
Abstract
Understanding that excess body weight can increase disability and limit daily occupations, occupational therapists must consider how to support patients with weight management within a larger health care system. To develop a clinical tool for health care professionals to (a) support referrals to occupational therapists to address weight management and (b) assess priorities for weight management interventions. This research utilized a co-design process with six occupational therapists from primary care to design a screening tool prototype. The design process revealed three challenges to supporting patients with excess body weight that were addressed through the design elements of the screening tool: (a) weight is a “sticky” topic, (b) negative messaging around weight can adversely impact patient care, and (c) occupational therapy involvement in weight management is impacted by a lack of referrals. This design process yielded the Occupational Therapy Health Routines Screening Tool prototype.
Plain Language Summary
Excess body weight affects an increasing number of people worldwide and can affect individuals’ abilities to engage in meaningful occupations. Therefore, it is important for occupational therapists to consider how to help patients with weight management challenges. Occupational therapy tools and assessments for helping patients with weight management are limited. Therefore, this research was done to create a screening tool to identify lifestyle behaviors that can lead to obesity. The screening tool was designed to be used by health care providers to identify potential intervention areas and support referrals to occupational therapy when needed. This study involved discussions with occupational therapists to identify patient and clinician needs to create an effective screening tool. The results of these discussion groups informed the development of the Occupational Therapy Health Routines Screening Tool.
Introduction
Excess body weight (EBW) is defined by excessive fat accumulation, encompassing both overweight (body mass index [BMI] more than 25) and obesity (BMI more than 30). The prevalence of EBW in the United States is 74%, meaning that a large proportion of patients treated within our health care system are impacted by health-related weight concerns (i.e., disability, functional limitations, and comorbidities; Centers for Disease Control and Prevention [CDC], 2021). It is more important than ever for occupational therapy practitioners to address weight within evaluations and interventions, since larger proportions of patients will be dealing with weight management challenges that directly impact health and functioning.
EBW and Occupational Participation
Previous research has indicated that EBW can have significant impacts on a person’s participation in daily occupations. Participation has been shown to be limited for individuals with EBW due to physical factors (i.e., decreased walking speed and stability), socioemotional factors (i.e., beliefs and attitudes), and environmental factors (i.e., spaces that are not accommodating to larger body types) (Forhan et al., 2010; Kim et al., 2022). Daily occupations are shown to be limited when living with EBW due to factors including pain, fatigue, incontinence, dyspnea, musculoskeletal disorders, social anxiety, and inaccessible spaces (Forhan et al., 2010). Overall, people with EBW have increased disability, or limitations in abilities to complete desired activities, compared with those without (Ilvig & Christensen, 2017). These findings demonstrate the importance of acknowledging the role of weight management in occupational participation.
Contemporary Weight Management Interventions
Most weight management interventions for adults focus on weight loss once significant health concerns have been established (Pearce et al., 2019). Less than 3% of individuals without EBW receive services to help them maintain a healthy current weight (Lutfiyya et al., 2008). Lifestyle and pharmacological interventions demonstrate limited long-term results for weight loss (Douketis et al., 2005). For those who do lose weight with such interventions, most eventually regain what they had lost (MacLean et al., 2015). Receiving preventive health care services decreases the risk of various diseases, disability, and death (Borsky et al., 2018). Therefore, preventive versus reactive care could be an important missing link in effective adult weight management.
In addition, contemporary care has often narrowly focused on diet and/or exercise (Muntefering et al., 2023). Patients are frequently retold the same message of “eat less, move more” by multiple providers without acknowledging the highly complex and interconnected factors that impact one’s weight (English & Vallis, 2023). Previous research has indicated that occupational therapists have supported adult patients in weight management by referring them to dietitian services and offering physical activity advice (Lang et al., 2013). However, the factors influencing weight are broader than diet and exercise alone, including behavioral patterns, social determinants of health, genetics, environment, medical conditions, and medications (CDC, 2021). Therefore, multifaceted interventions addressing this range of factors could more effectively support patients (Jessen-Winge et al., 2022).
Exploring How Occupational Therapy Can Better Support Weight Management
As a field that is both focused on patient-centered care and the holistic factors of a person, their environment, and their occupations, occupational therapy is a profession that could contribute new and positive approaches to weight management (Hildenbrand & Lamb, 2013; Nielsen & Christensen, 2018). In addition, in the most recent update of the Occupational Therapy Practice Framework, “health management” was added as a new occupation category (American Occupational Therapy Association, 2020b). Within this framework, health management encompasses numerous occupations that are necessary for weight management, including activities dealing with health promotion and maintenance, symptom/condition management, communication with the health care system, medication management, physical activity, and nutrition management, demonstrating occupational therapy’s role in this space. Occupational therapy practitioners work with diverse populations to mitigate barriers that cause decreased occupational engagement. However, despite the understanding that living with EBW can significantly impact occupational engagement, occupational therapy practitioners’ role in preventive weight management practices has been limited and overlooked (Hildenbrand & Lamb, 2013). Furthermore, occupational therapy practitioners are rarely included in interdisciplinary teams assisting individuals with EBW, like in weight management clinics where dieticians, nurses, physicians, exercise physiologists, and physical therapists are the most common providers included in weight management interventions (Muntefering et al., 2023). In a mixed-methods study exploring practice patterns among occupational therapists in primary care settings, many therapists vocalized a reluctance to discuss weight-related topics with patients, with some even circumventing such conversations when patients brought them up (Muntefering et al., in press). In addition, Lang and colleagues (2013) found that, while previous studies had identified occupational therapy practitioners’ potential role in weight management, the occupational therapists participating in their research voiced that such care was outside their scope of practice.
Despite occupational therapy practitioners’ expertise, positioning them to provide proactive, multifaceted, and sensitive weight management care, the field demonstrates confusion and hesitancy about how to approach patients with weight management concerns. In addition, research has highlighted that other health care disciplines are unaware of occupational therapists’ expertise in this realm, limiting referrals for patients with weight management challenges (Muntefering et al., 2025). Therefore, the objective of this research was to design a clinical tool to be used by multidisciplinary providers (i.e., physicians, nurses, physical therapists, and nutritionists) that (a) identified priorities for weight management interventions and (b) supported referrals to occupational therapy practitioners when needed.
Method
This study utilized a five-stage co-design process to develop a clinical tool to be used by multidisciplinary health care providers to identify priorities for weight management interventions and support appropriate referrals to occupational therapy when needed (Werner et al., 2022). Occupational therapists acted as participants in the co-design sessions to iteratively develop a prototype for supporting patients’ weight management within primary care settings. Throughout this paper, occupational therapists who acted as participants in the co-design sessions will be subsequently referred to as “co-designers.” The stages of the design process included problem identification, solution generation, convergence, prototyping, and evaluation (Reddy et al., 2019). This research study was approved by the University of Wisconsin- Madison Institutional Review Board, application number 2023-0794.
Participants and Recruitment
Individuals were invited to participate as co-designers if they met the following inclusion criteria: (a) board-certified occupational therapists (occupational therapy assistants were not included since evaluation patterns were being explored); (b) actively or previously (within the past five years) having provided care to adult patients in primary care settings; (c) delivering care in the United States; (d) English speaking; and (e) having expertise in one of five defined primary care practice areas (women’s health, mental health, community setting, hospital/clinic setting, or home health). These were five areas of primary care defined by the American Academy of Family Physicians (2022, Primary Care Section) that also aligned with primary care settings where occupational therapists practice. Co-designers were recruited from a previous research study exploring practice patterns of occupational therapists addressing preventive weight management with adult patients in primary care (Muntefering et al., in press). Participants from the previous study who met the eligibility criteria for this study were sent an invitation via email to participate. Those who agreed to participate were sent a Qualtrics survey to provide informed consent.
Participatory Design Sessions
Pre-session Preparation
The six co-designers completed pre-work before each co-design session to prepare for engagement in each session. Pre-work included activities like reflective journaling, ranking activities, and prototype drafting. For activities involving prototype drafting, the participants were given prompts to focus their efforts prior to the session meeting (i.e., creating a title and developing section headers).
Co-design Session Process
The co-designers attended five co-design sessions over 9 weeks remotely via videoconference between March 2024 and May 2024. Each co-design session was separated by 2 weeks, lasted 90 min, and was audio- and video-recorded. At the outset of the study, researchers discussed with the co-designers that the purpose of the sessions was to create a clinical support tool or document that provided increased support for occupational therapy practitioners to work with patients with weight management challenges. The ideas and themes that were generated for each co-design session were synthesized, developed, and iterated in successive sessions. Synthesis and development of ideas from the sessions occurred using the Rapid Identification of Themes from Audio-recordings (RITA) method, which is described in more detail in the Data Analysis section (Neal et al., 2015). Two members of the research team (C.M. and M.L.) synthesized ideas for co-designers for subsequent co-design sessions. The five sessions were all facilitated by the lead researcher (C.M.) with assistance from additional research team members (C.H., M.L., and E.S.). All four members of the research team created reflexive memos after each co-design session to reflect on their bias and positionality in the research process (McGrath, 2021).
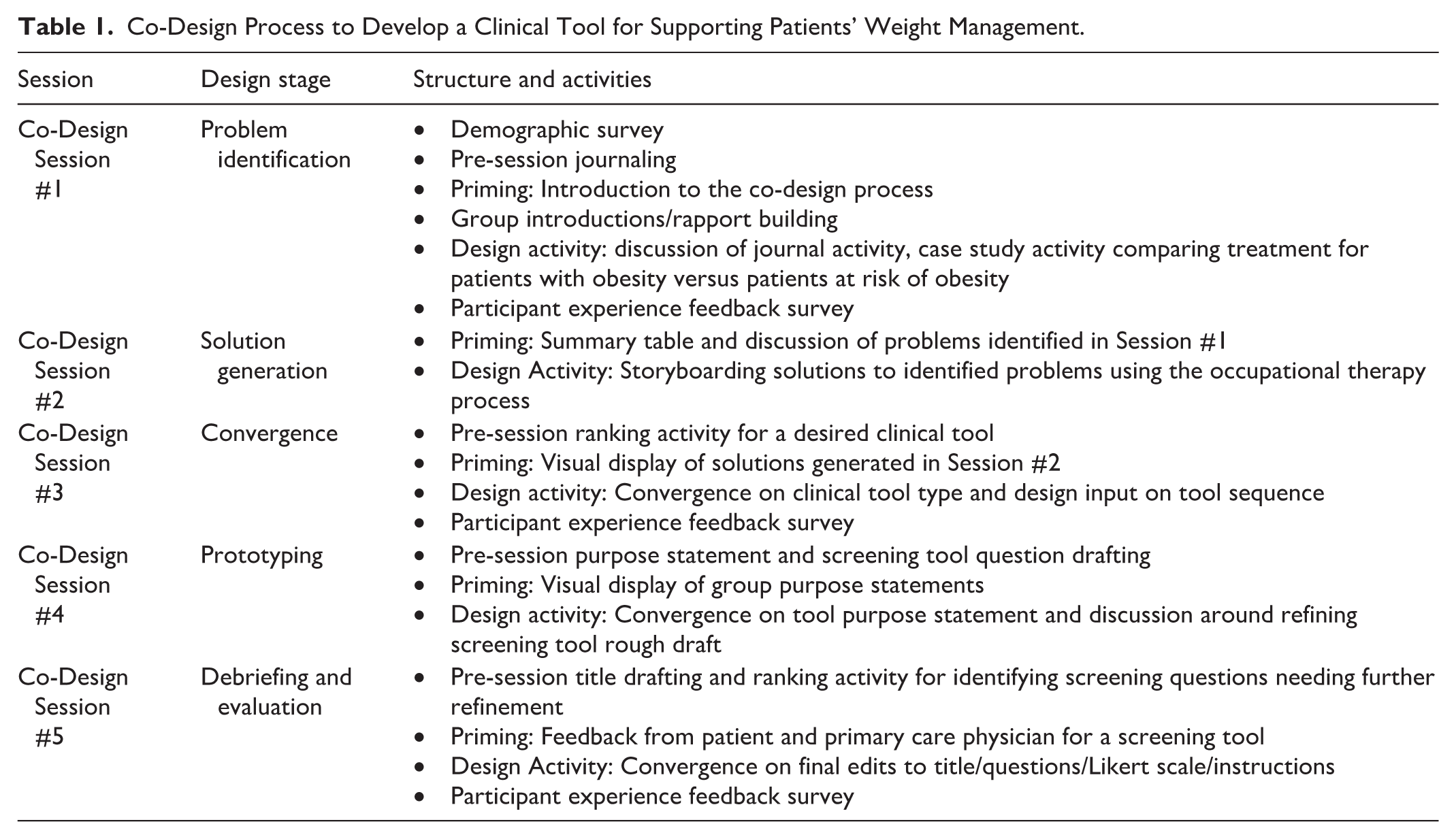
Each session began with priming activities to support co-designers’ full immersion in the topic of discussion, followed by activities to promote the iterative design of the final prototype across the five sessions (see Figure 1 for a sample storyboarding activity completed in co-design Session 2). Table 1 outlines the structure and activities that made up each of the sessions. The session agendas for the five co-design sessions were designed and modified by the research team with additional input from other consultants on the study (i.e., experts in participatory design, health care, and occupational therapy). Participants were given a $50 Amazon e-gift card for each of the sessions they attended.
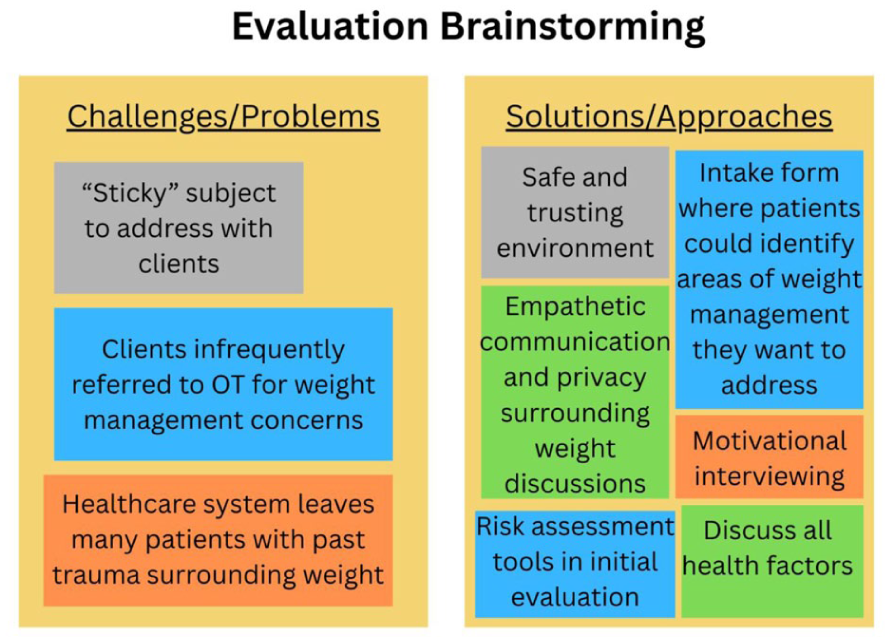
Sample Storyboarding Co-Design Session Activity
Co-Design Process to Develop a Clinical Tool for Supporting Patients’ Weight Management.
Surveys
Demographic Survey
Prior to the first session, co-designers were sent a Qualtrics survey via email to collect demographic data to promote study veracity.
Acceptability of Intervention Measure/Intervention Appropriateness Measure
To examine the implementation outcomes of this screening tool, we assessed acceptability using the Acceptability of Intervention Measure (AIM) and appropriateness using the Intervention Appropriateness Measure (IAM) (Weiner et al., 2017). The AIM and IAM are each four-question, validated measures that contain statements about acceptability and appropriateness, respectively, with each statement rated on a Likert-type scale from completely disagree (1) to strongly agree (5) (Weiner et al., 2017). A score of 20 is the maximum score on each. We utilized these measures with co-designers during the final session to measure their perceived acceptability and appropriateness of the final prototype. Co-designers completed the AIM and IAM individually by reviewing the final prototype and responding to the questions related to perceived acceptability and appropriateness. While neither of these measures currently has cut-off scores for interpretation available, higher scores indicate greater acceptability and appropriateness.
Data Analysis
Analysis of co-design sessions occurred both within and between sessions. Within sessions, our research team led participants in generating, grouping, and converging upon design solutions. During the 2-week period between sessions, two research team members (C.M. and M.L.) reviewed recordings of the sessions using the RITA method (Neal et al., 2015). RITA is a method used to rapidly identify themes from audio recordings, which allows researchers to code and analyze qualitative data without time-consuming transcription. We followed the five-step process outlined by Neal and colleagues (2015), moving from the identification of a research foci, then to deductive and iterative coding, and finally to evaluating the reliability of coding between investigators. Prototype design specifications were our identified research foci, as Neal et al. (2015) recommend focusing on components of the project that require immediate feedback. A coding template was created by our research team and given to both researchers taking part in the RITA coding process. The template divided the co-design session recordings into 3-min segments. The research team additionally combined the themes generated from the RITA with the analysis of any other outputs created in the sessions (i.e., storyboard, ratings, and participant notes). Co-designers were provided with an informational flyer to share with their practice to identify occupational therapy patients who would volunteer for peer debriefing. Similarly, informational flyers were shared with primary care physicians within the research team’s network to identify a physician who would volunteer for peer debriefing. Peer debriefing occurred with a former occupational therapy patient with EBW and a primary care physician between sessions 4 and 5 to review the prototype draft and provide feedback (Collins et al., 2013). The patient provided feedback about readability and sensitivity of language, while the primary care physician provided feedback about the feasibility of using the screening tool in health care practice settings (i.e., timing, efficiency, and provider compliance). The feedback shared by these two peer debriefers was included with the analysis results of the RITA during the final session. Demographic data were analyzed using descriptive statistics using SPSS (v.29) (IBM Corp, 2022). Descriptive statistics consisted of percentages, means, and standard deviations. The data from co-design session surveys (i.e., AIM and IAM) were also summarized using descriptive statistics.
Results
Demographics
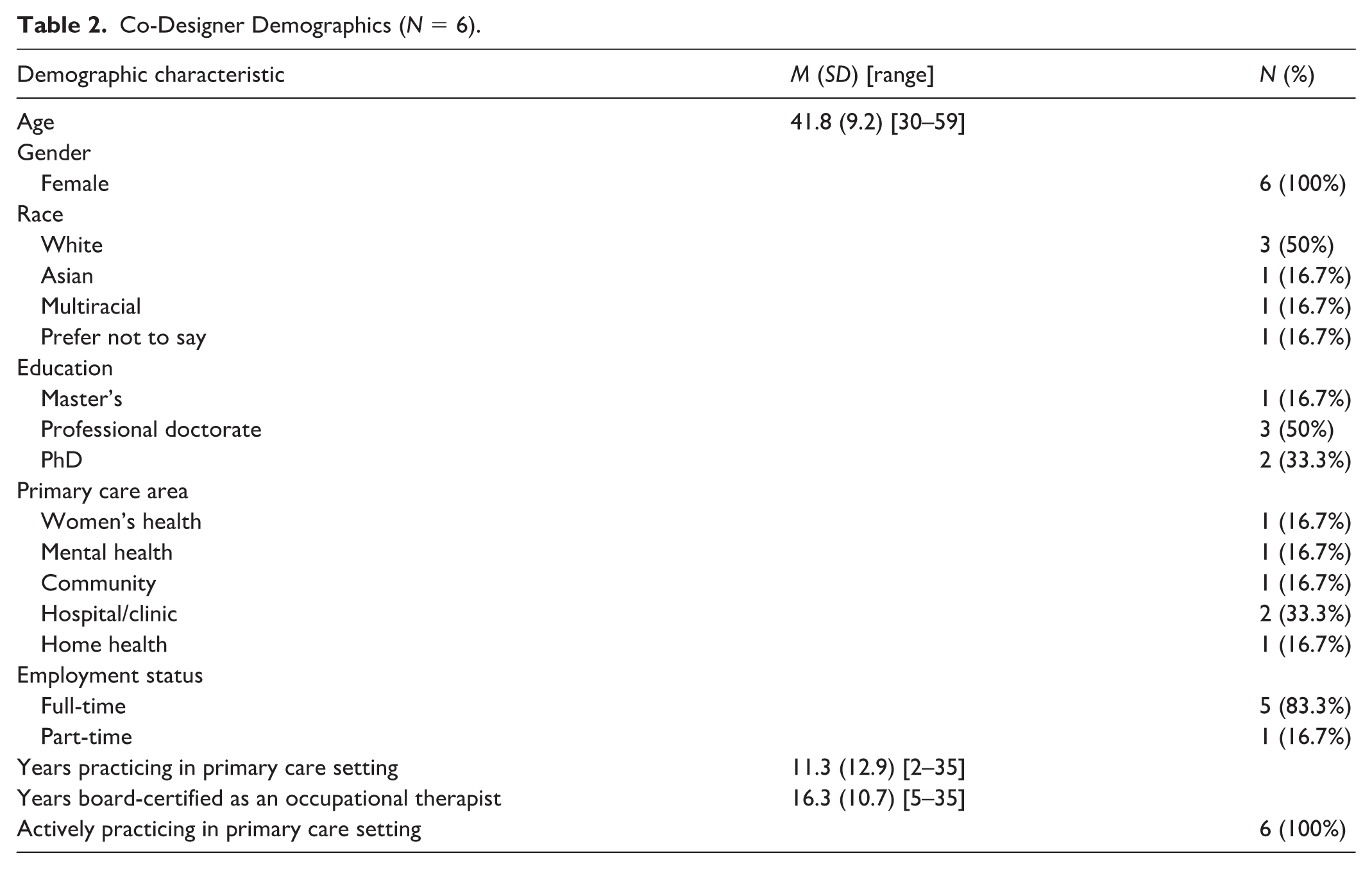
Six co-designers participated in the co-design process. Three of the six co-designers attended all five sessions, and the remaining three attended four sessions. Co-designers were occupational therapists who were actively treating in primary care settings, which encompassed practicing in the following states: Arizona (1), California (2), Florida (1), Iowa (1), and Missouri (1). For demographic characteristics of the co-designers, refer to Table 2.
Co-Designer Demographics (N = 6).
Main Results
Analyses yielded three overarching challenges co-designers faced in addressing weight management with patients. Each challenge is defined and explained in greater detail, along with the design elements generated for the final prototype developed to address these problems.
Challenge 1: Weight is a “Sticky” Topic
Co-designers emphasized how conversations with patients about weight can be very “sticky, sensitive, nuanced, and layered.” With this challenge in mind, co-designers wanted the screening tool to include sensitive language, avoiding shameful messaging. Design features addressing this challenge included (a) the exclusion of the word “weight” and (b) the use of neutral or unbiased language. In addition to the design element of sensitive language, co-designers expressed the importance of creating features in the screening tool that served to clarify to occupational therapy practitioners the scope of their practice relevant to weight management. This design element is intended to decrease confusion about what areas of weight management are appropriate and within occupational therapy’s scope. Features addressing this included (a) questions organized by areas of occupation that are potential risk factors for weight management and (b) scoring divided among these areas of occupation to establish clear areas for priority in health routines of the patient. See Table 3 for these identified challenges and design elements.
Challenges, Design Requirements, Supporting Quotations, and Prototype Features.
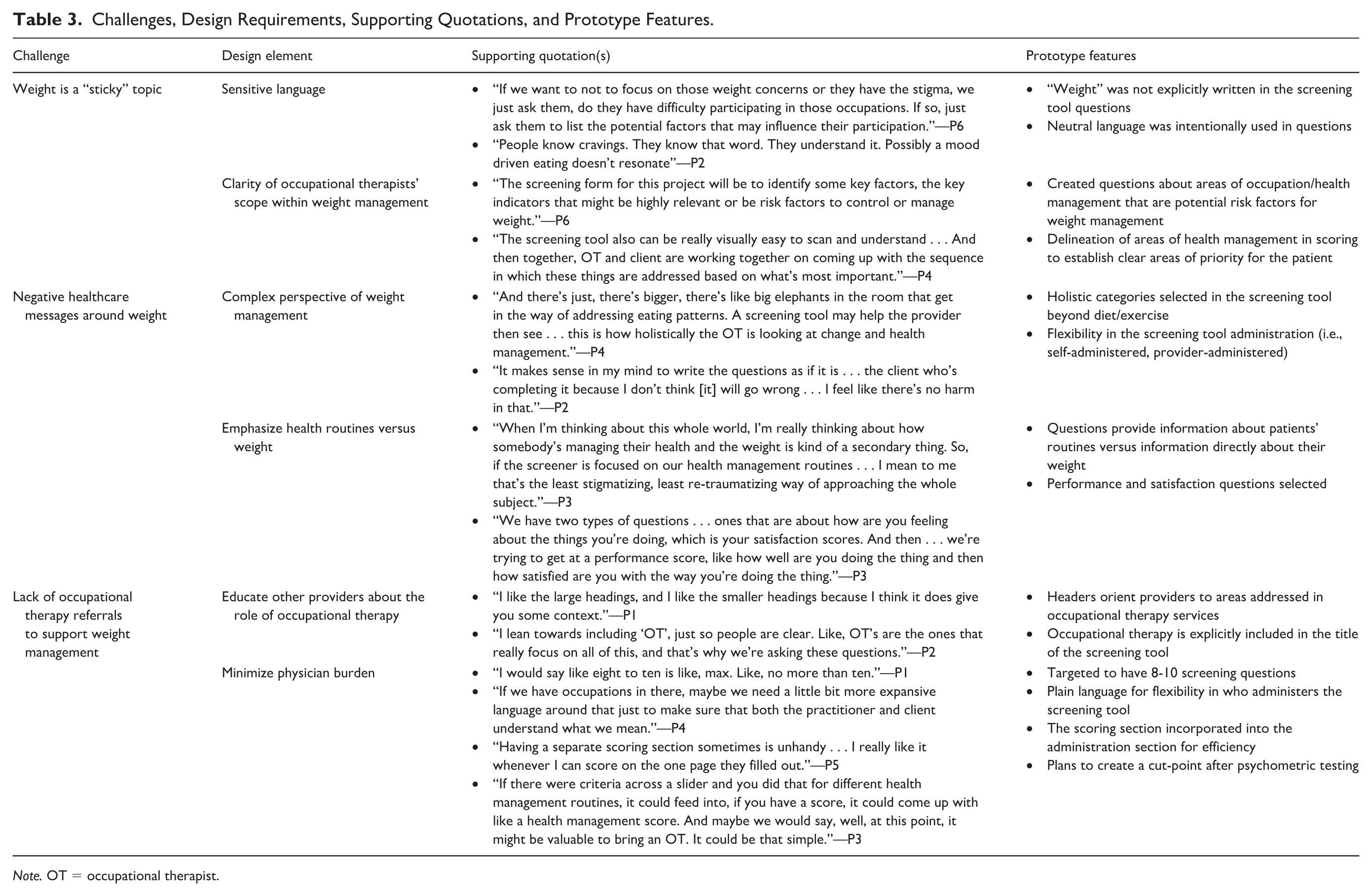
Note. OT = occupational therapist.
Challenge 2: Negative Health Care Messages Around Weight
Co-designers expressed that navigating the sensitive topic of weight can be even more challenging when many patients have heard stigmatizing messages in their prior health care experiences. They discussed that “eat less and move more” was a phrase that patients have often heard repeatedly, minimizing the complexity of weight management. For this reason, co-designers wanted the screening tool to offer a more complex perspective of weight management. Design elements addressing this challenge included (a) focusing on holistic categories of health routines beyond diet and exercise, and (b) providing flexibility in screening tool administration (i.e., self-administered or provider-administered).
In addition to aiming to provide a more complex perspective of weight management, co-designers wanted the screening tool to focus on the outcome of the individual’s experience within their health routines, rather than weight on the scale. This was achieved by (a) the inclusion of questions about the patient’s routines versus directly about their weight and (b) the inclusion of questions targeting both the individual’s performance and satisfaction in their routines.
Challenge 3: Lack of Occupational Therapy Referrals to Support Weight Management
Finally, co-designers discussed how a further challenge to addressing weight management with patients is the limited referrals that occupational therapists receive for supporting patients in their weight management. For this reason, the co-designers wanted the screening tool to be a multidisciplinary tool that helped educate other providers about the scope of occupational therapy related to weight management. To address this design element, the following features were included in the tool: (a) bold headers that orient providers to areas of routines addressed by occupational therapy and (b) “occupational therapy” included in the title of the screening tool. While the screening tool was intended to be a multidisciplinary tool, the co-designers specifically chose to use “occupational therapy” in the title to increase awareness of a profession that has historically been underutilized in weight management care.
In addition to providing education to support referrals, the co-design team understood that the tool would need to minimize burden on diverse health care providers to ensure its effective utilization in health care practices. This was achieved through the following features: (a) a projected final screening tool targeted to have no more than eight to 10 questions, (b) plain language to support the flexibility of administration, (c) a scoring section incorporated onto the same page as the administration section for efficiency, and (d) plans to create a cut-off point after psychometric testing.
Acceptability and Appropriateness
After the final session, the average AIM score of the developed screening tool prototype was 20 (standard deviation [SD] = 0) and the average IAM score was also 20 (SD = 0).
Discussion
This research study used a co-design process to include occupational therapists in creating a screening tool for multidisciplinary health care professionals to (a) support referrals to occupational therapists to address weight management and (b) assess priorities for weight management interventions. Co-designers designed their prototype with the recognition that occupational therapists’ involvement in weight management care is supported when they are incorporated in multidisciplinary teams that address weight, and hence the creation of a multidisciplinary tool. The co-designers produced a screening tool with six key design elements that supported a strong concept guiding the final development of a screening tool for health management routines, the Occupational Therapy Health Routines Screening Tool (OT-HR) (See Supplemental Material).
Within health care settings, there has been an overreliance on BMI as a metric to screen and determine care surrounding weight management (Mishra & Floegel-Shetty, 2023). However, repeated evidence has shown that care related to EBW cannot be based solely on BMI, especially since this metric has demonstrated limitations in predicting chronic disease and can demonstrate a distorted risk in individuals with high levels of muscle mass (Aluyor & Idialu, 2022; Wu et al., 2024). Our results also highlighted the need for clinical tools that have a more complex perspective of weight management that extends beyond considering diet and exercise alone. Standard weight management advice in our health care system has been “eat less, move more.” Despite growing literature that indicates how narrow and ineffective this suggestion is (Correia et al., 2020; Fitch, 2020), significant care targeted at the prevention of weight gain has continued to focus solely on diet and/or exercise (Muntefering et al., 2023). Care that focuses on these narrow factors could also be ineffective, considering that EBW significantly impacts mobility, making “moving more” not only challenging, but also with risk of injury (Kim et al., 2022). Weight management is highly complex and influenced by multiple personal (i.e., genetics and medical conditions), environmental (i.e., social determinants of health), and occupational (i.e., behavioral patterns) factors (CDC, 2021). Therefore, our co-designers aimed to acknowledge the complexity of weight management by highlighting screening tool questions that addressed diverse areas of occupation relevant to health management (i.e., sleep, social participation, meal preparation, and symptom management)—including such complex questions acknowledged social determinants of health, recognizing that these factors can heavily influence someone’s day-to-day participation and health. Heeren and colleagues (2023) demonstrated evidence indicating that interventions solely addressing individual-level factors will continue to be insufficient in promoting optimal weight management within populations. They argued that addressing systems-level factors, like social determinants of health reflected in questions within our screening tool, will be necessary to improve weight-related interventions.
Occupational therapists are uniquely equipped to address the complexity of factors addressing weight management because of their expertise in activity analysis, as well as their consideration for the interplay of people, occupations, and environments (Jessen-Winge et al., 2021). A holistic approach to weight management has been argued to be most sustainable for yielding long-term solutions, especially since there are a multitude of factors affecting weight (Gupta et al., 2024). Occupational therapy has been argued to be a profession supporting holistic health (Miller, 1992). The OT-HR was designed to evaluate comprehensive factors influencing EBW to provide more holistic weight management care.
Our results also emphasized the need for improved interdisciplinary collaboration in supporting patients’ weight management. While the original aim of this research was to advance clinical tools for occupational therapists supporting patients with weight management concerns, our co-designers emphasized that a barrier to occupational therapy addressing weight management was a lack of referrals for such patient concerns. Therefore, the co-design team ultimately created a multidisciplinary tool to help drive referrals from other health care providers to occupational therapists for patients with weight management needs. This is consistent with previous literature demonstrating how crucial an interdisciplinary approach is to fully understanding and managing EBW (Bischoff et al., 2017).
Concerning next steps, the developed screening tool requires further acceptability, feasibility, and usability testing. While this research examined acceptability of the screening tool by the co-designers, the evolution of the OT-HR into a multidisciplinary tool warrants the need to explore acceptability among other health care providers, patients, as well as other occupational therapists. In addition, the co-design team discussed the intention of the OT-HR to be administered with patients as part of regular preventive screenings during annual primary care visits with their physician but determining when and where to optimally administer this tool requires further feasibility testing. Usability testing should include focus groups with health care organizations, including both providers and patients in conversations about how to optimize the use of the tool. To support integration of the OT-HR into primary care settings, implementation frameworks like the Consolidated Framework for Implementation Research should be utilized to guide use of the tool in practice (Damschroder et al., 2022). In addition, in implementation planning, it could be beneficial to establish a toolkit of resources and strategies that health care providers can offer patients dealing with barriers related to health management routines and social determinants of health that are identified through the OT-HR. Such resources and strategies would provide health care providers with next steps to supporting their patients, in addition to referring out to occupational therapy.
Strengths and Limitations
Numerous strengths of this study should be mentioned. First, this study developed a clinical tool using a participatory design process, which is a valuable research process in utilizing end-users to inform and assist in the development of applicable research (Shilton et al., 2008). We also utilized peer debriefing with a physician and a previous occupational therapy patient to support reflexivity and provide the opportunity for critical dialogue with other valuable end-users who would be involved in using this screening tool.
Despite these strengths, multiple limitations of this study should be considered. First, while we attempted to best include the ideas and feedback of all co-designers, some shared more within our design sessions than others and thus could have more strongly influenced our final product. Second, although we aimed to recruit a diverse group of occupational therapists to serve as co-designers, our participants were all female. Given that 91% of American occupational therapists in the workforce are female, it is not surprising that we were unable to recruit a male participant as a co-design participant (American Occupational Therapy Association, 2020a). Another limitation was the irregular attendance by some co-designers, which could have impacted or limited their overall participation in the co-design process. In addition, there was no equal representation of the five primary care practice settings, since one therapist represented each area, but two therapists were working in a hospital or clinic setting. There was also no equal geographic representation among study participants.
Finally, the prototype development could have been limited by the fact that the co-designers were solely made up of occupational therapists. Since this research was in response to another study that demonstrated limited occupational therapy clinical tools for supporting patients with weight management, the original objective of the co-design sessions was to develop a prototype that could support occupational therapists working with patients with weight management concerns. However, through the problem identification and solution generation phases of the co-design process, the co-designers identified that a critical barrier to incorporating occupational therapists in weight management care was the lack of referrals for this need to occupational therapy from other health care providers. Therefore, the co-design team felt it was more imperative to create a multidisciplinary tool that could help (a) identify referrals to occupational therapy by other health care providers and (b) identify priorities for weight management interventions to be conducted by occupational therapy. Since the co-designers had already been organized and established, the incorporation of a physician as a peer debriefer to provide feedback on the prototype was in direct response to this limitation.
Conclusion
This research advances clinical approaches for the prevention of weight-related health problems by creating a screening tool that could support the referral of patients with weight management challenges to occupational therapy and support intervention planning. The screening tool that was developed through this research, the OT-HR, is intended to be utilized by diverse health care professionals to identify (a) patients who would benefit from a referral to occupational therapy for weight management concerns and (b) intervention priorities to address to support patients’ weight management. While the OT-HR still requires further psychometric testing, the screening tool has the potential to help multidisciplinary providers understand when to refer to occupational therapists for weight management needs, and to clarify to occupational therapists treatment areas that are within their scope to address with patients. The results from this study extend guidance on the need to use nonjudgmental and respectful language around weight with patients. Our results also demonstrate the need for clinical tools that view weight management as more complex than energy in, energy out. Finally, this research demonstrates the need for effective multidisciplinary collaboration to support patients with weight concerns.
Footnotes
Acknowledgements
Appreciation is extended to Ella Schroder and Corrina Holcomb for their assistance with developing the co-design process agendas and facilitating co-design sessions.
Ethical Considerations
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Consent to Participate
Participant consent was provided verbally.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Marsh Center Pilot Grant through the University of Wisconsin-Madison. Dr. Voils’ effort was supported by a Research Career Scientist award from the Department of Veterans Affairs (RCS 14-443). The views in this research are those of the authors and do not represent the VA or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not publicly available due to qualitative data containing information that could compromise the privacy of research participants.