
Abstract
Lifestyle research on cognitive health has been largely unidirectional and cross-sectional, with limited attention to multidimensional and bidirectional relationships; this study examines longitudinal associations in middle- and older adults. Data from the Korean Longitudinal Study of Aging (2006–2020) included physiological and psychosocial lifestyle factors and cognition assessed by the Korean version of the Mini-Mental State Examination (K-MMSE). Analyses used Mplus 8.9 with cross-lagged panel model (CLPM) and random intercept CLPM (RI-CLPM), adjusting for sex, age, smoking, drinking, and disability. CLPM showed significant lagged effects of lifestyle on cognition across waves (β = .010 to .013, p < .01), with intermittent reverse effects (β = .013 to .015, p < .05). The RI-CLPM confirmed a stable effect of lifestyle on cognition (β = .013 to .017, p < .05), whereas effects from cognition to lifestyle were mixed and nonsignificant (β = −.054 to .034, p > .05). A multidimensional lifestyle was associated with cognitive maintenance, whereas cognitive decline shows variable influences on lifestyle.
Plain Language Summary
As people age, changes in memory and thinking become more common. Understanding what helps maintain brain health is important for supporting independence and quality of life. Many previous studies have focused on single lifestyle factors—such as exercise or diet—and often looked at them at only one point in time. This study examined how a combination of everyday habits relates to thinking ability over a long period. We used data from over 5,101 middle-aged and older adults in Korea who were followed for 14 years. We looked at several aspects of lifestyle, including physical activity, eating habits, social relationships, and participation in work or community activities. We then examined how these factors were related to changes in cognitive function over time. The findings showed that people with healthier and more active lifestyles tended to maintain better cognitive function over time. In contrast, declines in cognitive function did not consistently lead to changes in lifestyle. This suggests that daily habits may play a more important role in supporting brain health than changes in cognition do in shaping lifestyle. Overall, the results highlight the importance of maintaining a balanced and active lifestyle that includes both physical and social activities. Encouraging older adults to stay physically active, socially connected, and engaged in meaningful daily activities may help support their cognitive health. These findings are especially relevant for health care professionals, including occupational therapists, who work to promote healthy aging and independence in later life.
Keywords
Introduction
Population aging is accelerating worldwide, highlighting the importance of maintaining health and quality of life in later adulthood (World Health Organization [WHO], 2021). Age-related cognitive decline compromises daily functioning and heightens dementia risk, thereby threatening older adults’ independence and well-being (Campbell et al., 2025). In 2020, an estimated 57 million people were living with dementia, with nearly 10 million new cases annually, placing heavy burdens on individuals, families, and societies (Nandi et al., 2024; WHO, 2025). Because cognitive function declines gradually across the life course, identifying factors linked to cognitive decline and dementia is critical for prevention (Hou et al., 2024).
Lifestyle, defined as habitual patterns of daily behavior, is a key determinant of health (Brivio et al., 2023). Health research has traditionally focused on physiological factors such as physical activity, sleep, diet, and substance use (Lippman et al., 2024; Liu et al., 2022). More recently, holistic perspectives have emphasized psychosocial elements, broadening the concept of lifestyle to include social and contextual dimensions (Burke & Dunne, 2022). Park et al. (2023) described a healthy lifestyle as a multidimensional construct encompassing physical activity, nutrition, social relationships, and occupational participation, which together shape health and quality of life. Such multidimensional lifestyles are strongly associated with cognitive preservation, underscoring the need for longitudinal examination of their relationships (Ngandu et al., 2015).
Cognitive function, the capacity to process environmental stimuli, is shaped by repeated behaviors and social interactions (Hsu & Bai, 2022). Cognitive reserve theory suggests that education, physical activity, occupational tasks, and social participation enhance brain plasticity and delay decline (Sumowski, 2015). Regular activity, balanced nutrition, and social engagement thus provide cognitive stimulation and protect brain health (Wen et al., 2025). Examining causal pathways between lifestyle and cognition is therefore crucial to identify modifiable targets for preventing or managing decline (Livingston et al., 2024).
Lifestyle and cognition can be understood within broader theoretical frameworks. Ecological Systems Theory (Bronfenbrenner, 1979) highlights that lifestyle behaviors are shaped by physiological factors and multilayered contextual interactions, supporting the multidimensional approach of this study. Cognitive Reserve Theory proposes that regular lifestyle engagement enhances neuroplasticity and delays decline, while recognizing that deterioration can in turn undermine lifestyle behaviors over time (Jauny et al., 2022; Stern, 2002). Activity Theory further suggests that sustained participation in personal and social activities promotes cognitive health (Havighurst, 1961), consistent with the bidirectional link between decline and reduced social or occupational engagement.
Healthy lifestyle factors such as physical activity, social participation, and diet are associated with reduced risk of cognitive decline (Ngandu et al., 2015). Conversely, cognitive impairment may lower physical activity, increase social isolation, and promote unhealthy eating, thereby worsening cognitive health (Sutton et al., 2022). Yet causal inference between lifestyle and cognition remains limited. Many longitudinal studies emphasize average trends rather than the dynamic, bidirectional interplay between variables (Ngandu et al., 2022). Short follow-up periods and limited time points further constrain interpretation, conflating between-person differences with within-person changes (Borgeest et al., 2020; Kimura et al., 2019). Treating associations as static or cross-sectional may thus underestimate the complexity of lifestyle–cognition links (Heneghan et al., 2023). Addressing these gaps requires methods that capture within-person change and bidirectional interactions across time (Bloomberg et al., 2024).
The present study investigates the longitudinal association between lifestyle and cognitive function in middle- and older-aged adults from a bidirectional perspective. Specifically, we applied cross-lagged panel models (CLPMs) and random intercept cross-lagged panel models (RI-CLPMs) to examine temporal pathways between lifestyle—encompassing physical activity, nutrition, social relationships, and occupational participation—and cognitive function, while controlling for individual-level covariates.
Method
Study Design
This study employed a longitudinal quantitative design using secondary data from the Korean Longitudinal Study of Aging (KLoSA). The analysis examined long-term associations between lifestyle factors and cognitive function among older adults. This research was approved by the Institutional Review Board of Yonsei University (approval number: 1041849-202508-SB-169-01).
Data Source and Sample
The data for this study were drawn from the KLoSA, a nationally representative panel survey conducted by the Korea Employment Information Service to provide systematic statistics on population aging. KLoSA has followed household members aged 45 years and older biennially, collecting extensive information on demographic characteristics, family composition, health status, employment, occupation, income and consumption, subjective expectations, and quality of life, thereby providing a comprehensive dataset for socioeconomic and health policy research.
The baseline sample consisted of 10,254 respondents in the first wave. By the eighth wave, the retained sample included 5,717 individuals, with a panel retention rate of 77.1% (Korea Employment Information Service, 2022). This study utilized data from eight waves (time points) spanning 2006 (Wave 1) to 2020 (Wave 8). The dataset was merged across waves by respondent ID to construct repeated measures, yielding 11,174 person-wave observations. We excluded 1,202 participants who were newly enrolled or had incomplete responses, as well as 4,871 cases without integrated sampling weights.
The final analytic sample comprised 5,101 respondents. Missing data on the Mini-Mental State Examination (MMSE), used as the measure of cognitive function, ranged from 3.9% to 5.0% across waves. To address missingness while minimizing bias and preserving statistical power, we employed full information maximum likelihood (FIML), which uses all available information to estimate parameters under the assumption of missing at random.
Measurements
Observed Variables-Lifestyle
Lifestyle factors influencing health were defined based on the theoretical framework of Lifestyle-DEPER (Decision, Execution, Personal Factor, Environment, Resources) (Park et al., 2023). Health-related lifestyle indicators were operationalized into four domains: physical activity, nutrition, social relationships, and occupational participation. For this study, each domain was recoded into categorical variables.
Physical activity was assessed using two items: frequency of weekly exercise and average duration per session. Weekly total activity time (minutes) was calculated by multiplying these two variables. Following WHO (2020) guidelines, less than 75 minutes per week was coded as “1 = low activity,” 75–150 minutes as “2 = moderate activity,” and 150 minutes or more as “3 = sufficient activity.”
Nutrition was assessed using meal consumption patterns across two consecutive days (yesterday and the day before) (Cho, 2022). Skipping two or more meals per day (out of breakfast, lunch, dinner) was coded as a “skipped day.” Respondents who skipped meals on both days were coded as “1 = persistent skipping,” one skipped day as “2 = irregular intake,” and no skipped days as “3 = regular intake” (Yi et al., 2015).
Social relationships were measured using household size, frequency of contact with close friends, and contact with non-cohabiting parents and offspring (Choi & Jeon, 2021). Household status was dichotomized as “0 = living alone” and “1 = living with others,” and contact variables were dichotomized as less than once per week “0 = low connectivity” and once per week or more “1 = high connectivity.” The four indicators were summed to create a composite score (range: 0–4), which was categorized as “1 = disconnected” (0), “2 = limited” (1), and “3 = active” (≥2).
Occupational participation was measured using seven items on engagement in productive activities and participation in organized groups (religious, social, leisure, cultural, and sports) (Lim & Park, 2023). Productive activity was recoded as a binary variable: “0 = not engaged” and “1 = engaged,” and group participation was recoded as “0 = less than once per week” and “1 = regular participation” (≥ once per week). The indicators were summed to create a composite score (range: 0–7), which was categorized as “1 = no participation” (0), “2 = limited participation” (1), and “3 = diverse participation” (≥2).
The composite lifestyle index was constructed as a continuous variable by summing the recoded scores across the four domains.
Observed Variables—Cognitive Function
Cognitive function was assessed using the Korean version of the Mini-Mental State Examination (K-MMSE), a widely used screening tool for older adults. The K-MMSE evaluates five domains: orientation, memory, attention, language, and visuospatial ability (Kwon, 1989; Park, 1989). In this study, the K-MMSE total score was treated as a continuous variable, with higher scores indicating better cognitive function.
Sociodemographic Factors and Covariates
The sociodemographic variables included in this study were gender, age, educational level, residential area, smoking, alcohol consumption, and disability status. Gender was coded as male (0) and female (1), and age was recategorized as ≤64 years (0) and ≥65 years (1). Educational level was classified as no formal education (0), elementary school graduate (1), middle school graduate (2), high school graduate (3), and college graduate or higher (4). The residential area was categorized into metropolitan (1), small- to medium-sized cities (2), and rural areas (3). Marital status, smoking, alcohol consumption, and disability status were coded as absent (0) or present (1).
To estimate the temporal effects between lifestyle and cognitive function, gender, age, smoking, alcohol consumption, and disability status were included as covariates. These covariates were incorporated into the observed variables at each wave to control for the influence of individual background characteristics.
Data Analysis
To examine the longitudinal relationship between lifestyle and cognitive function, we applied both the CLPM and the RI-CLPM. All analyses were conducted using Mplus version 8.9, employing the Robust Maximum Likelihood Estimation (MLR) method. Missing values were handled using FIML. CLPM allows for the estimation of autoregressive and cross-lagged effects over time, but it does not control for stable between-person heterogeneity. To address this limitation, RI-CLPM was employed, which separates stable between-person differences through random intercepts and thereby minimizes bias in cross-lagged effects, allowing for the analysis of within-person changes (Hamaker et al., 2015; Mulder & Hamaker, 2021).
Descriptive statistics were used to examine the sociodemographic characteristics of participants, and means, standard deviations, skewness, kurtosis, and Pearson correlations were computed for key study variables. Based on CLPM and RI-CLPM, causal associations between lifestyle and cognitive function were analyzed at both the between-person and within-person levels. Six constrained models were compared to evaluate model fit: (1) an unconstrained model, (2–3) equality constraints on autoregressive effects, (4–5) equality constraints on cross-lagged effects, and (6) equality constraints on error covariances (Supplemental 1).
Model fit was assessed using multiple indices: the Comparative Fit Index (CFI) and Tucker–Lewis Index (TLI), with values ≥ 0.90 indicating acceptable fit; the Root Mean Square Error of Approximation (RMSEA), with values ≤ 0.08 considered acceptable and ≤ 0.05 considered good; and the Standardized Root Mean Square Residual (SRMR), with values ≤ 0.08 indicating acceptable fit (Kline, 2016). For the final selected model, covariates including sex, age, smoking, drinking, and disability status were included to control for potential confounding effects.
Results
Demographic Characteristics of the Sample
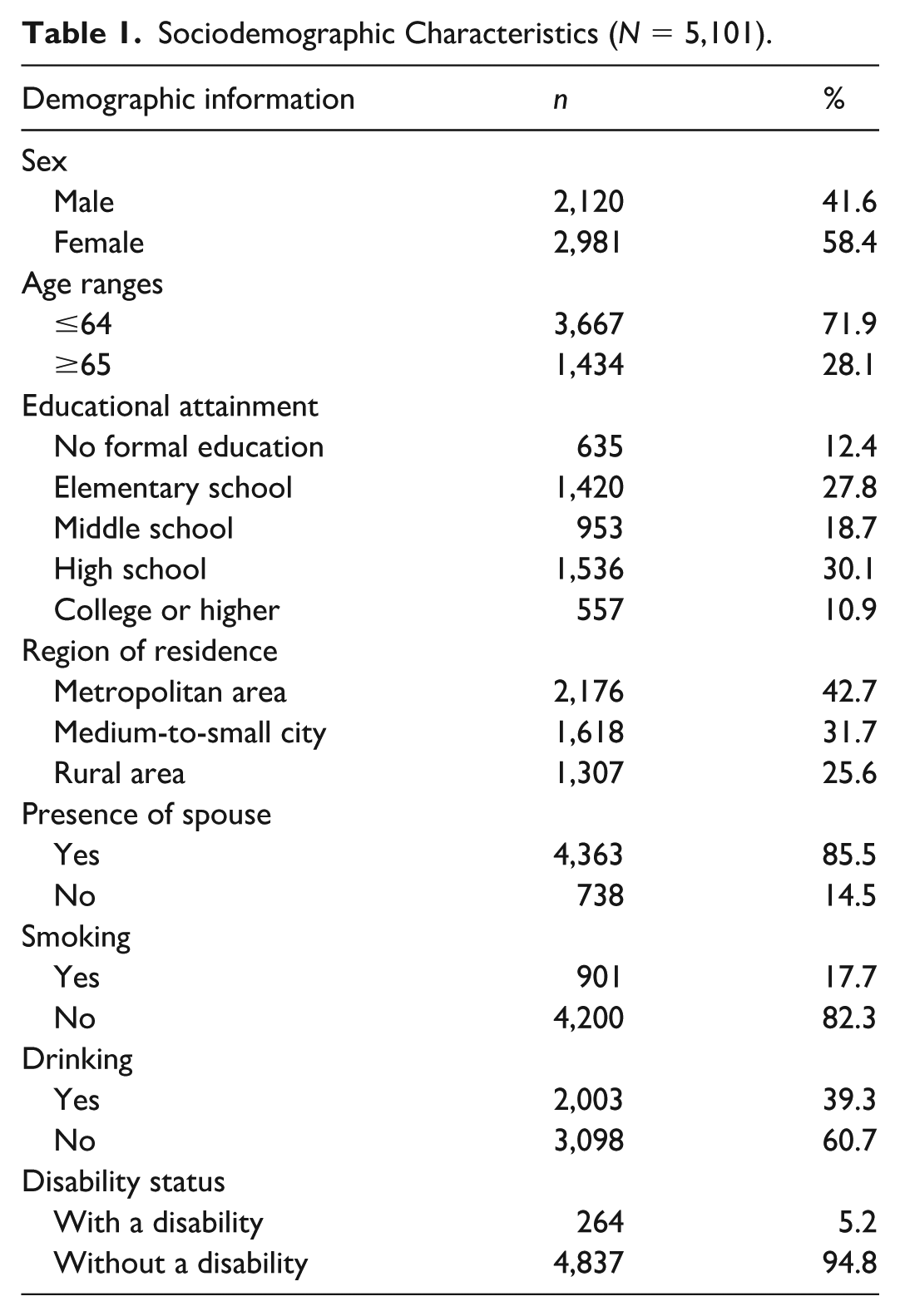
Among the study participants, women accounted for 2,981 individuals (58.4%), a higher proportion than men. By age group, 3,667 participants (71.9%) were aged 64 years or younger, while 1,434 participants (28.1%) were aged 65 years or older. Regarding education level, 635 (12.4%) had no formal education, 1,420 (27.8%) had completed elementary school, 953 (18.7%) had completed middle school, 1,536 (30.1%) had completed high school, and 557 (10.9%) had attained college or higher education. In terms of residential area, the largest group resided in metropolitan areas (n = 2,176, 42.7%), followed by small-to-medium cities (n = 1,618, 31.7%) and rural areas (n = 1,307, 25.6%). Marital status showed that 4,363 participants (85.5%) had a spouse. For health-related behaviors, 4,200 (82.3%) were non-smokers and 3,098 (60.7%) were non-drinkers. In addition, 4,837 (94.8%) reported having no disabilities (Table 1).
Sociodemographic Characteristics (N = 5,101).
Descriptive Statistics and Correlations of Key Variables
The correlations of key variables across measurement waves are presented in Supplemental 2. None of the correlation coefficients exceeded .90, indicating no multicollinearity concerns. Lifestyle variables at each wave were positively and significantly correlated (r = .203 to .616, p < .01). Adjacent waves of lifestyle showed relatively high correlations, confirming temporal stability across repeated measures. Cognitive function variables were also significantly and positively correlated across waves (r = .509 to .741, p < .01), with stronger autocorrelations observed in later waves.
The correlations between lifestyle and cognitive function were statistically significant and positive at all measurement points, ranging from weak (r = .137, p < .01) to moderate levels (r = .422, p < .01). These associations tended to become stronger in the later waves, suggesting that the relationship between lifestyle and cognitive function increased over time.
Normality assumptions for the distribution of each variable across waves were assessed using skewness and kurtosis. All absolute values were within the recommended thresholds (skewness < 2, kurtosis < 7), satisfying the criteria for normality (Kline, 2016).
Model Fit Analysis of Lifestyle and Cognitive Function
The model fit indices for the equality-constrained models of the CLPM and RI-CLPM are presented in Table 2. For the CLPM, the unconstrained model (Model 1) demonstrated the best overall fit (CFI = .993, TLI = .989, RMSEA = .021, SRMR = .015) and the lowest Akaike information criterion (AIC; 326,129.463). However, when considering statistical parsimony, the constrained model with equal cross-lagged effects of lifestyle (Model 4) showed comparable fit indices (CFI = .993, TLI = .989, RMSEA = .021, SRMR = .017) and yielded the lowest Bayesian information criterion (BIC; 326,636.878), suggesting that this model was more parsimonious. Similarly, for the RI-CLPM, Model 1 exhibited acceptable fit (CFI = .989, TLI = .981, RMSEA = .028, SRMR = .034), while Model 4 provided nearly equivalent fit (CFI = .988, TLI = .981, RMSEA = .027, SRMR = .035) but demonstrated the lowest BIC (326,802.075), indicating greater parsimony.
Model Fit Indices for CLPM and RI-CLPM.
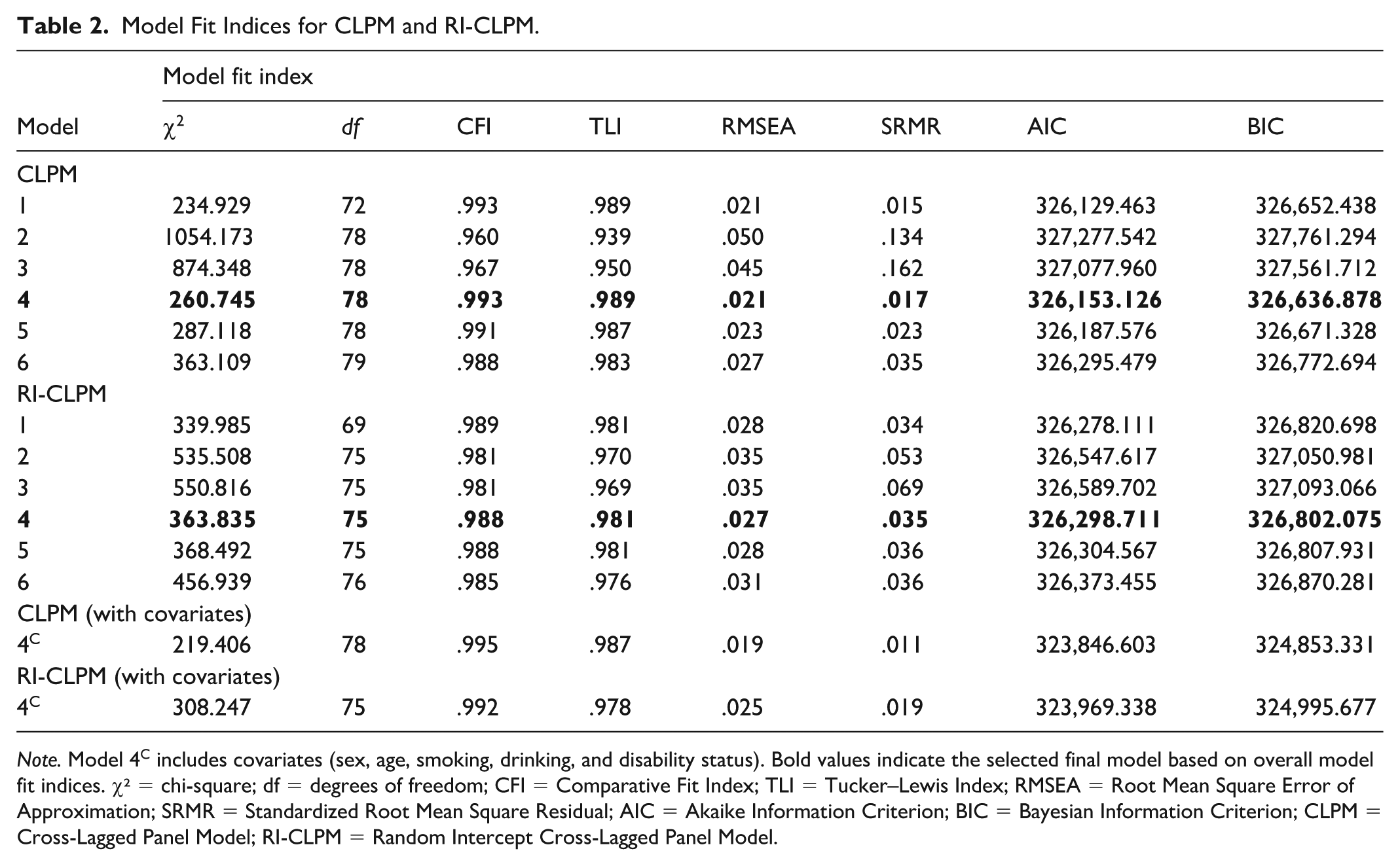
Note. Model 4C includes covariates (sex, age, smoking, drinking, and disability status). Bold values indicate the selected final model based on overall model fit indices. χ² = chi-square; df = degrees of freedom; CFI = Comparative Fit Index; TLI = Tucker–Lewis Index; RMSEA = Root Mean Square Error of Approximation; SRMR = Standardized Root Mean Square Residual; AIC = Akaike Information Criterion; BIC = Bayesian Information Criterion; CLPM = Cross-Lagged Panel Model; RI-CLPM = Random Intercept Cross-Lagged Panel Model.
When covariates (age, sex, smoking, drinking, disability status) were incorporated into both the CLPM and RI-CLPM Model 4, the fit indices improved compared to the baseline models. Therefore, the constrained models with covariates were deemed the most appropriate analytical models, as they offered both parsimony and interpretability (Little, 2024).
Main Findings of CLPM and RI-CLPM
The standardized path coefficients for CLPM Model 4 and RI-CLPM Model 4 with covariates are presented in Table 3. Both models included autoregressive effects, cross-lagged effects, and synchronous correlations, while RI-CLPM additionally estimated between-person effects.
Standardized Path Coefficients of CLPM and RI-CLPM.
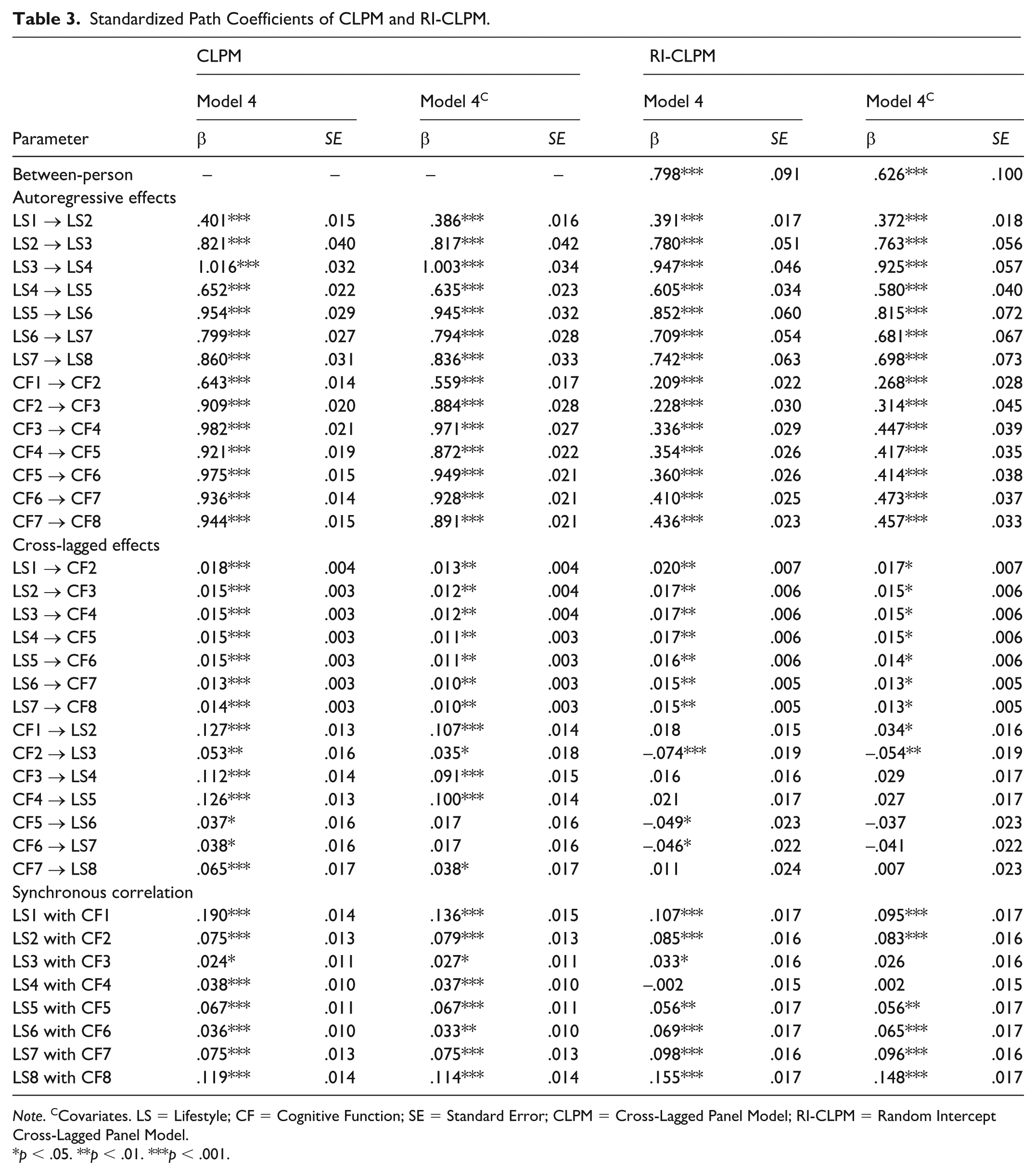
Note. CCovariates. LS = Lifestyle; CF = Cognitive Function; SE = Standard Error; CLPM = Cross-Lagged Panel Model; RI-CLPM = Random Intercept Cross-Lagged Panel Model.
p < .05. **p < .01. ***p < .001.
For both CLPM and RI-CLPM, the autoregressive paths of lifestyle and cognitive function in Model 4 were statistically significant (β = .209 to 1.016, p < .001). Cross-lagged effects were significant in most cases, except for the paths from cognition to lifestyle in RI-CLPM (β = .011 to .021, p > .05). Given that model fit indices improved with the inclusion of covariates, the interpretation primarily focused on the constrained models with covariates (Model 4C).
In the CLPM (Model 4C), as illustrated in Figure 1, the autoregressive paths of lifestyle and cognitive function were significant across all waves (β = .386 to 1.003, p < .001). Cross-lagged effects from lifestyle to subsequent cognitive function were consistently significant across waves (β = .010 to .013, p < .01), while the reverse paths from cognitive function to lifestyle were significant only at some time points (β = .013 to .015, p < .05). Synchronous correlations were significant and positive at all waves (β = .027 to .136, p < .05).

CLPM of lifestyle (LS) and cognitive function (CF) across T1–T8.
In the RI-CLPM (Model 4C), as illustrated in Figure 2, the between-person effect was statistically significant (β = .626, p < .001). At the within-person level, autoregressive effects of both lifestyle and cognitive function remained stable across all waves (β = .268 to .925, p < .001). Cross-lagged effects from lifestyle to subsequent cognitive function were consistently significant (β = .013 to .017, p < .05). By contrast, the reverse effects from cognitive function to lifestyle included both negative and positive coefficients but were only partially significant (β = −.054 to .034, p < .05). Synchronous correlations were generally significant, except for LS3 ↔ CF T3 and T4, where they did not reach significance (β = .056 to .148, p < .01).
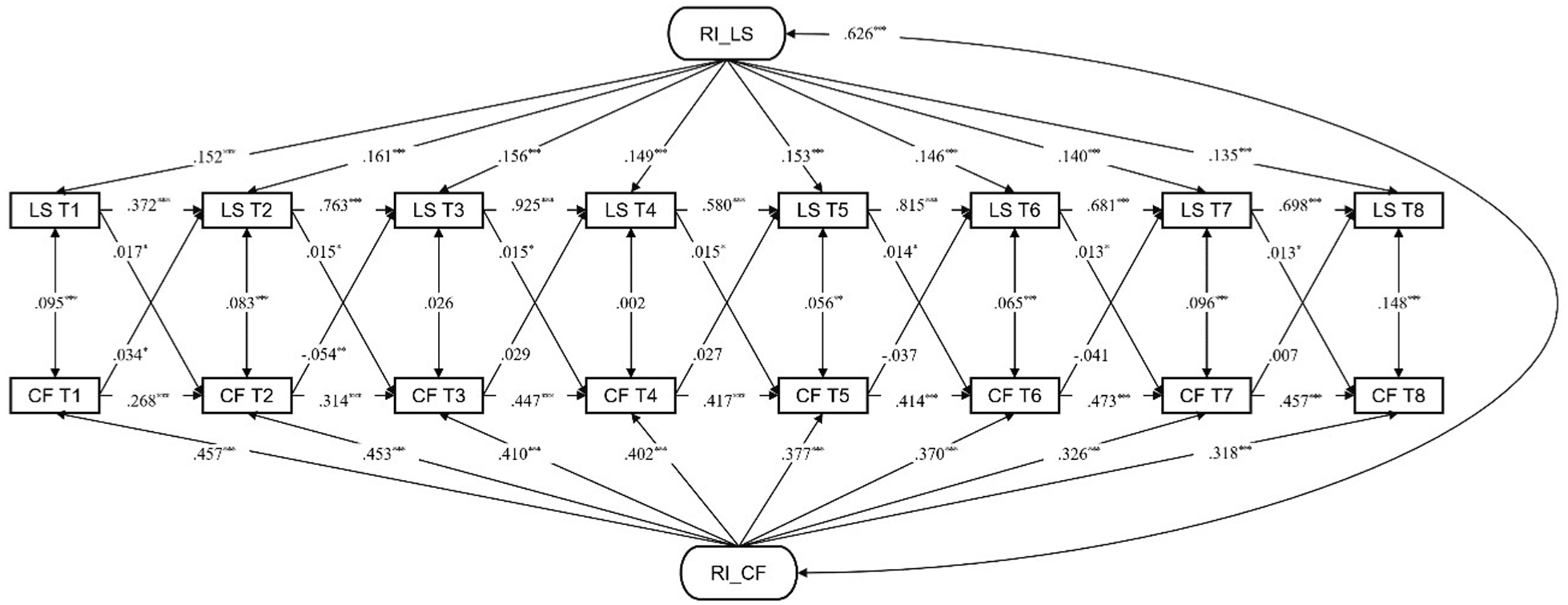
RI-CLPM of lifestyle (LS) and cognitive function (CF) across T1–T8.
Discussion
The multidimensional lifestyle of older adults is a protective factor that strengthens cognitive reserve and lowers the risk of cognitive decline and dementia (Kivipelto et al., 2020; Lourida et al., 2019). This study used the CLPM and RI-CLPM to examine the bidirectional relationship between lifestyle and cognitive function in middle-aged and older adults. CLPM results showed that lifestyle consistently predicted cognitive function across all time points. Although the effect sizes were modest, these findings suggest that multidimensional lifestyle is associated with cognitive function over time. In contrast, RI-CLPM revealed stable effects of lifestyle on cognition but largely nonsignificant reverse effects, suggesting a potential role of lifestyle in sustaining cognitive health.
Previous studies consistently show that lifestyle factors support cognitive function and help prevent decline (Dhana et al., 2020; Jia et al., 2023). However, many emphasized physiological factors such as physical activity, sleep, smoking, and alcohol use or relied on cross-sectional designs that could not capture temporal changes or reciprocal effects. Few have tested the reverse pathway by which cognitive decline influences lifestyle behaviors (Wen et al., 2025). Using CLPM and RI-CLPM, this study extends prior research by incorporating multidimensional lifestyle factors—including physiological and psychosocial elements—and statistically estimating the reciprocal relationship between lifestyle and cognition over time while distinguishing within-person from between-person processes (Hamagami & McArdle, 2001; Mund & Nestler, 2019).
The CLPM results underscored the consistent but modest longitudinal association between lifestyle and cognition, aligning with prior findings that multidimensional lifestyle factors strengthen cognitive reserve by supporting neural efficiency and adaptive mechanisms (Lourida et al., 2019; Stern, 2002). Nevertheless, CLPM is constrained by its focus on average population trends, without disentangling stable between-person differences from within-person fluctuations (Mund & Nestler, 2019). Thus, while affirming the role of lifestyle as a primary pathway for maintaining cognitive health, CLPM results must be interpreted with caution.
The RI-CLPM provided more nuanced insights by separating between-person and within-person effects (Mulder & Hamaker, 2021). Results showed sustained effects of lifestyle on cognition but nonsignificant reverse effects from cognition to lifestyle. This suggests that accumulated lifestyle patterns are relatively stable and not easily altered by short-term decline. These findings align with Activity Theory, which emphasizes the stabilizing role of ongoing activities (Havighurst, 1961), and Cognitive Reserve Theory, which highlights the protective impact of cumulative lifestyle engagement (Stern, 2002). The nonsignificant reverse effects may also reflect individual or contextual variability: some individuals reduce activities sharply after decline, while others maintain engagement through social or familial support (Weng et al., 2018). Overall, the lifestyle–cognition relationship is not uniform but may be moderated by personal and contextual factors, underscoring the need for future research on moderators such as social support, health status, and education.
The present study contributes to the literature by analyzing the reciprocal associations between lifestyle and cognition using longitudinal data. Unlike prior studies that focused narrowly on physiological variables, this study incorporated psychosocial elements such as social relationships and occupational participation, thereby providing a broader interpretation of how multidimensional lifestyle factors interact with cognition. By applying both the CLPM and RI-CLPM, the study distinguished between- and within-person processes and revealed temporal dynamics that are often overlooked in unidirectional approaches. These findings underscore that lifestyle may contribute to cognitive health over time, whereas the influence of cognitive decline on lifestyle appears to be is more context-dependent. From a clinical perspective, these findings support the integration of socially embedded roles and meaningful occupational participation with key physiological lifestyle factors such as physical activity, diet, sleep, and substance use in the promotion of cognitive health. Consequently, a multidimensional lifestyle that includes psychosocial factors is associated with cognitive function over time and may support cognitive health, providing empirical evidence for occupational therapy interventions that promote social and occupational engagement in older adults.
Several limitations must also be acknowledged. The longitudinal data were derived from a selective cohort, which may restrict generalizability. The fixed 2-year intervals limited the ability to detect short-term fluctuations. In addition, nutrition was assessed based on meal consumption, which does not capture detailed dietary intake and may limit measurement precision. Cognitive function was assessed using the MMSE, a screening tool that may be subject to ceiling effects, limited sensitivity to subtle changes, and insufficient coverage of executive function. While RI-CLPM enabled the separation of between-person and within-person effects, it could not fully account for heterogeneity in within-person pathways. In addition, the use of constrained models to ensure statistical parsimony may have reduced analytic flexibility, potentially overlooking complex interactions or heterogeneous patterns. Future research should employ more flexible modeling strategies, sensitive assessment tools, and objective longitudinal tracking methods to capture nuanced temporal processes and individual variability more accurately.
Conclusion
This study longitudinally examined the relationship between lifestyle and cognitive function in middle-aged and older adults using both the CLPM and RI-CLPM, showing that lifestyle is modestly associated with cognitive health over time. Although the effect sizes were relatively small, the findings suggest that a multidimensional lifestyle including physiological factors such as physical activity and nutrition and psychosocial elements such as social relationships and occupational participation may contribute to the maintenance of cognitive function. In contrast, reverse effects of cognition on lifestyle were limited, suggesting that accumulated lifestyle patterns are relatively stable and not easily altered by short-term decline. These results highlight the potential importance of multidimensional lifestyle as a key intervention for promoting cognitive health and provide practical evidence for designing management programs for older adults at both policy and clinical levels. Furthermore, the study supports the need for tailored health strategies that reflect the specific characteristics of older adults, emphasizing preventive lifestyle management as an important approach for sustaining cognitive health in aging societies.
Supplemental Material
sj-docx-1-otj-10.1177_15394492261452169 – Supplemental material for Bidirectional Association Between Lifestyle and Cognitive Function in Aging Adults
Supplemental material, sj-docx-1-otj-10.1177_15394492261452169 for Bidirectional Association Between Lifestyle and Cognitive Function in Aging Adults by Young-Myoung Lim and Ji-Hyuk Park in OTJR: Occupational Therapy Journal of Research
Footnotes
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Review Board of Yonsei University (approval number: 1041849-202508-SB-169-01).
Consent to Participate
The requirement for written informed consent was waived by the board because the study involved the secondary analysis of de-identified, publicly available data and posed minimal risk to participants.
Author Contributions
Young-Myoung Lim was responsible for conceptualization, methodology design, data analysis, and preparation of the original draft, including visualization of the results. Ji-Hyuk Park contributed to the conceptualization of the study, provided supervision throughout the research process, and participated in reviewing and editing the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data used in this study were obtained from the Korean Longitudinal Study of Aging (KLoSA), a publicly accessible dataset provided by the Korea Employment Information Service.
Patient and Public Involvement Statement
No patient or public involvement. This study was based on secondary analysis of anonymized, publicly available data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.