
Abstract
Keywords
Introduction
Latinx 1 individuals comprise of 18% of the United States (U.S.) population (Noe-Bustamante, Lopez, & Krogstad, 2020), but only represent 9.3% of participants enrolled in National Institute of Health (NIH)-funded research (Office of Research on Women Health, 2019). A myriad of factors that further marginalize Latinx immigrants may contribute to their underrepresentation in research and health care compared to U.S.-born Latinx individuals. Underrepresentation of Latinx individuals in research poses challenges to advance public health, namely to adequately understand disease prevalence and symptom expression of illnesses affecting the Latinx population, and limits knowledge of culturally relevant strategies that can reduce existing health disparities and promote health equity (George, Duran, & Norris, 2014; Moreno-John et al., 2004; Salman, Nguyen, Lee, & Cooksey-James, 2016; Whitfield, 2005). Adequate representation of Latinx individuals in research holds promise of increasing generalizability of research findings, culturally tailoring evidence-based practices, and improving population health of Latinx individuals (Salman et al., 2016). Factors contributing to the underrepresentation of Latinx participants in research, however, are multifaceted and complex and attributed to historical and contemporary influences.
Historical Harms Against Underrepresented Groups in Research
The relationship among researchers, research institutions, and racial/ethnic minoritized communities is punctuated by historical mistreatment and unethical research practices globally. In the name of science, researchers and health care professionals conducted experiments to understand untreated disease progression (e.g., Tuskegee syphilis experiment [Cobb, 1973]), to cultivate and proliferate cells used in biomedical research (e.g., “HeLa cells” from the late Henrietta Lacks; [Khan, 2011]), and to understand the effects of ionizing radiation and radioactive contamination on the human body (Washington, 2006), among others. Specific historical harms in research against the Latinx community occurred both in the United States, (e.g., the experimentation of contraceptives in Latinx women in San Antonio [Kim, 2012] and Puerto Rico [Blakemore, 2019]) and in immigrant’s home countries, such as the Guatemala syphilis experiment (Reverby, 2012) and Cariporide trial in Argentina (De Young & Nelson, 2000). A long legacy of historical harms to racial/ethnic minoritized groups by researchers and health care systems contribute to their underrepresentation in research (Moreno-John et al., 2004; Salman et al., 2016; Shahabi et al., 2011). A hallmark of these abuses is illegal human experimentation without proper consent and fair treatment (De Young & Nelson, 2000; Kim, 2012; Reverby, 2012). The downstream effect of these abuses has created a culture of mistrust and fear of research among racial/ethnic minoritized groups, thereby creating barriers to research participation (Clark et al., 2019; Luebbert & Perez, 2016; Scharff et al., 2010; Smirnoff et al., 2018).
Recognition of these events as human rights abuses led to notable efforts to prevent unethical research practices. Institutional Review Boards (IRB)—the oversight committees over research at U.S. institutions—require training on the rights and welfare of human subjects in research (Steneck, 2007). Additionally, the NIH developed guidelines to promote the inclusion of underrepresented groups in NIH-funded clinical research (National Institutes of Health (NIH), 2017). There were also attempts to provide reparations for these abuses, such as financial compensation to the family of Henrietta Lacks (Witze, 2020).
Prejudice, Discrimination, and Racism in Health Care and Research
Minoritized groups experience significant discrimination and racism in everyday life (Pew Research Center, 2017; Robert Wood Johnson Foundation, 2017) and in health care systems (Benjamins & Middleton, 2019; Institute of Medicine, 2003), further increasing their mistrust in research and clinical care (Brandon, Isaac & LaVeist, 2005; García, Zuñiga, & Lagon, 2017; Moreno-John et al., 2004). The implications of unequal treatment for minoritized groups are lower health care utilization, poorer patient-provider relationships, and poorer health outcomes (Lee, Ayers, & Kronenfeld, 2009; Quach et al., 2012; Rivenbark & Ichou, 2020). Latinx individuals face additional challenges in research and health care settings including fear of deportation for disclosing an undocumented immigration status, lack of linguistically appropriate materials, and interpretation during clinical encounters (López-Cevallos & Harvey, 2016; Steinberg, Valenzuela-Araujo, Zickafoose, Kieffer, & DeCamp, 2016). Cultural differences in health beliefs and attitudes among researchers and Latinx participants and language/literacy barriers may influence their willingness to participate in research (Huang, Ezenwa, Wilkie, & Judge, 2013; Salman, Nguyen, Lee, & Cooksey-James, 2016). A lack of understanding of cultural factors among providers and researchers could further contribute to negative experiences within the health care system and for engaging and recruiting Latinx individuals in research.
Lack of Diverse Research Workforce and Infrastructure to Engage Underrepresented Groups
The lack of representation of doctorally prepared researchers from racial/ethnic minoritized groups in academic positions further contributes to the challenges in engaging underrepresented groups in research. Approximately 1.6% of U.S. adults hold a doctorate degree 2 , but of those with a doctorate degree, a mere 5.7% are Latinx (U.S. Census Bureau, 2017). Historically, research studies were conducted by White researchers where White participants largely comprise study samples (George et al., 2014). Individuals from underrepresented groups are more likely to participate in research when the research staff demonstrates cultural congruence, understands cultural nuances and linguistics, and relates to their lived experiences (Doran, Castelblanco, & Mijanovich, 2018; García et al., 2017; George et al., 2014). A lack of access to bilingual and bicultural researchers creates additional challenges to develop cultural- and linguistically appropriate recruitment strategies to engage Latinx individuals in research (García et al., 2017).
An infrastructure that optimally facilitates research participation by Latinx individuals is also lacking. Research studies are often introduced to participants through their health care providers, creating missed opportunities to engage underrepresented groups in research for individuals without a source of care (Caraballo et al., 2020). Individuals from underrepresented groups also encounter limited access to health care due to availability of resources, lack of insurance, and face employment constraints from working multiple jobs (García et al., 2017; Luebbert & Perez, 2016; Moreno-John et al., 2004; Salman et al., 2016). The Latinx community also has higher uninsured rates than Black, White, and Asian individuals in the United States (19.0%, 11.5%, 7.5%, 6.8%, respectively; Artica, Orgera and Damico, 2020).
Sociopolitical Climate
The sociopolitical climate has become increasingly hostile for immigrants. Federal immigration policies enforced increased patrol at the U.S.–Mexico border, detained immigrants, forbade sanctuary cities from receiving federal assistance, and increased use of Immigration and Customs Enforcement (ICE) agents (Ink, 2020). Such immigration policies and enforcement practices have created a restrictive immigration climate in the U.S. Additionally, policies enacted to reduce the spread of communicable diseases to allow for immigration into the U.S. (DeSisto et al., 2015) may further contribute to these negative experiences. As a result, undocumented, Latinx immigrants may feel reluctant to participate in research because of instilled fears of deportation (Doran et al., 2018; García et al., 2017) and face additional barriers to research participation such as lacking a driver's license or social security number (Salman et al., 2016) to receive study compensation.
Several states, however, refused to enforce immigration laws to protect immigrant communities (Ink, 2020) and have become sanctuary jurisdictions. Many U.S. cities implemented measures to provide immigrants access to health care, legal counsel, and municipal identification, regardless of their immigration status (Ink, 2020; National Immigration Law Center, 2015). Sanctuary policies, however, vary by state with some states supporting the restrictive immigration policies, and others prohibiting them (National Conference of State Legislatures, 2019). Restrictive immigration laws may create a harsh environment for Latinx immigrants and further exacerbate their experiences with discrimination (López-Cevallos, & Harvey, 2016) which has contributed to mistrust in research.
Strategies to Mitigate Barriers for Recruitment of Latinx Participants
Several recruitment and engagement strategies are used to mitigate research participation barriers among Latinx participants and hold promise for effective recruitment in research (García et al., 2017). Community-engaged strategies, snowballing sampling methods, direct contact with participants, and using bilingual and bicultural research staff fostered trust and increased engagement in research of Latinx participants (Mier et al., 2006; Nápoles-Springer et al., 2000; García et al., 2017). These strategies, however, have generally been implemented in behavioral studies and have not been well explored in biobehavioral research where anthropometric measurements and biospecimens are collected. Gathering biospecimens from Latinx participants may create additional challenges for engagement and recruitment for biobehavioral research. To date, there is limited knowledge on recruitment and engagement of Latinx, young adult immigrants in biobehavioral research. To address this gap, we sought to examine the effect of targeted strategies for recruitment of young adult, Latinx immigrants into a biobehavioral research study.
Methods
Study Design
The Salud (Health), Estrés (Stress), y Resiliencia (Resiliency) (SER) Hispano Study is an ongoing longitudinal, observational, community-engaged research (CEnR) study that follows a cohort of young adult, Latinx immigrants in the U.S. Southeast across 2 years (N = 391). The overarching aim of the study is to determine the cumulative impact of acculturation stress and resilience on health outcomes among Latinx immigrants over time, in an emerging Latinx immigrant community. This study utilized CEnR approaches for recruitment, engagement, and retention by partnering with the chief executive officer (CEO) of a community organization and recruitment coordinators who reside in the community where recruitment occurred. All procedures occurred outside the health care system. A combination of self-reported measures (e.g., standardized surveys), anthropometric measurements (e.g., height, weight, and blood pressure), and biospecimens (e.g., blood and urine) were collected in participants’ homes or in the partnering community organization's office.
Community Partners
The research team partnered with a local, trusted community-based organization (CBO) that provides programs in education, economic development, health and wellness, and community advocacy for Latinx communities. The CBO serves over 11,000 immigrants annually and has a long-established relationship with the academic institution. The CBO's CEO served as a study co-investigator. A bilingual, bicultural community specialist was hired to foster trust with the Latinx community, coordinated outreach programs and events for engagement and recruitment, and developed strategies for study promotion in the Latinx community. The CBO and research team worked together through an iterative process to provide feedback to the study design, selection of key measures, and engagement and recruitment efforts.
Sample and Population
Recruitment occurred across three local counties in the U.S. Southeast, within an hour radius of the academic institution. We selected this radius to reduce the time between biospecimen collection and laboratory processing. The Latinx community represented 8.6%, 10.4%, and 13.7% of the counties’ population, respectively (U.S. Census Bureau, 2019). Eligible participants included young adults who: (a) self-identified as Latinx, (b) immigrated from a Spanish-speaking country (e.g., Latin America or Caribbean) within the past year, and (c) were between ages 18 and 44 years, (ages when immigrants are most likely to arrive in the U.S. [U.S. Department of Homeland Security, 2016] and when risk behaviors and mental health conditions peak [Mulye et al., 2009]). Exclusion criteria included individuals who planned to move from the region within 2 years because the study was limited to the three selected counties. This study received IRB approval from Duke University Health System.
Recruitment Strategies and Procedures
Using CEnR approaches, we developed a comprehensive, strategic recruitment plan that included: (a) developing a recruitment team, (b) identifying recruitment efforts within the CBO and events where Latinx individuals frequented, (c) gathering information of existing partnerships, and, (d) developing cultural- and linguistic-appropriate recruitment materials. Recruitment sites were selected using existing partnerships with the study team members and the CBO, who established rapport with the Latinx community and other local community organizations.
We selected recruitment strategies addressing common barriers to research participation among Latinx immigrants (Table 1). Barriers were identified through a literature review, experiences from the research team on previous studies, and conversations with CBO staff. The research team and CBO brainstormed innovative solutions that capitalized on the CBO's trust and reputation in the community and selected recruitment locations that were not local to the academic institution. The CBO coordinated community events for engagement and recruitment so that participants associated the study with an academic researcher staff and trusted community staff, most of who were bilingual and bicultural. Weekly meetings were held to reevaluate and revise recruitment strategies. Revisions were made through an iterative process based on data gathered from recruited and enrolled participants.
Targeted Recruitment Efforts to Address Barriers to Research Participation Among Latinx Participants.
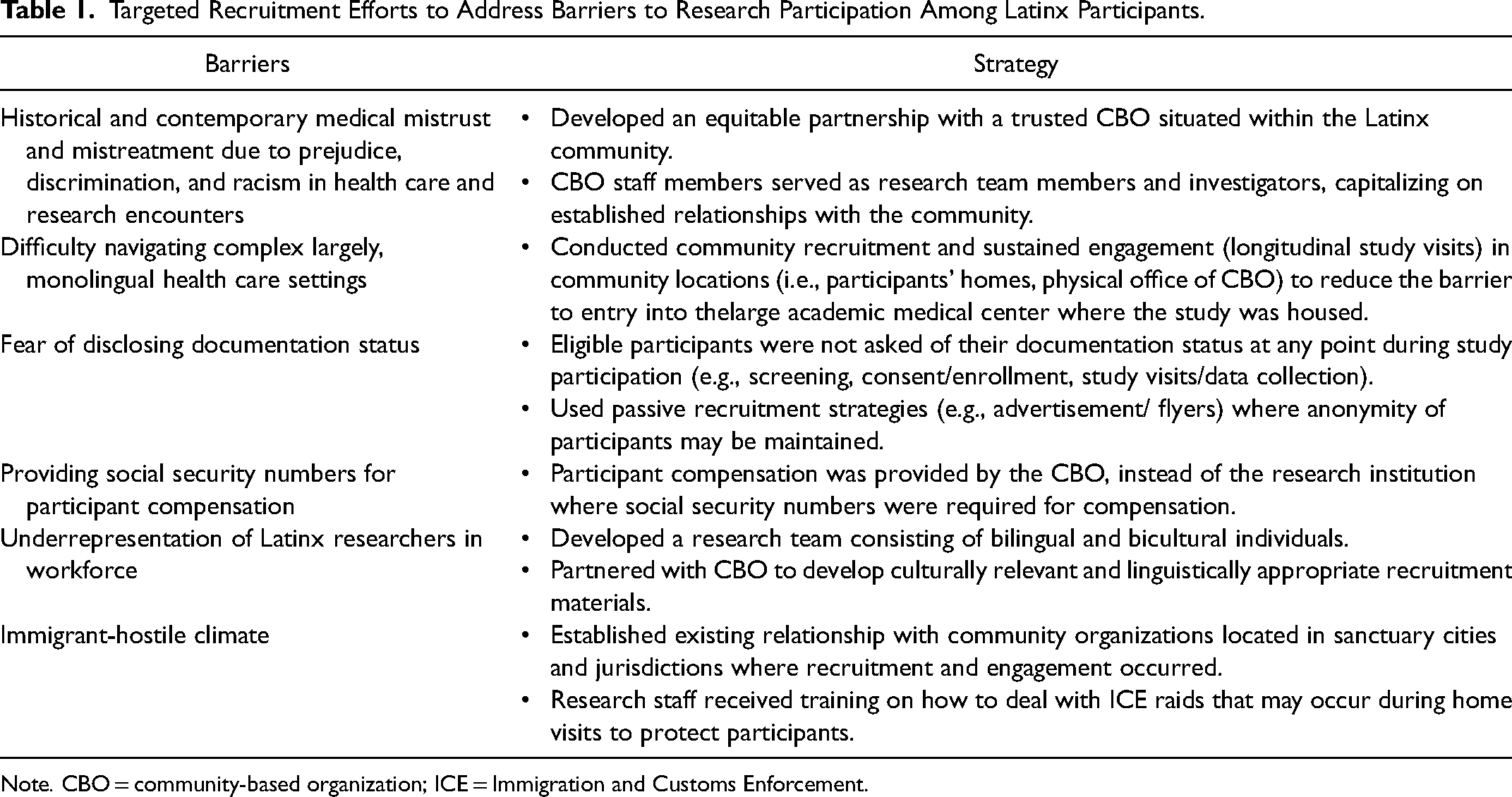
Note. CBO = community-based organization; ICE = Immigration and Customs Enforcement.
We retrospectively reviewed data gathered by the study team from participants recruited in 2018 and 2019. Data included participants’ contact and demographic information, recruitment location, and method of recruitment (e.g., community outreach, advertisement, social media, email listservs, and word-of-mouth). We assessed the method of recruitment used to recruit and enroll participants and grouped strategies into two types of recruitment: active recruitment and passive recruitment (Estabrooks et al., 2017), informed by effective recruitment methods salient to the Latinx community (García et al., 2017).
Recruitment and engagement procedures
After establishing initial contact, participants were screened for eligibility. A three-call threshold was placed to reach participants. The screening call consisted of explaining the study's purpose, participant expectations, and assessing for eligibility. Participant expectations included completing five visits throughout a 2-year period, and willingness to have their body measurements and biospecimens obtained. Baseline visits were scheduled at participants’ homes or at the CBO to alleviate transportation barriers, promote privacy, and accommodate work schedules. Survey items and informed consents were offered in Spanish or English language by a bilingual, bicultural research team member. Written consent was obtained at the initial visit where participants were enrolled in the study.
We implemented several strategies to engage and retain participants, such as sending welcome emails, reminders about study visits and events, quarterly updates of study findings, and invitations to attend an annual symposium to learn about preliminary study findings and local community resources. Messages and postcards were sent to participants to celebrate life events (e.g., new births and birthdays). During the COVID-19 pandemic, participants were also sent information regarding COVID-19 testing and vaccination sites and available resources to address their social and health needs.
Statistical Analysis
Descriptive statistics were analyzed to describe the characteristics of recruited participants and type of recruitment strategies. Nondirectional statistical tests were conducted with a significance set at 0.05 for all tests and were analyzed using SPSS, version 27 (IBM Corp, 2020). Chi-square tests were conducted to test the association between type of recruitment strategy and participant enrollment. Logistic regression analysis was conducted to examine which recruitment strategy best predicted participant enrollment. The multivariate logistic model included the four recruitment strategies and the primary outcome, participant enrollment. Adjusted odds ratios (AOR) and their 95% CIs were reported to address clinical relevance and effect size.
Results
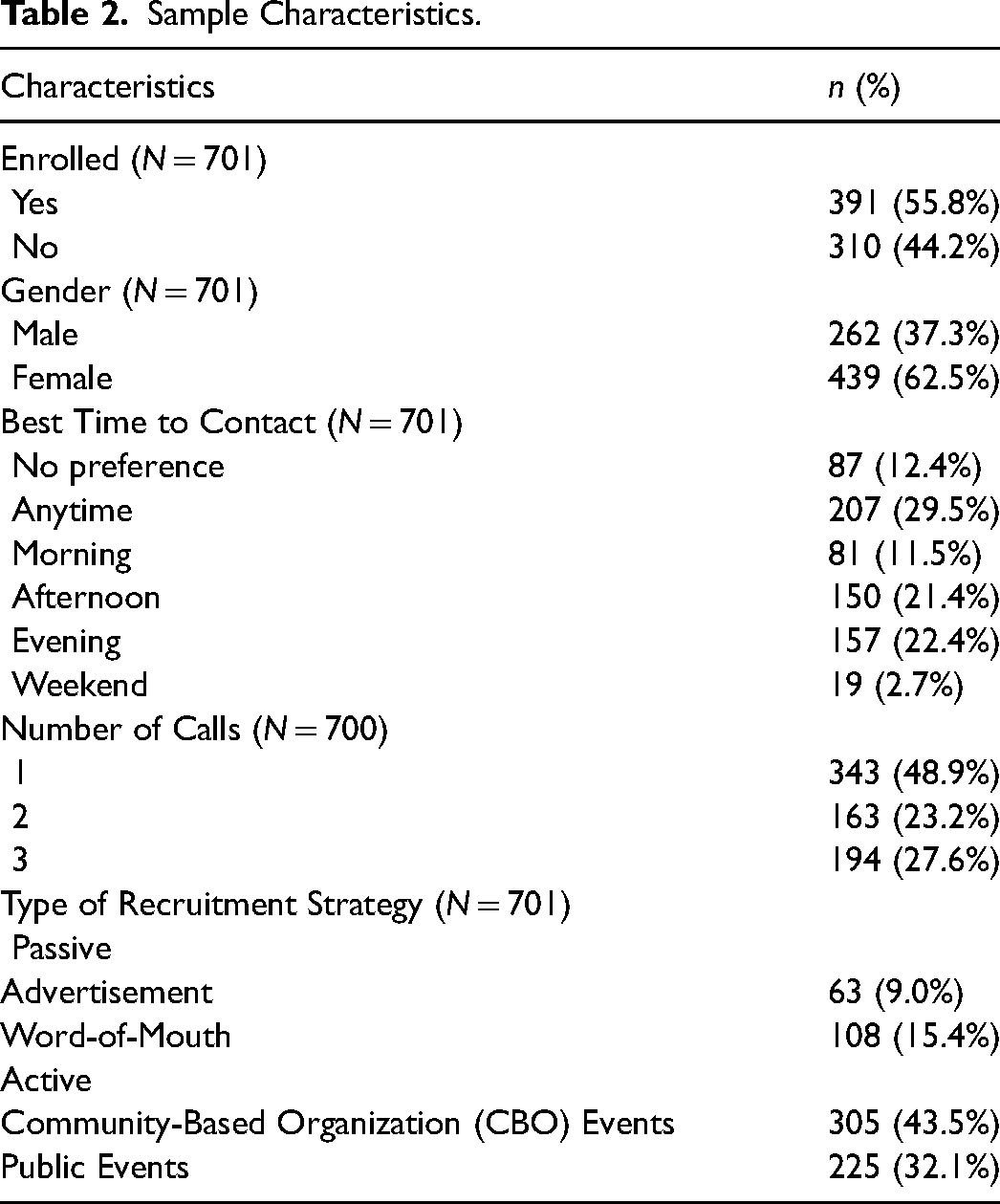
Figure 1 shows the flow diagram of participant enrollment. Table 2 presents the sample characteristics of recruitment strategies and participants enrolled in the study. Among 701 participants approached for recruitment, 391 participants enrolled (55.8%). Most enrolled participants were women (63%) and nearly half (48.9%) were reached within one phone call. Most participants were approached using active strategies, with 43.5% of participants approached through CBO events, followed by public events (32.1%). Among passive recruitment strategies, more participants were approached through word-of-mouth (15.4%) compared with radio and flyer advertisements (9.0%).
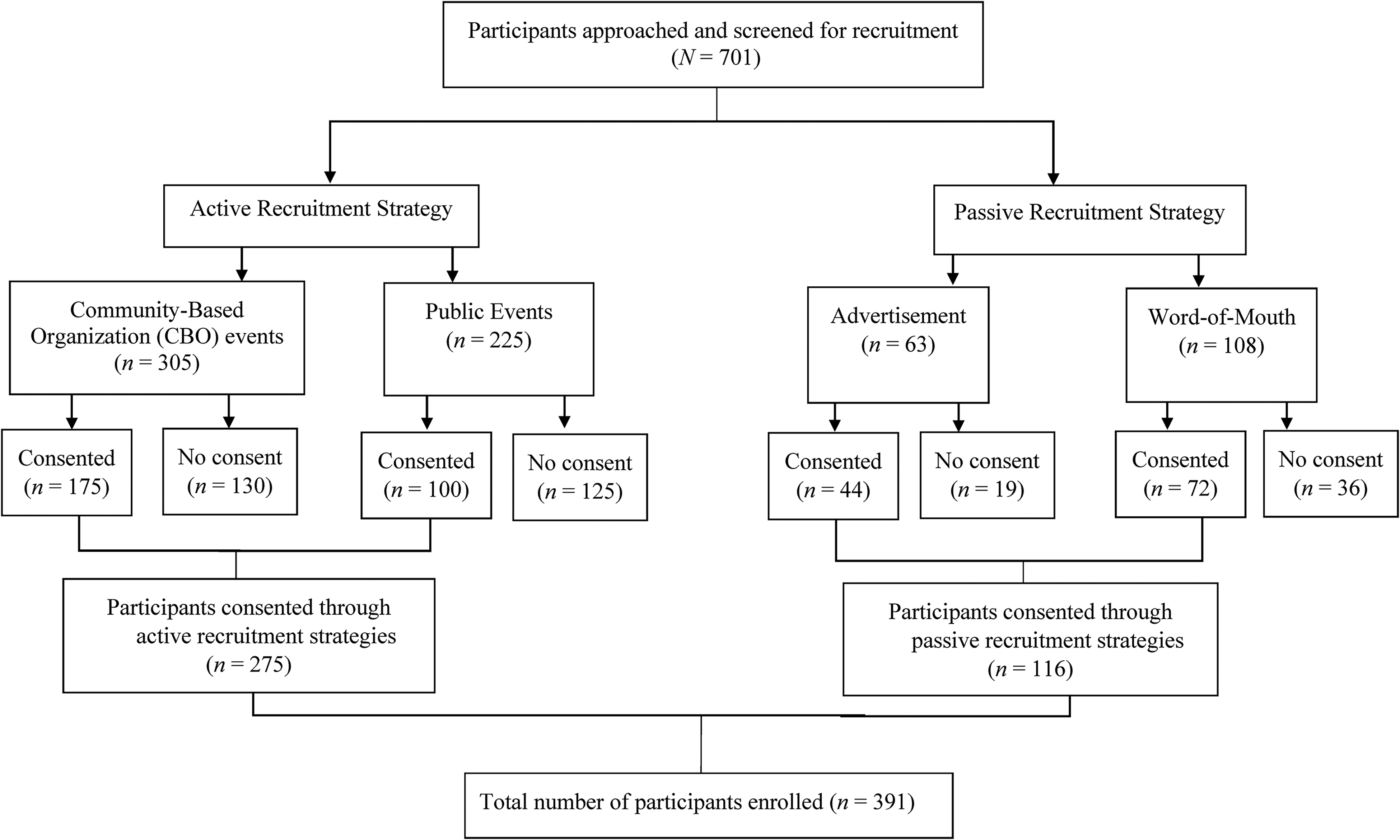
CONSORT diagram of participant enrollment.
Sample Characteristics.
Type of recruitment strategy was significantly associated with participant enrollment (χ2 = 13.33, df = 1, p < .001) (Table 3). Among participants recruited through active recruitment strategies, roughly 52% enrolled in the study and nearly 48% did not enroll. Among participants enrolled using passive recruitment strategies, roughly 68% enrolled in the study and 32% did not enroll.
Chi-Square Analysis of Recruitment Strategies and Participant Enrollment, N = 701.
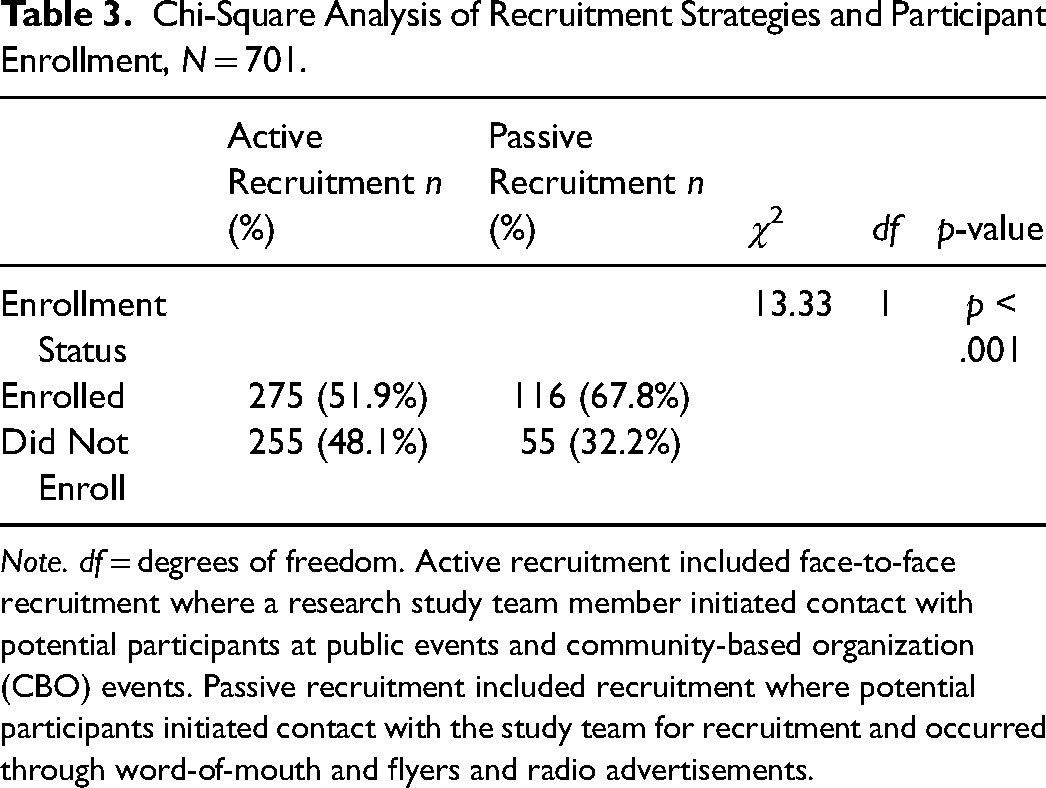
Note. df = degrees of freedom. Active recruitment included face-to-face recruitment where a research study team member initiated contact with potential participants at public events and community-based organization (CBO) events. Passive recruitment included recruitment where potential participants initiated contact with the study team for recruitment and occurred through word-of-mouth and flyers and radio advertisements.
The odds of enrollment were 2.9 times greater when participants were recruited through radio and flyer advertisements compared with participants recruited through public events (AOR = 2.90, 95% CI [1.59, 5.27], p = .001) (Table 4). The odds of enrollment were 2.5 times greater and nearly 1.7 times greater when participants were recruited through word-of-mouth (AOR = 2.50, 95% CI [1.55, 4.03], p < .000) and CBO events (AOR = 1.68, 95% CI [1.19, 2.38], p = .003), respectively, compared with recruitment through public events.
Logistic Regression Analysis of Type of Recruitment Strategy and Participant Enrollment.
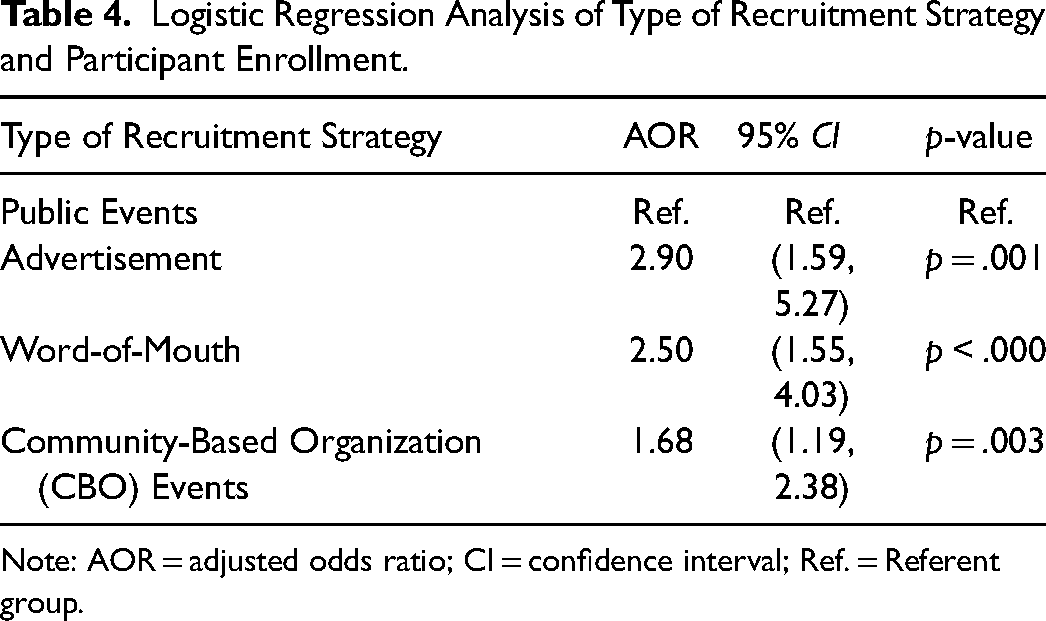
Note: AOR = adjusted odds ratio; CI = confidence interval; Ref. = Referent group.
Discussion
This study identified active and passive recruitment strategies to enroll young adult, Latinx immigrants into a longitudinal, biobehavioral study. Undocumented immigration status, language barriers, and cultural health beliefs and attitudes are noted barriers to recruiting Latinx immigrants in research (López-Cevallos & Harvey, 2016; Salman et al., 2016; Steinberg et al., 2016). We sought to mitigate these barriers by not requiring participants to disclose their immigration status or provide social security numbers for study compensation and used bicultural and bilingual research staff to develop and implement recruitment strategies. Overall, participants exposed to radio and flyer advertisements had greater odds of enrollment into our biobehavioral study. This study identified useful strategies targeting barriers specific to Latinx immigrants that may improve their representation in future research.
Although most participants were recruited using active recruitment strategies, these strategies generated less enrollment than passive strategies. This finding differs from other studies that found face-to-face recruitment through CBOs highly effective in recruiting participants from vulnerable populations (Estabrooks et al., 2017; Greiner et al., 2014; Reidy, Orpinas, & Davis, 2012; Wieland, Doubeni, & Sia, 2020). Difference in findings may be explained by strategies used for active recruitment in other studies, such as telephone outreach, or promotional activities in community settings (Estabrooks et al., 2017; Sha, McAvinchey, Quiroz, & Moncada, 2017). Due to the IRB restrictions at our institution, we were unable to employ these recruitment strategies further highlighting the barriers that institutional research infrastructures can create for recruitment. Further, although the partnering CBO—who established trust in the Latinx community—facilitated study promotion at community events, there may have been an initial skepticism to engage in the study until individuals established their own trust with the research study team.
Differences in findings may also be explained by the smaller sample sizes in the passive recruitment strategies. Passive recruitment strategies were disseminated through email listservs, social media, and flyers posted and left at CBOs and other community establishments. Therefore, we were unable to document the number of individuals exposed to radio and flyer advertisements to estimate the yield in the total population. Future research should consider using population-based approaches to examine the most effective recruitment strategies to recruit Latinx participants. Future research studies should also consider using random sampling designs to identify which recruitment strategies are effective in the engagement and retention of Latinx participants.
To our surprise, passive recruitment strategies using radio and flyer advertisements and word-of-mouth generated more enrollment of Latinx, young adult immigrants. Younger individuals may appeal to electronic formats for recruitment (e.g., flyers sent via social media or email listservs) compared to older individuals. Future research should consider exploring effective recruitment strategies for Latinx immigrants across age groups. A major strength of passive strategies is that interested participants can engage in recruitment without revealing their identity, which may be beneficial to undocumented individuals who fear disclosing their immigration status. Word-of-mouth may also facilitate participant enrollment. The Latinx culture places strong beliefs in familism, which places high values on family life (Landale, Oropesa, & Bradatan, 2006). A strength to using word-of-mouth is the ability for participants to receive a referral for study participation from a trusted person. Radio and flyer advertisements from trusted sources and from individuals who participants could relate to (e.g., ethnic and language concordance), may have played a role and is described as important strategies in the literature (Avery, Hernandez, Hebl, 2004; Kayrouz, Dear, Karin, & Titov, 2016). Passive strategies, when leveraged with trusted sources, may be a promising approach to overcoming mistrust in research and health care experienced in Latinx communities.
This finding also sheds light on the characteristics of individuals enrolled through passive recruitment strategies. Participants self-selected and contacted the study team. Therefore, these individuals may be more engaged and willing for study participation than individuals approached through active recruitment strategies. Recruitment efforts should consider targeting popular social group settings and social media platforms among the Latinx community to increase recruitment into future research. Use of social media platforms may also assist with tracking the number of people viewing advertisements for recruitment in research studies to accurately assess participant engagement with these recruitment strategies.
Limitations
This study has several limitations. The sample size for the passive recruitment strategies was small which may have potentially overinflated the strength of association between recruitment strategies used and participant enrollment. This study was limited in the ability to track the number of people who were exposed to advertisements. Thus, there may have been more participants who expressed study interest that could not be accounted. This study focused on one segment of the Latinx population. Thus, the generalizability of the study findings are not applicable to children, older adults, gender identities, and individuals living in other Latinx countries. Lastly, the study design was limited in the ability to examine the cost-effectiveness of multiple recruitment strategies compared to “head to head.” Therefore, cause and effect relationships between the type of recruitment strategy and participant enrollment cannot be ascertained.
Conclusion
The Latinx population experiences significant health disparities yet are underrepresented in research aiming to improve health outcomes. This study provides a guide of culturally relevant recruitment strategies that can increase Latinx representation in future research. Study findings can inform future recruitment efforts for Latinx immigrants that consider the resource investment for various active and passive recruitment strategies. These strategies can also be considered for health care and community-based interventions targeting the Latinx population. More research is needed, however, to examine the cost-effectiveness of different strategies to recruit and engage Latinx immigrants in research.
Footnotes
Acknowledgments
Research reported in this publication was supported by the National Institute on Minority Health and Health Disparities of the National Institute of Health under Award Number R01MD012249. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Minority Health and Health Disparities (grant number R01MD012249).