
Abstract
Driving self-efficacy influences driving behavior and decisions about continuing to drive, yet no validated Japanese measure has been available. This study examined the reliability and validity of the Japanese version of the Adelaide Driving Self-Efficacy Scale (ADSES-J) in 100 community-dwelling licensed drivers, with a 2-week retest in 20 participants. Internal consistency was assessed using Cronbach’s α and test–retest reliability using ICC (2,1). Convergent validity was examined through correlations with driving-related measures, and discriminant validity through correlations with general self-efficacy and mental health scales. Exploratory factor analysis supported a unidimensional structure explaining 71.6% of the variance. The ADSES-J demonstrated excellent internal consistency (α = .962) and test–retest reliability (ICC = .965), with no floor or ceiling effects at the total score level, although Item 1 showed a ceiling effect. These findings indicate that the ADSES-J is a reliable and valid instrument for assessing driving-specific self-efficacy among community-dwelling drivers in Japan.
Plain Language Summary
Automobile driving supports community life through commuting, shopping, and social participation. For many people, including older adults and individuals with brain injuries, driving helps maintain independence and social roles. When considering whether to continue or resume driving safely, it is important not only to assess driving ability but also how accurately individuals judge their own ability. Driving self-efficacy refers to a person’s belief in their capability to manage driving situations safely and effectively. This study examined the reliability and validity of the Japanese version of the Adelaide Driving Self-Efficacy Scale (ADSES-J) in community-dwelling drivers in Japan. We surveyed 100 licensed drivers who had driven within the past year, and 20 participants completed the questionnaire again after two weeks to examine score stability. We evaluated whether the items consistently measured a single concept and whether scores were stable over time. We also examined how ADSES-J scores related to driving-related measures, including driving style and driving workload, and whether the scores were distinct from general self-efficacy and mental health. In addition, we assessed the questionnaire’s factor structure. The ADSES-J showed excellent internal consistency and very high test–retest reliability. The total score did not show floor or ceiling effects, although one item showed a ceiling effect. ADSES-J scores were positively associated with confidence in driving skills and negatively associated with several aspects of driving workload, but were not associated with general self-efficacy or mental health. Factor analysis supported a clear one-factor structure. These findings indicate that the ADSES-J is a reliable and valid tool for assessing driving-specific self-efficacy in Japan. It may support discussions about driving safety and appropriate driving support. Further studies in older and clinical populations are needed.
Introduction
Automobile driving is an essential mode of transportation that supports community life through commuting, shopping, and social participation. For many individuals, including older adults and those with brain injuries, driving is vital for maintaining independence in daily life and fulfilling social roles. However, age- or disease-related declines in cognitive and physical function can impair driving ability. When considering the safe continuation or resumption of driving, it is crucial not only to assess driving ability but also to evaluate the accuracy of one’s self-appraisal, including driving self-efficacy (Hatakka et al., 2002).
According to Bandura (1997), self-efficacy refers to the belief in one’s capability to perform tasks and achieve goals in specific situations. This psychological factor influences behavioral initiation, persistence, and adaptation in response to stress. Overestimated self-efficacy carries the risk of failure as a result of excessive challenges, whereas underestimated self-efficacy may inhibit the full expression of one’s abilities. In the driving domain, self-efficacy and risk perception have been shown to correlate with self-reported driving behaviors (Morisset et al., 2010), and overconfidence in driving ability is associated with increased crash risk (Wood et al., 2013).
More recent studies have broadened the focus to include decision-making about driving cessation and mobility transition in later life.
Betz et al. (2022) reported that an online decision aid for older drivers reduced decisional conflict and improved knowledge regarding whether to continue or stop driving. Fields et al. (2023) argued that self-efficacy is relevant to the transition from driving to alternative transportation, and Park (2022) reported an association between driving efficacy and driving fitness in older adults with generalized anxiety disorder.
Together, these recent studies suggest that self-efficacy is relevant not only to driving performance but also to decision-making and adaptation related to mobility in later life.
Against this background, the assessment of driving self-efficacy remains important not only for understanding perceived driving ability but also for supporting clinical judgment and communication about safe driving continuation, cessation, and mobility planning. Therefore, reliable and valid instruments are needed to quantify driving-specific self-efficacy.
The Adelaide Driving Self-Efficacy Scale (ADSES; George et al., 2007), widely used internationally, assesses drivers’ confidence or self-efficacy across various driving scenarios. Previous studies in post-stroke drivers have shown that higher driving self-efficacy correlates with better performance on driving tests (Stapleton et al., 2012), whereas low self-efficacy in older drivers is associated with reduced driving frequency and distance (McNamara et al., 2015). Thus, the ADSES is applicable to a broad range of populations, from individuals with brain injuries to older adults.
In addition to the original Australian version, Norwegian (Rike et al., 2015), Korean (Park & Kim, 2019), and Persian (Havaei et al., 2021) versions of the ADSES have been developed. However, the findings of these studies should be interpreted cautiously rather than treated as directly comparable. The target populations of these previous studies differed substantially, including drivers after brain injury, general licensed drivers, and older adults, and such differences are likely to influence score distributions, item relevance, and the likelihood of floor or ceiling effects. In addition, the scope of psychometric evaluation was not identical across studies, and the studies were conducted in different cultural and traffic environments. Therefore, favorable findings from previous studies should not be interpreted as evidence of automatic generalizability to Japanese drivers.
In Japan, research specifically addressing driving self-efficacy remains limited, and validated measures for assessing this construct have not been sufficiently available. We translated the ADSES into Japanese (ADSES-J) following the International Society for Pharmacoeconomics and Outcomes Research Task Force guidelines (Wild et al., 2005), and content validity was verified (Kagino et al., 2023). However, the psychometric properties of the ADSES-J—such as reliability (for example, internal consistency and test–retest reliability) and validity (for example, construct validity)—have not yet been sufficiently examined.
This study aimed to clarify the psychometric properties of the ADSES-J among community-dwelling drivers. Specifically, we evaluated (a) internal consistency, (b) test–retest reliability, and (c) construct validity using driving-related and general self-efficacy or mental health scales to confirm its usefulness as a driving self-efficacy assessment tool in Japan.
Method
Participants and Sample Size
Community-dwelling licensed adult drivers who provided written informed consent were included. Participants were recruited through convenience sampling via the authors’ professional networks, including family members of the authors and co-investigators, staff of affiliated institutions, university students, and their relatives or acquaintances.
The inclusion criteria were as follows: (a) possession of a valid Japanese driver’s license and (b) active driving within the past year. Individuals with self-reported neurological, psychiatric, or musculoskeletal conditions that could substantially affect driving ability were excluded.
The analysis in this study was conducted with reference to the COSMIN checklist. Regarding sample size recommendations for psychometric studies, the COSMIN checklist suggests a minimum of 100 participants for examining reliability and validity (Mokkink et al., 2010; Prinsen et al., 2018; Terwee et al., 2007). In addition, 20 participants were randomly selected from the obtained sample to evaluate test–retest reliability.
Measures
The ADSES-J was used to assess driving self-efficacy. To evaluate validity, the Driving Style Questionnaire (DSQ; 18 items, 8 subscales; Ishibashi et al., 2007) and the Workload Sensitivity Questionnaire (WSQ; 38 items, 10 subscales; Ishibashi & Okusa, 2008) were used as driving-related measures for convergent validity. For discriminant validity, the General Self-Efficacy Scale (GSES; 16 items; Sakano & Tojo, 1986; Schwarzer & Jerusalem, 1995) and the General Health Questionnaire (GHQ-12; 12 items; Goldberg, 1972; Goldberg & Williams, 1988; Nakagawa & Daibo, 1996) were used as indicators of general self-efficacy and mental health, respectively. The reliability and validity of each scale have been reported in previous studies. Details for each measure are provided below.
ADSES-J
The ADSES-J is a self-report measure consisting of 12 items assessing confidence in performing a range of driving situations. Each item is rated on an 11-point scale from 0 to 10, and total scores range from 0 to 120, with higher scores indicating greater driving self-efficacy. The scale includes items related to common driving situations involving traffic complexity, visibility, traffic sign and signal response, merging, and parking, based on the published Japanese version of the ADSES-J.
Driving-Related Measures for Convergent Validity
Driving Style Questionnaire
This questionnaire evaluates psychological characteristics such as attitudes, orientations, and thoughts toward driving. It comprises 18 items rated on a 4-point scale and comprises eight subscales: Confidence in driving skills, Passivity toward driving, Impatient driving tendency, Meticulous driving tendency, Advance preparation for signals, Car as a status symbol, Unstable driving tendency, and Worrisome tendency.
Workload Sensitivity Questionnaire
This questionnaire measures the types and degree of workload sensitivity associated with driving. It consists of 38 items rated on a 5-point scale and assesses 10 subscales: Traffic situation awareness, Road environment awareness, Driving concentration impairment, Reduced physical activity, Driving pace impairment, Physical discomfort, Route awareness/searching, In-car environment, Control operation, and Driving posture.
Measures for Discriminant Validity
General Self-Efficacy Scale
The GSES measures the level of general self-efficacy cognition and consists of 16 items answered with “Yes” or “No.” The total score ranges from 0 to 16, with higher scores indicating higher self-efficacy.
Twelve-Item General Health Questionnaire
The GHQ-12 assesses general mental health status and consists of 12 items. Respondents rate each item on a 4-point scale reflecting non-specific psychological distress, including depressed mood, anxiety, impaired social functioning, and dissatisfaction with daily activities. Higher scores indicate poorer mental health status.
Procedure
Participants completed all questionnaires in a single session. To evaluate the test–retest reliability of the ADSES-J, 20 participants completed a retest 2 weeks later. No additional assessments or interventions were conducted during the interval.
Analysis
Descriptive Statistics and Distribution
Participants with incomplete questionnaires were excluded, and only complete cases were analyzed. For the ADSES-J total score, the mean, standard deviation (SD), and range were calculated, and the score distribution was examined. Floor and ceiling effects were considered present if ≥ 15% of respondents achieved the minimum or maximum score (Terwee et al., 2007).
Reliability
Internal consistency was assessed using Cronbach’s α. Values of .61–.70 were considered acceptable, .71–.80 good, and .81–.90 excellent (Taber, 2018). Test–retest reliability was assessed using the intraclass correlation coefficient (ICC [2,1]) for total scores and weighted κ for individual items, with 95% confidence intervals (Koo & Li, 2016). Cohen’s weighted κ was interpreted based on Fleiss’s criteria (Fleiss et al., 1981): poor (κ < .40), fair to good (.40 ≤ κ < .75), and excellent (κ ≥ .75). Measurement error indices included the standard error of measurement (SEM) and the minimal detectable change at the 95% confidence level (MDC95), calculated as 1.96 × √2 × SEM.
Validity
Convergent and Discriminant Validity
Correlations between ADSES-J scores and other scales were examined using Spearman coefficients. For convergent validity, we hypothesized moderate or stronger correlations (|r| ≥ 0.40) with the DSQ and WSQ, specifically a positive correlation with the DSQ “confidence in driving skills” subscale and negative correlations with WSQ subscales. For discriminant validity, we hypothesized weak or negligible correlations (|r| ≤ .20) with the GSES and GHQ-12 (George et al., 2007; McNamara et al., 2015; Williams & Rhodes, 2016).
Structural Validity
To examine structural validity, an exploratory factor analysis (EFA) was conducted using principal axis factoring. The suitability of the data for factor analysis was assessed using the Kaiser–Meyer–Olkin (KMO) measure and Bartlett’s test of sphericity. Factors with eigenvalues greater than 1 were retained, and the scree plot was examined to determine the number of factors. Given the psychological nature of the construct, correlations among factors were allowed. Factor loadings ≥.40 were considered meaningful. If more than one factor was retained, a promax rotation was applied to allow for correlated factors.
The significance level was set at p < .05. Analyses were performed using IBM SPSS Statistics, version 27.0.
Ethical Considerations
Participants received written and verbal explanations and provided written informed consent. The study was approved by an institutional ethics review committee (Approval No. 2023-066) and conducted in accordance with the principles of the Declaration of Helsinki.
Results
Participant Demographics
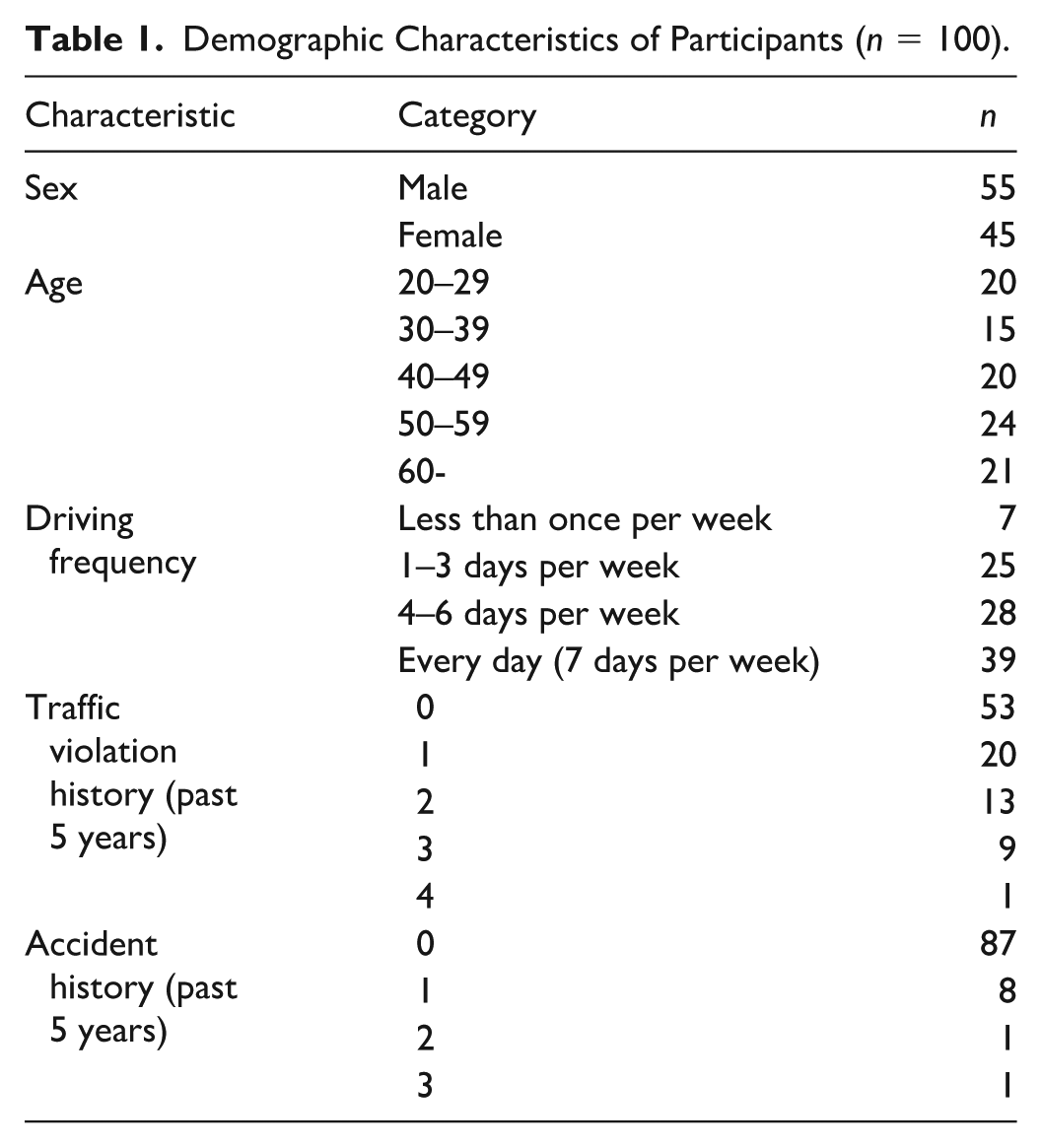
A total of 104 participants were recruited. Four participants were excluded because of incomplete questionnaire responses, leaving 100 participants for analysis. Twenty participants completed the retest. Table 1 presents the basic attributes of the participants (n = 100). The mean age was 46.8 years (SD = 16.8), and 55% were male. Driving frequency was as follows: daily 39%, 4–6 days/week 28%, 1–3 days/week 25%, and <1 day/week 7%. Within the past 5 years, 47% reported at least one traffic violation, and 13% at least one crash; the majority reported neither.
Demographic Characteristics of Participants (n = 100).
Floor and Ceiling Effects
The total score range for the ADSES-J was 11–120 points, with a mean score of 75.5 (±22.7). Participants were rarely clustered near the minimum score of 11 or the maximum score of 120, with only one participant near the minimum and four near the maximum, both representing <5% of the total. At the total score level, no floor or ceiling effects were observed (9% at the maximum). However, item-level analysis revealed a ceiling effect for Item 1 (22%), exceeding the 15% threshold (Table 2). This finding suggests limited discrimination at the higher end for this specific driving situation.
Descriptive Statistics and Floor/Ceiling Effects of the ADSES-J Items and Total Score.
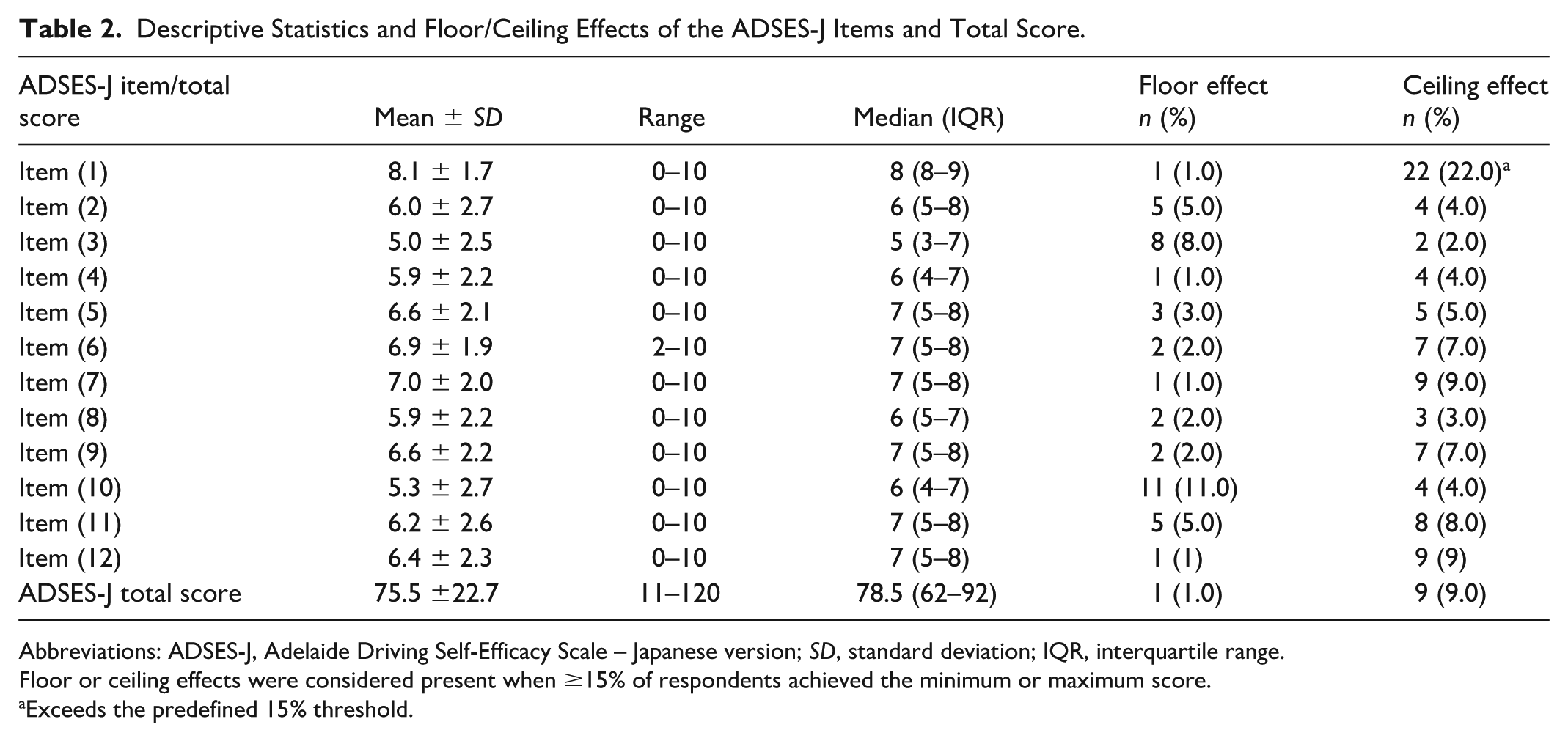
Abbreviations: ADSES-J, Adelaide Driving Self-Efficacy Scale – Japanese version; SD, standard deviation; IQR, interquartile range.
Floor or ceiling effects were considered present when ≥15% of respondents achieved the minimum or maximum score.
Exceeds the predefined 15% threshold.
Reliability
Internal consistency: Cronbach’s α for the ADSES-J total score was .96, indicating excellent internal consistency (Table 3).
Test–Retest Reliability and Measurement Error of the ADSES-J Total Score and Item-Level Agreement.
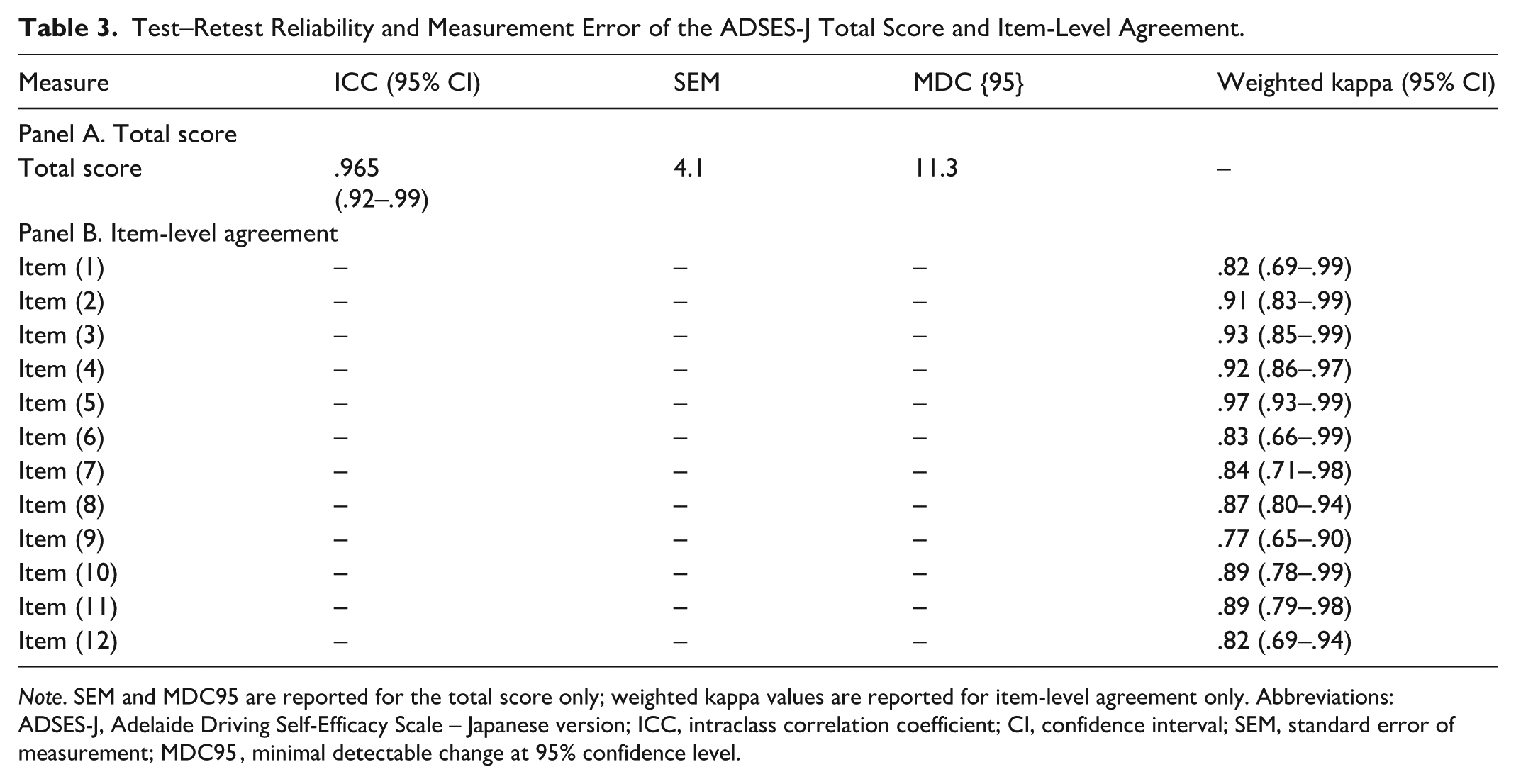
Note. SEM and MDC95 are reported for the total score only; weighted kappa values are reported for item-level agreement only. Abbreviations: ADSES-J, Adelaide Driving Self-Efficacy Scale – Japanese version; ICC, intraclass correlation coefficient; CI, confidence interval; SEM, standard error of measurement; MDC95 , minimal detectable change at 95% confidence level.
Test–retest reliability: Over a 2-week interval (n = 20), the total score showed ICC (2,1) = .965. Item-level weighted κ ranged from .77 to .97, with all items having κ ≥ .75. Measurement error indices were SEM = 4.06 and MDC95 = 11.26; estimates from a difference-score method (SEM = 4.14; MDC95 = 11.47) were comparable.
Validity
Convergent Validity
Driving-related scales: On the DSQ, ADSES-J correlated positively with Confidence in driving skills (ρ = .54, p < .01) and negatively with Passivity (ρ = −.31, p < .05) and Worry tendency (ρ = −.38, p < .01; Table 4). On the WSQ, significant negative correlations were observed with Traffic situation awareness (ρ = −.52, p < .01), Road environment awareness (ρ = −.50, p < .01), Driving concentration impairment (ρ = −.55, p < .01), Reduced physical activity (ρ = −.41, p < .01), Driving pace impairment (ρ = −.28, p < .01), Physical discomfort (ρ = −.23, p < .05), Route awareness/search (ρ = −.48, p < .01), In-car environment (ρ = −.39, p < .01), Control operation (ρ = −.050, p < .01), and Driving posture (ρ = −.33, p < .01). The hypothesized negative direction was supported; several subscales reached moderate correlations, whereas others were weaker. In contrast, no significant associations were found for several DSQ subscales related to stylistic or attitudinal tendencies (e.g., Impatience in driving, Meticulous driving).
Correlation Coefficients Between ADSES-J Total Score and Related Psychological and Driving Measures (n = 100).
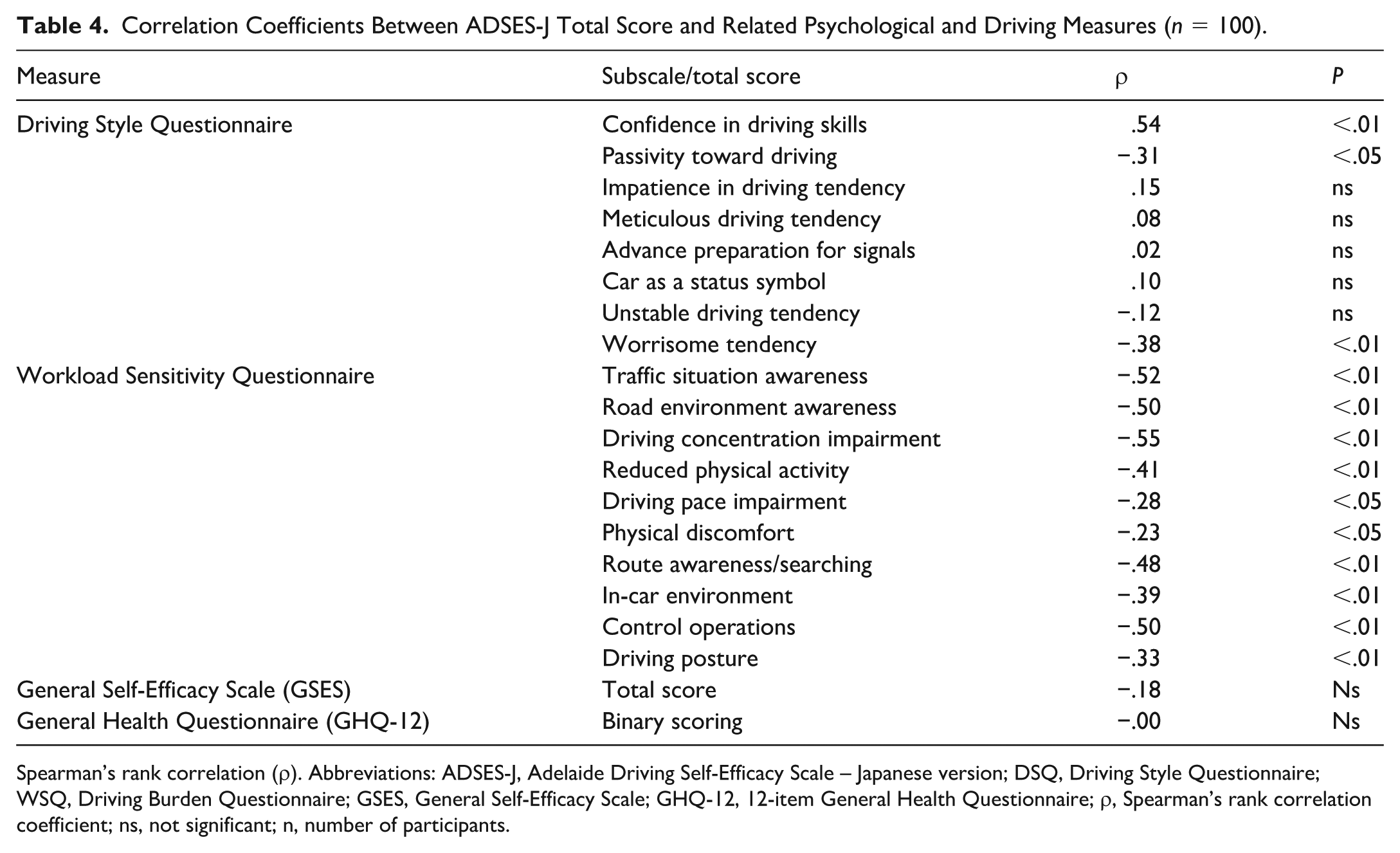
Spearman’s rank correlation (ρ). Abbreviations: ADSES-J, Adelaide Driving Self-Efficacy Scale – Japanese version; DSQ, Driving Style Questionnaire; WSQ, Driving Burden Questionnaire; GSES, General Self-Efficacy Scale; GHQ-12, 12-item General Health Questionnaire; ρ, Spearman’s rank correlation coefficient; ns, not significant; n, number of participants.
Discriminant Validity
No significant association was found between the GSES and the ADSES-J total score. Similarly, no significant correlation was observed between the GHQ-12 and the ADSES-J total score. As hypothesized, neither the GSES nor the GHQ-12 total scores showed a significant association with the ADSES-J total score. These results indicate that the ADSES-J measures domain-specific self-efficacy related to driving skills and is distinct from general self-efficacy and generic mental health indicators.
Structural Validity
The KMO measure of sampling adequacy was 0.93, indicating excellent suitability for factor analysis (Table 5). Bartlett’s test of sphericity was significant (χ² = 1297.19, df = 66, p < .001), confirming that the correlation matrix was appropriate for factor analysis.
Exploratory Factor Analysis of the ADSES-J Using Principal Axis Factoring (n = 100).
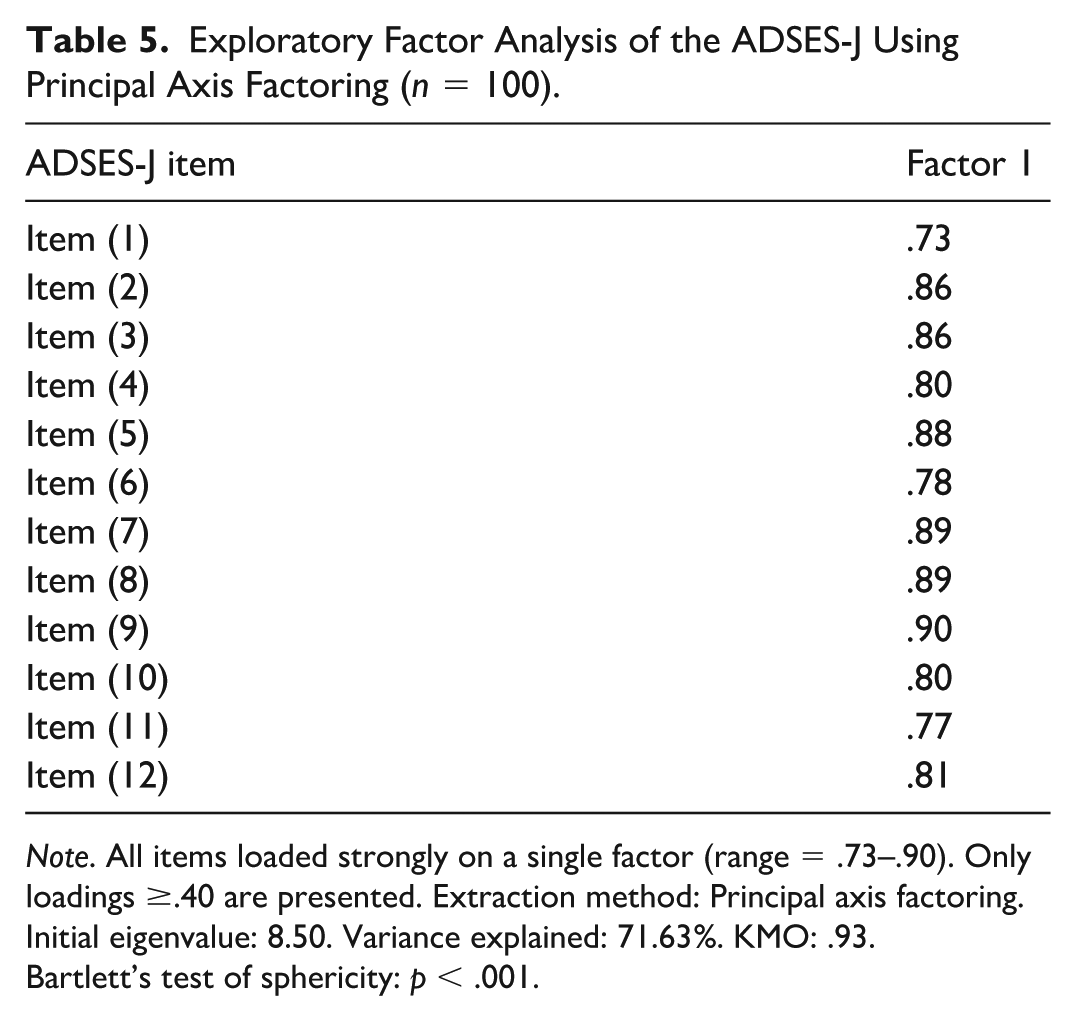
Note. All items loaded strongly on a single factor (range = .73–.90). Only loadings ≥.40 are presented. Extraction method: Principal axis factoring. Initial eigenvalue: 8.50. Variance explained: 71.63%. KMO: .93.
Bartlett’s test of sphericity: p < .001.
EFA revealed a single factor with an eigenvalue of 8.60, accounting for 71.6% of the total variance. All 12 items loaded strongly on this factor, with factor loadings ranging from .73 to.90. No secondary factors with eigenvalues greater than 1 were identified. These findings support a clear unidimensional structure of the ADSES-J. A single-factor solution was retained; therefore, rotation was not applicable.
Discussion
The present study provides strong evidence supporting the psychometric robustness of the ADSES-J. EFA demonstrated a clear unidimensional structure, with the first factor explaining 71.6% of the total variance and all items showing strong loadings (.73–.90). These findings confirm that driving self-efficacy, as assessed by the ADSES-J, represents a coherent and global domain-specific construct rather than multiple independent dimensions. Importantly, the strong single-factor structure provides empirical justification for the use of a total score and supports the assumption of unidimensionality underlying the calculation of Cronbach’s α. The internal consistency observed in the present study (α = .96) is consistent with that reported in the original Australian version (α = .98), which included stroke and non-stroke samples (George et al., 2007). Similarly, high reliability was reported in the Korean version (α = .98) among drivers with at least 1 year of driving experience (Park & Kim, 2019). Although the Persian version targeting older adults aged 60 years and above reported a lower coefficient (α = .77), it remained within an acceptable range (Havaei et al., 2021). Taken together, these findings suggest that the ADSES demonstrates generally stable internal consistency across different cultural contexts, age groups, and clinical backgrounds.
In terms of reliability, the ADSES-J demonstrated excellent internal consistency (α = .96) and outstanding test–retest reliability (ICC [2,1] = .97). Item-level stability was also high, with weighted κ values of .75 or greater for all items, indicating excellent agreement over the 2-week interval according to Fleiss’s criteria (Fleiss et al., 1981). These findings suggest that the scale yields highly stable measurements at the total score and individual item levels. The ICC observed in this study is comparable to those reported for other language versions of the ADSES, including the Korean version (ICC = .81) and the Persian version (ICC = .97), supporting the cross-cultural reproducibility of the scale.
Measurement error indices further supported score stability. The SEM was approximately 4 points, and the MDC95 was 11.26 points. Clinically, a change of approximately 12 points or more may be interpreted as a true change beyond random measurement error and may serve as a practical benchmark in intervention studies and clinical settings. Although the retest sample comprised only 20 participants and these estimates should therefore be interpreted with caution, the high ICC and consistent measurement error indices reinforce the reliability of the ADSES-J.
In examining convergent validity, the ADSES-J showed clear correlations with driving-related measures. Its positive correlation with “confidence in driving skills” and negative correlations with “passivity” and “worry tendency” on the DSQ suggest that the ADSES-J is meaningfully associated with participants’ perceived driving ability and driving-related attitudes. This aligns with findings from the original Australian ADSES (George et al., 2007), which reported that higher self-efficacy correlated with better performance on driving skill tests. Specifically, the strongest correlation was observed with confidence in driving skills, suggesting that the ADSES-J reflects a similar construct. Negative correlation with the WSQ suggest that individuals who report greater difficulty in maintaining awareness of traffic conditions, perceiving the road environment, or sustaining concentration while driving exhibit lower self-efficacy. Although several WSQ subscales demonstrated moderate correlations (|r| ≥ .40), others, such as Physical discomfort (ρ = −.23), showed weak but statistically significant associations. In addition, some subscales, such as Impatience in driving on the DSQ, did not demonstrate significant correlations. These findings suggest that some assessed by the WSQ subscales are more strongly related to driving self-efficacy than others. During validation of the original version, low self-efficacy among older adults was associated with reduced driving frequency and distance and with poorer on-road test performance (McNamara et al., 2015). Moreover, studies have shown that reduced attentional capacity for monitoring traffic conditions lowers on-road test performance (Devos et al., 2014). These findings support the present study’s result that difficulties in monitoring traffic conditions, perceiving the road environment, and maintaining concentration while driving correspond to lower self-efficacy. Overall, these findings support the convergent validity of the ADSES-J, as significant associations were observed for some DSQ subscales and for multiple WSQ subscales in the hypothesized directions.
The lack of significant associations with measures of general self-efficacy or mental health status, such as GSES and GHQ-12, indicates that driving self-efficacy is a domain- or behavior-specific construct. This demonstrates that it is distinct from general self-efficacy and overall mental health. Rodwell et al. (2022) reported that among parents of young drivers, parental driving self-efficacy (ADSES) was significantly associated with the quality of supervised driving practice, whereas parental general self-efficacy showed no such association. The GHQ-12 is designed as a measure of general mental health and theoretically does not overlap with task-specific self-efficacy for driving, aligning with the lack of association observed with ADSES. Research on older drivers (Toups et al., 2022) supports our findings, as driving performance primarily depends on cognitive function and driving skills rather than general mental health. Conversely, Park (2022) reported that anxiety exceeding a certain level affects driving self-efficacy among older drivers with generalized anxiety disorder, but found no strong linear relationship between anxiety scores and driving self-efficacy. These findings support the notion that driving self-efficacy is a task-specific concept distinct from general mental health or self-efficacy. Overall, no association was found at the total score level between GSES and GHQ-12, suggesting they are distinct constructs. Clinically, this indicates that the ADSES-J cannot be substituted for general mental health indicators and holds unique value for assessing self-efficacy specific to the driving task.
At the total score level, no ceiling effect was observed, suggesting that the ADSES-J demonstrates adequate discriminative capacity across a broad range of driving self-efficacy levels in community-dwelling drivers. However, at the item level, Item 1 showed a ceiling effect exceeding the recommended 15% threshold. This may reflect that certain relatively common or less demanding driving situations are perceived as highly manageable by most licensed drivers, resulting in clustering at the upper end of the scale. Although this item-level ceiling effect does not appear to compromise overall scale performance, it may indicate reduced sensitivity for detecting subtle improvements among individuals with already high self-efficacy in that specific driving context.
In summary, our findings support the ADSES-J’s ability to differentially assess driving-specific self-efficacy, positioning it as a potentially useful tool for evaluating driving self-efficacy among community-dwelling drivers in Japan. Further validation in older adults and clinical populations is required before broad clinical application. Self-efficacy is known to influence behavioral choices, attentional allocation, and performance under stress (Bandura, 1997). In the driving domain, higher self-efficacy has been reported to correlate with actual driving performance (George et al., 2007; Park & Kim, 2019). Furthermore, among older drivers, self-efficacy has been associated with decisions regarding continuing or discontinuing driving (Betz et al., 2022; Fields et al., 2023; Liddle et al., 2008). The findings of this study are useful for appropriately assessing an individual’s driving self-efficacy when providing driving support and for integrating this assessment into intervention planning.
Some limitations should be considered. First, the sample consisted of community-dwelling licensed drivers with a mean age of 46.8 years and was recruited through convenience sampling from the authors’ professional networks. Therefore, generalizability to older adults, clinical populations, and broader driver populations remains to be established, and selection bias cannot be ruled out. In addition, because previous ADSES validation studies were conducted in different populations and cultural contexts, direct comparison across language versions should be interpreted with caution. Second, although EFA supported a unidimensional structure, confirmatory factor analysis in larger and more diverse samples would further strengthen the evidence for structural validity. Third, test–retest reliability was examined in a relatively small subsample (n = 20). Although the ICC indicated excellent stability, the MDC95 should be interpreted with caution because of the limited retest sample size. Finally, the cross-sectional design precluded evaluation of predictive validity, including associations with future driving cessation or objective driving performance.
Conclusion
ADSES-J was shown to be a reliable and valid measure of driving self-efficacy in Japan and may be useful for assessing driving-related self-efficacy among community-dwelling drivers. Future longitudinal studies are needed to establish its predictive validity and clarify its potential clinical utility in supporting decisions regarding driving continuation, cessation, and alternative mobility.
Footnotes
Acknowledgements
The author would like to express sincere gratitude to Ms. Mizuho Kuki, occupational therapist at Kotonoura Rehabilitation Center, for her dedicated assistance in data collection and data entry. The author also extends heartfelt thanks to all occupational therapists and staff members who contributed to this study through their cooperation and support. Their valuable efforts made this research possible.
Ethical Considerations
Participants received written and verbal explanations and provided written informed consent. The study was approved by the Ethics Review Committee of Morinomiya University of Medical Sciences (Approval No. 2023-066) and conducted in accordance with the Principles of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all individual participants included in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (Grant Number 25K13427; Principal Investigator: Shohei Kagino).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Use of Artificial Intelligence Statement
Artificial intelligence (AI) tools were used only to assist with language editing and revision of the manuscript. No scientific data, analyses, results, or interpretations were generated or modified using AI. The authors take full responsibility for the accuracy, originality, and integrity of the manuscript.