
Abstract
Keywords
Introduction
According to 2018 Kids Count Data, Latinx children are the largest ethnic minority in the United States (US) with over 18.5 million children or 25% of the ethnic minority population. This makes Latinx populations the largest ethnic minority in the US overall (US Census, 2019). From 2000 to 2010, South Carolina had the fastest-growing Latinx population in the country, with an increase of 148% (US Census, 2012). Latin American countries continue to make up the largest percentages of countries of origin for immigrants in the state with 24% of the immigrant population being of Mexican origin. Immigrants in South Carolina are more likely than their native-born counterparts to have less than a high school education (22% of immigrants in the state vs. 11% of native-born citizens; Annie E. Casey Foundation, 2018). Furthermore, South Carolina immigration trends point to 4% of children born in the US living with at least one undocumented family member (American Immigration Council, 2016). By comparison to larger states with more established immigrant communities, South Carolina has a small but growing immigrant population (American Immigration Council, 2016). As such the immigrant population within the state is a newer Latinx settlement and has different needs than more established and larger immigrant populations.
One of the unique needs of growing Latinx settlement areas includes educating families and increasing awareness of the American education system and expectations for school readiness. According to the American Academy of Pediatrics (AAP), school readiness includes early academic skills, physical health, language skills, social and emotional development, motivation to learn, creativity, and general knowledge (AAP, 2016). It is widely known that communities and families play critical roles in all areas of school preparedness in children. Furthermore, the AAP supports funding research agendas that examine the ways in which school preparedness can be most effectively achieved and disseminated to families, child care providers, and educators. Primary care pediatric offices are well positioned to be a hub for this critical period in children's and family's lives. In a tri-county area in coastal South Carolina, there have been increases of 163%, 207%, and 321% in the overall Latinx population, respectively, in the last 14 years (US Census, 2012). According to the Children’s Hospital University Pediatrics Clinics (CHUP), two community-based patient-centered pediatric medical homes (PCPMHs) in this tri-county area that are affiliated with the state’s only academic health sciences center, 46% (n = 1787) of publicly insured patients are identified as targeted care for the age ranges of 0–5 years old.
The purpose of this paper is to provide a programmatic evaluation of a culturally sensitive parenting and school preparedness program for first-generation Latinx children using a home visitation model with community health workers (CHWs). The program described in this paper, Connections for Child Development (CCD) is directly tied to two known and trusted PCPMH settings in the same community.
Background
The AAP clinical practice guidelines and Bright Futures health prevention guidelines highlight the need for promotion of healthy development as part of each well-child preventative care visit from birth through the school-age years (Hagan et al., 2018; Lipkin & Macias, 2019). The AAP recommends targeted developmental screenings at key ages throughout childhood as well as early literacy programs for all children (High & Klass, 2014; Lipkin & Macias, 2019). When developmental delays are recognized, early intervention is most successful when it is implemented between the ages of 0 and 5 years. Undiagnosed developmental delays or developmental delays without early intervention can impact learning and future academic success (Heckman & Masterov, 2007; Williams & Lerner, 2019).
Despite clear evidence supporting the importance of developmental screenings and early intervention, few culturally appropriate community resources exist for Latinx children to promote and foster routine developmental surveillance and school readiness. Justvig (2017) successfully used CHWs in a pediatric medical home with Latinx families receiving Medicaid coverage both in the newborn period and for children with chronic illness such as asthma or diabetes (Justvig, 2017). Positive results from the involvement with CHWs existed for participants that completed the program, including families that reported increased independence from CHWs over time. It is noteworthy that Latinx families completed the program more frequently than any other participants, suggesting that there are care gaps for limited English proficient patients and families that are known to be at greater risk for receiving poor care (Jacobs et al., 2006).
The literature supports that CHWs are an effective intervention in primary care pediatric practice for several patient outcomes, including decreasing missed appointments, assisting in management of chronic health care conditions, providing patient and parent education including newborn care and safety, reducing preventable emergency room visits for vulnerable youth, and increasing adherence to childhood immunization schedules (Anugu et al., 2017; Jacobs et al., 2006; Pati et al., 2015; Uchima et al., 2019). Despite these observed improvements in patient care of pediatric populations with chronic disease, utilization of CHWs remains scarce in pediatric practice when compared to adult practice with patient management of chronic disease.
Peacock et al. (2013) state that home visitation holds promise for socially at-risk children and their families particularly when initiated prenatally and at regular intervals. They also acknowledge that future studies are needed to determine the recommended frequency for positive effect and how to increase retention among participants (Peacock et al., 2013). Falbe et al. (2017) describe that CHW experiences may help increase self-efficacy to implement healthful changes in participant homes and be better prepared for health care visits. While many programs are developed as a response to immigrant children entering elementary school, gaps in the literature are seen in proactive initiatives to better prepare children for school within this critical time window, with only limited programs aimed at or attended by preschool Latinx children and families. Hernandez-Mekonnen et al. (2016) and Crosnoe and Ansari (2016) found that Latinx children are less likely than other ethnic groups to enroll in formal preschool education at the age of 4 years. Examining the role of CHWs (linked to a PCPMH) in increasing developmental surveillance and school preparedness for limited English proficient Latinx children and families warrants further investigation to address this current gap in pediatric care and services.
Methods
Sample
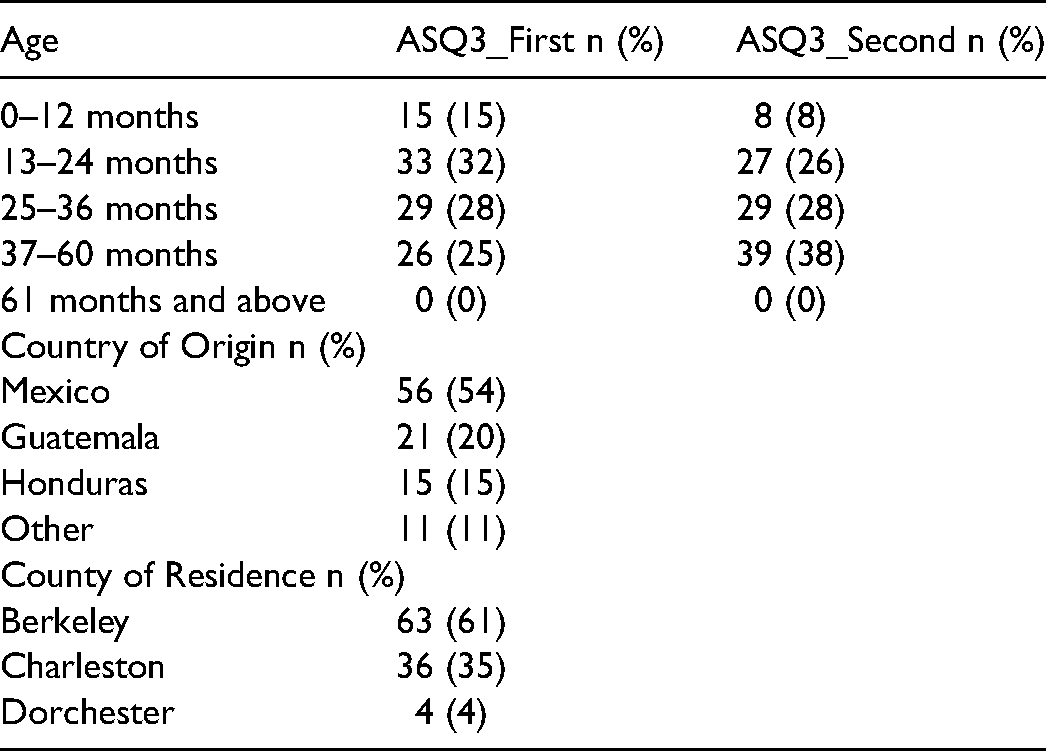
The current study sample included 103 families identified as immigrants, Spanish-speaking, and with at least one child in the age range of 0–5 years. Inclusion in the program included that the child lives in one of the three counties being served, is in the age range of 0–5 years at the time of the program, and has at least one Spanish-speaking, limited English-proficient parent or primary caregiver. Participation in the program is voluntary. The CHWs describe the program, including privacy protections for any patient-identifiable information given that all CHWs in the program are fully Health Insurance Portablity and Accountability Act (HIPPA) trained prior to employment and complete yearly mandatory training in HIPPA. Next, if the participants chose to enroll in the voluntary program, they are presented a university-approved, program-specific consent form ensuring that participation is completely voluntary; the document is signed by both the participant families and CHW when participants agreed to take part in the program. Descriptive characteristics of the sample are reported in Table 1, including age of child, country of origin, and county of residence. University Institutional Review Board (IRB) determined that this was a quality improvement study and not subject to IRB review or approval prior to initiating the program and then again, within a new Quality Improvement/Program Evaluation Self-Assessment tool that was completed in preparation for publication of this manuscript.
Population Demographics, n = 103.
Measures
The Ages & Stages Questionnaires®, Third Edition (ASQ®-3) was used to evaluate participant children. The ASQ®-3 tool thoroughly assesses development in the home environment and tailors parent/caregiver education based upon these results. The ASQ®-3 is used to pinpoint developmental progress in children of ages 1 month to 5 and a half years. It has been used for over 20 years and has six questions across the five major developmental domains: communication, gross motor, fine motor, problem–solving, and personal-social. There are 21 total questionnaires to be used, according to the child's age, across the first 5 and a half years of life. Prematurity is corrected for the first 2 years of life. It can be completed by the parent, caregiver, at a childcare center where the child receives care, in person at a medical appointment, over the phone, or in the home. The sensitivity of the ASQ®-3 ranges from 75% to 100% with 86% overall agreement. The specificity of the ASQ®-3 ranges from 70% to 100% with an 85% overall agreement. The ASQ®-3 is one of the developmental screening tools recommended by the AAP and as a reference, they consider high-quality developmental screenings to have specificities and sensitivities of 70%–80% (AAP, 2006).
Setting
For purposes of this program, an ASQ®-3 was administered at the first home visit with a CHW trained on the assessment measure. The ASQ®-3 was readministered at a second home visit if this follow-up visit was deemed necessary based upon results of the ASQ®-3, other social factors, or participant needs. Of the 103 participant children, 84 or ∼82% qualified for a second home visit solely on the basis of their initial ASQ®-3 scores. To ensure rigor, the CHW observed the child performing all tasks, as described on the corresponding ASQ®-3 questionnaire used at the home visit rather than completing the questionnaire based upon parental or caregiver report. To do this, the CHW brought a toolkit to each home visit that included all necessary objects to complete tasks on the ASQ®-3. Participants were referred by a medical provider from CHUP, self-referral by parents following community outreach events, or self-referral via word of mouth from the community.
Data Collection
In the first 3 years of this program, 103 children received both an initial and a follow-up ASQ®-3 tool; participants with only one ASQ®-3 score were not included in the statistical analysis as this evaluation was designed to compare results in ASQ®-3 screenings in children enrolled in the CHW program for continued surveillance (i.e., scoring in the monitoring and at-risk ranges). The data were then analyzed to look at each domain for each child screened and assess if they were: above the cut-off, close to the cut-off, or below the cut-off for each of the five developmental domains, based upon age. For purposes of this program, each of the five domain-specific results was classified as average, monitoring, and at-risk. If participant children scored average in each of the five categories, a second CHW-administered ASQ®-3 was offered to the family as an optional component of a second visit and then all ASQ®-3 results were communicated to the primary care provider. If participant children scored in the monitoring classification for two or more domains, a second home-based ASQ®-3 was recommended and scheduled; parents were given the option for a second screening if their child was in the monitoring classification for only one domain. If the participant child scored in the at-risk classification, education was provided, and the child was rescreened within three months. If the participant children were close to the cut-off or below the cut-off on one or more domains, the parents or caregivers received specific education on how to strengthen that domain through developmentally appropriate play and structured activity within the home setting. Enrollment in the program includes an age-appropriate toolkit that includes a toothbrush and children's toothpaste with fluoride (to promote dental health), a refrigerator magnet with the food guide pyramid (to promote healthy eating), an age-appropriate book (to infuse literacy into the program) and an age-appropriate toy that fosters typical development and reciprocal play at each visit. The CHWs spend time at each home visit role modeling and demonstrating the use of all of the items in the toolkit. In addition, these results were communicated back to the primary care medical provider. In the event that the child did not have a primary care medical provider, the CHW assisted the family in connecting them to one. It should be noted that this was often determined by the eligibility of insurance type and status.
Data Analysis
The ASQ®-3 results were analyzed pre-intervention and post-intervention to determine change over time. The results of the screening, education provided, and resource connection was entered into a secure nonprofit case management software, Apricot®. All members of the program team, including CHWs, are Health Insurance and Portability and Accountability Act (HIPAA) trained per the institutional recommendations.
Questionnaire data were aggregated with no identifying information. Data analyzed included responses from children that completed both the first and second ASQ®-3 questionnaire (n= 103). If participants did not have at least two ASQ®-3 results, they were not included in the statistical analysis. Descriptive statistics were used to analyze mean and standard deviation for the first and second ASQ®-3 scores, by five separate domains: communication, gross motor, personal-social, problem-solving, and fine motor. Percent change was calculated on mean scores from the first to second questionnaire and paired t-tests were utilized to test for statistical significance, with p < .05 considered significant. Descriptive statistics were also utilized to calculate counts and frequencies of children that earned scores to be classified in the categories of “at-risk, monitoring, and average” in the first and second ASQ®-3 questionnaires. Microsoft Excel and SAS 9.4 were utilized for the analysis.
Results
One hundred and three children completed the first and second ASQ®-3 questionnaire and all children included in the sample were younger than 61 months old. As noted in Table 1, over half of the parent participants reported Mexico as their country of origin with 11% reporting other (e.g., Venezuela, Bolivia, Peru, Columbia, Dominica, El Salvador, Nicaragua). The highest percentage of children lived in Berkeley County (61%), followed by Charleston County (35%) and Dorchester County (4%).
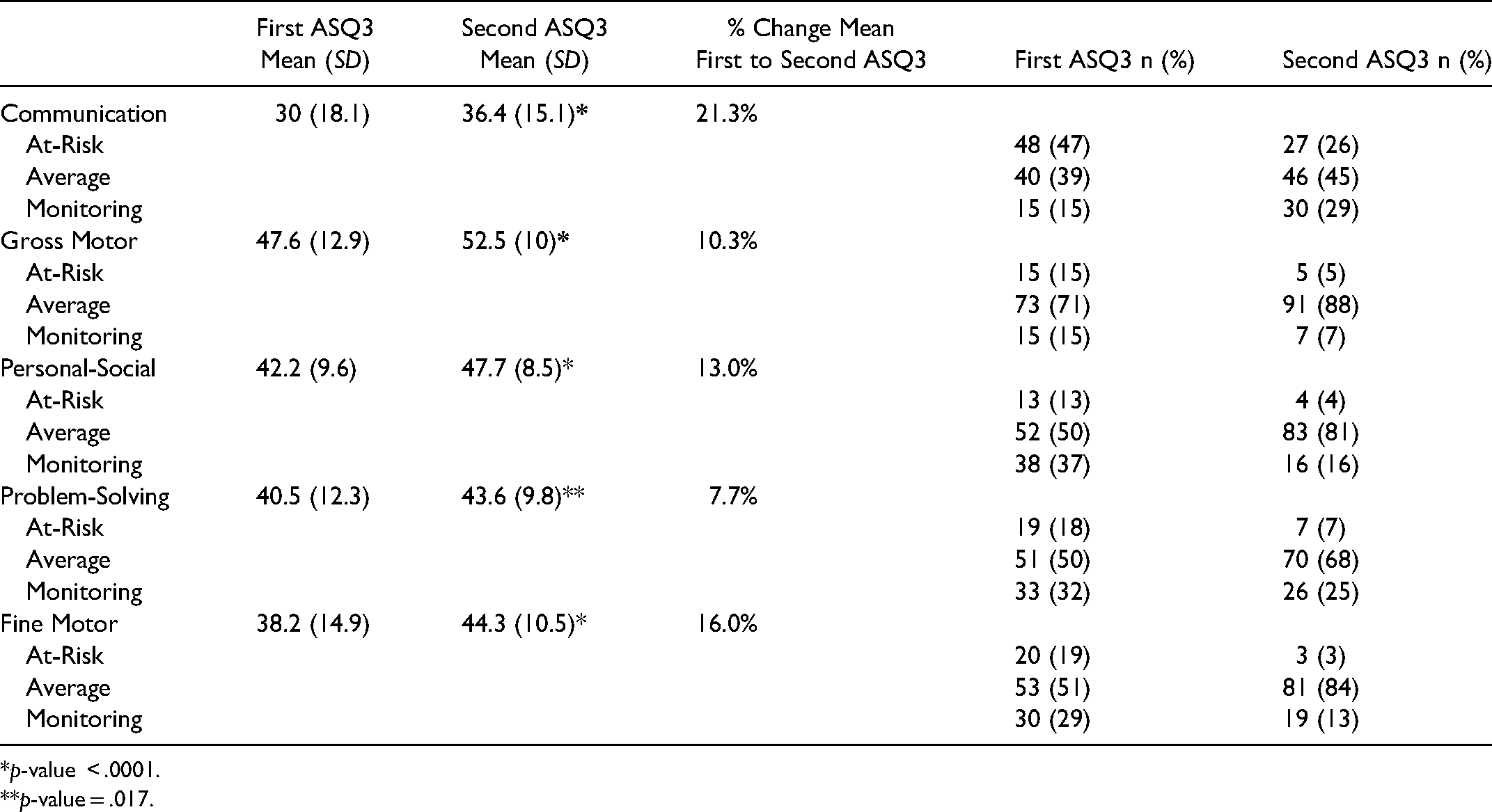
Results from the paired t-tests indicate statistically significant improvement in mean scores from the first to second ASQ®-3 in all five domains, as noted in Table 2.
First and Second Ages & Stages Questionnaires®, Third Edition (ASQ®-3) Rankings per Domain.
*p-value < .0001.
**p-value = .017.
The largest improvement was in the communication domain, with a mean increase of 6.4 points and percent increase of 21.3%. The second largest improvement was in the fine motor domain with a mean increase of 6.1 points and percent increase of 16.0%. All increases in mean questionnaire values were statistically significant with p-value of less than .05. In all five domains, the percentage of children scores from the first to second ASQ®-3 that ranked in the “at- risk” category decreased, with the largest decrease in the communication category (48 children to 27 children; 21% decrease in children “at-risk”). In addition, the percentage of children scores ranked in the “average”’ category increased in each domain with the largest increase in the fine motor domain (33% increase in children ranked as average) followed by personal-social with a 31% increase. Lastly, most domains had a decrease in children ranked as “monitoring” from their first to second ASQ®-3, with the exception of the communication domain which had an increase of 14% of children ranked in this domain, representing an additional improvement given that less children were in the at-risk category on their second ASQ®-3 overall when compared to the first.
Discussion
Given the disparities in skills related to school preparedness in children of Latinx immigrant families, this study examined a CHW program to help screen Latinx children for developmental delays in five early childhood development domains while supporting families with tools and resources to enhance school preparedness skills. Findings from this programmatic evaluation show that participation in this program showed improvement in all five domains of early childhood development in a statistically significant way.
The most dramatic gains were made in the communication domain, suggesting that intervention during this critical developmental period in childhood by culturally sensitive CHWs is beneficial for development. This is likely due in part to the infusion of literacy within the program with intentional choices in bilingual children's books as an activity at each home visit, emphasis on obtaining and utilizing the community library, role modeling of parroting language with children, and labeling things in the child's natural environment as these are all known to increase communication skills in early childhood (High & Klass, 2014). The second largest increase was in the fine motor skill domain. The program assisted family's learning of fine motor skill acquisition by role modeling crafting, cutting, drawing, writing, and self-feeding with utensils. The personal-social and problem-solving domains were improved by participation in the program. During home visitation, these supportive skills were facilitated by role modeling developmentally appropriate play techniques with dolls, stuffed animals, puzzles, and games and teaching children and families core components of these developmental domains through displays of affection, self-care techniques, and appropriate responses to problems. Within the gross motor domain, physical activity and physical play are major components of the program. Supportive skills of this domain encourage families of young children to seek outside play every day for 3 h per day that is light, moderate, or vigorous in intensity to encourage gross motor skills while concurrently combating lifestyles more likely to be associated with childhood obesity (Lobelo et al., 2020). Several of the program's developmentally appropriate toolkits include a ball large enough for catching, throwing, and kicking.
Key findings from the evaluation are consistent with the evidenced-based literature. This evaluation supports previous literature by Jacobs et al., and Uchima et al., regarding the need to better understand the ways in which language barriers affect health and that involvement of CHWs in the care team can improve health outcomes, respectively (Jacobs et al., 2006; Uchima et al., 2019). This evaluation did not specifically examine if there were increased up-to-date vaccination status of the participant children as a result of work with CHWs as Pati et al., did in their study (Pati et al., 2015). Additionally, the evaluation did not examine for interval pediatric emergency department use as Angu et al. did (Anugu et al., 2017). Given that the program is closely tied to two PCMH sites this could be accomplished in a follow-up study. Similar to the patient demographic variables in Anugu et al.’s (2017) study, this program demonstrated that provision of a home visitation program aimed at socially-at-risk immigrant children during the preschool years, even at this low frequency of two home visits with phone calls as needed prior to, in between and at follow-up proved to be beneficial across all five major developmental domains.
Use of CHWs is known to improve outcomes for individuals and communities and Latinx children are less likely to enroll in a structured preschool setting (Hernandez-Mekonnen et al., 2016). This was validated within this program, making home visitation programs like CCD appealing to families who have preschool-aged children that are not in a structured preschool setting. This home visitation program is a mechanism to further disseminate evidenced-based practice guidelines related to developmental surveillance in early childhood and to highlight the continued need for culture and linguistically appropriate services to better manage health disparities. In addition, it addresses the theme in the literature of Latinx children coming to kindergarten less prepared because they have not had an opportunity to receive programs aimed at children from birth to age of 5 years, prior to entering school.
Key Lessons Learned
Key lessons learned from this evaluation are that planning, implementing, and sustaining a program like this one requires large-scale buy-in from the broader community, partnering with advocacy organizations across the state, medical home provider buy-in, and finally participant buy-in. This program would not have been as successful without these components.
Facilitators of the program are that the CHWs are known and trusted community leaders that have pre-established trust in the larger community; thus assisted in participation in the program. Many of the CHWs have similar immigration stories and experiences raising children in the US as the participant parents which establishes a quick level of comfort between the CHW and parent. The CHWs have access to resources within the community that assists in managing the vulnerabilities that the participant families face. The program partners with and builds from the state's largest Latinx advocacy group. This partnership facilitates cultural competence, cultural humility, linguistically appropriate and strengths-based care within the program. Finally, the home visitation model is ideal for many of the participant mothers who do not drive or have regular access to transportation.
Barriers to this program existed for children that received a diagnosis of developmental delay as the CHWs are not equipped to manage this diagnosis but rather become a liaison between the participant family and access to statewide early intervention services. However, these CHWs contributed to facilitating an expedited referral to early intervention services because of this liaison role. Another challenge was participant follow-through with medical provider referrals. If participants did not respond to three phone calls from the CHW to set up an appointment, they stopped calling and notified the medical provider so this could be discussed at the next visit. This did not always result in participation and diagnoses of developmental delays could be prolonged without the information from the home visit with the CHW. Continued funding for the program is another area of challenge. Given the successes of the program in from this pilot work that was funded by the Duke Endowment, the state's early childhood network has now funded a total of five full-time CHW positions to carry out the program in four different counties with higher-than-average rates of Latinx immigrant children when compared to other counties in the state. Therefore, other states or regions will need to consider funding for the sustainability of such a program.
Future research and evaluation should include some of the following lessons learned. The length of time from identification of a developmental delay to referral to initial appointment needs to be looked at in subsequent programmatic evaluations to ensure early access to services. Aligning this program to participant children's statewide standardized Kindergarten Readiness Assessment (KRA) when they enter kindergarten should also be considered. The assessment's results can be compared between children that did not receive this program and those that did to see if there is any significant difference in scores between participant and nonparticipant children with similar demographic data.
To address other observations from this evaluation, additional programmatic evaluations must include a qualitative component to assess parental and caregiver willingness to participate in a program like this when provider concerns about their child's development arise but are not conclusive for a diagnosis. This may give increased insight into willingness to participate in the program. An additional qualitative evaluation must be conducted for satisfaction with the program from participant caregivers including how they think it has benefited the child and
Strengths and Limitations
CCD provides best practices for school preparedness by employing AAP recommendations for developmental screening, connection to community resources, provision of care, and teachings to parents to foster healthy development in their children. The purpose of this paper was fulfilled when programmatic data were analyzed for statistical significance, giving way to a programmatic evaluation that showed increases in all five major developmental domains for participant children. By fulfilling this purpose, it seems evident that in response to the gaps in the literature surrounding the frequency of home visits to have an effect on development in early childhood; even those with only two home visits in early childhood have the capability to improve overall development during this critical timeframe. Additional evaluations will need to be completed to assess if this increase is sustained over time or diminishes at completion of the program and to assess parental hesitancy and satisfaction with the program. Bias exists for children that did not receive a second ASQ®-3 when they scored in the monitoring category on their first evaluation given that some of their peers did receive a second ASQ®-3 and are included in this sample. Sample size was solely determined by participant children that received two ASQ®-3 screenings; they are the only participants reflected in this evaluation.
Conclusion
Patient-centered medical homes are ideal settings to initiate these types of programs as many parents cite that this is the setting where they have high levels of trust in regard to receiving information about their child's health, development, and behavior. The program filled the purpose of providing a culturally sensitive parenting program to a growing first-generation Latin American population of children that lack community resources necessary for school preparedness. This programmatic evaluation could be helpful to others to initiate this same program in conjunction with a PCPMH. Having buy-in at the state and/or local levels is essential to fully explore funding sustainability as it relates to early childhood funding in the state, state Medicaid programs, and local school districts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Duke Endowment (grant number 6593-SP).