation avoiding, and low registration and concluded that hypersensitivity and low registration may be related in individuals with post-traumatic stress symptoms. Post-traumatic stress disorder also occurs with more frequency in those diagnosed with CRPS versus the general population (Speck et al., 2017).
Congruent with current study results, Bar-Shalita et al. (2018) illustrated that individuals with SMD may be a risk factor in developing CRPS compared with those without SMD, given the trend toward SOR. This risk is 2.68 times higher for individuals with SOR and 8.21 times higher for individuals with SUR (Bar-Shalita et al., 2018). Future research may be indicated investigating SMD as a precipitating or maintaining factor for CRPS.
Patterns of sensation avoiding and sensation seeking was also noted. This may be an interesting area of future research further breaking down which types of sensations are being both sought and avoided. Furthermore, it is worth noting that the avoidance of sensation may stem from mechanisms outside of those assessed in the AASP. Legrain et al. (2012) suggest spatial perception deficiencies, may play a role in defense mechanisms limiting use of a painful limb. Further research is needed to better understand the neglect-like symptoms associated with CRPS in relation to sensory processing patterns (Legrain et al., 2012).
Finally, the relationship between low registration and sensation avoiding in older adults was not anticipated. Given that during the development of the AASP, researchers found that older adults scored higher on lower registration and lower on sensory sensitivity (Brown & Dunn, 2002), this was the hypothesized pattern. The pattern found by the current research leads one to posit that there may be a sensory processing pattern change toward an active behavioral strategy versus a passive behavioral strategy for individuals with CRPS. Further research specifically focused on an older adult population and their sensory process changes may allow for improved interventions for this population.
Sensory Processing and Pain
It is unknown if the participant responses on the AASP would have been the same prior to their precipitating CRPS injury. However, it is known that individuals with CRPS experience sensory, motor, and autonomic information in a disrupted pattern influenced by both central and peripheral mechanisms (Halicka et al., 2020). Further supporting the study hypothesis is the experience that hypersensitivity and avoidance of temperature or other tactile stimuli, movement, and pain intensifiers are commonly seen in patients with CRPS (Goebel et al., 2018; Ten Brink et al., 2020).
Rommel et al. (2001) found that 66% to 69% of participants with CRPS experienced sensory loss or sensory gain; additionally, a generalized sensory change was significantly correlated with a longer duration of impairment. Health care professionals could use information gathered from the AASP to identify potential factors that exacerbate pain and develop strategies to reduce exposure to those contexts. Gathered information may help guide interventions and treatment approaches and establish environmental adaptations to support functional performance. A narrative review by Packham and Holly (2018) concluded that no single treatment approach should be used with all people with CRPS. Grading activities while controlling pain and fear avoidance is recommended, as is graded thermal stimulation (Packham and Holly, 2018). Packham and Holly (2018) propose that sensory input, in particular, tactile input, has varied effects on people with CRPS, and the findings from this study may be an additional tool to help identify who may respond or react to sensory input and provide an opportunity for unique approaches to care. The use of sensory modulation strategies, like graded sensory stimulation, during functional rehabilitation may allow providers to help integrate specific and targeted functional daily activities in their own time and life contexts (Engel-Yeger & Dunn, 2011).
Frith et al. (2000) suggest that our perception of sensory input is the largest contributing factor to how we experience sensations and motor responses. McCabe et al. (2005) additionally proposed that the impaired efferent neurons relay the perceived message that movement will lead to pain, thus contributing to an altered perception of sensations by some individuals with CRPS. Furthermore, Dance et al. (2021) suggest sensory imagery and sensory sensitivity are related; specifically, aphantasics (people unable to create mental images) have lower imagery and sensitivity (Dance et al. 2021). One could then posit that graded motor imagery, a known effective intervention in some people with CRPS, may be less effective for individuals with low registration (Bowering et al., 2013). Understanding the relationship between sensory processing and pain perception may further influence intervention approaches.
Given the results of this study, it could be speculated that this altered perception extends to all areas of sensory processing, as evidenced by the percentages of participants that illustrated their sensory processing experiences were outside of the “similar to most people” pattern (Table 2). Unfortunately, the current study could not determine in what way sensory processing may influence CRPS. It is possible that individuals with SMD or altered sensory processing experience CRPS differently, are predisposed to CRPS, or that sensory processing changes occur in relation to the CRPS. Further research is warranted.
Limitations
This study has limitations. As a cross-sectional survey design, participants self-identified as having CRPS, potentially introducing self-selection bias. Although this may challenge the external validity of this study and threaten the generalizability of findings across the CRPS population, the conclusions from this study highlight the need for further research in clinical contexts. In addition, the low response rate may introduce sampling bias. As having a CRPS diagnosis was self-reported, clinical verification of CRPS diagnosis using the Budapest or Valencia Criteria as part of the inclusion criteria may increase the generalizability of findings in future research (Goebel et al., 2021; Harden et al., 2010). Moreover, the inclusion criteria for this study were selective to only the upper extremity, which limited the sample size. Despite a small sample size, the post hoc analysis revealed the sample was sufficient for statistical analysis. A post hoc analysis, however, increases the risk for Type I error. Despite this limitation, the exploratory findings in this research present information that can be expanded on in future clinical studies. Finally, additional analysis by duration of pain or CRPS symptomatology could have strengthened this study, as disease presentation may vary.
Areas of Future Research
This study highlights several areas for future research that can be used to guide clinical treatment for people experiencing CRPS. Expanding the inclusion criteria to include CRPS of all extremities in future studies related would capture a more representative population of those with CRPS. In addition, it would be beneficial to investigate the psychometric properties of the AASP for adults, specifically in the CRPS population. In addition, as Engel-Yeager and Dunn (2011) found an association in typical adults between sensory processing patterns and pain using the Pain Catastrophizing Scale, a measure recommended by the COMPACT (Grieve et al., 2017), future research may investigate further associations within sensory processing in the CRPS population. Finally, investigating the relationship of CRPS with sensory processing as related to occupational engagement or participation could contribute valuable information to the profession.
Implications for Occupational Therapy Practice
Findings suggest that understanding a person’s unique sensory profile may help to guide more individualized treatment interventions in persons with CRPS. In addition, the results of this study corroborate with a study by Bar-Shalita et al. (2018) that SUR or SOR may be a risk factor in the development of CRPS. Because it is unknown if SMD predisposes a person to CRPS or if there are implications in its progression, completing a sensory screening prior to surgery or rehabilitation or immediately following an injury may serve as a useful tool to identify those who could potentially develop CRPS or help mitigate its perpetuation. A sensory screen may help guide treatment choices.
The use of a sensory processing evaluation throughout the treatment process may also provide information on recovery, sensory process changes, and efficacy of interventions, as it is unknown if sensory changes are a temporary state or an individual trait. These underlying potential sensory processing difficulties for individuals may impact participation in traditional multidisciplinary interventions, as pain can limit occupational performance and engagement (MacLean et al., 2022). Occupational therapists have a foundational understanding of sensory processing to substantiate potential interventions for CRPS, given these study results.
Occupational therapists have a foundational understanding of sensory processing as it relates to interactions within the environment, adaptive responses, and occupational participation. Given this unique lens on interactions between sensory stimuli, neural processes, and adaptive responses, occupational therapists can play a critical role in substantiating potential interventions for CRPS based on unique sensory profiles and sensory processing patterns, given these study results. Further research examining the patterns and relationships between sensory processing and SMD in individuals with CRPS within clinical contexts is warranted.
Conclusion
Patterns exist between sensory processing subtypes in people diagnosed with CRPS. Participants, on average, scored outside of the “norm” for all four subscales on the AASP. A positive relationship exists between low registration and sensory sensitivity, low regulation and sensory avoiding, sensory sensitivity and sensation avoiding, and sensory avoiding and sensory seeking. There are many aspects of sensory processing mechanisms that are yet to be understood, and the objectives of this research and future research remain a work in progress.
Footnotes
Appendix
Acknowledgements
The authors gratefully acknowledge the Reflex Sympathetic Dystrophy Association (RSDSA) for assisting with survey distribution to make this study possible.
Author Contributions
All authors contributed to data collection and the manuscript writing. Statistical analysis was completed by the Southwest Health Equity Research Collaborative at Northern Arizona University and acknowledged in the funding section.
Research Ethics Section and Patient Consent
Institutional Review Board approval was granted by Northern Arizona University. Approval reference number: 1742880-6
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the use of the services and facilities of the Southwest Health Equity Research Collaborative at Northern Arizona University (U54MD012388) and seed grant funding received from Northern Arizona University College of Health and Human Services.