
Abstract
Little is known about how, when, or why individuals with intellectual and developmental disabilities (IDD) retire. Recognizing the changing needs of older adults with IDD is critical to support person-driven services and development of best practices in aging transitions. Using secondary analysis of the 2016 to 2017 National Core Indicators–Adult Consumer Survey (NCI-ACS) data for adults with IDD, we examined the relation between independent mobility (i.e., without aids), age group, level of intellectual disability, and type of employment/activity program, with a focus on mobility and community-based employment in older age groups. There was an overall age-related decline in mobility, but the prevalence of mobility impairment by age group was related to employment type. The percentage who were independently mobile was highest for community employment in every age group. The percentage of individuals by age group in community employment fell significantly from middle age onward, suggesting some former community-based workers had retired. There was no significant age-related difference in the percentage in facility-based employment across these age groups. Mobility limitations may be a barrier to obtaining or retaining community-based employment. Age-related mobility impairment may be associated with premature retirement, and could affect travel to and from work, undertaking work tasks, or both. Closer examination is needed of aging, community employment, and age-related mobility limitations to understand the specific causes of these effects on employment and identify supports and accommodations.
Retirement, defined as withdrawal from paid work, is typically related to aging (Stancliffe, Brotherton, O’Loughlin, & Wilson, 2017; Wang & Shultz, 2010), but the age when people retire can vary. The average age for retirement in the United States is around 62 years (U.S. Census Bureau, 2014). Nowadays, many people with intellectual and developmental disabilities (IDD) are living beyond the common retirement age of 65 years (Coppus, 2013). Some people enter retirement by choice, after careful planning and supplementing income, whereas others are forced into retirement by poor health, job instability, or other circumstances (Stancliffe et al., 2017). Workers with IDD do retire (Stancliffe, Kramme, & Nye-Lengerman, 2018), but little is known about individuals’ ages at, or reasons for, retirement. Retirement represents a major life transition, so it is critical to examine the context of when, how, and why individuals with IDD retire.
Retirement is defined as exiting from paid community- or facility-based employment (Stancliffe et al., 2017; Wang & Shultz, 2010). Departure from unpaid activity, such as a day program or volunteering, does not meet this definition. Retirement differs from unemployment, because an unemployed individual is seeking paid work. Retirement is typically permanent, and the person is no longer seeking paid employment (Stancliffe et al., 2017).
Although there are low rates of individuals with IDD in paid community work, research suggests an age-related decline in employment among individuals with IDD (Stancliffe et al., 2018). Community-based employment is often referred to as competitive, integrated employment, which is employment in the general workforce at or above minimum wage (Hiersteiner, Butterworth, Bershadsky, & Bonardi, 2018). Even today, it is common for people with IDD to work in facility-based (sheltered) settings. In 2016 to 2017, 21% of people with IDD worked in sheltered employment, compared with 15% of individuals with IDD who worked in integrated community settings, and 6% in community group employment (Hiersteiner et al., 2018). Other adults with IDD participated in unpaid activities in a facility setting (38%), or unpaid community setting (24%), or had no structured activities outside home (Hiersteiner et al., 2018). Individuals may take part in more than one type of employment or day activity. These data highlight the low workforce participation of individuals with disabilities in general but acknowledge the disturbingly low rates of individuals with IDD in paid community work. Furthermore, participation in paid community work may decline with the age of individuals with IDD. Overall employment rates of people with IDD fall after ages 45 to 54 years, although about 18% remain employed after age 65 years (Stancliffe et al., 2018).
It is currently unknown at what age or why people with IDD retire. Stancliffe et al. (2018) found that most people with IDD leave work suddenly, rather than gradually transitioning to retirement. One possible reason for retiring could be age-related decline in independent mobility. Mobility impairments are a barrier for gaining and retaining employment in the general community (Crawford, Hollingsworth, Morgan, & Gray, 2008) and among disability groups. More than one third of unemployed people with disabilities reported barriers to employment that could be addressed with workplace accommodations, and people who received such accommodations were more likely to be employed (Anand & Senak, 2017). Mobility limitations may require modifications of the employee’s transportation, physical environment, or workstation. Workplace accommodations, including the built environment, job restructuring, and other supports have been shown to help people with disabilities maintain employment in inclusive settings (Anand & Senak, 2017; Tompa et al., 2015). Nord, Stancliffe, Nye-Lengerman, and Hewitt (2016) controlled for multiple factors including health and level of IDD, and found that adults with IDD who were independently mobile without aids were 6.5 times more likely to have community jobs than those who were not mobile. People with IDD who are employed most commonly report working in building maintenance, grounds crew, or cleaning (32.4%); food service or preparation (20.4%); and in retail, including stock or sales clerk (14.7%; Butterworth, Hiersteiner, Engler, Bershadsky, & Bradley, 2015). These employment types often require physical mobility unless job accommodations can be identified and utilized. Because people with IDD are living longer than ever before (Coppus, 2013) and are more likely to experience mobility limitations as they age (Ferrucci et al., 2016), the impact of mobility limitations on work and retirement as people with IDD age is of interest.
Although a diagnosis of IDD does not imply co-occurring physical disabilities, some people with IDD experience limitations in independent physical mobility. Developmental disabilities, such as cerebral palsy, can affect both intellectual and physical functioning, and mobility impairment may increase over the life course. Like the general community, some individuals with IDD may acquire a mobility impairment in older age, having previously been independently mobile without aids (Evenhuis, 1997). Prevalence rates of mobility limitations among adults with IDD range from 3% to 63%, depending on the measure used and sampling factors such as age, gender, diagnosis, and level of IDD (Cleaver, Hunter, & Ouellette-Kuntz, 2009). Prevalence and severity of mobility limitations generally increase with age. Among Dutch adults above 50 years, people with intellectual disability (ID) were more likely than the general population to develop frailty earlier, and poor health or frailty was related to the use of a mobility device or wheelchair (Evenhuis, Hermans, Hilgenkamp, Bastiaanse, & Echteld, 2012). A longitudinal study of 77 older people with ID in the Netherlands showed 30% of people with ID aged 60 to 75 years used an aid for walking or a wheelchair, increasing to 58% for people above 75 years (Evenhuis, 1997).
In addition to mobility impairments, transportation may affect paid employment as access to transportation is needed to get from home to paid employment. Most individuals with IDD do not drive, and so they require transportation to work (Bezyak, Sabella, & Gattis, 2017). Across disability types, access to transportation, physical location, and travel requirements were noted as major considerations in finding and keeping employment (Graham, Inge, Wehman, Seward, & Bogenschutz, 2018). McCausland, Stancliffe, McCallion, and McCarron (2019) reported that older people with IDD in Ireland mostly used transportation provided by disability staff to attend work or day programs, with a minority traveling independently using public transportation. Those working in community employment were more likely to use public transportation than people involved in segregated employment or day programs (McCausland et al., 2019). Public transportation use is more difficult for people with a mobility impairment, so age-related mobility problems may affect travel to work, especially for community employment. Transportation may be a factor in retirement as well.
Age and level of ID may also affect the different types of employment or day activities for individuals with ID. As noted, employment rates fall in older age groups (Bush & Tassé, 2017; Stancliffe et al., 2018), whereas mobility impairment is more prevalent in older age (Evenhuis, 1997; Evenhuis et al., 2012; Lehmann et al., 2013). Level of ID is significantly related to employment, with those with milder ID experiencing better community employment outcomes (Bush & Tassé, 2017). Participants in community-based employment tend to be younger than facility-based employment (Bush & Tassé, 2017). Thus, there is a need to consider these interrelations when examining, for example, the association between mobility and different types of employment.
Researchers have begun to focus on retirement by people with IDD, but many fundamental issues remain unexamined, such as the factors associated with retirement. The current study focuses on one specific factor, mobility impairment. It is currently unknown how mobility impairment is related to employment rates and whether mobility limitations affect retirement for people with IDD. The specific purpose of this study was to explore the relation between age group, mobility impairment, participation rates for different types of employment or activity programs, level of ID, and transportation, with a particular focus on mobility impairment and community employment rates among the older age groups. For this study, we undertook a secondary analysis of National Core Indicators–Adult Consumer Survey (NCI-ACS) 2016 to 2017 data. The research questions were as follows:
We propose that environmental and demographic factors related to mobility and transportation may affect at what age, or from what setting, an individual with IDD retires. We hypothesize that those in community-based employment are less likely to use mobility aids or disability transportation but are more likely to retire than peers in facility-based employment.
Method
NCI–ACS
The NCI project, a voluntary effort by participating U.S. states, measures both state and national trends in IDD service system indicators and outcomes (Bradley & Moseley, 2007). Each state that participates is asked to recruit a random sample of at least 400 adult service users with IDD who receive case management and at least one other IDD service. Within the NCI project, there is an annual, cross-sectional ACS. The NCI-ACS has three sections, but in the present study, all variables were drawn from the first section, “Background Information.” This section includes questions about demographics (e.g., gender, age), disability diagnoses (e.g., level of ID), mobility, employment/daily activity, and disability services (e.g., transportation). Psychometric properties of the NCI-ACS are described by the National Association of State Directors of Developmental Disabilities Services and Human Services Research Institute (2012). Available psychometric data on the NCI-ACS have focused on Section I that involves an in-person interview with the adult with IDD. We know of no specific psychometric data about the “Background” section.
Sample
The 2016 to 2017 NCI-ACS sample contained data for 21,548 participants from 39 states (AL, AR, CO, CT, DC, DE, FL, GA, HI, ID, IL, IN, KS, KY, LA, ME, MI, MN, MO, MS, NC, NE, NH, NJ, NV, NY, OH, OK, OR, PA, RI, SD, TN, TX, UT, VA, VT, WI, WY). Our analyses involved comparisons by age group. The age group coding used in these analyses involved people aged 20 or older who participated in work/day activities; who were not enrolled in educational programs such as public school, vocational school, or college; and who did not live in an institution or nursing home. Because we were interested in comparing mobility across different types of work and day programs, we only included participants with a single type of job or day program and valid (i.e., nonmissing) data on age and mobility. This was to ensure that there was a clear relation between job/day activity type and other variables such as age and mobility. The four types of employment were (a) paid community-based employment, (b) paid facility-based (sheltered/segregated) employment, (c) unpaid community-based activities, and (d) unpaid facility-based activities. These criteria yielded a sample of 8,129 participants. The characteristics of these participants are presented in Tables 1 and 2.
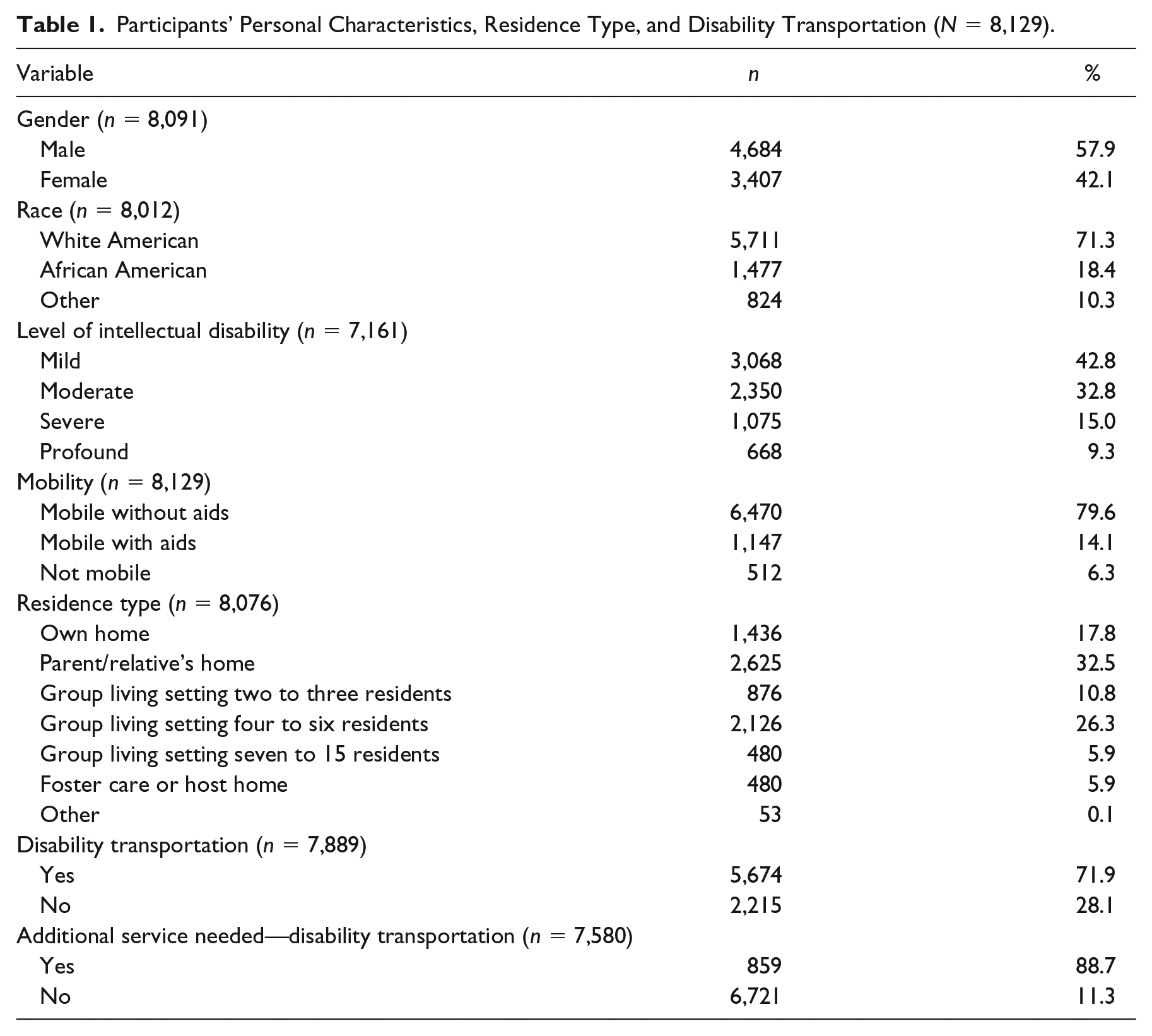
Participants’ Personal Characteristics, Residence Type, and Disability Transportation (N = 8,129).
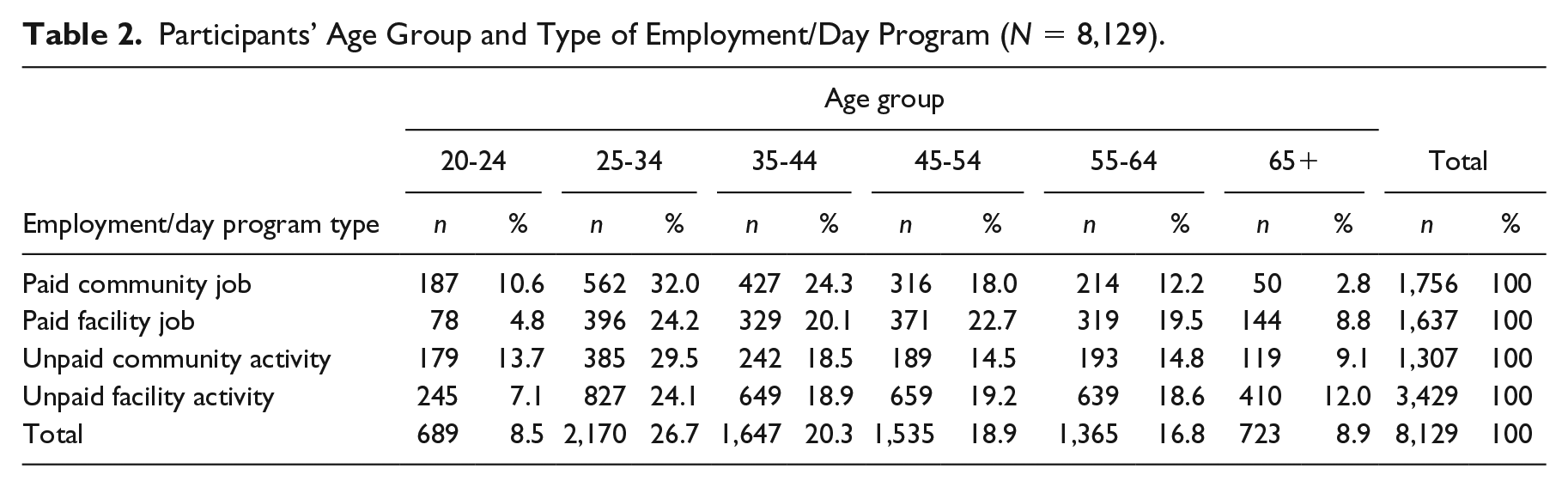
Participants’ Age Group and Type of Employment/Day Program (N = 8,129).
Because we excluded 13,419 (62.3%) of the original NCI-ACS sample of 21,548, we compared the selected and nonselected groups to see whether they differed on important variables. We found several significant differences, but most were relatively small. More participants in the selected (79.6%) than the nonselected (75.0%) sample were independently mobile without aids, χ2(2, N = 21,098) = 94.74, p < .001. Regarding employment, 21.6% (selected) and 18.8% (nonselected) had community-based employment, χ2(2, N = 20,054) = 23.32, p < .001. By contrast, 20.1% (selected) and 19.9% (nonselected) had facility-based employment, χ2(2, N = 19,407) = 0.23, p = .64. The selected sample (38.1% mild ID, 8.3% profound) had milder ID than the nonselected sample (34.3% mild, 9.5% profound), χ2(6, N = 21,181) = 238.79, p < .001. The selected sample was older (M = 43.32 years) than the nonselected sample (M = 41.45 years), t(18,068) = 8.76, p < .001.
Measures
Data for the independent variables came from the NCI-ACS “Background Information” section and included (a) age (which we recoded into age group), (b) level of ID, (c) mobility, (d) participation in employment/day activities (community- and facility-based reported separately), (e) disability transportation, and (f) need for transportation. Mobility also served as a dependent variable in the logistic regression analysis.
Data on employment and day activities came from separate items asking whether the person engaged in each of the following activities during a typical 2-week period: (a) paid job in a community-based setting (data on individual and small-group community jobs were combined), (b) unpaid community-based activity, (c) paid facility-based job, and (d) unpaid facility-based activity.
For individuals with a diagnosis of ID, the NCI-ACS asks which level of ID is applicable (mild, moderate, severe, profound) with no further definition provided. Individuals without ID or with an unspecified level of ID were classified as having missing data for this item. The NCI-ACS mobility item asked, “How would you describe this person’s mobility? Check ONE.” The response options were (a) moves self around environment without aids; (b) moves self around environment with aids or uses wheelchair independently; (c) nonambulatory, always needs assistance to move around environment; and (d) don’t know.
As Table 1 shows, overall, only 14.1% were mobile with aids (e.g., uses wheelchair independently) and 6.3% were not mobile and always needed assistance. The relatively small size of these two groups may have introduced problems of small cell size in more complex analyses, so for most analyses, we combined them. In those cases, the mobility data effectively became a binary (yes/no) variable, meaning independently mobile without aids or with aids.
The NCI-ACS asks whether the participant receives transportation as a disability service. The response options are (a) yes and (b) no. No information is available about where the service transports people (e.g., work, day program, elsewhere). The NCI-ACS also asks about need for additional services, including for disability transportation. This is also a yes/no question.
Procedures
Data for the NCI-ACS “Background” section are typically collected from the case manager, service coordinator, or system records. Where relevant, the person’s job coach may provide information about employment. In some cases, the individual, guardian, or family members may also serve as respondents for the “Background” section.
Analyses
The prevalence of missing data is shown in Table 1. All analyses used available data with no missing data imputation. Sample sizes are reported for each analysis. Most analyses involve two- or three-way chi-square analyses. We were interested in the details of differences (e.g., across age groups), so for many chi-square analyses, we also summarized the findings of Bonferroni corrected pairwise comparisons of column proportions conducted using the SPSS BPROP subcommand. Logistic regression was used to control for age and level of ID for our analysis of the relation between type of employment/day program and mobility.
Results
Employment by Age Group
To answer Research Question 1, it is necessary to describe the relation between age and employment. Our sample yielded a significantly different pattern of participation in work and day programs by age group as shown in Figure 1, χ2(15, N = 8,129) = 314.16, p < .001. There was a marked decline in the percentage with a community-based job in older age groups, from 25.9% (35-44 years) to 6.9% (65+ years). For individuals aged 35 to 44 years, as the age group increased, the drop in the percentage with a community job was significant from each age group to the next (pairwise comparisons, p < .05, Bonferroni adjusted), suggesting that many who worked in community employment when younger began to retire from middle age onward.

Percentage by work or activity type and age group (N = 8,129).
By contrast, the percentage with a facility-based job did not change significantly in the four older age groups, from 20.0% (35- to 44-year-olds) to 19.9% (individuals aged 65 years and older; pairwise comparisons were all nonsignificant). Likewise, there was no significant change between the four older age groups in their percentage of participation in unpaid community activities, from 14.7% (35- to 44-year-olds) to 16.5% (individuals aged 65 years and older; pairwise comparisons all nonsignificant). However, for unpaid facility-based activities, there was a significant increase by age group from 39.4% (35- to 44-year-olds) to 56.7% (individuals aged 65 years and older; p < .05 Bonferroni adjusted). In conjunction with the opposite trend among older age groups in participation in community employment, one likely interpretation is that many individuals who retire from community employment join facility-based day programs in retirement. See Figure 1.
Mobility by Age Group
Figure 2 shows significant overall trends in mobility by age group, χ2(10, N = 8,129) = 313.89, p < .001. There was a significant age-related reduction in those who were mobile without aids (mobile), from 87.8% (20- to 24-year-olds) to 61.3% (individuals aged 65 years and older; pairwise comparisons for the 45-54, 55-64, and 65+ age groups, all ps < .05, Bonferroni adjusted). Likewise, there was a significant increase by age group in those who were mobile with aids, from 6.5% (20- to 24-year-olds) to 31.4% (individuals aged 65 years and older; pairwise comparisons for 45-54, 55-64, and 65+ age groups, all ps < .05, Bonferroni adjusted). By contrast, there was no significant age-related difference in the percentage who were not mobile, from 5.7% (20- to 24-year-olds) to 7.3% (individuals aged 65 and older; all pairwise comparisons were nonsignificant). Although these data were cross sectional, the clear pattern across the increasing age groups was for fewer people to be independently mobile without aids and for a commensurate increase in those who were mobile with aids, with no change in the percentage who were not mobile. These results are consistent with a pattern of age-related mobility impairment for a large minority of participants, requiring them to use mobility aids to move about their environment. See Figure 2.
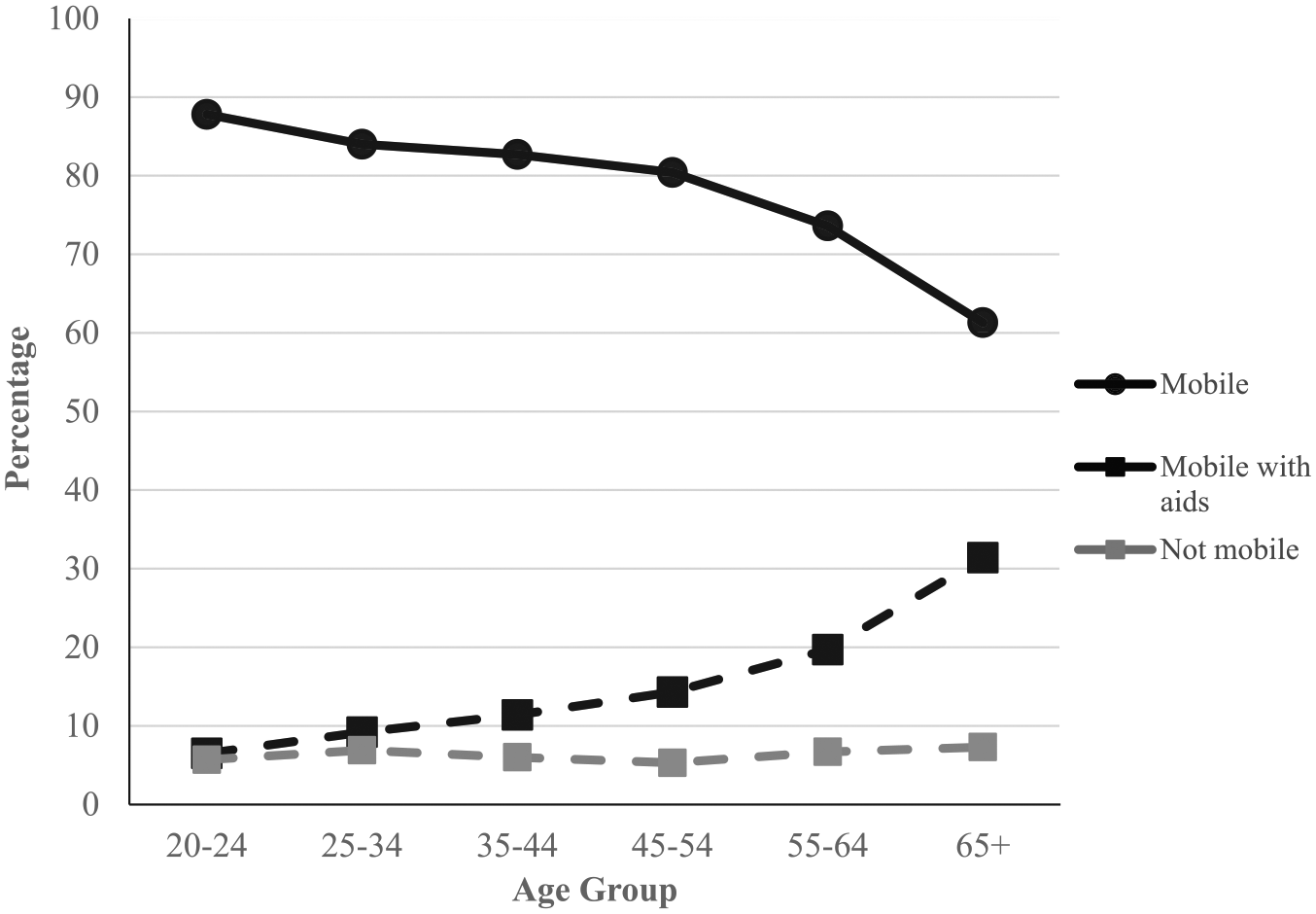
Mobility by age group (N = 8,129).
Mobility by Employment/Day Activity Type
Those in community-based employment were more likely to be independently mobile without aids. Using the original, three-level mobility variable, each employment/day activity type differed significantly. The percentage who were independently mobile without aids was 93.3% for participants in paid community employment, 84.7% for paid facility-based employment, 76.3% for unpaid community activities, and 71.4% for unpaid facility-based activities, χ2(6, N = 8129) = 434.44, p < .001, with each of these four types differing significantly (all pairwise comparisons ps < .05, Bonferroni adjusted). Compared with each of the other three groups, the community employment group had a significantly smaller percentage who were mobile with aids (pairwise comparisons all ps < .05, Bonferroni adjusted). Those who were not mobile (i.e., always need assistance) revealed the opposite trend, from 0.3% of individuals in community employment, 2.6% of individuals in facility-based employment, 7.6% of individuals in community activities, to 10.6% of individuals in facility-based activities. Here too, the four employment/day activity types differed significantly from one another (all pairwise comparisons ps < .05, Bonferroni adjusted). Figure 3 shows these differences.
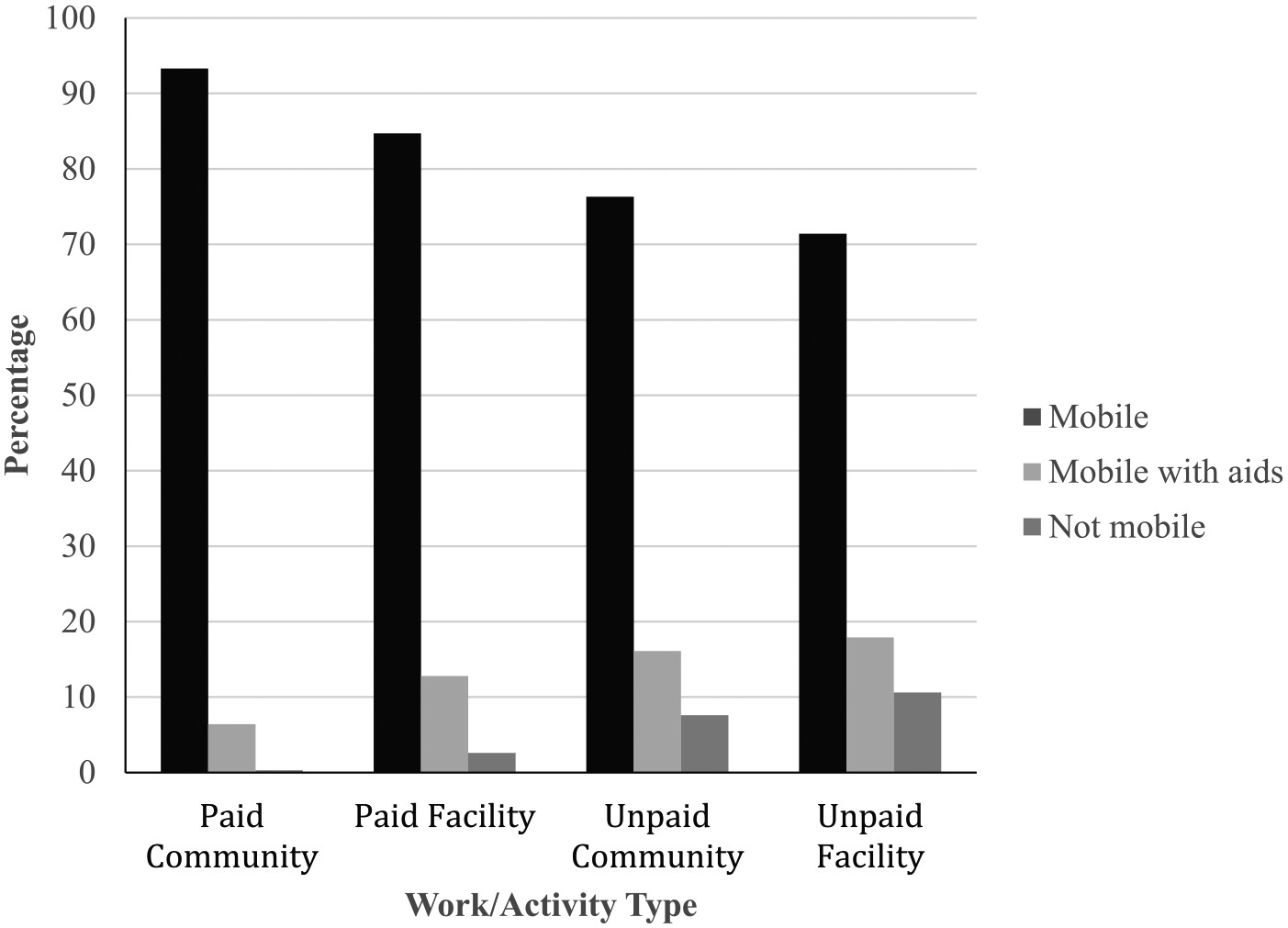
Mobility by work/activity type (N = 8,129).
In answering Research Question 2, and for subsequent analyses, we combined the two groups with mobility impairment (i.e., independently mobile with aids and not mobile). Therefore, we have not separately reported the percentage with mobility impairment because these numbers are simply the difference between the percentages shown in Figure 4 and 100%.
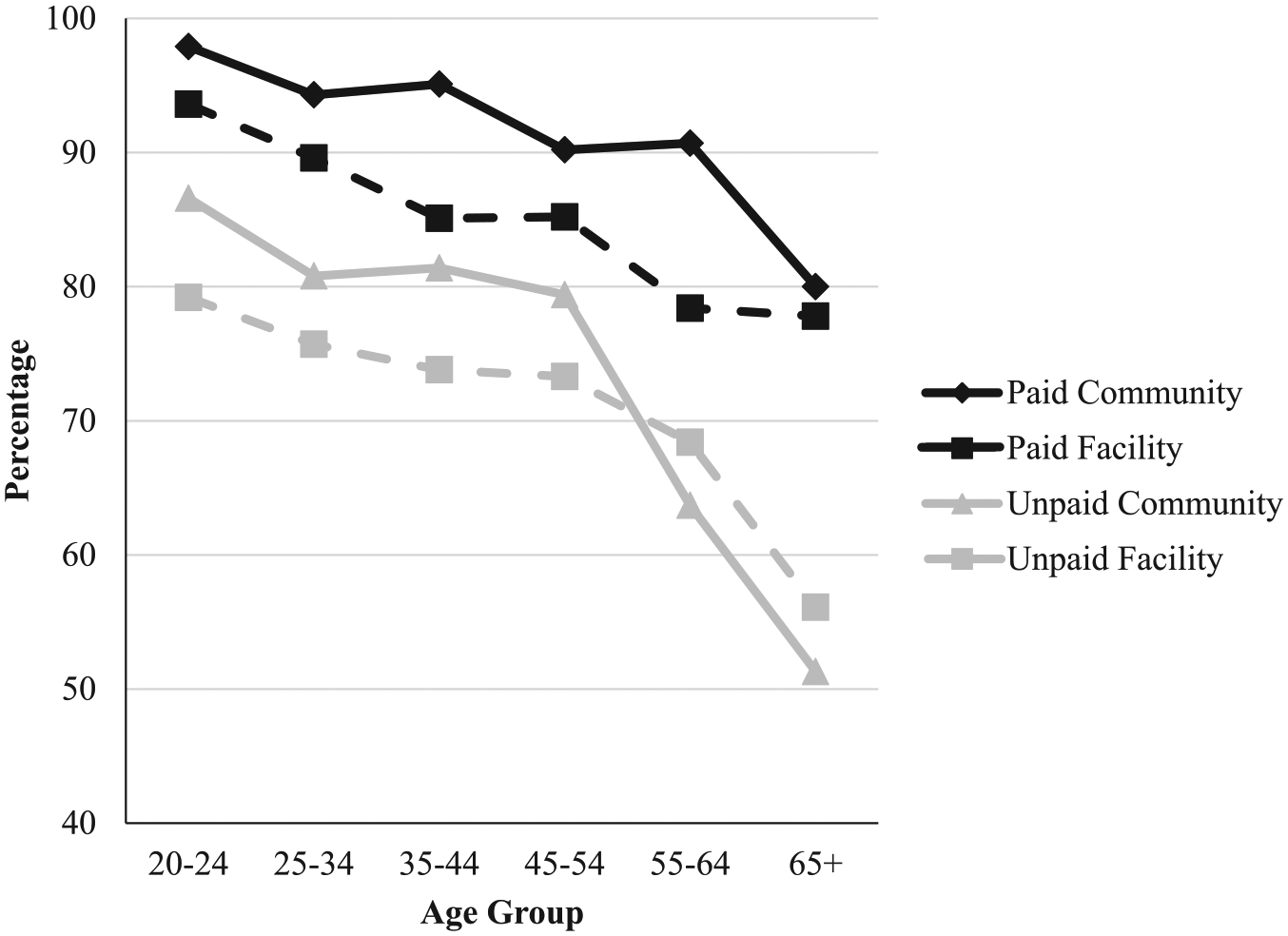
Percentage mobile without aids by work/activity type and age group (N = 8,129).
Chi-square comparisons within each employment/day activity type by age group revealed significant age-related declines (all ps < .001) for all four groups who were independently mobile without aids: χ2(5, N = 1,756) = 30.65, p < .001, community employment group; χ2(5, N = 1,637) = 27.48, p < .001, facility-based employment; χ2(5, N = 1,307) = 77.31, p < .001, community activity; and χ2(5, N = 3,429) = 67.62, p < .001, facility-based activity.
There were smaller age-related declines for both paid employment groups. For community employment, the decline from the 20 to 24 age group (97.9%) to the 65+ age group (80.0%) was 17.9%, with no significant pairwise differences among the 45 to 54, 55 to 64, and 65+ groups. The equivalent declines for the other three groups were facility-based employment (15.8%), community activities (35.3%), and facility-based activities (23.1%).
Interrelated variables
To examine the potential confounding effect of interrelated variables on the relation between mobility and employment, we began by looking at differences in level of ID and age between the four employment/day activity groups. There was a strong relation between level of ID and job/day activity type, χ2(9, N = 7,161) = 1,031.35, p < .001. Fewer participants with community-based employment had moderate (24.4%), severe (4.1%), or profound (1.1%) ID compared with facility-based activities (34.7%, 21.9%, and 16.1%, respectively). The percentage who were independently mobile without aids differed significantly between each level of ID from profound (50.0%), severe (71.1%), moderate (83.9%), and mild (86.4%), χ2(3, N = 7,161) = 528.37, p < .001. As seen in Figure 2, there was also a significant relation between mobility and age, with a lower percentage who were independently mobile without aids in older age groups. Therefore, the higher percentage in community-based employment who were independently mobile could be an artifact of their younger age and milder level of ID, rather than a direct effect of mobility itself.
Logistic regression
To control for age and level of ID, we entered these variables into a logistic regression of the relation between type of employment/day program and mobility. Because 968 cases had missing data for level of ID (see Table 1), the sample was 7,161. Table 3 shows that, controlling for age group and level of ID, using unpaid facility-based activities as the reference group, those in community employment were 3.85 times as likely to be independently mobile without aids (p < .001). As expected, Table 3 also shows that, relative to the 65+ reference group, younger age groups were significantly more likely to be mobile without aids. Consistent with the notion of age-related mobility impairment, the odds ratios increase uniformly with each successively younger age group, indicating an increasing likelihood of being independently mobile. The Nagelkerke R2 for the logistic regression was .17.
Results of Logistic Regression of Independent Mobility Without Aids (N = 7,161).
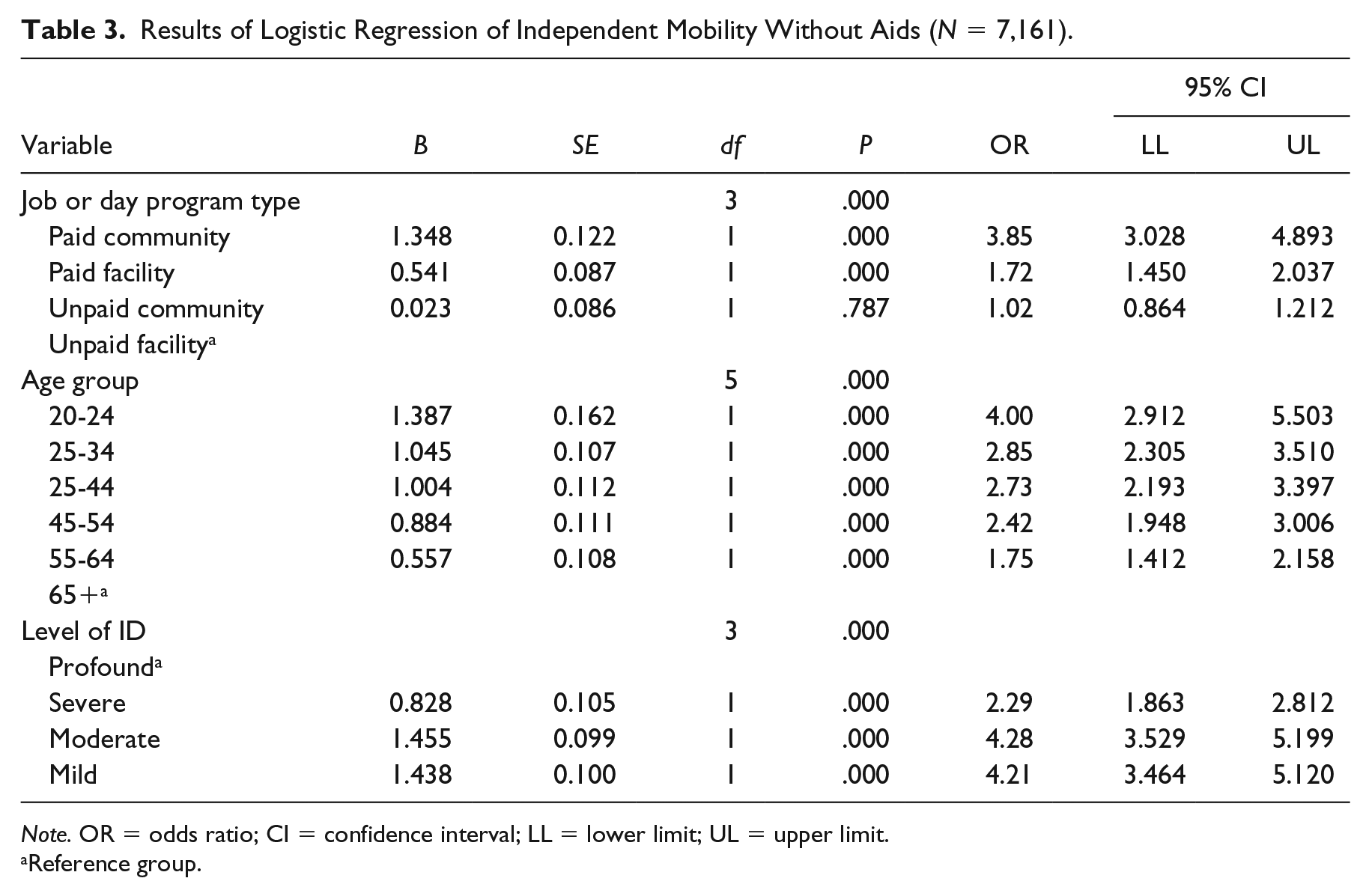
Note. OR = odds ratio; CI = confidence interval; LL = lower limit; UL = upper limit.
Reference group.
Transportation Services
In relation to Research Question 3, we found significant differences in availability of transportation by work/day program type, χ2(3, N = 7,889) = 207.07, p < .001. Those in community-based work (65.3%) or community-based unpaid activities (61.1%) had significantly less access to disability transportation than those in facility-based work (82.5%) or facility-based activities (74.2%; pairwise comparisons, ps < .05, Bonferroni adjusted).
We also examined the availability of disability transportation and found overall significant age-group differences, χ2(5, N = 7,889) = 127.54, p < .001. Across every age group except 65+, there were consistently lower percentages with disability transportation in community employment as compared with facility-based employment (pairwise comparisons, ps < .05, Bonferroni adjusted). For community-based employment, access to disability transportation increased with age, χ2(5, N = 1,689) = 21.32, p = .001, suggesting that the problems arising from age-related mobility problems for travel to community employment likely were at least partially offset by increased availability of disability transportation. There was no significant change by age group in access to disability transportation for those in facility-based employment, χ2(5, N = 1,609) = 8.42, p = .13. Disability transportation appears to be part of the package for most attending facility-based employment, regardless of age group.
Figure 5 shows the percentage by age group and by community- or facility-based employment reporting that they needed disability transportation. A higher percentage of those in community employment responded that they needed disability transportation. In both employment groups, the percentage needing disability transportation fell significantly as the age group increased, χ2(5, N = 1,626) = 25.68, p < .001 (community employment), and χ2(5, N = 1,516) = 15.58, p = .008 (facility-based employment). These data suggest that disability transportation needs were more often met in older age groups, with a low level of unmet need in the 65+ group.
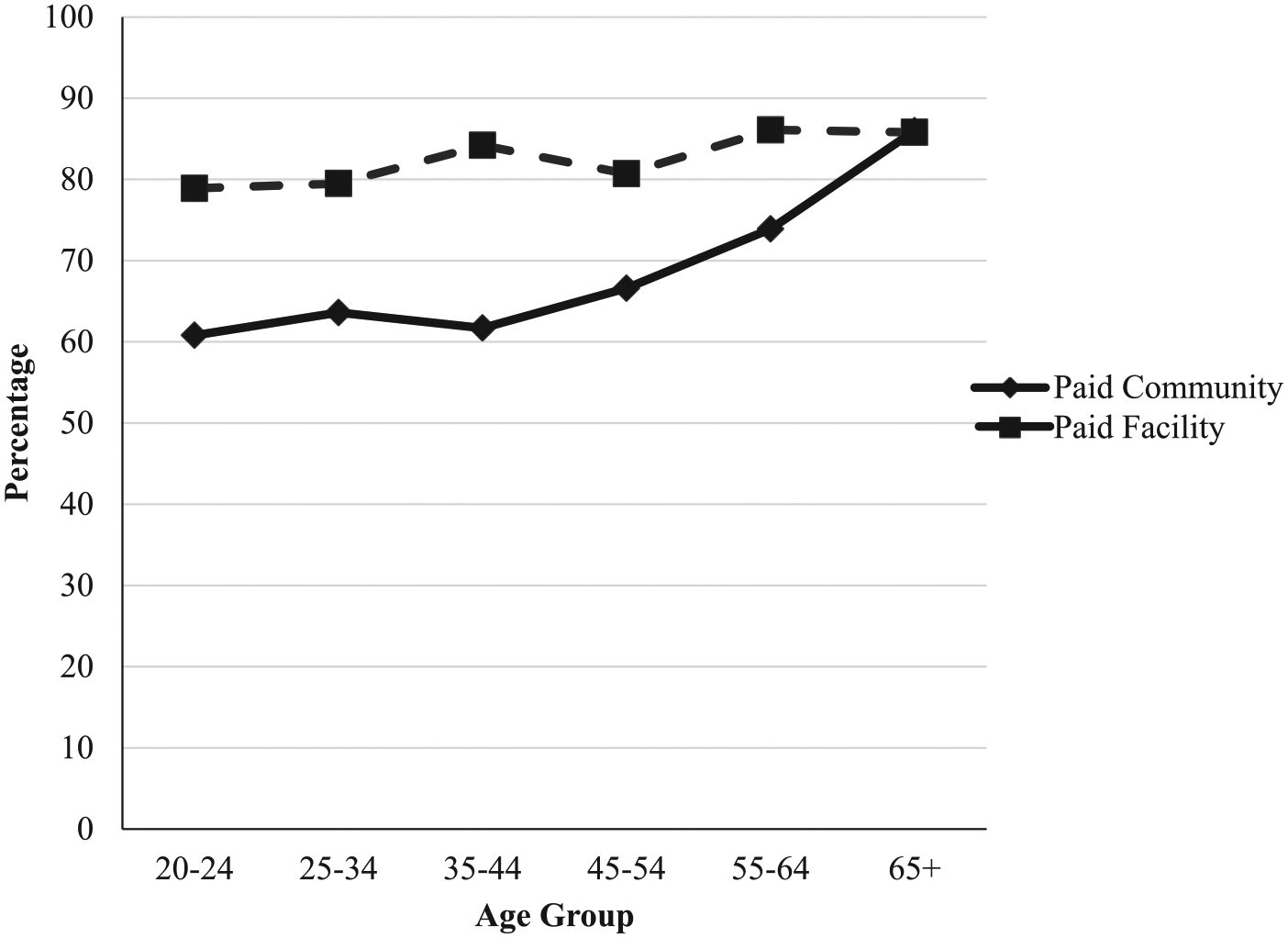
Percentage needing disability transportation by age group and employment type (N = 3,142 shown).
Discussion
This study examined the relations between aging, employment, mobility, transportation, and retirement using NCI-ACS data. Using “exit from paid employment” as the definition for retirement, we were able to examine demographic and environmental factors that we infer are related to retirement. Our secondary analysis of 2016 to 2017 NCI-ACS data highlighted factors that may play a role in both employment and retirement. Relative to facility-based employment, there was a more marked decline in the percentage of participants in older age groups who work in community-based employment. The latter group’s percentage fell significantly in each age group from 35 to 44 years, whereas there was no significant age-related difference in the percentage in facility-based employment in this age range. This finding clearly suggests an age-related factor that more strongly affects community employment, and by inference retirement, in older age groups. This study investigated whether age-related mobility impairment is one such factor.
Mobility
Adults with IDD, like the rest of the community, experience a higher prevalence of mobility impairment in older age (Lehmann et al., 2013). With increasing age, we found a large increase in the percentage who use aids for independent mobility. The large scale of the age-related decline in independent mobility without aids represents an important disability system challenge, especially for older workers, that requires careful research and evidence-informed policy action to minimize any detrimental effects. In addition, participants with severe disabilities had a much higher prevalence of mobility impairment, a finding that likewise warrants significant policy initiatives.
If mobility was not related to employment, the percentage who are independently mobile without aids should be very similar for all employment/day activity groups. Instead, we found that the community employment group had the highest percentage of individuals who were independently mobile without aids in every age group, suggesting that many older workers who acquired an age-related mobility impairment retired from community employment. The types of work that many individuals in community employment perform, such as janitorial, service, maintenance, and food preparation (Butterworth et al., 2015), are physical and require mobility to do the job tasks, making it difficult for older workers with age-related mobility impairment to continue to do their job as before if accommodations cannot be implemented. Likewise, the higher prevalence of mobility impairment among people with severe disabilities presents a barrier to them working in these types of community jobs.
Especially in paid community employment, a mobility impairment is a significant barrier to getting and keeping a job, suggesting problems with job retention if a worker develops an age-related mobility impairment during their period of community employment. Logically, the effect could be on travel to work, on undertaking work tasks, or both. With impairment, work- or travel-related aspects of mobility (e.g., walking long distances, using stairs, catching buses) become more difficult or impossible. Brotherton, Stancliffe, Wilson, and O’Loughlin (2019) reported that a number of older Australians with ID and many years’ experience of community employment retired because their health and mobility made work tasks and/or travel to work via public transportation difficult or unsafe. For example, four of the five participants had stopped traveling to work by public transportation before they retired.
One important issue is the relation between the severity of mobility impairment and associated activity limitations. We found some employment effects related to the severity of the mobility impairment. First, significantly fewer individuals with mobility impairment were employed in either community or facility-based work. Second, those not mobile were excluded from community employment, with a negligible 0.3% so employed. Within the category of independently mobile with aids, there is a spectrum of severity ranging from using a walking stick but meeting the mobility requirements of all work tasks, to those with severe impairment who are unable to use stairs or carry items. Many of the latter group would likely experience substantial employment impacts.
Facility-Based Employment
Compared with community employment (93.3%), significantly fewer people (84.7%) in facility-based employment were independently mobile without aids, yet the participation rate in facility employment in older age groups did not decline relative to middle age, which suggests that facility settings better accommodated older workers with age-related mobility impairment. It is unknown whether this outcome was due to (a) facility-based work tasks being less demanding, (b) these settings being better at providing mobility accommodations, or (c) facility-provided disability transportation making travel to work easier.
Unlike community employment, the percentage in facility-based work did not decline significantly in older age groups and was still around 20% even for the 65+ age group. We do not know why so few older workers retired from facility-based employment, whether continuing to work in older age was freely chosen or a result of the need for community living providers to have somewhere for residents to go during the day, regardless of age. Australian research reports that many older group home residents with IDD were not offered the option of retiring from sheltered employment because their accommodation service was unstaffed during the day (McDermott & Edwards, 2012).
Transportation
We found that those in community employment had significantly less access to disability transportation than those in facility-based work, suggesting that more in the community employment group traveled to work independently (e.g., by public transportation) or were driven by family members. One interpretation is that transportation is easier and cheaper for disability services to provide when they are transporting multiple individuals to a single location (e.g., to a facility), as compared with community locations that are dispersed and more individualized. Another interpretation is that those in community employment are more able, so more capable of getting themselves to work (walking, independent public transportation use). Taken alone, the finding of less access to disability transportation by those in community employment could indicate these individuals would be more affected by age-related mobility impairment because of the increased difficulty of traveling to work by public transportation or because of the nonavailability of aging parents to drive them. However, we also found that access to disability transportation by this group increased significantly in older age groups, suggesting that mobility-related travel problems in older age may be partially offset.
Limitations
The NCI-ACS has no specific questions about retirement or reasons for retirement. NCI-ACS data are cross sectional, thus precluding causal inferences. Stancliffe et al. (2018) noted that cross-sectional aging research can be subject to age cohort effects, especially for older participants who began working before community employment was as available. These workers may have remained in facility-based employment all their career. This factor may partially explain the lower percentage we found in community employment in older age groups. However, cohort effects do not explain the disproportionate numbers in community employment in all age groups who were independently mobile without aids. Cohort effects may have had some influence, but we contend that the association between aging, mobility impairment, and community job loss/retirement is real and important. No psychometric data about the NCI-ACS “Background” section were available, so its reliability is unknown, but the items involve factual questions often answered from written records, suggesting satisfactory reliability. We had no data on the mobility or travel requirements of the community- or the facility-based jobs of workers with IDD. More detailed data on severity of mobility impairment and on disability transportation would have enabled more refined examination of these issues. For these reasons, we inferred that mobility impairment was related to employment status and retirement, but we did not directly demonstrate this relation.
The NCI-ACS data represent a random sample of individuals with IDD who receive services from IDD systems in 39 states. We excluded people not involved in employment or day programs, and people who participated in more than one type, so our findings may not be representative of these excluded groups. We found significant but modest differences between the selected and nonselected samples from the overall NCI-ACS cohort for community employment, mobility, level of ID, and age, but no difference in participation rate for facility-based employment. Our results, although informative, cannot be generalized beyond the population represented in our analyses. Furthermore, some subgroups were relatively small, such as the 65+ community-employment group, which could have influenced the reliability of findings for that subgroup. Table 2 reports subgroup sample size to enable readers to make their own judgments about this issue.
Future Research
There are many unanswered questions about retirement and aging of individuals with IDD (McDermott & Edwards, 2012; Stancliffe et al., 2018). Longitudinal aging research is especially important and can reveal causal relations. Causes of retirement, such as health changes (including age-related mobility impairment), precede effects on outcomes such as employment and retirement. Future longitudinal research on age, mobility, transportation, employment, and retirement could evaluate whether changes in mobility are followed by changes in transportation to work, or by (premature) retirement (McCausland et al., 2019). Examination of the nature of work tasks and workplace accommodations (Anand & Senak, 2017; Tompa et al., 2015) could determine how they influence workplace participation and retirement. Prevention of age-related mobility impairment should also be a focus. For example, there is evidence that exercise and balance interventions reduce the risk of falling (Cortes-Amador et al., 2019), so future research could examine the effect of such interventions on employment and retirement among older workers.
The higher prevalence of mobility impairment among people with severe disabilities and their much lower rate of community employment should be the focus of future research examining whether the physical and mobility demands of many community jobs (e.g., janitorial, Butterworth et al., 2015) contribute to low community employment rates. If so, additional research on job matching and workplace accommodations suitable for people with severe disabilities should follow.
In addition, future research should examine the relation between severity of mobility impairment and the mobility requirements of work tasks, especially for older workers whose mobility may decline over time. Longitudinal research is also needed into the time course of changes in mobility and the opportunities for prevention of mobility impairments, and/or job accommodations for those with impaired mobility. The specific effects of mobility impairment were the focus of the current study, as opposed to other age-related health issues, including declining vision or hearing (Stancliffe et al., 2012). It could be that any additional disability or chronic health diagnosis as well as IDD is sufficient to increase the chances of job loss and premature retirement. Researchers could compare the specific employment effects of different age-related health conditions on different types of job tasks. For example, mobility impairment may have stronger effects on work requiring good mobility but have more limited impact on sedentary jobs where workers sit.
Implications for Practice
We found that large numbers of older workers with IDD are affected by age-related mobility impairments. In addition, individuals with severe disabilities often do not access paid employment settings. Yet, even those with severe disabilities report a desire to work and can be successfully employed (Ali, Schur, & Blanck, 2011; Freedman & Fesko, 1996). Our study’s findings serve as a reminder that those with severe disabilities continue to be more often absent from paid employment and may, in turn, miss out on benefits and choices in retirement. If many are retiring prematurely from community employment because of mobility-related problems with travel to work or with work tasks, then employers and service providers have a major role in solving these problems for individuals who want to keep working. Conversely, the higher participation rates in facility-based employment for the oldest workers suggest that some are not permitted to retire despite wanting to. Self-determined retirement planning and meaningful, socially inclusive activities in retirement would be an appropriate response.
The study’s overall findings also provide key lessons for state policies and the provider system. Workforce participation remains drastically low, especially for people with severe disabilities, despite policies and practices that can facilitate employment for people with IDD (Nord, Luecking, Mank, Kiernan, & Wray, 2013). If staying in the workforce is important to the person, we should provide supports and accommodations that grow with the person as they age, including job task changes or customization that allow individuals to keep working regardless of age or mobility. Workplace accommodations and modifications are most effective when individualized and employers are involved in implementing them (Tompa et al., 2015).
Conclusion
People with IDD can and want to work. Although mobility needs, aging, and transportation access can affect where, and how much, a person works, an individual’s desires and preferences should be prioritized. Individuals with IDD who are older and/or have higher support needs may need additional assistance with employment, but should not be denied the opportunity to work. State IDD systems and service providers can work in partnership with individuals and families to maximize expectations around participation and choice, to reduce the barriers that mobility impairments, transportation, or aging may have on workforce inclusion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is supported by Cooperative Agreement 90RTCP0003-01-00 from the National Institute on Disability Independent Living and Rehabilitation Research (NIDILRR) within the Administration for Community Living (ACL), Department of Health and Human Services (HHS), which was awarded to the Research and Training Canter on Community Living (RTCCL) at the University of Minnesota.
Editors-in-Charge: Meghan M. Burke and K. Charlie Lakin