
Abstract
Given the longer lives of individuals with disabilities and the increasing likelihood of siblings fulfilling family caregiving roles, it is critical to identify correlates of sibling caregiving. Yet, little research has examined the relation between the severity of the disability and sibling caregiving. The purpose of this study was to understand the relation between the severity of the disability (defined as functional ability and maladaptive behaviors) and sibling caregiving, including advocacy and future planning. Adult siblings of older individuals with disabilities (N = 141) completed a national survey. Results indicated that individuals with less functional ability were significantly more likely to receive greater sibling caregiving, advocacy, and future planning. There was a nonlinear relation with respect to sibling caregiving and functional ability with individuals with severe disabilities requiring disproportionately greater sibling caregiving. Furthermore, there was a nonlinear relation between maladaptive behaviors and caregiving demands such that siblings of individuals with the greatest asocial behaviors reported significantly greater caregiving demands.
Increasingly, individuals with disabilities are enjoying longer lives. However, there are limited systemic supports for older individuals with disabilities. The Arc of the United States (2011) reported that 32% of adults with disabilities were waiting for government-funded services for more than 5 years. In addition, due to the lack of sufficient funding for adult services, 75% of individuals with disabilities do not receive formal services and supports (Braddock et al., 2015). Consequently, caregiving for individuals with disabilities falls onto family members.
As individuals with disabilities outlive their parents, siblings of individuals with disabilities may fulfill caregiving roles (Hodapp, Sanderson, Meskis, & Casale, 2017). Based on their roles, siblings may provide a range of caregiving responsibilities. For example, Burke, Taylor, Urbano, and Hodappcolleagues (2012) found that siblings secured residential arrangements, made financial plans, held legal guardianship roles, interacted with the service delivery systems, and offered companionship to their brothers and sisters with disabilities. Furthermore, some siblings provide no caregiving (Lee, Burke, Arnold, & Owen, 2018), whereas other siblings report providing full-time care to their brothers and sisters with disabilities (Freedman, Krauss, & Seltzer, 1997; Woodman, Mailick, Anderson, & Esbensen, 2014). Notably, caregiving roles may change throughout the life span (Hodapp, Glidden, & Kaiser, 2005). Specifically, as parental health declines, siblings may provide greater types and amounts of caregiving (Lee, Burke, Arnold, & Owen, 2019).
The extent of caregiving may be defined as a range of caregiving demands, and the number of caregiving hours; both facets of caregiving may be influenced by several factors, including the severity of the disability. For example, previous research has suggested that several sibling characteristics (e.g., identifying as female, being the only offspring without a disability in the family) and sibling relationship characteristics (e.g., having close proximity between siblings, reporting positive sibling relationships) facilitate caregiving roles (for a review, see Lee & Burke, 2018). However, the research is limited and mixed regarding characteristics of the individual with a disability that may correlate with caregiving, especially disability severity. Only five studies have examined the relation between the severity of the disability (i.e., functional ability and/or maladaptive behaviors) and sibling caregiving. In two studies, when individuals had more severe disabilities (i.e., less functional ability and/or more maladaptive behaviors), siblings were more likely to provide caregiving (Lee et al., 2019; Seltzer, Begun, Seltzer, & Krauss, 1991). Other studies either reported opposite findings (e.g., Krauss, Seltzer, Gordon, & Friedman, 1996) or no relation between the severity of the disability and sibling caregiving (Burke et al., 2012; Heller & Kramer, 2009).
Furthermore, severity of the disability may impact the advocacy of the sibling and future planning. Regarding the former, when individuals have severe disabilities, families often advocate more for needed supports and services (Neely-Barnes, Marcenko, & Weber, 2008; Taylor & Henninger, 2015). Furthermore, as older adults with disabilities are more likely to need health and other services into their old age (Burke & Heller, 2016), advocacy may become even more important for their caregivers. Future planning may also correlate with the severity of the disability. Previous findings are mixed with some research finding a positive correlation between the severity of the disability and future planning (Burke, Arnold, & Owen, 2018; Lee et al., 2019) and some research finding no relation (Heller & Kramer, 2009).
Although siblings are likely to fulfill caregiving roles, little is known about the relation between sibling caregiving and the severity of the disability. Specifically, there is limited extant research about the relation between disability severity with sibling advocacy (Burke, Patton, & Lee, 2017) and future planning (Burke et al., 2018). The research about caregiving and disability severity is limited and has mixed findings. Furthermore, none of the limited extant research has directly examined caregiving, advocacy, and future planning among siblings of older adults with disabilities (Lee & Burke, 2018). Because siblings often fulfill caregiving roles later in their life when their parents are no longer able to provide caregiving (Hodapp et al., 2017), it is especially necessary to examine sibling caregiving among older adults with disabilities. The absence of research is problematic as parents of individuals with the most severe disabilities report significant caregiving burden and greater advocacy (McCann, Bull, & Winzenberg, 2012). However, it is unknown whether such a nonlinear pattern applies to adult siblings. In addition, by the time siblings fulfill caregiving roles, their brothers and sisters with severe disabilities are older adults, only increasing the need for caregiving, advocacy, and planning. Indeed, older adults with disabilities may have great support needs related to their aging, physical and mental health problems, and disability needs (Lin, Lin, & Hsu, 2016).
It is critical to better understand the relation between the severity of the disability and sibling caregiving, including advocacy and future planning. Specifically, it is important to quantify at what point the severity of the disability impacts sibling caregiving. For this study, we had two research questions.
We defined the severity of the disability by examining functional ability and maladaptive behaviors (i.e., externalizing, internalizing, and asocial behaviors) of individuals with disabilities. In alignment with previous research about older adults with disabilities, “older adults” were defined as individuals aged 40 and above (Heller, 1997; Seltzer & Krauss, 1987). When an individual has a more severe disability, they often have more intensive supports necessitating greater caregiving demands and hours for daily care and service coordination (Burke et al., 2018), thus we hypothesized that the severity of the disability would positively correlate with the extent of caregiving, caregiving hours, caregiving demands, and caregiving supporters, as well as advocacy and future planning. Specifically, we hypothesized a positive, nonlinear pattern between the severity of the disability and sibling caregiving, advocacy, and future planning. A positive nonlinear pattern indicates that there is a significant increase in caregiving, advocacy, and future planning only when individuals have the most severe disabilities.
Method
Participants
Participants were a subset (N = 141) of 1,100 adult siblings of individuals with disabilities who completed a national, web-based survey about siblings of individuals with disabilities. The inclusionary criteria were as follows: siblings who were older than 18 years of age, had brothers/sisters with disabilities who were older than 40 years of age, and completed more than 75% of the scaled measures in the survey. Consequently, participants with brothers or sisters younger than 40 years old (n = 863), and who completed less than 75% of the scaled measures (n = 96) were excluded from this study. Therefore, we included 141 participants.
In Table 1, the demographic characteristics of the participants and their brothers and sisters with disabilities are summarized. Participants were primarily female (89.4%, n = 126), White (89.4%, n = 126), and had at least a college degree (96.4%, n = 136). The mean age of the sibling respondent was 55.87 years (SD = 8.48), with a range from 33 to 78 years. We also gathered information from participants about their brothers or sisters with disabilities. Half of the participants’ brothers or sisters with disabilities were male (51.8%, n = 73); on average, they were 51.46 years of age (SD = 8.70), ranging from 44 to 76 years old. In addition, 27.7% (n = 39) of the brothers or sisters with disabilities lived in their family homes. The sample represented 33 of the 50 states.
Participants’ Characteristics (N = 141).
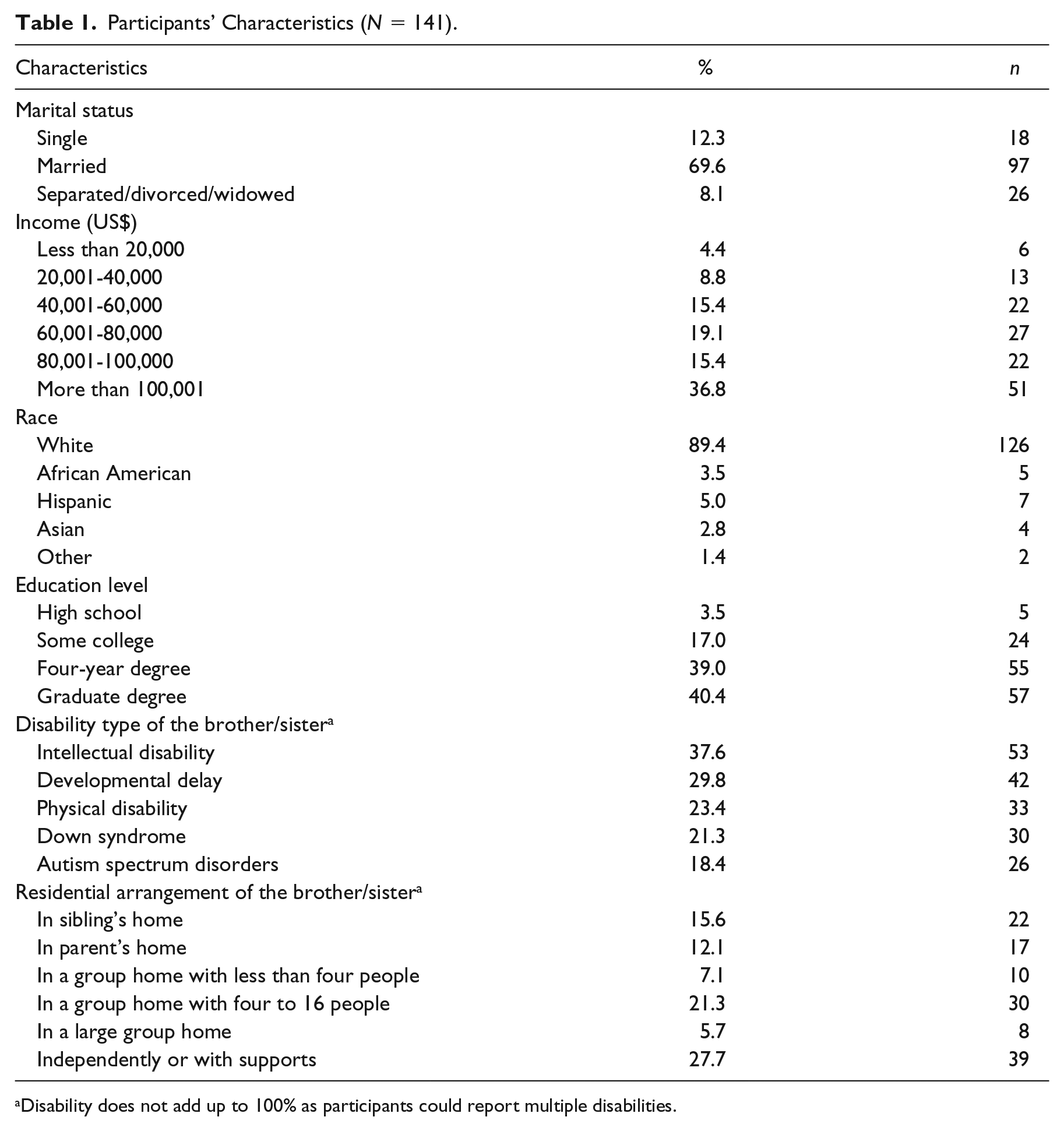
Disability does not add up to 100% as participants could report multiple disabilities.
Adult Sibling Survey
In collaboration with the Sibling Leadership Network, we developed the Adult Sibling Survey. We received feedback from professors, professionals, and siblings of individuals with disabilities. Then, we piloted the survey with five siblings of individuals with disabilities; revisions were minimal. For example, we revised a multiple-choice question to a ranked order question; also, we added a response option with respect to family size. All recruitment and study procedures were approved by the University Institutional Review Board. The survey was put onto a secure survey platform, Qualtrics, and was available from September 2018 to May 2019 With respect to the survey, there was a total of 250 questions which, using branching logic, took 20 to 25 min to complete. For this study, we used the following measures as independent and dependent variables.
Independent variable: Severity of the disability (functional ability)
To measure functional ability, we used the Activities of Daily Living (ADL) Index, which was developed by Lawton, Moss, Fulcomer, and Kleban (1982). Respondents were asked about 15 items in relation to the functional abilities of their brother or sister with disabilities. Items included “laundry,” “prepare meals,” and “eat.” For each item, there were three potential responses: (a) with no help, (b) with some help, and (c) with total help. Higher scores denoted a more severe disability. In a previous study of parents of adults with disabilities, the ADL scale had high reliability (Cronbach’s α = .94, Heller & Kramer, 2009). In this study, the ADL scale also had high reliability (Cronbach’s α = .94).
Independent variable: Severity of the disability (maladaptive behaviors)
To measure maladaptive behavior, the Scale of Independent Behavior–Revised (SIB-R; Bruininks, Woodcock, Weatherman, & Hill, 1996) was used in this study. The scale has eight items, grouped in three factors: internalizing behaviors (i.e., hurtful to self, unusual or repetitive habits, withdrawal or inattentive behavior), externalizing behaviors (i.e., hurtful to others, destructive to property, disruptive behavior), and asocial behaviors (i.e., socially offensive behavior, uncooperative behavior). Together, the frequency and severity of the maladaptive behaviors were summed into the General Maladaptive Index (GMI) indicating the degree of serious maladaptive behaviors. Higher scores indicated more serious maladaptive behaviors. Previous researchers reported high reliability (Lee et al., 2019; Cronbach’s α = .91). In our sample, reliability was high (Cronbach’s α = .90). The individual factors (i.e., externalizing, internalizing, and asocial behaviors) were also used in this study; each factor had acceptable reliability (Cronbach’s αs = .68, .77, and .66, respectively).
Dependent variable: The extent of caregiving
Using an established scale developed by Horowitz (1985), respondents completed 10 items about the extent of caregiving. Specifically, participants answered the following question: “In which domains, do you provide caregiving for your brother or sister with a disability?” The domains included the following: transportation, household help, shopping, meal preparation, personal care, health care, financial management, linkage with formal services, emotional support, and financial assistance. Responses were on a 5-point Likert-type scale including 0 = never, 1 = rarely, 2 = somewhat, 3 = often, and 4 = frequently. Responses were summed to create an aggregate score. In a previous study, this scale had high internal consistency (Cronbach’s α = .82, Horowitz, 1985). For this study, the reliability was high (Cronbach’s α = .94).
Dependent variable: Caregiving hours
Respondents answered one question about the number of hours spent on caregiving: “How much time did you spend caregiving for your brother or sister in the last week?” Responses options were (0) none, (1) 1 to 2 hr per week, (2) 3 to 4 hr per week, (3) 5 to 14 hr per week, (4) 15 to 30 hr per week, (5) 31 to 60 hr per week, and (6) more than 60 hr per week.
Dependent variable: Caregiving demands
Using an established scale developed by Perkins and Haley (2010), respondents were asked to rate seven statements about difficulties due to caregiving responsibilities. Statements included the following: “I am unable to have the time to do things that I enjoy,” “I lack adequate help from others,” “I feel stressed and emotionally drained,” “I am physically tired,” “I need to prioritize caregiving demands,” “I need to find someone to care for my child when I’m caring for my brother or sister,” and “I am unable to maintain my own job.” Response options were rated on a 5-point Likert-type scale ranging from 1 = not a problem to 5 = a very serious problem. A summed variable ranging from 7 to 35 was used for this study. Previous studies have reported high reliability for this scale (e.g., Cronbach’s α = .86, Perkins and Haley, 2010). For this sample, the Cronbach’s alpha was .92.
Dependent variable: Total number of caregiving supporters
One question was asked about caregiving supporters: “Who besides you is involved in caregiving or helping your brother or sister with disabilities?”; notably, this question has been used in prior studies to characterize the number of caregiving supporters (Penrod, Kane, Kane, & Finch, 1995). Respondents could choose multiple responses including the following: father/mother, other sibling, relatives, friends, community (church or neighbors), paid workers, and others. The summed variable ranged from 0 to 7 indicating the total number of caregiving supporters.
Dependent variable: Advocacy
Using an established advocacy scale about adult services (Taylor, Hodapp, Burke, Waitz-Kudla, & Rabideau, 2017), respondents answered 11 questions about their disability advocacy experiences. Questions included the following: “Have you searched the Internet to find agencies and/or services to meet your sibling’s needs?” “Have you talked with others about agencies and/or services to meet your sibling’s needs?” and “Have you called adult service provider agencies to ask about eligibility and services?.” All items were rated on a Likert-type scale ranging from 0 = not at all to 4 = very often. In a previous study, this scale had strong reliability (Cronbach’s α was .92, Taylor et al., 2017). In this study, Cronbach’s alpha was .84.
Dependent variable: Future planning
Using the established scale developed by Heller and Kramer (2009), this scale consisted of 11 future planning activities. Participants were asked the following: “The questions below describe various activities related to future planning and your involvement, or barriers to involvement, in these activities. Have you or your family . . . ?” Activities included the following: created a letter of intent, located an attorney, established legal guardianship or powers of attorney, established a special needs trust, identified a successor, looked into a residential program, made residential plans, and discussed future plans with the entire family and person with a disability. Potential responses were dichotomous: 0 = no or 1 = yes. A summed variable ranging from 0 to 11 was used for this study; this scale had strong internal consistency in a prior study about families of individuals with disabilities (Kuder–Richardson coefficient = .86; Burke & Heller, 2016). For this sample, the Kuder–Richardson coefficient was .86.
Covariate: Income
Participants were asked about their annual household income. Response options were as follows: 1 = US$20,000 or less, 2 = US$20,001 to US$40,000, 3 = US$40,001 to US$60,000, 4 = US$60,001 to US$80,000, 5 = US$80,001 to US$100,000, and 6 = More than US$100,000.
Covariate: Residential arrangement
Participants were asked one question about the residential arrangement of the brother or sister with a disability. We dichotomized the residential arrangement into two options: (a) living in a family home (i.e., sibling’s home, parent’s home) or (b) living outside of a family home (i.e., in a group home, independently in the community).
Procedures
Information about and access to the survey was disseminated through different platforms to recruit a diverse national sample. E-mails and recruitment flyers were distributed to local and state disability organizations as well as state chapters of the Sibling Leadership Network throughout the United States. In addition, the flyer was distributed to state and local chapters of The Arc and the 67 University Centers for Excellence in Developmental Disabilities. E-mails were also distributed to the 7,843 agencies listed in the Yellow Pages for Kids with Disabilities. Such agencies included the following: private service providers (n = 3,025), advocacy and legal agencies (n = 1,725), schools and educational agencies (n = 1,386), nonprofit disability agencies (n = 1,271), and parent support groups (n = 436). There was no financial incentive to participate in the survey.
All surveys were completed electronically. To access the survey, respondents were asked to click on a uniform resource locator provided in an e-mail or posted on a website. Responses were stored in Qualtrics Survey Software and downloaded periodically to guard against computer malfunctions. None of the individual responses were linked to identified individuals. Responses were subsequently transferred into a Statistical Package for the Social Sciences (SPSS) data set.
Data Analyses
For preliminary analyses, we conducted descriptive statistics (e.g., frequency) and imputed missing values for scaled measures by substituting mean scores for missing values (Harrell, 2001). We evaluated the internal reliability of the scaled measures using Cronbach’s alpha and Kuder–Richardson coefficients. Also, we reviewed the distribution of the scaled measures. All measures were normally distributed. We proceeded with parametric statistics (e.g., Pearson correlations, linear regression). For the primary analyses, we conducted Pearson correlations to examine the relations between the severity of the disability and caregiving, advocacy, and future planning. Next, we conducted linear and curvilinear regressions to determine the best fitting models for the relations between caregiving, advocacy, future planning, and the severity of the disability. Notably, income level and residential arrangement were correlated with dependent variables. Thus, income and residential arrangement were included as covariates in the regressions.
Results
Nature of Caregiving by Siblings of Older Adults with Disabilities
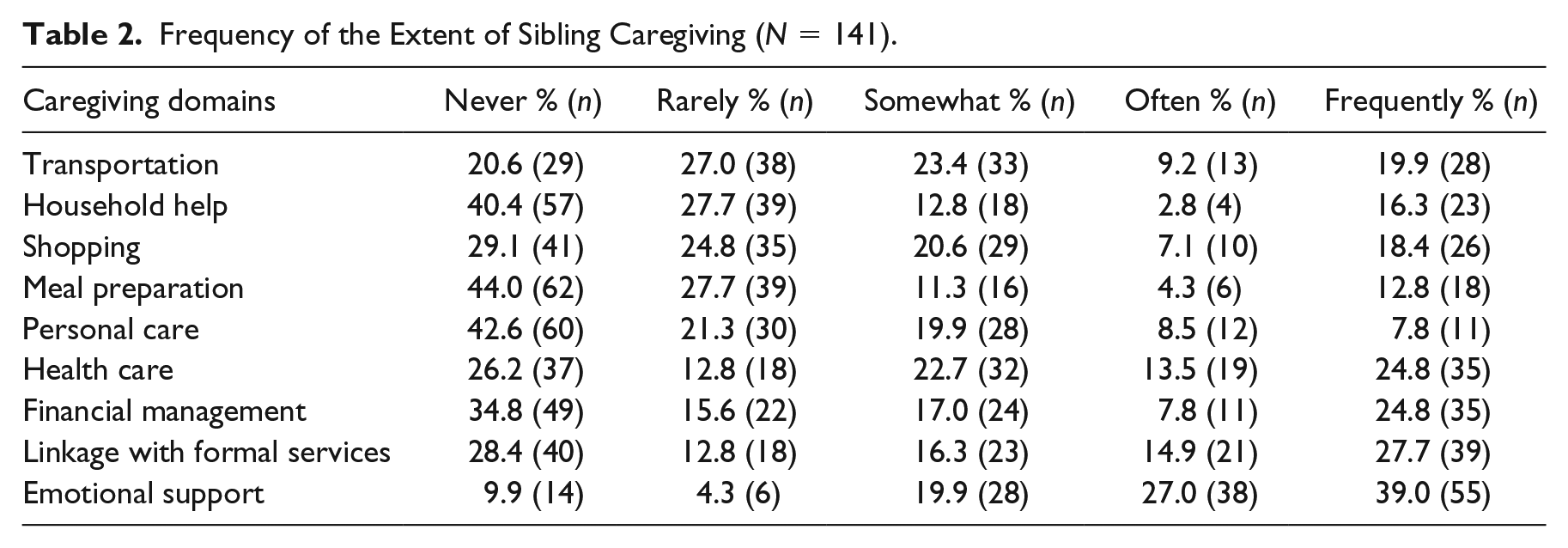
The most frequent caregiving domains (i.e., domains wherein participants reported conducting each caregiving domain as “often” or “frequently”) were as follows: providing emotional support (66.0%, n = 93), linking the adult with a disability with formal services (42.6%, n = 60), and accessing health care for the adult with a disability (38.3%, n = 54). The least frequent caregiving domains were as follows: providing personal care (16.3%, n = 23), offering meal preparation (17.1%, n = 24), and conducting household help (19.1%, n = 27) (see Table 2).
Frequency of the Extent of Sibling Caregiving (N = 141).
With respect to caregiving hours, 30.5% (n = 43) of siblings provided no caregiving in the last week, 23.4% (n = 33) of siblings provided 1 to 2 hr per week, 10.6% (n = 15) of siblings provided 3 to 4 hr per week, 14.9% (n = 21) of siblings provided 5 to 14 hr per week, 8.5% (n = 12) of siblings provided 15 to 30 hr per week, 4.3% (n = 6) of siblings provided 31 to 60 hr per week, and 7.8% (n = 11) of siblings provided caregiving more than 60 hr per week.
With respect to caregiving demands, the most frequent type of caregiving demands (i.e., demands wherein participants reported as “a serious problem” or “a very serious problem”) were as follows: I feel stressed and emotionally drained (29.1%, n = 41), I am physically tired (27.0%, n = 38), and I need to prioritize caregiving demands (19.8%, n = 28). With respect to number of caregiving supporters, 2.1% (n = 3) of siblings had no caregiving supporters, 48.9% (n = 69) of siblings had one supporter, 28.4% (n = 40) of siblings had two supporters, 14.2% (n = 20) of siblings had three supporters, 2.8% (n = 4) of siblings had four supporters, 2.8% (n = 4) of siblings had five supporters, and 0.7% (n = 1) of siblings had six supporters.
We also examined the relation between residential arrangements and the nature of sibling caregiving. Altogether, 39 siblings had a brother or sister with a disability living in a family home and reported the following caregiving hours: 12.8% (n = 5) of siblings reported no caregiving, 25.6% (n = 10) of siblings reported 1 to 2 hr per week, 7.7% (n = 3) of siblings reported 3 to 4 hr per week, 10.2% (n = 4) of siblings reported 5 to 14 hr per week, 7.7% (n = 3) of siblings reported 15 to 30 hr per week, 15.4% (n = 6) of siblings reported 31 to 60 hr per week, and 20.5% (n = 8) of siblings reported more than 60 hr per week. In comparison, 102 siblings had a brother or sister with a disability living outside of the family home; they reported the following caregiving hours: 37.2% (n = 38) of siblings reported no caregiving, 22.5% (n = 23) of siblings reported 1 to 2 hr per week, 11.8% (n = 12) of siblings reported 3 to 4 hr per week, 16.7% (n = 17) of siblings reported 5 to 14 hr per week, 8.8% (n = 9) of siblings reported 15to 30 hr per week, and 2.9% (n = 3) of siblings reported more than 60 hr per week. There was a significant difference in caregiving hours for living in a family home (M = 4.03, SD = 2.22) and outside of a family home (M = 2.49, SD = 1.57); t(139) = 4.60, p < .001.
Functional Abilities and Caregiving, Advocacy, and Future Planning
There was a strong, positive correlation between the functional abilities of individuals with disabilities and the extent of caregiving r(141) = .220, p < .01 and caregiving hours r(141) = .21, p < .05. Furthermore, functional abilities positively correlated with advocacy and future planning, r(141) = .316 and .503, ps < .01, respectively. Because higher scores on the ADL is related to less functional ability, this correlation indicates that individuals with less functional ability received greater sibling caregiving, advocacy, and future planning. However, the total number of caregiver supporters and caregiving demands were not significantly correlated with functional abilities (see Table 3).
Correlation Matrix.
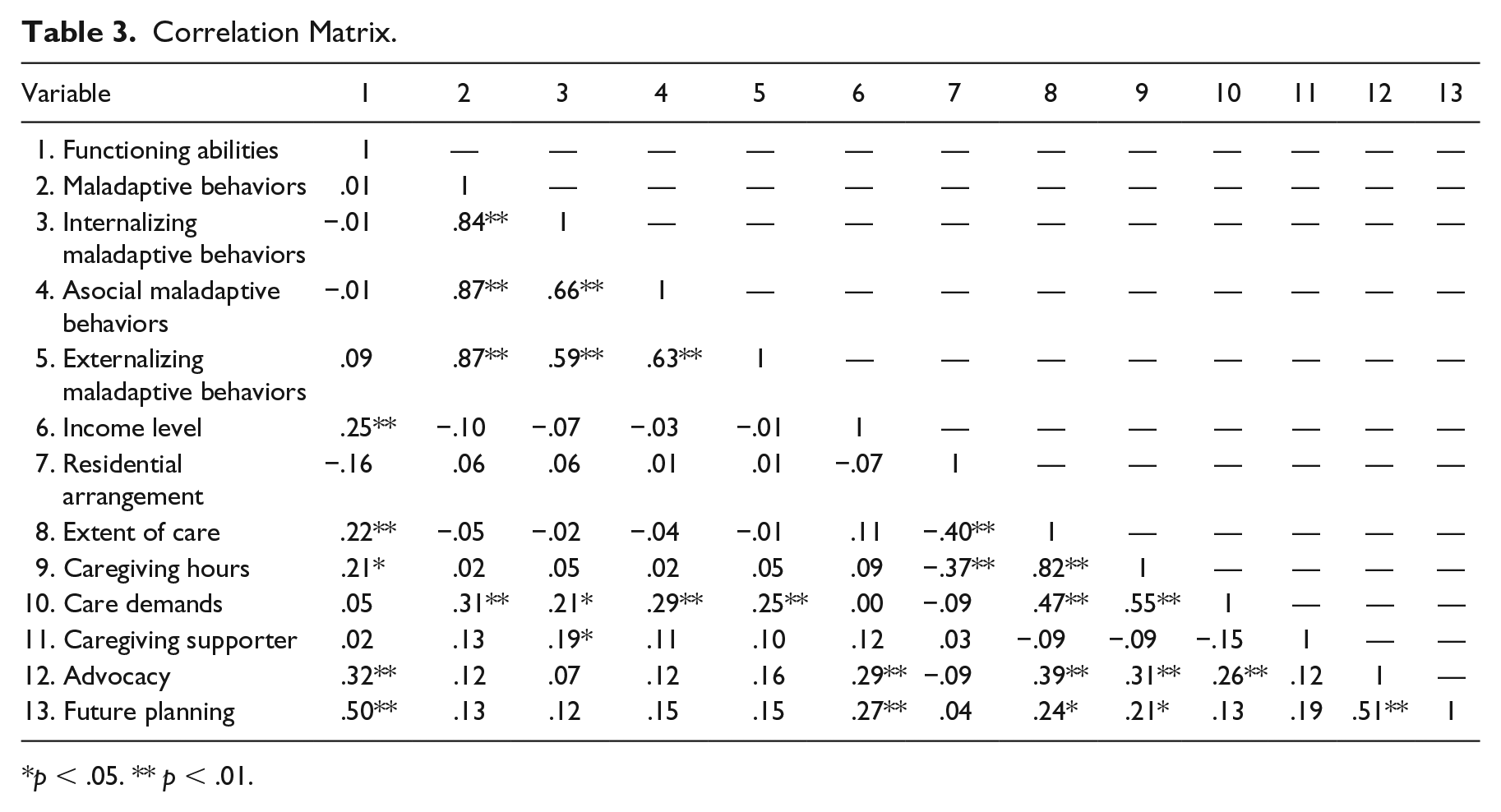
p < .05. ** p < .01.
Given that individuals with the fewest functional abilities (i.e., individuals with the most severe disabilities) may be the most likely to require caregiving, advocacy, and future planning, linear and curvilinear regressions were conducted to determine the best fitting models for the relations between functional abilities and caregiving, advocacy, and future planning. Notably, income and residential arrangement were included as covariates in the linear and curvilinear regressions. Regarding the extent of caregiving, a strong curvilinear (vs. linear) relation existed with functional abilities. Specifically, functional abilities explained only 18.6% of the variance, F(3, 138) = 10.03, p < .001, whereas the curvilinear regression explained 20.1% of the variance, F(4, 137) = 8.23, p < .001. With respect to caregiving hours, the linear regression explained 16.8% of the variance, F(3, 138) = 8.86, p <.00, whereas the curvilinear regression explained 17.4% of the variance, F(4, 137) = 6.91, p < .001. Similarly, curvilinear (vs. linear) regressions explained more variance with respect to advocacy and future planning. Regarding advocacy, the linear regression explained 13.6% of the variance, F(3, 138) = 6.90, p < .001, whereas the curvilinear regression explained 14.9% of the variance, F(4, 137) = 5.72, p < .001. Regarding future planning, the linear regression explained 29.1% of the variance, F(3, 138) = 13.27, p < .001, whereas the curvilinear regression explained 35.2% of the variance, F(4, 137) = 13.04, p < .001.
Maladaptive Behaviors and Caregiving, Advocacy, and Future Planning
Only caregiving demands were significantly, positively correlated with maladaptive behaviors, r(141) = .307, p < .01. To carefully examine the relation of different types of maladaptive behaviors with caregiving, correlations were conducted with each type of maladaptive behavior (i.e., internalizing, externalizing, and asocial maladaptive behaviors) and caregiving, advocacy, and future planning. There were positive correlations between internalizing behavior and caregiving demands r(141) = .212, p < .05, externalizing behavior and caregiving demands r(141) = .247, p < .01, and asocial behavior and caregiving demands r(141) = .288, p < .01. In addition, there was a positive correlation between internalizing behavior and number of caregiving supporters r(141) = .193, p < .05. No other correlations were significant (see Table 3).
After controlling for income and residential arrangement, there were no significant relations between internalizing and externalizing maladaptive behaviors and caregiving demands. Only asocial maladaptive behaviors significantly related to caregiving demands. Specifically, the linear regression explained 7% of the variance, F(3, 138) = 2.95, p = .035, whereas the curvilinear regression explained 7.5% of the variance with respect to caregiving demands, F(4, 137) = 2.36, p = .058. For the number of caregiving supporters, the curvilinear (vs. linear) regression explained more variance regarding the relation with internalizing behavior. Specifically, the linear regression explained 7.1% of the variance, F(3, 138) = 3.01, p = .03, whereas the curvilinear linear regression explained 7.7% of the variance, F(4, 137) = 2.43, p = .05.
Discussion
Overall, sibling caregivers of older adults with disabilities provided caregiving for a range of caregiving domains and hours. Specifically, functional ability displayed a curvilinear relation with caregiving, advocacy, and future planning. In addition, only asocial maladaptive behaviors positively correlated with caregiving demands. Finally, there was a positive, curvilinear relation between internalizing maladaptive behaviors and the number of caregiving supporters.
This study has four main findings. First, siblings provided specific types of care for older adults with disabilities. Consistent with prior studies (Burke et al., 2012; Freedman et al., 1997; Woodman et al., 2014), siblings may pursue diverse types and amounts of caregiving. This study extends the literature by identifying caregiving domains that were prevalent among siblings of older adults with disabilities. For example, more than two thirds of participants were engaged in accessing health care services for their brothers and sisters with disabilities. Although previous studies (Burke et al., 2012) did not include health care as a caregiving domain, aging and disability-related health issues have been consistently addressed as a national priority for family caregiving (Krahn & Fox, 2014). Our finding suggests that sibling caregivers of older adults with disabilities not only provide caregiving with respect to daily life care, emotional support, and linkage to formal service delivery system but they also provide caregiving in the area of health care.
Second, older adults with the least functional abilities were significantly more likely to have siblings who engaged in caregiving, advocacy, and future planning. This finding aligns with prior research suggesting a positive correlation between the severity of the disability and family caregiving (Lee et al., 2019; Seltzer et al., 1991), advocacy (Neely-Barnes et al., 2008; Taylor & Henninger, 2015), and future planning (Burke et al., 2018; Lee et al., 2019). This study extends the literature by demonstrating that this relation is nonlinear with respect to caregiving. Perhaps because most sibling research focuses on small samples (Hodapp et al., 2017), prior studies have had insufficient power to examine the relation between the severity of the disability and caregiving. Future research should include larger samples with older adults with severe disabilities to more closely examine the relation with caregiving, advocacy, and future planning.
Third, maladaptive behaviors of older adults with disabilities were correlated positively with caregiving demands. For decades, research has suggested that there is a strong, bidirectional relation between maladaptive behavior and caregiving demands and burden (e.g., Burke et al., 2018; Neece, Green, & Baker, 2012). However, most of the prior studies have been limited to parents of individuals with disabilities (Unwin & Deb, 2011). This study extends the literature by demonstrating that maladaptive behaviors also relate to greater caregiving demands among siblings of adults with disabilities. This finding is important as greater maladaptive behaviors have other, negative effects on siblings including more negative sibling relationships (Krauss et al., 1996; Orsmond, Kuo, & Seltzer, 2009). By identifying another negative relation with maladaptive behaviors, this study adds credence to supporting siblings of older adults with significant maladaptive behaviors.
Furthermore, there was a significant, nonlinear pattern between asocial behavior (i.e., socially offensive behavior, uncooperative behavior) and caregiving demands. Specifically, siblings of individuals with the most severe asocial behaviors had the most caregiving demands. Among parents of adults with disabilities, there is also a positive correlation between asocial behaviors and caregiving demands (Bailey, Raspa, Olmsted, & Holiday, 2008). Replicating this finding among siblings suggests that a similar pattern may exist across all family caregivers (i.e., siblings and parents). However, given that this was a cross-sectional study, future research is needed to determine the direction of the relation between maladaptive behaviors and caregiving demands.
Finally, there was a strong, nonlinear relation between internalizing behavior (i.e., hurtful to self, unusual or repetitive habits, and withdrawal or inattentive behavior) and the number of caregiver supporters. Little research has examined the relation between internalizing behavior and family caregiving among adults with disabilities. However, the literature about internalizing behaviors among children with disabilities suggests that greater internalizing behaviors relates to greater parent stress (Bauminger, Solomon, & Rogers, 2010). Compared with externalizing behaviors, internalizing behaviors are less visible and more difficult to manage (Dowdy, Chin, Twyford, & Dever, 2011). Thus, it may be that greater internalizing behaviors among older adults with disabilities signals that more support is needed for sibling caregivers.
Implications for Future Research
In the future, longitudinal research is needed to examine the effect of disability severity of older adults with disabilities on the health and well-being of sibling caregivers. From this study, it seems that caregiving demands increase with maladaptive behaviors; furthermore, the extent of caregiving increases when individuals with disabilities have less functional ability. Although unexplored in the sibling literature, the research about parent caregivers of adults with disabilities suggests a “wear and tear” effect on parents wherein caregivers’ physical and mental health is gradually worsening due to caregiving demands (Pearlin, Schieman, Fazio, & Meersman, 2005). Notably, the “wear and tear” effect intensifies with the severity of the disability (Seltzer et al., 2010). Future research should examine whether there is a similar “wear and tear” effect among sibling caregivers; specifically, such research should examine whether this effect specifically impacts siblings of individuals with more severe disabilities.
Future research is also needed to identify other sources of variance with respect to caregiving, advocacy, and future planning. From this study, it seems that the severity of the disability is only one piece of the puzzle in explaining caregiving, advocacy, and future planning. Indeed, maladaptive behaviors explained only 7% of the variance in relation to caregiving demands. Future research may examine other caregiver characteristics, such as race (Namkung, Greenberg, & Mailick, 2017; Sonik, Parish, & Rosenthal, 2016), age (Lee et al., 2019; Sonik et al., 2016), and distance to their brother or sister’s residence (Orsmond & Seltzer, 2007). For instance, older (vs. younger) siblings are significantly more likely to be caregivers for their brothers and sisters with disabilities (Lee et al., 2019). Future research should identify other correlates of sibling caregiving, advocacy, and future planning.
Limitations
First, although a national sample was used in this study, the web-based survey format may have limited participation from siblings who were less educated or from low-income or minority backgrounds. Relatedly, there was no response rate for this study; thus, the differences between responders and nonresponders are unknown. Second, siblings who participated in the survey may have more positive relationships with their brothers and sisters with disabilities; as such, this may not be a representative sample of siblings. Third, this study relied on cross-sectional data. The direction of effects cannot be determined without longitudinal data.
Implications for Practice
When parents shift their caregiving roles to siblings, siblings should be prepared to provide caregiving in a variety of domains. Our study suggests that siblings often engage in navigating adult service delivery systems and health care services for their brothers and sisters with disabilities. Thus, it is important to support siblings to effectively advocate for adult services for their brothers and sisters with disabilities (Arnold, Heller, & Kramer, 2012). To do so, adult service providers may educate sibling caregivers about available services (Friedman, Caldwell, Kennedy, & Rizzolo, 2019). Adult service providers may also provide information to sibling caregivers about health promotion programs for individuals with disabilities (Heller & Sorensen, 2013).
Also, practitioners may need to address the caregiving demands of siblings of individuals with greater maladaptive behaviors. Especially, practitioners may need to focus efforts on sibling caregivers of older adults with greater asocial behaviors. For example, to reduce caregiving demands, practitioners may help secure respite for caregivers (Williamson et al., 2016). Receipt of respite care has been found to decrease parent stress, improve marital relationships, as well as increase caregiver financial well-being (Caldwell & Heller, 2003; Harper, Dyches, Harper, Roper, & South, 2013). Given the effects of respite, adult service providers may consider referring sibling caregivers to respite programs.
Footnotes
Editors-in-Charge: Stacy K. Dymond and K. Charlie Lakin
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided from the Texas Developmental Disabilities Council. However, the manuscript solely reflects the opinions of the authors and not the funding agency.