
Abstract
Background:
Substance use during pregnancy threatens maternal and fetal health, and the COVID-19 pandemic may have altered patterns of use and disparities.
Methods:
We analyzed 2019–2021 Nationwide Emergency Department Sample data to examine emergency department visits among pregnant individuals with documented substance use (opioids, cannabis, alcohol, or nicotine). A difference-in-differences approach assessed pandemic-related changes and disparities by race/ethnicity and insurance status.
Results:
During the pandemic, odds of emergency department visits involving alcohol use increased by 16% (adjusted odds ratio [aOR] = 1.16, 95% confidence interval [CI] = 1.05–1.27) and cannabis use by 10% (aOR = 1.10, 95% CI = 1.01–1.20). Prepandemic, Native American individuals had markedly higher odds of opioid use, while African American individuals had higher odds of cannabis and nicotine use. Disparities in cannabis use narrowed for Hispanic and Native American individuals compared to White individuals. Uninsured and Medicaid-insured patients showed consistently elevated odds for opioid, cannabis, and nicotine use.
Conclusions:
The pandemic was associated with increased alcohol and cannabis use in pregnancy and shifting disparities across racial and insurance groups. Targeted public health strategies are needed to address substance use among pregnant individuals, especially during societal disruptions.
Introduction
Perinatal substance use is a critical public health issue in the United States, particularly among pregnant individuals. 1 The negative effects of substance use impact both the mother and the unborn child, often leading to serious complications. These include long-term neurological abnormalities and adverse perinatal outcomes such as miscarriage, preterm birth, and low birth weight.2,3
Commonly used substances include alcohol, tobacco, and cannabis, while opioids are less frequently reported.2,4 Substance use during pregnancy is particularly prevalent among individuals aged 15–44, with adolescents (defined here as age 18 or younger, consistent with our analytic framework) showing the highest percentages of illicit substance use. 4 Specifically, studies have found that 11.5% of adolescent and 8.7% of adult pregnant individuals reported alcohol use, while 23.0% of adolescents and 14.9% of adults reported tobacco use. 4 Additionally, 7.0% of pregnant individuals reported cannabis use, 5 and 5.9% reported other illicit drug use. 4 Of particular concern, teenage pregnant individuals have the highest percentage of illicit drug use at 20.9%, compared to 8.2% among young adult pregnant individuals (ages 18–25) and 2.2% among older adult individuals (ages 26–44). 6
The COVID-19 pandemic and associated containment measures have raised widespread concerns about their potential impact on alcohol and other substance use. 7 Physical distancing, job loss, and financial uncertainty contributed to increased psychological stress and social isolation. As a result, many individuals turned to substances such as alcohol and drugs to cope with depressive symptoms, loneliness, and health-related anxiety.2,7 Emerging studies confirm a rise in overall substance use since the onset of the pandemic, with marginalized populations disproportionately affected.
The COVID-19 pandemic has exacerbated substance use disorders (SUDs), including opioid use disorder (OUD), and has accelerated the use of alcohol and other substances among pregnant individuals. 8 The pandemic introduced unique challenges such as increased psychological distress, disruptions in prenatal care, and heightened anxiety, which have led many pregnant individuals to use substances more frequently as a coping mechanism.9,10 For instance, before the pandemic, approximately 9.8% of pregnant individuals reported alcohol use, a figure that saw a slight increase during the pandemic due to heightened stress and changes in daily routines. 11 Cannabis use among pregnant individuals, which had been rising from 3.4% in 2002 to 7.0% in 2017, continued to increase during the pandemic as a means to manage anxiety and stress. 5 This trend may also be influenced by the legalization of recreational cannabis in many states, which has been associated with increased use during the preconception and postpartum periods among individuals who gave birth. 12 Opioid use among pregnant individuals increased fourfold from 1999 to 2014, 13 and between 2017 and 2020, the rate of overdose deaths related to pregnancy rose by 81%. 14 In contrast, while 7.2% of individuals who gave birth smoked cigarettes in 2016, 15 by 2021, 5.4% of individuals with a recent live birth reported cigarette smoking during pregnancy. 16
The emergency department (ED) is a critical touchpoint for addressing substance use among pregnant individuals. Those who use substances often require substantial health care services and have more frequent ED visits compared to those who do not use substances. 17 Specifically, individuals who used opioids or tobacco throughout the antepartum period had more ED visits than individuals who did not use either substance. 17 Despite these insights, the prevalence of substance-related disorders in ED settings, particularly for specific substances such as opioids, cannabis, alcohol, and nicotine, remains understudied.
Additionally, research highlights that pregnant individuals seeking care in the ED often present with significant mental health concerns, including anxiety, stress-related disorders, and depression. 18 The socioeconomic challenges faced by these individuals, including higher rates of poverty and lower educational attainment, exacerbate these health issues and result in poorer obstetric and delivery outcomes. 19
Pregnant individuals are screened for substance use approximately 51–75% less often than nonpregnant individuals, underscoring a notable gap in care.20,21 Furthermore, research reveals significant racial and ethnic disparities in substance use screening and treatment among pregnant individuals in the ED. These disparities are more pronounced among individuals of color, with substance use documented in the medical records of 74% of Black individuals and 78% of Hispanic individuals, compared to only 60% of White individuals. 22 These data are based on self-reported race/ethnicity. Systematic biases exacerbate these inequalities, as health care providers are more likely to perform toxicology tests on Black and Hispanic pregnant individuals despite similar substance use rates across racial groups, leading to disproportionately higher rates of Child Protective Services involvement for Black mothers.23,24 These disparities extend to care delivery: Black patients with SUD experience 35% longer ED wait times than White patients, 25 and Black pregnant individuals have higher ED visit frequencies even after accounting for neighborhood social determinants of health and severe maternal morbidity risk. 26 The racial and ethnic disparities can also extend to maternal outcomes. 27
Last, health insurance status plays a critical role in health care utilization among pregnant individuals, with those on public insurance, such as Medicaid, experiencing distinct disparities. Research shows that Medicaid-insured pregnant individuals are more likely to undergo toxicology testing than those with private insurance. 24 Additionally, these individuals have significantly higher rates of nonmedical opioid use, with those in the second trimester being 6.5 times more likely to misuse opioids than their privately insured counterparts. 28 Medicaid-insured individuals also receive larger perioperative opioid quantities and face a higher risk of persistent opioid use and OUD. 29 Furthermore, while insured pregnant individuals generally show lower odds of alcohol use, this protective effect does not extend to tobacco use. 30
The pandemic has also transformed the delivery of health care services, with a shift toward virtual or telemedicine visits. This shift has presented both challenges and opportunities for pregnant individuals with SUDs, including reduced access to in-person medication and support services but increased flexibility and reduced no-show rates through hybrid care models. 8
Given the lack of national data on the impact of the COVID-19 pandemic on substance use-related ED visits among pregnant individuals, this study seeks to explore potential changes in disparities based on race/ethnicity and health insurance status in the use of opioids, cannabis, alcohol, and tobacco. By comparing ED visits of pregnant individuals before and during the pandemic, the findings aim to shed light on how the pandemic has influenced perinatal substance use patterns. These insights will contribute to shaping future public health policies and strategies to address substance use during pregnancy, including in responding to public health emergencies.
Methods
Data source and study population
The study used the Nationwide Emergency Department Sample (NEDS), the largest publicly available, all-payer U.S. ED dataset, developed as part of the Healthcare Care and Utilization Project by the Agency for Healthcare Research and Quality (AHRQ). It includes discharge information on approximately 25–30 million ED visits annually, representing a 20% stratified sample of all U.S. ED visits. This dataset includes weights that allow for national estimates to be used in the analyses. Our study utilized data from 2019 to 2021 (the most recent publicly available), covering a total of 2,311,280 ED visits, which corresponds to a weighted national estimate of 9,829,658 visits among pregnant individuals. Prior to use, we completed a data use agreement with the AHRQ. Due to the de-identified and publicly available nature of the data, the study was reviewed by the university’s institutional review board and determined to be exempt from full review. We focused on ED visits by pregnant individuals in which substance use (opioids, cannabis, alcohol, nicotine) was documented using International Classification of Diseases, 10th Edition (ICD-10) codes. 31 Importantly, these codes reflect the presence of substance use as part of the clinical record and do not necessarily indicate that the ED visit was caused by an acute issue related to substance use.
Measures and statistical analysis
This study analyzed four binary dependent variables related to substance use: opioids (ICD-10 codes F11.xx, 32 which include conditions such as opioid use, abuse, and dependence with associated complications such as intoxication, withdrawal, mood, and psychotic disorders, and remission), cannabis (F12.xx), 33 alcohol (F10.xx), 34 and nicotine (F17.xx). 35 All codes within each category were included regardless of subtype or severity. These ICD-10 codes were recorded as part of either the primary or any secondary diagnoses during the ED visit. However, it is important to note that these codes do not necessarily indicate that substance use was the chief complaint or reason for the ED visit. Rather, they reflect any documentation of substance use during intake or diagnostic coding.
The primary independent variable was the COVID-19 period, defined as April to December of 2020 and the full year of 2021. The pre-COVID-19 period included all of 2019 and January to March of 2020. March 2020 was excluded from the COVID-19 period to reduce misclassification bias, as the declaration of the pandemic occurred mid-month (March 11) and health care disruptions varied widely during this transition period across different states. Data from before 2019 were excluded due to the availability of race/ethnicity information starting in 2019. Covariates included: (1) Race/ethnicity: Race/ethnicity was captured using the NEDS-provided variable, which reports a single, mutually exclusive race/ethnicity category for each patient, based on hospital administrative data. Patients who may identify with more than one race/ethnicity are categorized under a single group, as defined by the reporting hospital. The categories included were: White (reference), African American, Hispanic, Asian and Pacific Islander, and Native American; (2) payer source/health insurance status: This status was based on the primary expected payer recorded for the ED visit, as provided in the NEDS dataset. Although some patients may have more than one form of coverage, NEDS includes only a single payer category per visit, representing the primary source expected to cover the largest portion of the bill. Categories used in our analysis included private insurance [reference group], Medicaid, uninsured/self-pay, and open-access care; (3) age groups: ≤18, 18–24, 25–34 (reference group), 35–44, and ≥45. Although our study uses ≤18 to define the youngest age group, we note that some prior literature (e.g., Stone, 2015 6 ) defines “teenage” more narrowly as ages 15–17, while other sources do not provide a specific age definition; (4) median income by ZIP code in quartiles: 0–25 percentile, 26–50 percentile, 51–75 percentile, and 76–100 percentile (reference group); (5) patient location: rural, nonrural (reference group), and (6) hospital region: Northeastern, Midwest, South, and Western (reference group).
The analysis was conducted in two steps. First, descriptive and chi-squared statistics were used to examine patient characteristics and patterns of substance use. Second, a difference-in-differences analysis assessed the impact of the COVID-19 period on ED visits, adjusting for year, patient, and hospital characteristics. Interaction effects between the COVID-19 period and key covariates (e.g., race/ethnicity, payer source) were analyzed to explore disparities. Adjusted odds ratios (aOR) were used to quantify these effects. All statistical analyses were performed using SAS 9.4 (SAS Institute Inc.), with a significant level set at p-values <0.05 (2-tailed).
Results
Before COVID-19 and during COVID-19, there were 5,956,371 and 3,873,287 ED visits, respectively (Table 1). The 25–34 age group constituted the highest proportion of ED visits, accounting for approximately 47%. During the study period, the proportion of ED visits remained relatively stable across racial/ethnic groups, with slight variations observed: White individuals (40.42–40.90%), Black individuals (25.49–26.27%), and Asian and Pacific Islander individuals (3.28–3.29%). The proportion of visits by Hispanic individuals changed from 25.35% to 24.13%, and by Native American individuals from 0.58% to 0.51% (Table 1). Medicaid emerged as the predominant payer source, covering 52.27% of ED visits before COVID-19 and 53.22% during COVID-19. Private insurance coverage decreased from 35.96% to 33.92%, while the proportion of uninsured individuals increased from 8.07% to 9.41%. Open-Access care also declined from 0.41% to 0.27% (Table 1). The lowest income quartile had the highest representation, increasing from 36.22% to 37.44% of ED visits (Table 1).
Behavioral Health-Related ED Visits Before and During COVID-19 Among Pregnant Women
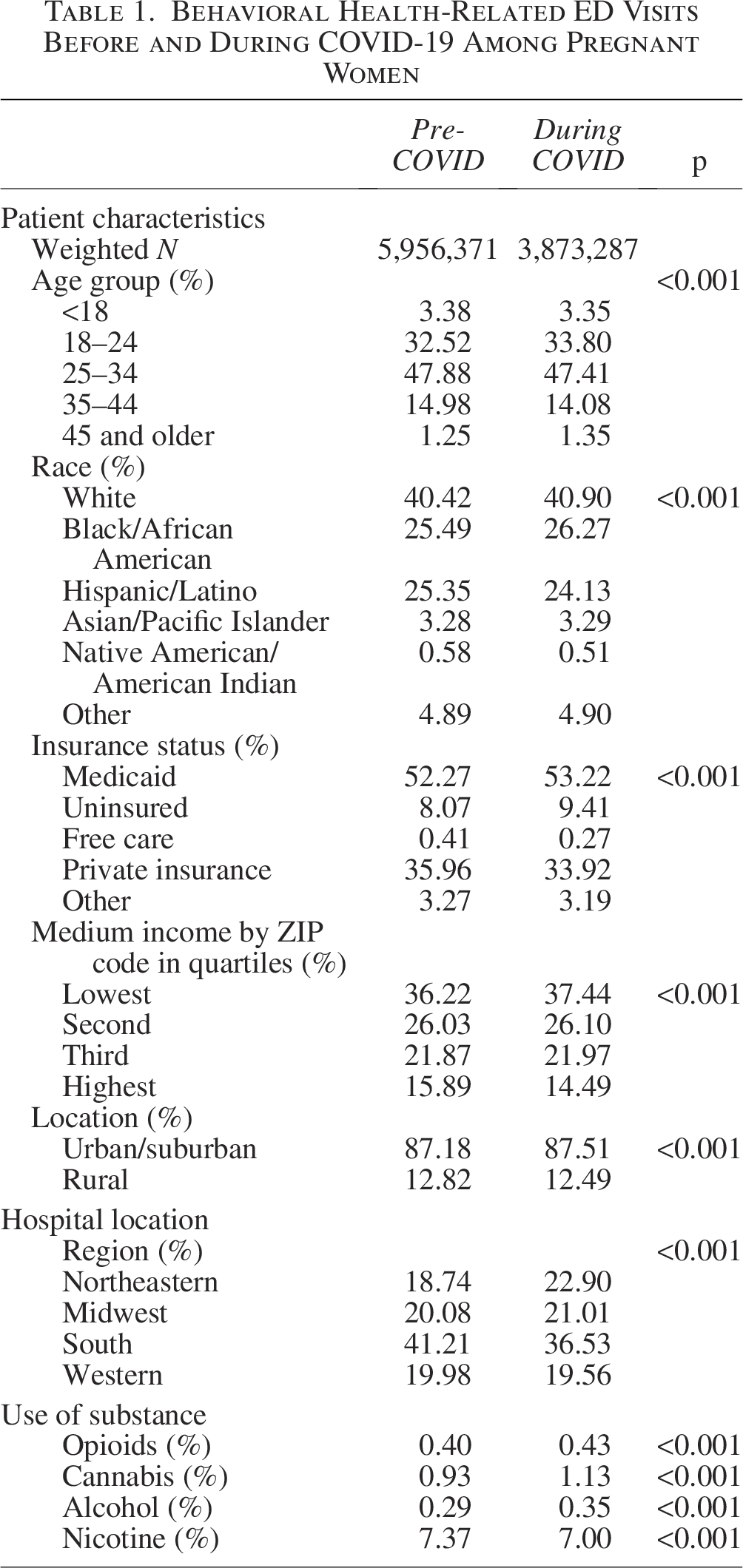
Similarly, ED visits from urban and suburban areas remained the highest, increasing slightly from 87.18% to 87.51% during the COVID-19 period (Table 1). The substance use patterns also shifted. The proportion of ED visits involving opioids rose from 0.40% to 0.43%, cannabis from 0.93% to 1.13%, and alcohol from 0.29% to 0.35%. Nicotine-related ED visits, however, declined from 7.37% to 7.00%. All these differences were statistically significant based on chi-squared tests (p < 0.001) (Table 1).
As shown in Table 2, during the COVID-19 period, the adjusted odds of ED visits with alcohol use were 16% higher (aOR = 1.16, 95% confidence interval [CI] = 1.05–1.27, p = 0.002), and 10% higher for cannabis use (aOR = 1.10, 95% CI = 1.01–1.20, p = 0.031) compared to pre-COVID-19. The increase in the odds of opioid-related visits was marginally significant (aOR = 1.10, 95% CI = 0.98–1.24, p = 0.099). Compared to White individuals, Hispanic pregnant individuals had lower odds of ED visits for opioid use (aOR = 0.56, 95% CI = 0.51–0.61, p < 0.001), cannabis use (aOR = 0.64, 95% CI = 0.60–0.67, p < 0.001), alcohol use (aOR = 0.64, 95% CI = 0.59–0.69, p < 0.001), and nicotine use (aOR = 0.45, 95% CI = 0.43–0.45, p < 0.001). Asian and Pacific Islander individuals also had lower odds across all four substances: opioids (aOR = 0.29, 95% CI = 0.22–0.37, p < 0.001), cannabis (aOR = 0.31, 95% CI = 0.26–0.36, p < 0.001), alcohol (aOR = 0.33, 95% CI = 0.26–0.41, p < 0.001), and nicotine (aOR = 0.51, 95% CI = 0.48–0.53, p < 0.001). African American pregnant individuals had lower odds of opioid-related ED visits (aOR = 0.50, 95% CI = 0.45–0.55, p < 0.001) but higher odds for cannabis (aOR = 1.71, 95% CI = 1.62–1.79, p < 0.001) and nicotine (aOR = 1.18, 95% CI = 1.15–1.19, p < 0.001) use (Table 2).
Racial and Health Insurance Disparities in Use of Opioids, Cannabis, Alcohol, and Nicotine Among Pregnant Women at Emergency Department Before and During COVID-19
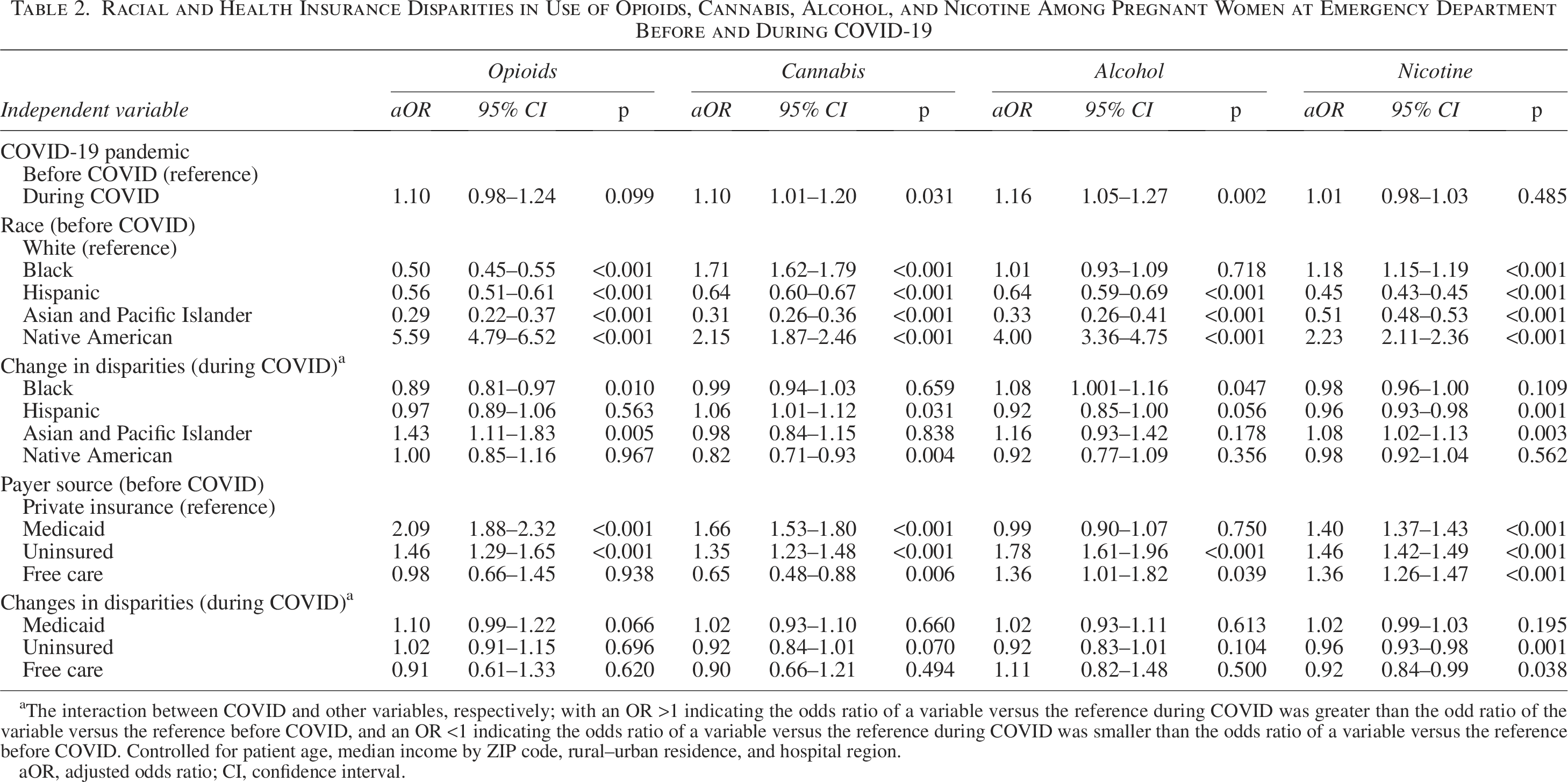
The interaction between COVID and other variables, respectively; with an OR >1 indicating the odds ratio of a variable versus the reference during COVID was greater than the odd ratio of the variable versus the reference before COVID, and an OR <1 indicating the odds ratio of a variable versus the reference during COVID was smaller than the odds ratio of a variable versus the reference before COVID. Controlled for patient age, median income by ZIP code, rural–urban residence, and hospital region.
aOR, adjusted odds ratio; CI, confidence interval.
Disparities in substance use-related ED visits among pregnant individuals shifted during the COVID-19 pandemic, as shown through interaction effects, with changes varying by substance type.
For opioid-related visits, the African American–White disparity widened, with an interaction aOR = 0.89 (95% CI = 0.81–0.97, p = 0.010), indicating a relative increase compared to the prepandemic aOR = 0.50 (95% CI = 0.45–0.55, p < 0.001). In contrast, the Asian and Pacific Islander–White disparity narrowed (interaction aOR = 1.43, 95% CI = 1.11–1.83, p = 0.005; pre-COVID aOR = 0.29, 95% CI = 0.22–0.37, p < 0.001).
For cannabis-related visits, disparities narrowed for Hispanic individuals (interaction aOR = 1.06, 95% CI = 1.01–1.12, p = 0.031; pre-COVID aOR = 0.64, 95% CI = 0.60–0.67, p < 0.001) and Native American individuals (interaction aOR = 0.82, 95% CI = 0.71–0.93, p = 0.004; pre-COVID aOR = 2.15, 95% CI = 1.87–2.46, p < 0.001), suggesting reduced differences compared to White individuals.
For nicotine-related visits, the disparity between Asian and Pacific Islander and White individuals narrowed (interaction aOR = 1.08, 95% CI = 1.02–1.13, p = 0.003; pre-COVID aOR = 0.51, 95% CI = 0.48–0.53, p < 0.001). Conversely, the disparity between Hispanic and White individuals slightly widened (interaction aOR = 0.96, 95% CI = 0.93–0.98, p = 0.001; pre-COVID aOR = 0.45, 95% CI = 0.43–0.45, p < 0.001). These patterns reflect how the pandemic influenced preexisting disparities in ED visits for substance use across racial and ethnic groups.
Compared to privately insured pregnant individuals, those who were uninsured had higher odds of ED visits in which substance use was documented, including opioids (aOR = 1.46, 95% CI = 1.29–1.65, p < 0.001), cannabis (aOR = 1.35, 95% CI = 1.23–1.48, p < 0.001), alcohol (aOR = 1.78, 95% CI = 1.61–1.96, p < 0.001), and nicotine (aOR = 1.46, 95% CI = 1.42–1.49, p < 0.001). Medicaid recipients also had elevated odds of ED visits involving opioid use (aOR = 2.09, 95% CI = 1.88–2.32, p < 0.001), cannabis use (aOR = 1.66, 95% CI = 1.53–1.80, p < 0.001), and nicotine use (aOR = 1.40, 95% CI = 1.37–1.43, p < 0.001). While the differences for opioid and cannabis use were substantial, the increase for nicotine use—though statistically significant—was more modest in magnitude. Open-Access care recipients had higher odds for alcohol-related visits (aOR = 1.36, 95% CI = 1.01–1.82, p = 0.039) and nicotine-related visits (aOR = 1.36, 95% CI = 1.26–1.47, p < 0.001), but lower odds for cannabis-related visits (aOR = 0.65, 95% CI = 0.48–0.88, p = 0.006). During COVID-19, disparities in nicotine use between uninsured and privately insured individuals narrowed (aOR = 0.96, 95% CI = 0.93–0.98, p = 0.001), down from a pre-COVID aOR of 1.46 (95% CI = 1.42–1.49, p < 0.001). Disparities in nicotine use between open-access care and privately insured individuals also narrowed (aOR = 0.92, 95% CI = 0.84–0.99, p = 0.038).
Discussion
This study adds to the existing body of research by highlighting the importance of understanding substance use among pregnant individuals who seek care in the ED, especially during major social disruptions such as the COVID-19 pandemic. By examining the use of various substances in this population, we demonstrate how socioeconomic disparities impact pregnancy health and how these disparities have been exacerbated during COVID-19. The increase in ED visits for pregnant individuals who use substances (opioids, cannabis, alcohol, and nicotine) during the COVID-19 pandemic compared to 2019 is similar to previous research.8,9,36 A scoping review conducted on pregnant individuals showed that COVID-19 represented a significant stressor for pregnant individuals. These findings align with broader evidence that the COVID-19 pandemic disproportionately affected pregnant individuals by disrupting health care access and intensifying mental health stressors. 8 In our study, the increased ED visits for substance use during this period likely reflect compounded stressors and barriers to timely care. 37
However, this study reveals a shift in racial disparities. Compared to White pregnant individuals, Hispanic and Asian Pacific Islander pregnant individuals had lower odds for all four substances. Notably, Native American and African American pregnant individuals were more likely to have ED visits in which substance use was documented during the COVID-19 pandemic. Previous research has identified racial and ethnic disparities in prenatal health and has related them to worsened mental health outcomes during the COVID-19 pandemic. 38 Several factors may explain the patterns we observed: systemic racism and historical discrimination have a profound impact on mental health outcomes for minority groups, particularly African Americans and Native Americans. Systemic racism is deeply embedded in societal structures, leading to widespread inequities that negatively affect mental health outcomes. 39 Research indicates that these populations are more likely to experience severe mental health challenges and have limited access to appropriate mental health resources, 40 which may, in turn, lead to increased substance use as a coping mechanism. 41 In contrast, among Asian populations, lower reported rates of substance use may reflect a combination of factors, including strong social stigma surrounding substance use, 42 underreporting due to shame or fear of social consequences, and disparities in access to culturally competent care. 43 Hispanic attitudes toward substance use can vary depending on factors such as country of origin, acculturation, and socioeconomic status. 44 Studies have shown that cultural norms and values significantly shape substance use behaviors, with different Hispanic subgroups exhibiting distinct coping mechanisms and usage rates. 45
Evidence has shown that the COVID-19 pandemic has disproportionately affected Native American communities compared to White communities. 46 Native Americans had three times as high rates of hospitalization and were approximately five times more likely to die from COVID-19 outcomes compared to White people. 46 Furthermore, Native Americans exceeded the general U.S. population suicide rates in 2020, further highlighting the high mental health burden. 46 Historical trauma, decreased social support, and stress from the COVID-19 pandemic may have contributed to increased substance use as a coping mechanism among this population. 46 Additionally, many Native American communities face geographical barriers such as remoteness, difficulty retaining clinicians, and limited health care access. These structural and contextual factors likely played a role in the observed increase in ED visits related to substance use during pregnancy. 47
The widening disparity in ED visits in which opioid use was documented between African American and White pregnant individuals is consistent with trends reported in previous studies.8,48 Evidence showed that COVID-19 increased the multisystemic hardships (such as access to health care, illness, social support, and racism), which disproportionately affected African American pregnant individuals. African American pregnant individuals have also historically faced barriers to treatment; for example, they are significantly less likely than White patients to receive medication therapy for OUD during pregnancy. 49 These challenges made it more difficult for them to receive timely health care, leading to increased ED visits related to substance use during the pandemic. 50 In addition to barriers to accessing mental health services, another possible explanation for the increased substance use-related ED visits among African American pregnant individuals is the inequitable distribution of life-saving medications such as naloxone, used to treat overdose episodes. Owing to structural racism, African American communities have historically been less likely to receive these medications, and the pandemic only worsened this disparity by reducing in-person health care visits and access to essential treatments, possibly contributing to the rise in ED visits for opioid use. 51
The disparity in ED visits with documented opioid use between Asian and Pacific Islander and White pregnant individuals narrowed during the pandemic. Direct evidence on opioid-related ED visits by race in pregnant individuals is limited. A single-center study of OUD in pregnant individuals at an Alabama hospital compared the year before COVID (March 2019–February 2020) to the first pandemic year (March 2020–February 2021). It found no significant change in the racial distribution of pregnant individuals with opioid-related acute care visits pre- versus post-COVID. 52 In other words, the proportion of White versus Asian and Pacific Islander (and other) patients remained similar, suggesting no major shift in that disparity within the study sample. This would contradict a narrowing gap if one was expected. However, the Alabama study’s sample had few Asian patients (being a single regional cohort), so it may not detect a true change if one occurred.
The disparity in ED visits with documented cannabis use between Hispanic and White pregnant individuals narrowed during the pandemic. No identified peer-reviewed study has directly examined ED visit rates for cannabis use in pregnancy by race/ethnicity before versus during COVID-19. One relevant data point comes from a large integrated health system in Northern California. Young-Wolff et al. analyzed prenatal cannabis use rates among pregnant individuals before and during the pandemic (using urine toxicology screens in an obstetric population). 53 They found that prenatal cannabis use increased significantly during COVID-19. 53 Importantly, the patient demographics did not shift substantially: there were “negligible differences in age or race and ethnicity in the two periods” studied. 53 In other words, the surge in cannabis use during the pandemic affected the population broadly, without a notable change in the racial/ethnic makeup of those testing positive. This implies that Hispanic and White pregnant individuals experienced a similar rise in cannabis use prevalence, leaving the disparity between them roughly unchanged (neither widened nor clearly narrowed) in that setting. This appears to be a gap in the literature.
The disparity in ED visits with documented cannabis use between Native American and White pregnant individuals also narrowed during the pandemic. We found no published studies that specifically evaluate ED visit disparities for cannabis use between Native American and White pregnant individuals during COVID-19. In fact, pregnancy-related substance use data for Native American populations are generally sparse in the literature, often due to smaller sample sizes. What we do know from broader data is that Native American communities have faced disproportionately high rates of substance use and related harms, which might lead one to expect a persistent or even widening gap rather than a narrowed one. For instance, a national study of pregnancy-associated overdose deaths in 2020–2021 found that Native American pregnant/postpartum individuals had the highest overdose mortality rates, higher than those of White individuals. 54 There is no direct research to support or refute our finding that the Native American–White disparity in cannabis-related ED visits narrowed in the COVID period. Given the lack of data, this must be viewed as a potential gap in the literature.
The disparity in ED visits with documented nicotine use between Hispanic and White pregnant individuals widened during the pandemic. We did not find any ED-based studies that directly examine smoking or nicotine-use visits in pregnant individuals by race during COVID-19. To infer what might have happened, we can look at overall prenatal smoking trends. National birth certificate data actually show that smoking during pregnancy declined for both White and Hispanic individuals from before the pandemic to 2020–2021. 55 Hispanic individuals continued to have far lower smoking rates than White individuals in the pandemic era. 55 This may support our finding of the widening of the disparity in ED visits with documented nicotine use between Hispanic and White pregnant individuals.
In contrast, the disparity in ED visits with documented nicotine use between Asian and Pacific Islander and White pregnant individuals narrowed during the pandemic. We did not find any pandemic-era study of ED visits related to nicotine use by race. Nonetheless, one study on pregnancy-related mortality in 2020–2021 did highlight that Pacific Islander individuals, along with Native American and African American individuals, had higher mortality rates than Whites. 54 That outcome suggests Pacific Islander pregnant individuals faced worse overall health impacts during the pandemic, which supports our finding of narrowing of disparities. However, this mortality figure is not specifically tied to smoking or ED visits.
The COVID-19 pandemic also significantly changed the pregnancy experience. Pregnant individuals experienced unique circumstances such as dealing with unknown effects of COVID-19 on the baby, limited visits, and restrictions on who could be present during labor and delivery (e.g., partners, doulas, or other support persons), among others. The combination of all these factors caused a detrimental effect on their mental health, increasing anxiety and depression. 50 Unfortunately, the structural and systemic inequities that have long impacted minority communities further limited the quality and availability of health care, prompting many to turn to substance use as a coping mechanism for mental health challenges.50,56
Compared to pregnant individuals with private insurance, those without insurance and those covered by Medicaid were more likely to have ED visits associated with tobacco, cannabis, and opioids. This finding is consistent with existing literature showing that lack of insurance and Medicaid coverage is associated with increased ED visits in the general population.57–59 Several socioeconomic factors tied to insurance status may help explain this disparity.
First, pregnant individuals with Medicaid or no insurance often face limited access to timely and consistent prenatal care, behavioral health services, and preventive interventions for SUDs.57,59,60 These barriers contribute to missed opportunities for early identification and treatment of SUDs, thereby increasing the likelihood of crisis-driven ED use. Medicaid does play an essential role in covering services for pregnant individuals with SUDs, and it is the primary payer for behavioral health services, including substance use treatment. However, access to high-quality, integrated care is not always consistent across states or providers, and workforce shortages and stigma may further limit service delivery. 60
For example, evidence has shown that uninsured patients and patients with public health insurance have more cannabis-associated ED visits compared to patients with private insurance. 59 Uninsured individuals may delay or forego routine care due to cost, leading to higher reliance on emergency care when health conditions, including substance use complications, become acute. 59 Conversely, pregnant individuals with private insurance may be less likely to visit the ED due to better access to universal health care services, including early screening and outpatient treatment for SUDs.
In addition, structural inequities such as poverty, housing instability, and limited social support systems are more prevalent among Medicaid and uninsured populations. These upstream determinants of health further increased the risk of substance use and may hinder treatment-seeking during pregnancy. For instance, data show that pregnant overdose decedents are more likely to be noncollege graduates, unmarried, and living in socioeconomically disadvantaged communities, compared to obstetric decedents. 61 Many of these deaths occur outside of health care settings, highlighting missed opportunities for prevention and engagement.
Given the disparities identified in substance use-related ED visits among pregnant individuals, particularly across racial/ethnic groups and insurance status, targeted evidence-based interventions must be tailored to address the unique needs of these populations at the individual, health care, community, state, and national levels. These should include expanding Medicaid benefits to cover comprehensive behavioral health and SUD treatment, improving care coordination, and addressing social determinants of health such as transportation and housing. These should include culturally competent and non-punitive strategies that actively reduce barriers to care and encourage pregnant individuals to seek and remain in treatment for substance use. 61
Limitations
This study had several NEDS-related limitations. First, it would have been beneficial to analyze data from a more extended timeframe to understand the broader effects of COVID-19; the study was constrained by the availability of only the 2020 and 2021 NEDS datasets. Consequently, the analysis could only capture the immediate short-term impact of COVID-19 on ED visits among pregnant individuals who use substances. Therefore, the study’s findings may not fully represent the long-term trends and effects of the pandemic. Second, NEDS lacks detailed clinical information typically available in electronic health records. As a result, it is not possible to distinguish between visits related to overdose, withdrawal, or treatment for SUDs, limiting clinical specificity in interpreting substance use-related diagnoses. In addition, since NEDS is discharge-based, it does not facilitate tracking patients for multiple ED visits, limiting the ability to analyze longitudinal trends. Third, pregnancy was identified using ICD-10 diagnosis codes associated with pregnancy-related conditions, and the analysis was restricted to patients coded as biologically female. NEDS does not include variables related to gender identity or sex assigned at birth, which limits our ability to identify transgender or nonbinary individuals who may have been pregnant during their ED visit. This reflects a broader gap in administrative data systems and highlights the need for inclusive demographic measures in large-scale health datasets. Despite these limitations, this study is the first to provide a national perspective using a difference-in-differences analytical approach, offering comprehensive insight into changes in sociocultural disparities in substance use among pregnant individuals in the ED setting following the onset of the COVID-19 pandemic.
Conclusion
Our study revealed an increased risk of ED visits associated with the use of opioids, cannabis, alcohol, or nicotine among pregnant individuals in the United States during the COVID-19 pandemic. Racial and ethnic disparities shifted during this period, with gaps in substance use between Native American and White pregnant individuals widening in 2021, while disparities between Hispanic, Asian, and Pacific Islander pregnant individuals and their White counterparts narrowed. Additionally, African American pregnant individuals were less likely to have opioid-related ED visits but were more likely to have cannabis- and tobacco-related ED visits. Uninsured pregnant individuals who use substances were also more likely to visit the ED during the pandemic, underscoring the role of insurance status in accessing non-ED care.
Health disparities related to substance use during pregnancy present significant challenges in accessing prenatal care, maternal health outcomes, and mental health support. Pregnant individuals who use substances face stigma, judgment, and limited resources, which hinder timely access to care and lead to adverse perinatal outcomes. These disparities disproportionately affect marginalized groups, exacerbating existing maternal health inequities. Disproportionate use of the ED underscores health care access disparities. Research gaps remain in understanding the intersection of substance use, pregnancy, and maternal health, necessitating further investigation. While variable selection methods yield models with fewer variables, they have limitations and may not be generalizable. Future studies should explore factors and policies related to substance use-associated ED visits among pregnant individuals over the long term to inform policy and intervention strategies aimed at mitigating adverse effects, particularly during public health crises such as COVID-19.
Authors’ Contributions
Concept and design: A.D.G.-A. and J.J.S. Acquisition, analysis, or interpretation of data: S.K. and J.J.S. Drafting of the article: A.D.G.-A., S.K., L.H., A.G.O.-A., and J.J.S. Critical review of the article for important intellectual content: Y.G., J.V., and J.J.S. Supervision: J.J.S.
Footnotes
Author Disclosure Statement
The authors declare they have no financial ties to any organizations with potential interest in this work, either currently or within the past 3 years. The authors confirm there are no other relationships or activities that could have influenced this work. All participants in this study provided consent, either explicitly or through a waiver.
Funding Information
The authors state that no financial support was received from any organization for this work.