
Abstract
Social frailty (SF) involves reduced social participation, roles, and support, and it is associated with adverse health outcomes. However, the relationship between SF and occupational participation, particularly hobbies, remains underexplored. We examined the association between SF and occupational participation, particularly hobbies, among older adults. A cross-sectional survey of 1,000 older adults in Japan (mean age: 74.08 ± 5.48 years) was conducted online. Participants were classified as robust, pre-SF (PSF), or SF using Makizako’s five-item criteria. Occupational participation was assessed using the Self-Completed Occupational Performance Index. Hobby categories and their frequencies were also recorded. Occupational participation was lower in SF than in PSF and robust. Participation in productive activities was negatively associated with PSF and SF, while leisure activities and cultural and artistic hobbies were negatively associated with SF. Occupational therapy should emphasize occupational participation and hobby engagement to help older adults cope with social frailty.
Plain Language Summary
As people age, they often face health issues and challenges in maintaining social connections. “Social frailty” is a term used when a person becomes less socially active or loses contact with their friends and community. This condition can lead to feelings of loneliness, isolation, and depression, and may increase the risk of future health issues or the need for long-term nursing care. This study investigated whether engaging in meaningful leisure activities, specifically hobbies, could help prevent social frailty among older adults in Japan. We conducted an online survey of 1,000 people aged 65 years or older. The current results indicate that individuals experiencing social frailty were less likely to engage in leisure and productive activities compared to their healthier counterparts. Participation in cultural and artistic hobbies—such as music, painting, and crafts—was associated with lower odds of social frailty. Overall, this study suggests that engaging in fulfilling leisure activities, particularly hobbies, can help older adults maintain social participation and enhance their overall well-being, potentially delaying or preventing the need for long-term care. Community-based programs that encourage participation in hobbies may promote healthy aging.
Introduction
In recent years, with the global aging of populations, frailty has garnered increasing attention as a key concern for older adults. Social frailty (SF), a frailty phenotype, is characterized by difficulties in engaging in social activities and participation, often resulting from social withdrawal or an inactive lifestyle (Bunt et al., 2017). SF encompasses different facets, including social isolation, loneliness, declining abilities, willingness, opportunities for social participation, loss of social roles, and insufficient social support (Yamada & Arai, 2023). Reduced outings and limited interactions with family, friends, and the community are key features of SF, resulting in social isolation and loneliness (Pan, 2024). The decline in opportunities to help others and the feeling of being valued by them are particularly linked to SF progression (Yamada & Arai, 2023). This lack of social engagement is closely associated with reduced life satisfaction, poorer health-related quality of life, adverse health outcomes, and reduced healthy life expectancy (Garre-Olmo et al., 2013; H. Ko & Jung, 2021; Y. Ko & Lee, 2022; Makizako et al., 2018).
Japan is experiencing a rapidly aging society with a declining birthrate, characterized by an increasing number of older households and care-dependent older adults (Cabinet Office, 2024). From a global perspective, social isolation in later life is particularly salient in Japan (M. Saito et al., 2021), making social engagement crucial for fostering mutual support within communities and promoting both a sense of purpose and functional independence in daily life.
Occupational participation—the ability to engage in meaningful activities across leisure, productivity, and self-care domains, maintain balance among them, and perform them satisfactorily (Imai & Saito, 2010)—may be particularly relevant for preventing SF. Takeda and Tanimura (2021) demonstrated that reduced occupational participation creates negative cycles with pre-physical frailty and poor psychological status among community-dwelling older adults. Although their study focused on physical frailty, the theoretical framework suggests that similar mechanisms may apply to SF, as meaningful activities significantly enhance social participation and reduce isolation (Papageorgiou et al., 2016). Similarly, a lifestyle re-design program demonstrated benefits in promoting mental health, leisure activities, and social participation among older adults (Levasseur et al., 2019), supporting the potential protective role of occupational participation against SF.
According to the Ministry of Internal Affairs and Communications (2021), older Japanese adults have approximately 9 hours per day outside of self-care, sleep, and productive activities (e.g., work, volunteering, caregiving, and housework). However, approximately 8 hours are spent on passive, home-based activities, such as watching television or resting. This indicates that leisure time is spent on passive or non-productive pursuits. Toepoel (2013) reported that positive activities, such as reading, handicrafts, and cultural activities, were significantly correlated with the strengthening of social boundaries, whereas passive activities did not exhibit the same relationships. This finding suggests that a lack of active leisure activities, such as hobbies, may limit social participation. Leisure activities promote social interaction and health-related quality of life, with hobbies linked to social confidence (Zheng et al., 2022). Engaging in two or more hobbies and social groups reduces the risk of decline in social functioning, healthy lifestyle habits, and cognitive abilities (Abe et al., 2022). Therefore, incorporating hobby-like activities into occupational therapy can reduce feelings of loneliness and create opportunities for social interaction (Col et al., 2022; Levasseur et al., 2019; Pitkala et al., 2011). However, the direct impact of occupational participation and hobbies on SF remains unclear.
In this study, “leisure activities” denotes both passive and active pursuits, whereas “hobbies” refer to sustained, self-chosen, purposive activities that require active engagement. We focused on hobbies because such active engagement is more likely to foster social ties and role acquisition than passive leisure, and is directly relevant to SF. This cross-sectional study aimed to (a) explore the characteristics and prevalence of SF, (b) examine the status of occupational participation and hobby engagement in SF, and (c) investigate associations between SF and both occupational participation and hobby-related factors (presence, number, types, and frequency-weighted scores) in community-dwelling older Japanese adults. Our findings are expected to contribute to developing approaches for supporting independent living and preventing long-term care by incorporating strategies to enhance social participation.
Method
Survey Design and Participants
This cross-sectional study involved older Japanese adults registered with the internet survey company Cross Marketing Group Inc. (Tokyo, Japan). Recruitment began in August 2023 and concluded approximately 1 month later. Participants completed an anonymous questionnaire online using a personal computer, smartphone, or tablet. The inclusion criteria for this study were as follows: (a) participants answered all questions; (b) they were independent in their activities of daily living (ADL), which include basic self-care such as eating, toileting, and bathing; and, optionally, (c) if applicable, they were eligible for the Long-term Care Prevention and Comprehensive Support Program in Japan’s long-term care insurance system. This optional criterion ensured that older adults engaged in municipal prevention services were not inadvertently excluded while keeping the analytic cohort independent in ADL. The exclusion criteria were (a) individuals certified as needing long-term care or support under nursing care insurance in Japan, and (b) individuals requiring assistance with their ADLs. Based on the power analysis (see the Statistical analysis section below), we aimed to collect a total of 1,000 participants with an equal distribution across sex and age groups (65–69, 70–74, 75–79, and 80–84 years). To achieve this, we continued recruiting respondents until we reached the target sample size using a stratified sampling strategy, resulting in a total of 1,298 participants enrolled. During this process, we excluded 212 individuals based on the exclusion criteria, and an additional 86 were removed due to missing data. Finally, 1,000 individuals were selected to ensure equal distribution across strata. Ethics approval was obtained from the institutional ethics committee, and the study adhered to the principles outlined in the Declaration of Helsinki.
Measures
Assessment of SF
SF was evaluated using Makizako’s five criteria (Makizako et al., 2015), which comprised five items: (a) going out less frequently than last year (yes), (b) visiting friends sometimes (no), (c) feeling like helping friends or family (no), (d) living alone (yes), and (e) talking with someone every day (no). Participants were categorized into three groups based on the outcomes of Makizako’s five criteria, with two or more characteristics classified as SF, one characteristic as pre-SF (PSF), and none as robust.
The Quality of Occupational Participation
The quality of occupational participation was evaluated using the Self-completed Occupational Performance Index (SOPI), which was developed to measure the quality of individuals’ involvement in meaningful daily activities (Imai & Saito, 2010). The SOPI comprises nine items: “occupational control,” “occupational balance,” and “satisfaction of performance” in the following three domains: “leisure (leisure activities including creative activities, outdoor activities, gaming, sports, travel, conversation with friends, social activities),” “productivity (socioeconomically productive activities including paid work, housework, child care, caregiving, volunteering, and study),” and “self-care (self-care and daily life activities such as personal care, shopping, using financial institutions, and transportation by car or public transit).” Participants rated their satisfaction with “occupational control,” “occupational balance,” and “satisfaction of performance” in each domain on a five-point scale (5: very satisfied, 1: hardly satisfied). The productivity domain encompasses both paid work or employment and unpaid activities that contribute socially and economically (e.g., housework, childcare, caregiving, volunteering, and studying). We calculated the score for each domain and the total score, from which the raw scores were summed and converted to a 100-point scale.
Kihon Checklist
We used a comprehensive self-reported health assessment tool, the Kihon Checklist (25 items), developed by the Japanese Ministry of Health, Labor, and Welfare, to evaluate functional independence in daily life. The Kihon Checklist was designed to identify potential risks to functional independence that individuals aged 65 years or older face in their daily lives, as well as to help prevent long-term frailty and promote healthy aging. We assessed physical decline, malnutrition, oral hypofunction, cognitive decline, and depressive symptoms using established criteria for each.
Hobby Categories and Frequencies
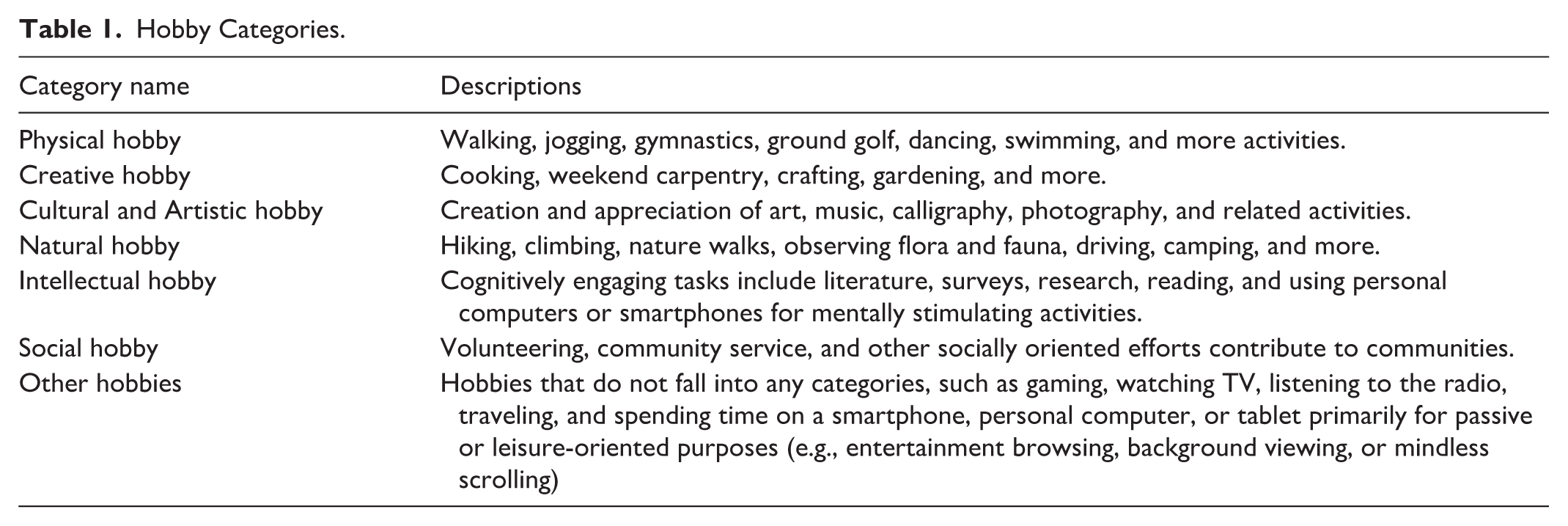
Participants were asked about their engagement in hobbies. This is based on a previous study that identified 11 categories from 58 potential leisure activities (Iwasa & Yoshida, 2018). These were reorganized into seven categories: (a) Physical, (b) Creative, (c) Cultural and Artistic, (d) Natural, (e) Intellectual, (f) Social, and (e) Other Hobbies (see detailed descriptions in Table 1). Participants were required to select up to three hobbies from these categories, along with the frequency of their participation in these hobbies (5: nearly every day, 1: several times a year).
Hobby Categories.
The significance of a particular hobby in one’s daily routine appeared to vary between individuals who engaged in that hobby alone and those who participated in three different hobbies, including that hobby. Therefore, we calculated the weighted hobby scores for each category using the formula below:

hc: the hobby category score, Nh: the number of hobbies, and fc: the frequency of the hobby category. The maximum hobby score is 15 points.
The total hobby score is given as follows:

H: the total hobby score, and the summation runs over all hobby categories. By construction, 0 < H ≤ 15, regardless of the number of hobbies (Nh) within the range of one to three. The maximum (H = 15) occurs when all selected categories are practiced “nearly every day,” fc = 5; for example, three hobbies at 5 → 5 + 5 + 5 = 15; two at 5 → (3/2) × 5 + (3/2) × 5 = 15; one at 5 → 3 × 5 = 15.
Other Variables
Participants provided demographic information, including factors such as sex, age, marital status (married or unmarried), whether they have children (present, living apart, or living together), educational attainment (ranging from elementary school to graduate school, with “one” indicating elementary school and “six” indicating graduate school), current financial situation (ranging from “one”, indicating significant economic difficulties, to “five”, indicating a very comfortable financial position), and employment status (employed or unemployed). Participants were also required to provide information about their medical history and ongoing medical conditions.
Statistical Analysis
A power analysis was conducted using G*Power (Faul et al., 2009) to ensure sufficient statistical power. We selected independent variables, adjusted variables, and covariates based on previous research findings (Akasaki et al., 2022; Hironaka et al., 2020; Maruta et al., 2022; Miyata et al., 2022; Sun et al., 2023). Thus, assuming up to 30 independent variables, an effect size of f2 = 0.15, an alpha level of .05, and a power of 0.90, the estimated required sample size was 226 per age group for a logistic regression analysis. Participants were classified into three groups according to Makizako’s five criteria: SF, PSF, and robust. First, we compared the demographic data, occupational participation (overall score and subdomain scores from the SOPI), hobby status (the presence or absence of hobbies, the number of hobbies, scores for each hobby category, and the total score), and the risks to functional independence in daily living according to the Kihon Checklist (i.e., physical decline, malnutrition, oral hypofunction, cognitive decline, and depressive symptoms) among the three groups. We performed the Kruskal–Wallis test on all continuous variables and used the Mann–Whitney U test with Bonferroni correction for multiple comparisons. A Pearson’s χ2 test was used to compare participants’ characteristics by categorical variables across the different groups.
Next, we conducted a multinomial logistic regression analysis (using maximum likelihood estimation) to clarify the relationship between SF and hobbies or occupational participation. Model 1 examined the direct effects of hobbies and occupational participation on SF. The SF classification was designated as the dependent variable, with the robust group serving as the reference category. The presence or absence of a hobby, the number of hobbies, the total hobby score, and the total SOPI score were included as independent variables.
Subsequently, we developed an adjusted model (Model 2) by incorporating modified variables to enhance our understanding of how hobbies and occupational participation affect SF. In this model, we included demographic variables—such as age, sex, and educational background—that may be related to SF (Akasaki et al., 2022; Maruta et al., 2022; Miyata et al., 2022), as well as any demographic variables that showed significant differences in our group comparisons. Further, we incorporated health-related variables (including medical history, ongoing treatment for diseases, physical decline, oral hypofunction, malnutrition, depressive symptoms, and cognitive decline) as covariates. These variables showed significant differences in group comparisons and have also been suggested to be associated with SF in prior research (Akasaki et al., 2022; Maruta et al., 2022; Miyata et al., 2022).
Finally, to examine the relationship between SF and participation in hobbies and meaningful activities in detail, Model 3 used scores for each hobby category and scores for each SOPI subdomain. The sub-scores from the SOPI and the hobby category scores that demonstrated significant differences in group comparisons were used as independent variables. We calculated each model’s adjusted odds ratios (ORs) and 95% confidence intervals (CIs). In each model of multinomial logistic analysis, we checked whether the Spearman rank correlation coefficient was greater than 0.7 and whether the variance inflation factor exceeded 10, considering the impact of multicollinearity. All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Significance was set at p < .05.
Results
Participants’ Characteristics
Participants’ characteristics and the response rates for Makizako’s five criteria are summarized in Tables 2 and 3. In total, 345 (34.5%) participants were classified as PSF, 409 (40.9%) as SF, and 246 (24.6%) as robust according to Makizako’s five criteria. The demographic data showed that SF participants were more likely to be unmarried, childless, and in a noticeably worse financial situation (p < .001 for each). In addition, they had a significantly higher prevalence of undertreated diseases (p = .016), physical decline (p < .001), oral hypofunction (p < .001), cognitive decline (p = .002), and depressive symptoms (p < .001) compared to the other two groups. Intriguingly, PSF participants were more likely than the other two groups to report feeling helpful to friends or family and to talk with someone every day (Makizako items; see Table 3).
Participants’ Characteristics.
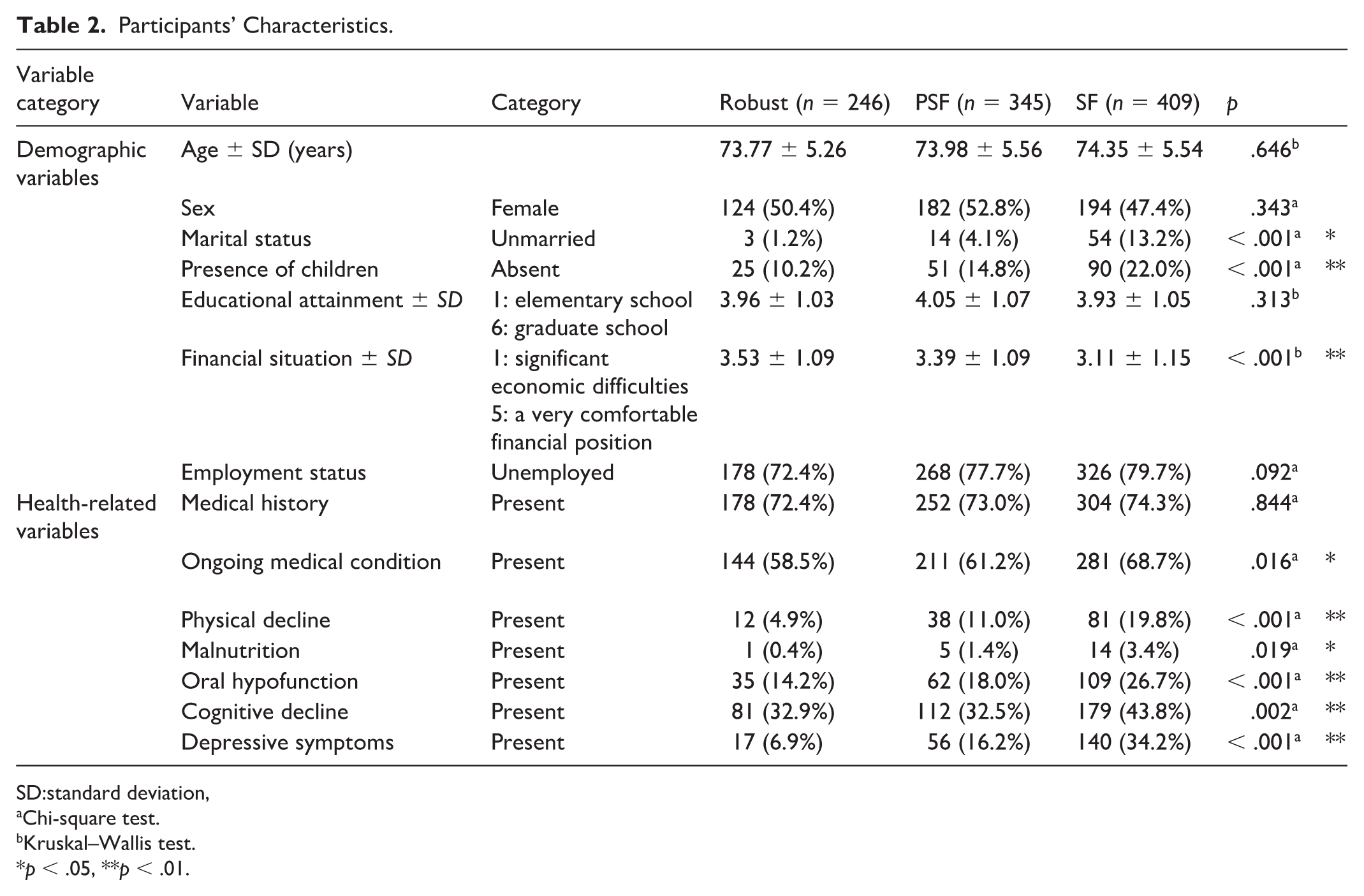
SD:standard deviation,
Chi-square test.
Kruskal–Wallis test.
p < .05, **p < .01.
Response Rate for Each Item in the Makizako Five.
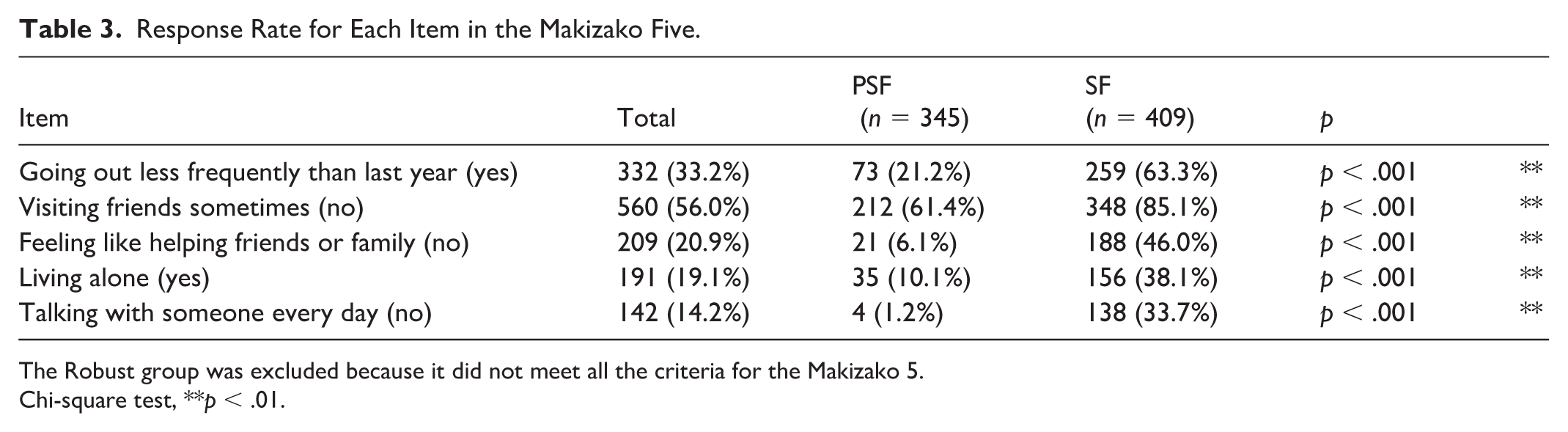
The Robust group was excluded because it did not meet all the criteria for the Makizako 5.
Chi-square test, **p < .01.
Comparison of Occupational Participation and Hobby Status
The results of group comparisons regarding the status of occupational participation and hobby status are summarized in Table 4. The SOPI total score was highest in those who were robust compared to PSF and SF (p < .001 for each). Similar results were obtained for the leisure, productive activity, and self-care subcategories.
Group Comparisons of Occupational Participation and Hobbies.
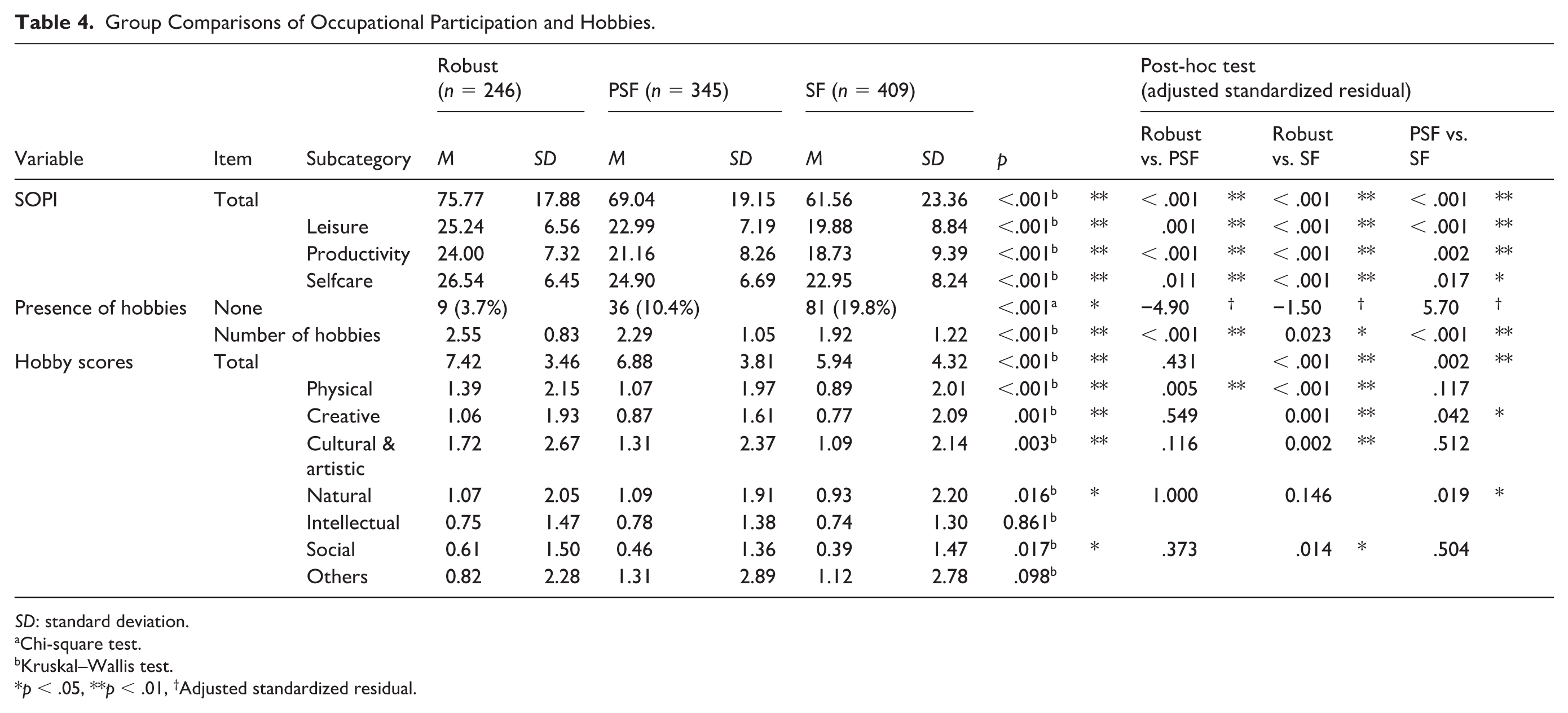
SD: standard deviation.
Chi-square test.
Kruskal–Wallis test.
p < .05, **p < .01, †Adjusted standardized residual.
The number of participants without a hobby was significantly greater in SF than in the other groups (p < .001). SF had significantly fewer hobbies compared to the PSF and robust groups (p < .001). The total score for hobbies was also the lowest in SF, which was significantly different from that of the robust group (p < .001) and PSF (p = .002). SF showed lower scores in all the hobby categories except for intellectual hobbies and other hobbies. Specifically, SF had a lower creative hobby score than the robust and PSF groups (p = .001 and p = .042, respectively), whereas the robust group had a higher physical hobby score than PSF and SF (p = .005 and p < .001).
Association of PSF and SF With Occupational Participation and Hobbies
Figure 1 summarizes the associations of occupational participation and hobby engagement with PSF and SF. In multinomial logistic regression, hobby engagement was significantly related to SF: the hobby scores (OR = 0.94, 95% CI = 0.89–0.99) and the number of hobbies (OR = 0.72, 95% CI = 0.57–0.92) were inversely associated with SF (Model 1). The inverse correlation between the number of hobbies and SF persisted after adjustment (Models 2 and 3). In addition, the fully adjusted model (Model 3) showed a significant inverse association between the cultural and artistic hobby score and SF (OR = 0.87, 95% CI = 0.81–0.95) and PSF (OR = 0.91, 95% CI = 0.85–0.98).
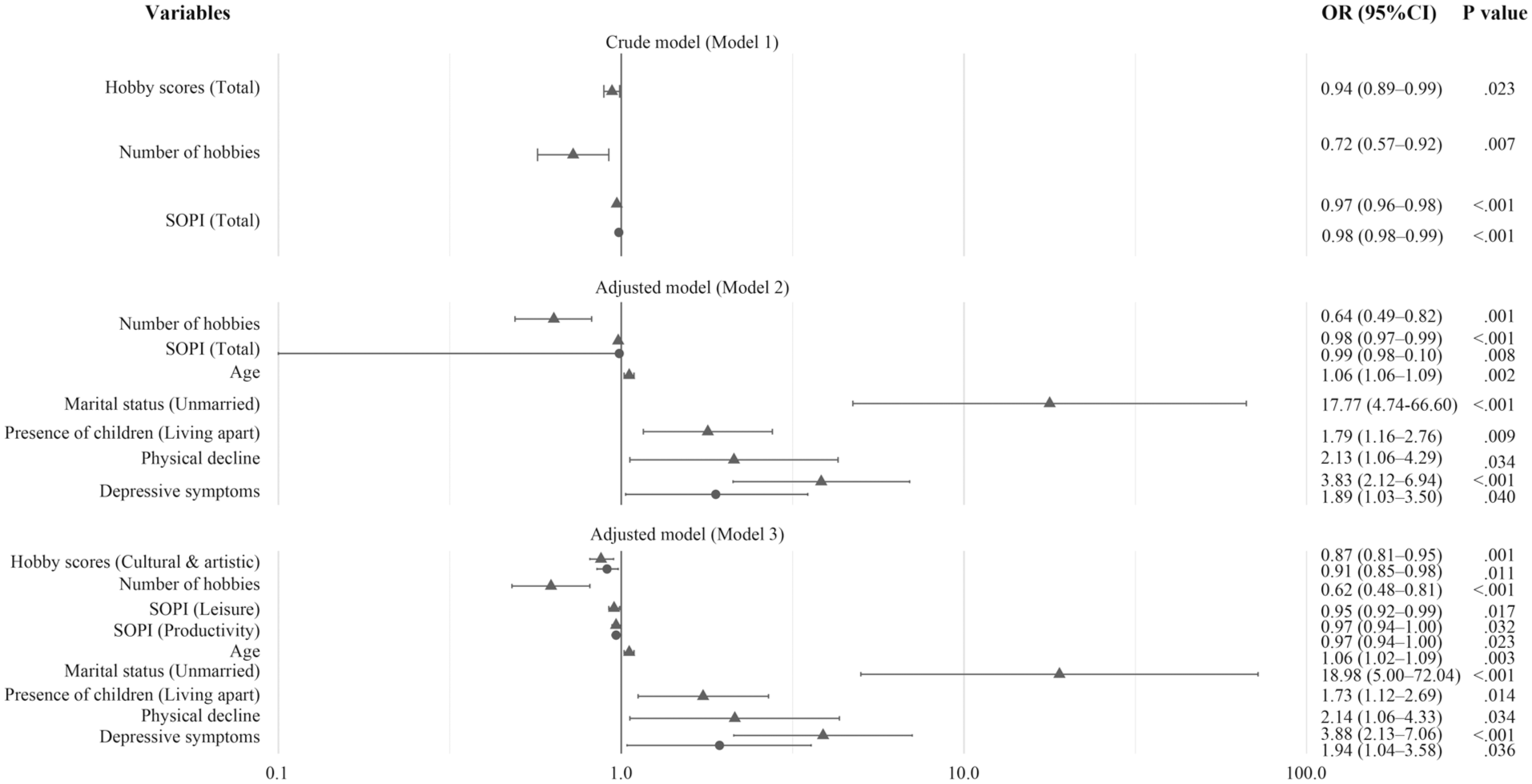
Forest Plot of Predictors of Social Frailty and Pre-Social Frailty.
Higher SOPI total scores were associated with lower odds of both PSF (OR = 0.98, 95% CI = 0.98–0.99) and SF (OR = 0.97, 95% CI = 0.96–0.98; Model 1). These associations remained significant in the adjusted Model 2 (PSF: OR = 0.99, 95% CI = 0.98–1.00; SF: OR = 0.98, 95% CI = 0.97–0.99). In the SOPI sub-scores, leisure activity was inversely associated with SF (OR = 0.95, 95% CI = 0.92–0.99), while productive activity was inversely related to both PSF (OR = 0.97, 95% CI = 0.94–1.00) and SF (OR = 0.97, 95% CI = 0.94–1.00). Depressive symptoms were associated with both PSF (OR = 1.94, 95% CI = 1.04–3.58) and SF (OR = 3.88, 95% CI = 2.13–7.06). In addition, SF was related to older age, being unmarried, not living with children, and experiencing physical decline (see Figure 1).
Discussion
This study aimed to clarify the association between occupational participation, hobbies, and SF. Older adults with SF showed significantly lower occupational participation, a higher rate of hobby absence, and fewer hobbies overall. Greater occupational participation and the number of hobbies were negatively associated with SF. Engagement in cultural and artistic hobbies was specifically associated with lower risks for SF. These results emphasize the importance of engaging in hobbies, especially cultural and artistic activities, as well as occupational participation for older adults facing SF.
Prevalence and Characteristics of PSF and SF in Older Adults
Our findings, consistent with prior work (Akasaki et al., 2022; Hironaka et al., 2020; Maruta et al., 2022; Miyata et al., 2022; Sun et al., 2023), show that in the fully adjusted logistic regression analysis (Model 3), SF was independently associated with depressive symptoms, as well as not living with children, older age, and being unmarried. The prevalence rates of PSF (34.5%) and SF (40.9%) in this study were higher than previously reported among Japanese individuals, which ranged from 10.2% to 18.7% (Makizako et al., 2015; Miyata et al., 2022; Tsutsumimoto et al., 2017). Regarding the participants’ characteristics, we note that the survey was publicized and completed online; therefore, participants were likely to have relatively strong information and communication technology (ICT) skills. This selective feature may have affected response patterns in social interactions (i.e., resulting in a higher likelihood of favoring online communication). In addition, those with PSF were less likely to report “not feeling helpful to friends or family” and were more likely to report “talking with someone every day” compared to other groups. These findings suggest a proactive effort to maintain social ties, motivated by concerns about social isolation among PSF.
Status of Occupational Participation and Hobbies Engagement
Occupational participation in the SF group was markedly lower than in both the robust and PSF groups, corroborating previous studies (Akasaki et al., 2022; Maruta et al., 2022; Miyata et al., 2022). Among the three domains of occupational performance, particularly notable were the low participation in productive activities among the PSF and SF groups and the low participation in leisure and self-care activities among the SF group. Both the PSF and SF groups reported fewer hobbies compared to the robust group, and the SF group exhibited the lowest frequency of hobby engagement. In particular, the lower engagement in physical hobbies among the SF and PSF group suggests limited social opportunities due to decreased physical activity or mobility problems (Gomes et al., 2022).
Notably, SF participants were less inclined to engage in creative, cultural, and artistic activities. Engaging in artistic activities or organized community creative and cultural events promotes social interactions and mitigates feelings of loneliness (McQuade & O’Sullivan, 2024; Watson et al., 2024). These results indicate that the overall decline in occupational participation, as well as low engagement in hobbies—particularly creative, cultural, and artistic activities—can contribute to SF.
The Relationships Between Occupational Participation, Hobbies, and SF
Results from the multinomial logistic regression analysis revealed that occupational participation was significantly associated with both PSF and SF, while hobbies were associated only with SF. Interestingly, even after adjusting for demographic and health factors (i.e., in Adjusted Model 3), participation in productive activities remained significantly associated with both PSF and SF. Due to employment promotion policies that raised the retirement age and reduced pension benefits, Japanese older adults have an exceptionally high employment rate globally (Kitao & Takeda, 2025). Their productive activities are diverse, encompassing paid work, volunteering, caregiving, and household chores, all of which are associated with higher life satisfaction and healthy aging (Fujii et al., 2024). However, while older men have high employment rates, these do not translate into social participation. In contrast, older women who engage in unpaid activities such as household work maintain better community connections (T. Saito et al., 2015; Tomioka et al., 2018). These findings underscore the importance of occupational therapy approaches that not only manage productive activities effectively but also consider their social components, underlying social resources, individual factors, and activity characteristics to promote social participation.
The finding that leisure participation and hobbies are associated only with SF suggests the importance of hobbies as active leisure activities in preventing SF. Interestingly, cultural and artistic hobbies are significantly associated with PSF and SF. Previous studies have demonstrated that participation in artistic endeavors among older adults positively influences well-being and physical health (Davies et al., 2023; Watson et al., 2024), fosters a sense of accomplishment through creative outlets, and nurtures social interaction along with a sense of purpose (Bradfield, 2021). In addition, engaging in group artistic and creative activities fosters emotional empathy and enhances the desire for a sense of community belonging (Wood et al., 2023). In occupational therapy settings focused on leisure activities for older adults, positive effects on reduced loneliness (Col et al., 2022; Levasseur et al., 2019) and the promotion of social interaction were observed (Pitkala et al., 2011). Considering these insights alongside our results, it can be inferred that cultural and artistic hobbies—particularly those requiring some social involvement (e.g., in a group or community format) —may reduce isolation and enhance feelings of social belonging, thereby contributing to the prevention of SF among older adults.
Implications for Occupational Therapy Practice and Occupational Science
Our findings align with occupational science perspectives that meaningful occupation underpins health, well-being, and belonging (Gallagher et al., 2015; Reitz et al., 2020). In practice, occupational therapists should screen for SF alongside SOPI-based occupational profiles, and then co-design hobby- and role-oriented programs that match clients’ interests and community resources. Given the independent links between physical decline and depressive symptoms, activity promotion should be paired with mobility support and mood management, providing an occupation-centered framework for community implementation and future trials.
Limitations
This study has some limitations. First, when categorizing hobbies, activities that use digital devices were included in the “intellectual” and “other” categories. Considering that older adults with sufficient IT skills to participate in an internet survey engaged in this study, “technology use” could have served as a distinct hobby category.
Second, the internet survey may have introduced participant bias, favoring older adults who value online social interactions. To address this bias, additional offline surveys or alternative survey methods should be considered to encourage broader participation among older adults.
Third, since this study employed a self-administered internet survey, the responses may heavily rely on participant subjectivity, raising concerns about the reliability of the results compared to expert evaluations. Future research would benefit from incorporating face-to-face objective assessments to enhance the reliability of responses.
Finally, as this was a cross-sectional study, it could not definitively establish a causal link between SF and the independent variables. Consequently, structural equation modeling is necessary to assess causal structures and conduct longitudinal studies with prospective cohorts.
Conclusion
This study demonstrated that active participation in diverse hobbies, as well as cultural and artistic activities during leisure time, could significantly lower the risk of SF. These findings could be particularly relevant for older adults facing the adverse impacts of psychological and physical decline, including feelings of social isolation, loneliness, and loss, which can exacerbate SF. Our findings suggest the necessity of a preventive approach to long-term care that accurately evaluates occupational participation and promotes hobby-based leisure and accessible community events to mitigate SF risk, considering the client’s unique challenges and available community resources.
Footnotes
Acknowledgements
We thank Editage® for editing a draft of this manuscript. The internet survey for this study was conducted on the online platform of Cross Marketing Inc.
Ethical Considerations
This study was approved by the ethics committee of the Faculty of Health and Welfare, Prefectural University of Hiroshima (No. 23MH019; approved on July 5, 2023) and conformed with the Helsinki Declaration of 1975, as revised in 2000.
Consent to Participate
Participants were described the study online, and their consent was implied by completing the survey.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by our institution’s basic research fund and not a specific grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to a lack of an institutional repository.
AI Use Statement
An AI language tool (ChatGPT, OpenAI) was used to assist the authors in drafting R (ggplot2) code for figure formatting. The tool did not generate, modify, or validate research data, analyses, results, or conclusions. All code was reviewed and executed by the authors, who take full responsibility for the content.