
Abstract
Introduction:
Preconception care is individualized health care designed to optimize health prior to pregnancy to reduce future pregnancy complications. Promoting preconception care for preventing pregnancy-related illnesses and death is needed, especially for those who are at highest risk. This study evaluated reception of preconception care among U.S. Black women of reproductive age.
Methods:
This study used Pregnancy Risk Assessment Monitoring System data from 2016 to 2021 with a sample of Black women across 44 states, the District of Columbia, New York City, and Puerto Rico who intended to become pregnant (n = 16,071). Multivariate logistic regression models evaluated the association between prepregnancy hypertension and preconception care reception.
Results:
Hypertensive Black women had 21% decreased odds (odds ratio [OR]: 0.79, confidence interval: 0.72–0.87) of receiving preconception care, compared with their counterparts without prepregnancy hypertension. An inverse dose–response was observed: As education and household income increased, the odds of receiving preconception care services decreased significantly (education: (OR: 1.39–0.64; income: OR: 0.74–0.30).
Conclusions:
These findings affirm that hypertensive Black women had lower odds of receiving preconception care services compared with Black women who did not begin pregnancy with hypertension. Given that women with chronic conditions would have more reasons to receive care prior to pregnancy, this finding is disconcerting.
Beginning pregnancy with uncontrolled chronic illnesses such as hypertension increases the risk for adverse health conditions 1 ; however, preconception care provides an opportunity to establish and maintain control of the condition prior to pregnancy. Preconception care is individualized health care designed to optimize health prior to pregnancy. 2 Composed of three categories of care (risk assessment, health promotion, and intervention), preconception care reduces the potential of pregnancy complications and adverse birthing experiences by addressing health concerns through provider counseling, chronic disease screenings, and treatment before pregnancy. 2,3
Preconception care reduces maternal mortality and improves birth outcomes by optimizing health and increasing awareness and therefore improving health decision-making, 4 –6 but receipt is low. 2,7 –9 In 2010, the reception of preconception care among women in the United States was low, with 14% of women reportedly receiving care by family physicians and OB-GYNs prior to pregnancy. 10 However, between 2016 and 2018, 27% of hypertensive women reported having received provider counseling on improving their health prior to pregnancy. 9
The literature investigating how Black women receive preconception care services (PCSs) is scant, even though Black women have the highest rates of maternal mortality and severe maternal morbidity in the United States. 11 The Maternal Mortality Review Committee, which annually evaluates the causes of maternal mortality in the United States, reconfirmed that pregnancy-related death is 83.5% preventable. 11,12 Therefore, the use of PCSs can ameliorate health prior to pregnancy to mitigate the potential occurrence of maternal morbidity or mortality. The reception of preconception care is important for Black women who have a rate of pregnancy-related death of 50.3 deaths per 100,000 live births, which is 3.5 times more than White women, 4.0 times more than Hispanic women, and 4.8 times more than Asian women in 2023. 13
As a source of guidance and standards of care for providers, the American College of Obstetricians and Gynecologists (ACOG) and the American Society of Reproductive Medicine recommend some level of preconception care for all women at reproductive years, beginning with the question “Would you like to become pregnant in the next year?” to assess the reproductive health goals and current health. 14 Assessing these predictors of positive pregnancy outcomes allows providers to focus on areas of health that may need improvement before conception occurs. Interventions focused on chronic disease management involve reviewing the use of teratogenic medications and ensure the management of the chronic disease is in line with the woman’s reproductive health plan. 15 Additionally, providers are expected to provide counseling to women with prepregnancy hypertension on the risks of pregnancy-related hypertensive disorders (preeclampsia, severe hypertension, and secondary hypertension) and to prioritize routine testing that assesses complete blood count, serum creatine level, hepatic transaminase levels, and urine collection to test protein levels. 16 Black women experience higher maternal mortality 13,17 –20 and other adverse pregnancy outcomes. Assuring high levels of preconception care for Black women can help improve their pregnancy outcomes and reduce these disparities.
Risks of hypertension before/during pregnancy
Prepregnancy hypertension increases the risk of developing pregnancy-related hypertensive disorders, 1 which remain the leading cause of severe maternal morbidity and mortality among Black women in the United States. 11,12 Conditions such as gestational hypertension; preeclampsia; hemolysis, elevated liver enzymes, and low platelet syndrome; and eclampsia disproportionately affect Black women. 21
The heightened risk of hypertension for this population is not isolated to a single source. The high prevalence of hypertension among Black women of reproductive age, hypertensive disorders in pregnancy, and cardiovascular disease are known to be multicausal. 1,22 The cumulative impact of negative social and environmental factors, beginning early in the lifespan of a Black woman, prompt high biopsychological stress, which leads to chronic illnesses, such as hypertension and cardiovascular disease. 23,24 The impact of weathering through lower socioeconomic factors consequentially alters gene expression in Black women, epigenetics, 25 which results in accelerated aging that increases the likelihood of adverse health conditions. 26 In an investigation of inpatient hospital childbirth deliveries between 2016 and 2018, Black women represented 14% of the deliveries but represented 37% of all deliveries with pregnancy-related hypertensive disorders, namely, gestational hypertension (17%) and preeclampsia/eclampsia (20%). 27 Research has confirmed that receiving counseling and a treatment plan for controlling hypertension prior to pregnancy positively alters the trajectory for adverse conditions. 28 –30
Barriers to coverage
The effects of the social determinants of health are a known factor in how or if Black women receive health care of any kind. 31 –34 The accessibility to preconception care not only is affected due to socioeconomic factors that originate upstream but also by the impact of negative provider interactions and the lack of patient-centered care that are the result of implicit bias. 21 Individual health care decision-making, which occurs downstream, is preceded by having the knowledge of how a particular health choice will impact one’s overall health. An adequate level of health knowledge 35,36 and health literacy 37 –39 makes the distinction between being a self-advocate for pertinent care during critical periods of the lifespan, like preconception, and the allowance of uncontrolled health conditions placing one on the path of adverse maternal health outcomes.
Significance
As the national rates of maternal mortality are beginning to decrease, unfortunately, the rate of pregnancy-related death is still disproportionately high for Black women in the United States. 40 The research on the reception of preconception care among Black women and the types of services received during the preconception care period is missing in the current research literature. This is the first study that investigates the preconception care received among Black women preparing for pregnancy and Black women who are preparing for pregnancy with hypertension. Our study aims to close the current research gap by investigating how Black women receive preconception care, what types of services they receive, their provider interactions during these clinical visits, and if a hypertension diagnosis improves their receipt of preconception care. The findings from this study provide a basis for future research in preconception care and the provider administration of care for those who are preparing for pregnancy with and without a hypertension diagnosis.
Objective
This study describes the receipt of preconception care experienced by Black women intending to become pregnant. We then compare the services received by the subset reporting a hypertension diagnosis to those without to determine if these higher-risk women were receiving preconception care at higher levels.
Methods
This cross-sectional secondary data analysis utilized Pregnancy Risk Assessment Monitoring System (PRAMS) data from 2016 to 2021. PRAMS, a preventive monitoring and surveillance system, is administered by the Centers for Disease Control and Prevention (CDC). Historically, women 41 across 47 states, District of Columbia, Puerto Rico, and tribal lands are sampled for the intended purpose of the collection of maternal health behaviors, preconception, prenatal, and postpartum experiences. 42 State live birth certificate data are used as the sampling frame to recruit women 2–6 months after giving birth to participate in the self-administered questionnaire or the telephone survey. Internal review board was not required for this study due to the use of a publicly available deidentified secondary dataset.
Participants and procedures
The 2016–2021 PRAMS dataset used in the present study included 242,573 women residing in 44 states, District of Columbia, New York City, and Puerto Rico. Consistent with our research objective, this analysis only included Black women (leaving 49,689 women who self-identified as Black), 18 years old and older, and intending to become pregnant. Our initial analytic sample, therefore, was 19,137.
The analysis included several covariates of interest that were analyzed for potential confounding based on the current literature related to receiving preconception care: marital status, educational status, method of payment, maternal age, and household income. Excluding respondents missing those items reduced the analytic sample to 16,182. A total of 2,955 unknown, blank, and not recorded responses (married n = 12, maternal education = 152, payment method = 92, maternal age = 1, household income = 2,357, and the year of birth = 341) were also excluded from the analysis. Unknown responses for the exposure variable indicating responses self-reported diagnosis of hypertension 3 months prior to pregnancy (n = 150) and unknown responses for hypertension diagnosed prior to pregnancy (n = 13) were removed from the analysis. Finally, unknown responses answering whether the outcome variable of PCSs were received (n = 154) were removed from the analysis. Thus, data for 16,071 women were available for the final analysis.
Measures
The primary exposure variable is the self-reported diagnosis of prepregnancy hypertension, a composite variable developed by combining the prepregnancy hypertension variable from the birth certificate worksheet and the PRAMS questionnaire self-report of hypertension responses to the question: “During the 3 months before you got pregnant with your new baby, did you have high blood pressure/hypertension?”. “Yes” demonstrates that the woman was positively diagnosed with hypertension prior to pregnancy, and “No” indicates hypertension was not diagnosed prior to pregnancy. Prehypertension was indicated if either response was “Yes.”
The outcome variable is the reception of preconception care visits, which offered response options as Yes or No, to the following question: “In the 12 months before you got pregnant with your new baby, did you have any health care visits with a doctor, nurse, or other health care worker, including a dental or mental health worker?” Secondarily, the type of PCS was also a part of the overall descriptive analysis. The PRAMS question “What type of health care visit did you have in the 12 months before you got pregnant with your baby?” offered seven PCSs items and an open text for individuals to respond specifically about their health care visit. In addition, the analysis also assessed 11 items related to preconception care counseling, which asks, “During any of your health care visits in the 12 months before you got pregnant, did a doctor, nurse, or other health care worker do any of the following things?” with response options as Yes or No.
Analytic approach
Along with examining the frequency of PCS reception and types of services received by all Black women, we utilized logistic regression to assess how receipt of PSC differed by hypertension status We use a backward elimination approach, including only variables with significance at the p < 0.20 level in the final model. 43 Bivariate analysis explored relationships between each covariate and the outcome variable. Referent categories in the logistic analyses were selected based on convention. For the within-states comparison, Michigan was selected as the referent, as it had the largest number of observations and would yield the most stable estimates. All analyses were conducted using SAS version 9.4.
Results
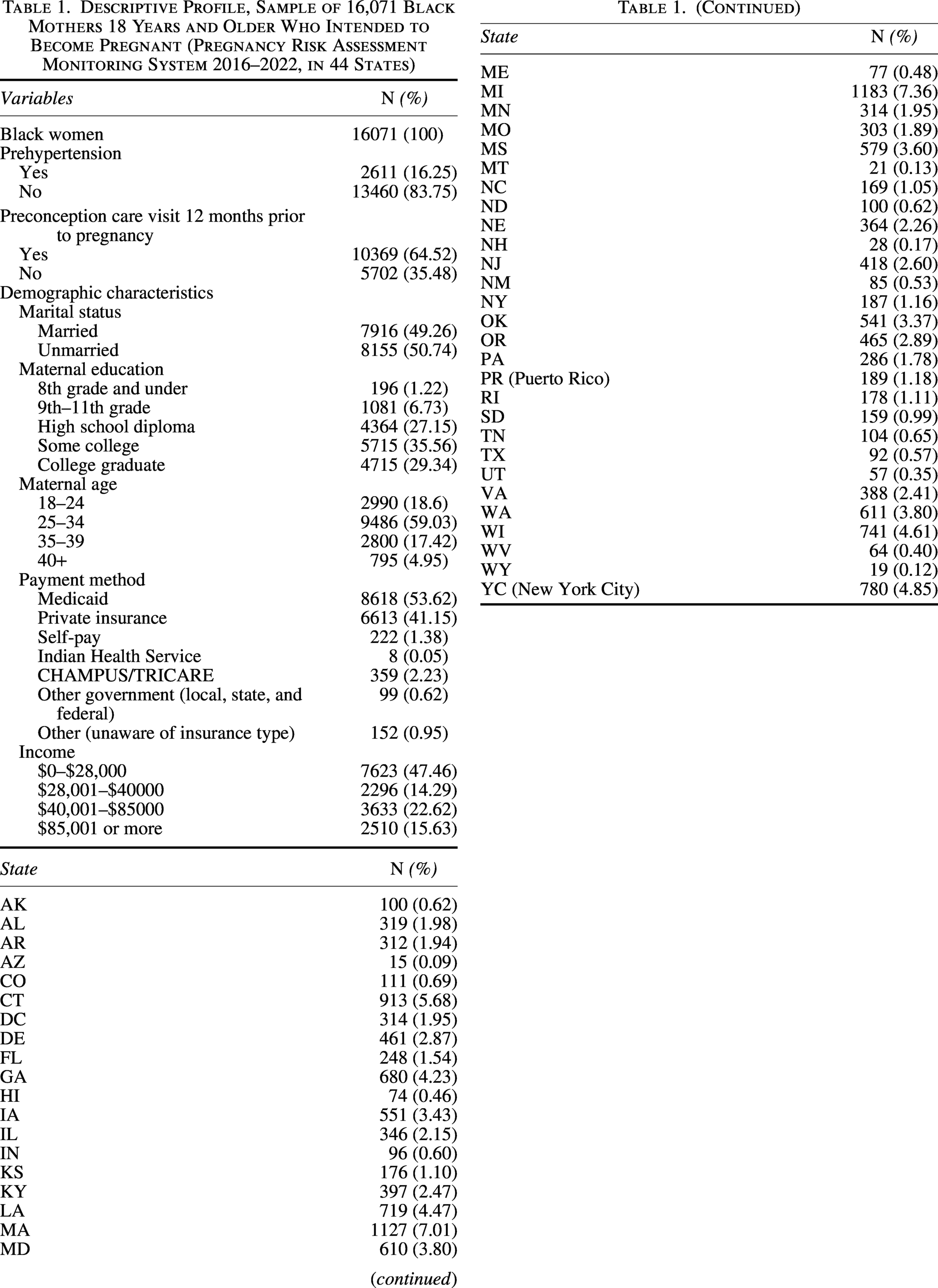
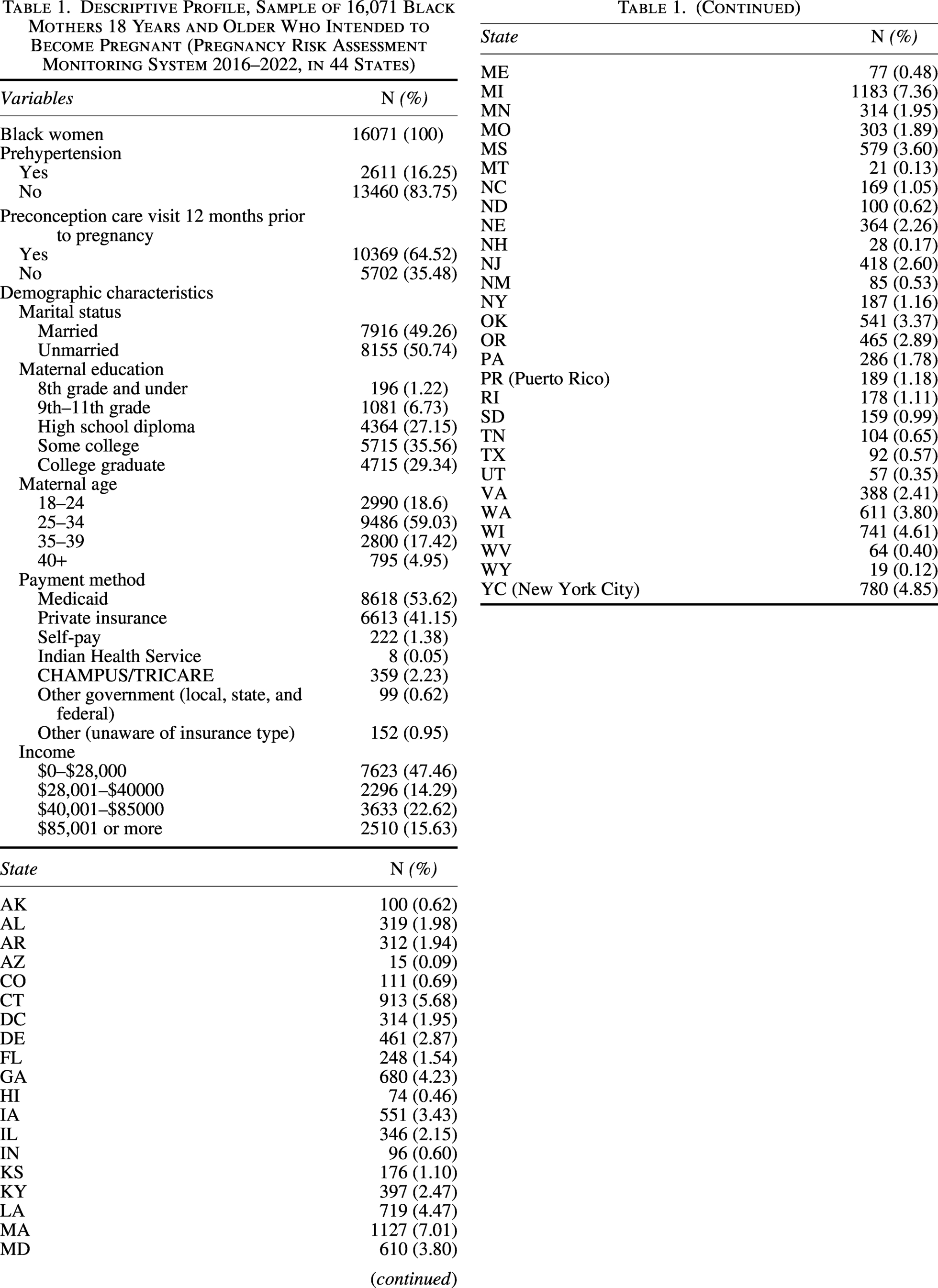
Of the final sample of Black women intending to become pregnant (16,071), 16.3% reported a hypertension diagnosis (Table 1). Among the sample, 64.5% of women self-reported having had a preconception care visit within the 12 months prior to their pregnancy.
Descriptive Profile, Sample of 16,071 Black Mothers 18 Years and Older Who Intended to Become Pregnant (Pregnancy Risk Assessment Monitoring System 2016–2022, in 44 States)
Preconception care services
The PCS most reported among all women, both those with and without hypertension, as received 12 months prior to pregnancy were regular checkups with a family doctor (65.1%) and OB-GYN (66.7%) and dentist visits to receive a routine dental cleaning (58%). Only 14% of all women, however, reported visits for chronic illness or chronic condition, such as hypertension. Similarly, visits to discuss family planning and birth control (20.59%) and depression and anxiety (10.27%) were infrequently reported as occurring in the months before conception occurred (Table 2).
Frequency Counts of Types of Preconception Care Health Visits Reported by Black Women 18 Years and Older Who Intended to Become Pregnant (All and the Subset with Prepregnancy Hypertension) in the United States, 2016–2021
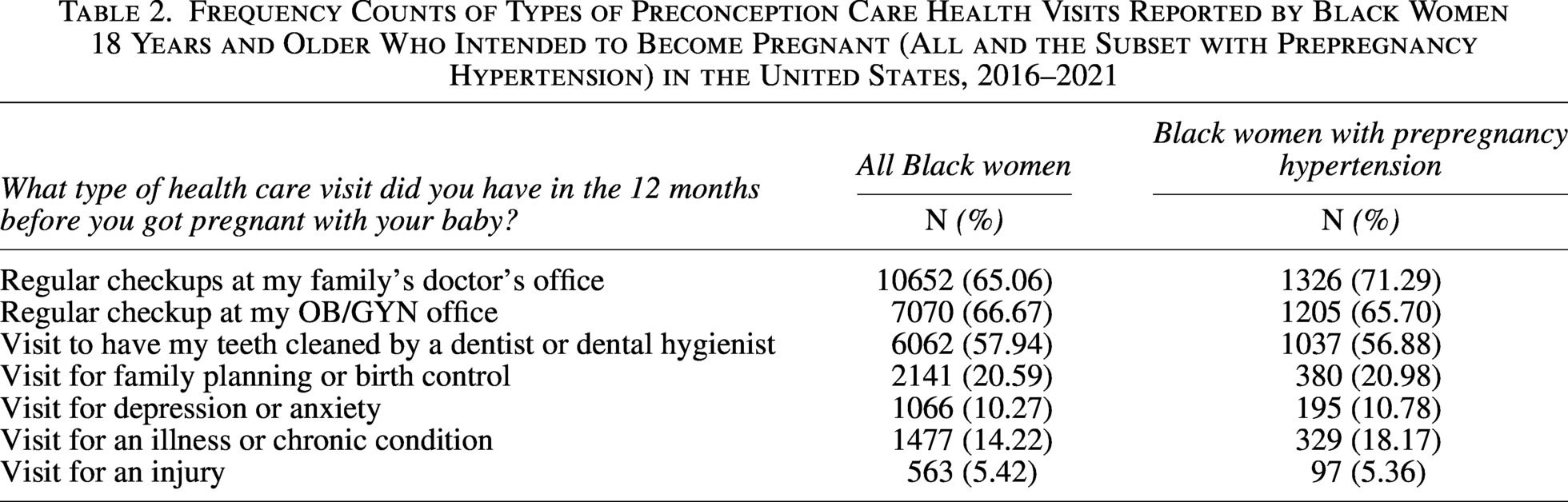
Women who began pregnancy with hypertension reported receiving regular checkups with their family doctor (71.3%) and OB-GYN (65.7%) 12 months prior to pregnancy. However, only 21% of those with prepregancy hypertension indicated receiving counseling related to family planning, and only 18% reported having a health visit specifically related to their chronic illness.
Provider interactions
Among all women reporting a visit 12 months before pregnancy, provider counseling regarding family planning (48.55%) did not occur nor did a discussion on how they could improve health before pregnancy (41.62%). Women also reported that no discussion on folic acid intake (36.78%) and controlling chronic conditions such as diabetes and hypertension (23.53%) occurred. In contrast, providers did ask women if they smoked cigarettes (77.84%), if they were experiencing interpersonal violence (58.95%), if they were feeling down or depressed (60.22%), and about their occupation (67.31%) (Table 3).
Frequency Counts of Provider Interactions Reported by Black Women 18 Years and Older Who Intended to Become Pregnant (All and the Subset with Prepregnancy Hypertension During Visits 12 Months Prior to Pregnancy Among Black Women (2016–2021)
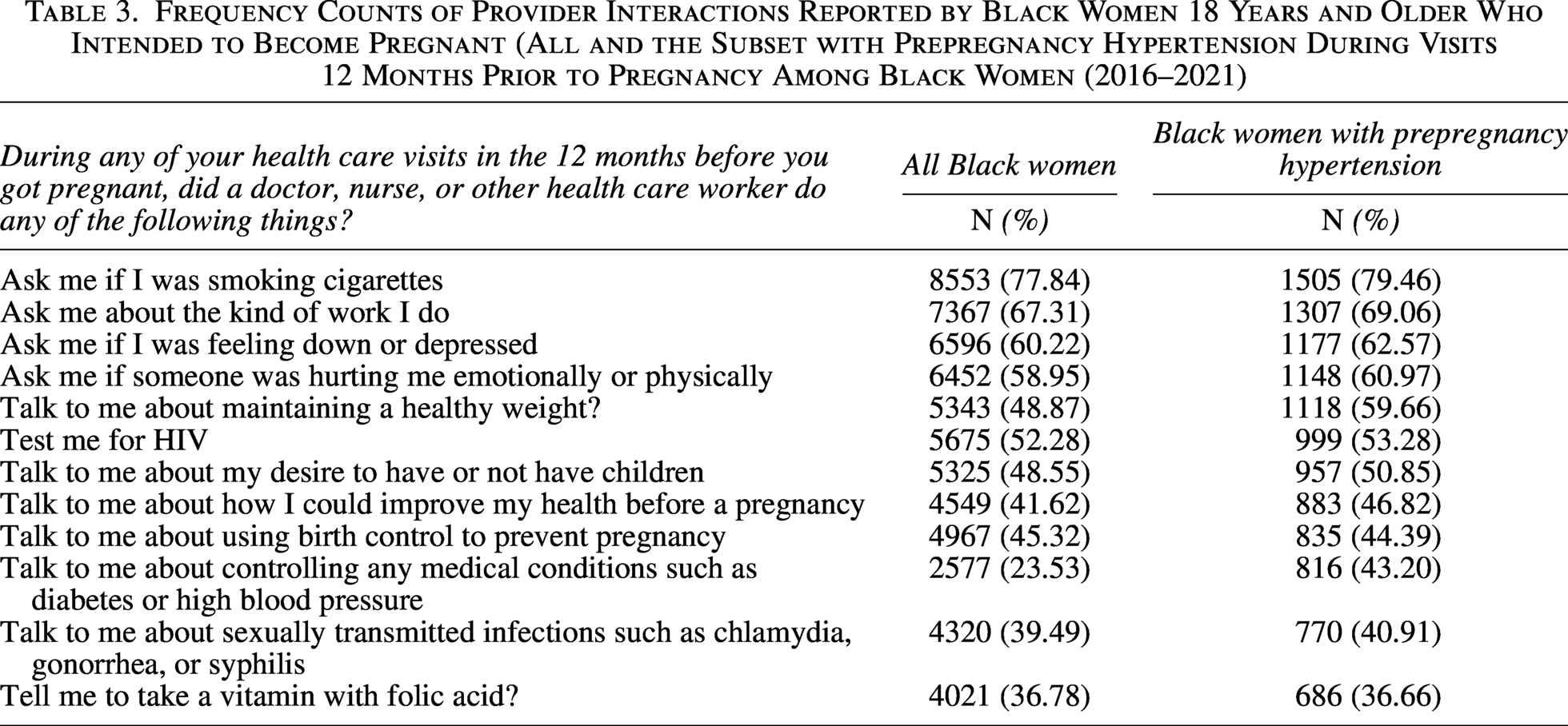
Hypertensive women similarly reported that their providers discussed folic acid intake (36.66%), controlling their chronic condition such as hypertension or diabetes (43.20%), or what would be needed to improve their current health status before pregnancy (46.82%). However, providers asked questions about their cigarette use (79.46%), experience with interpersonal violence (60.97%), feelings of depression (62.57%), and their occupation type (69.06%) at a higher frequency (Table 3).
Covariate analysis
Prior to adjustment, prepregnancy hypertensive women had 22% decreased odds (odds ratio [OR]: 0.78, confidence interval [CI]: 0.71–0.85) of receiving PCS compared with women who did not begin pregnancy with hypertension. Women who had some level of college education (OR: 0.64, CI: 0.58–0.69) or were college graduates (OR: 0.32, CI: 0.29–0.35) had significantly decreased odds of 37% and 68%, respectively, of receiving PCSs compared with high school graduates (Table 4).
Unadjusted and Adjusted Odds Ratio of Black Women 18 Years and Older Who Intended to Become Pregnant Receiving Preconception Care Services by Hypertension Status
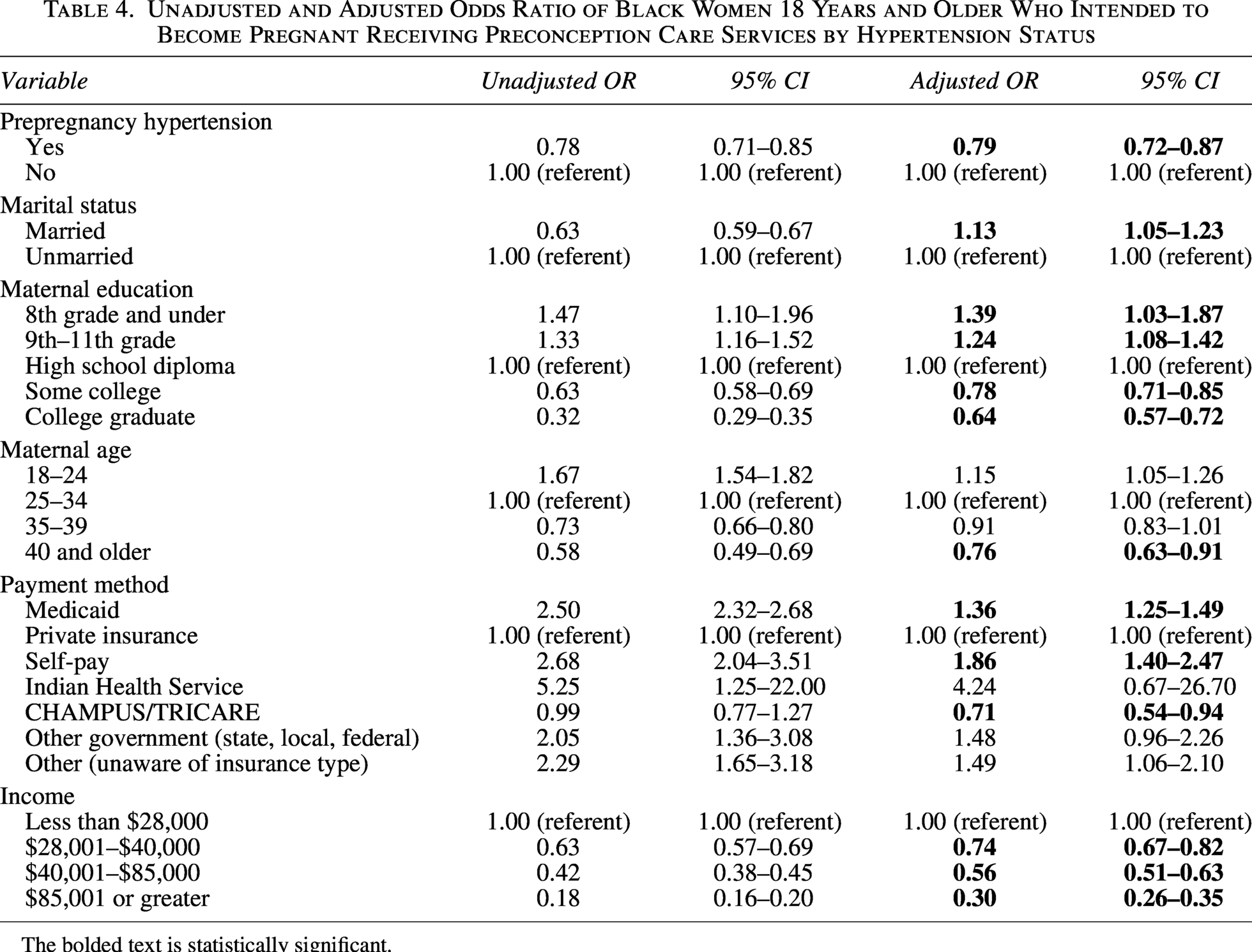
The bolded text is statistically significant.
An inverse dose–response relationship between age and receipt of PCSs was observed: Women 18–25 years old had 67% increased odds, and women 40 years and older had 42% decreased odds as compared with the 25–34 year-old referent group. Women who used payment methods such as Medicaid, self-payments, and other government forms of payment had increased odds of receiving PCSs compared with women who used private insurance (Table 4).
After controlling for age, education, payment method, marital status, state of birth, and income, the association between women with prepregnancy hypertension and their reception of PCSs improved slightly but maintained statistical significance. These women had 21% lower odds (OR: 0.79, CI: 0.72–0.87) of having had a visit with a provider 12 months prior to pregnancy, compared with their counterparts who did not have diagnosed hypertension prior to pregnancy.
In the adjusted model, the significant and unexpected inverse dose–response relationships persisted between educational attainment and household income and receiving PCSs. As Black women obtained more education, their odds of receiving PCSs decreased; 8th grade and under: (OR: 1.13, CI: 1.05–1.23), 9th–11th grade: (OR: 1.24, CI: 1.08–1.42), some college: (OR: 0.78, CI: 0.71–0.85), and college graduate: (OR: 0.64, CI: 0.57–0.72). As household income increased for Black women, their odds of receiving PCSs 12 months prior to becoming pregnant decreased: $28 K–$40 K (OR: 0.74, CI: 0.67–0.82), $40,001–$85 K (OR: 0.56, CI: 0.51–0.63), and $85 K and greater (OR: 0.30, CI: 0.26–0.35). Black women who used CHAMPUS/TRICARE to pay for their medical treatments had 28.7% lower odds (OR: 0.71, CI: 0.54–0.94) of receiving PCSs in comparison to women with private insurance. However, compared with other forms of payment, the military-based insurance plan was the only plan with decreased odds of receiving care prior to pregnancy (Table 4).
State findings
The state of Michigan was the largest group with 7.36%, including the final analysis; therefore, using Michigan as a referent, Black women residing in Montana (OR: 0.16, CI: 0.04–0.74), Illinois (OR: 0.51, CI: 0.38–0.67), Minnesota (OR: 0.56, CI: 0.42–0.76), New York (OR: 0.58, CI: 0.41–0.84), Wisconsin (OR: 0.58, CI: 0.47–0.71), Puerto Rico (OR: 0.64, CI: 0.46–0.89), Rhode Island (OR: 0.61, CI: 0.42–0.87), Louisiana (OR: 0.72, CI: 0.59–0.88), District of Columbia (OR: 0.72, CI: 0.54–0.95), Delaware (OR: 0.72, CI: 0.56–0.92), and Connecticut (OR: 0.73, CI: 0.60–0.88) had decreased odds of receiving PCSs. Increased odds of 32% for preconception care reception were observed for women of Washington (OR: 1.32, CI: 1.07–1.64), 41% for Kansas women (OR: 1.41, CI: 1.01–1.99), 44% for South Dakota women (OR: 1.44, CI: 1.01–2.04), 68% increased odds were observed for women of Georgia (OR: 1.68, CI: 1.37–2.05), and women of North Dakota had a 223% increased odds of receiving PCSs (OR: 2.23, CI: 1.44–3.44) in comparison to women of Michigan (Table 5).
Unadjusted and Adjusted Odds Ratio of Black Women 18 Years and Older Who Intended to Become Pregnant Receiving Preconception Care Services by the U.S. State and Prepregnancy Hypertension Status
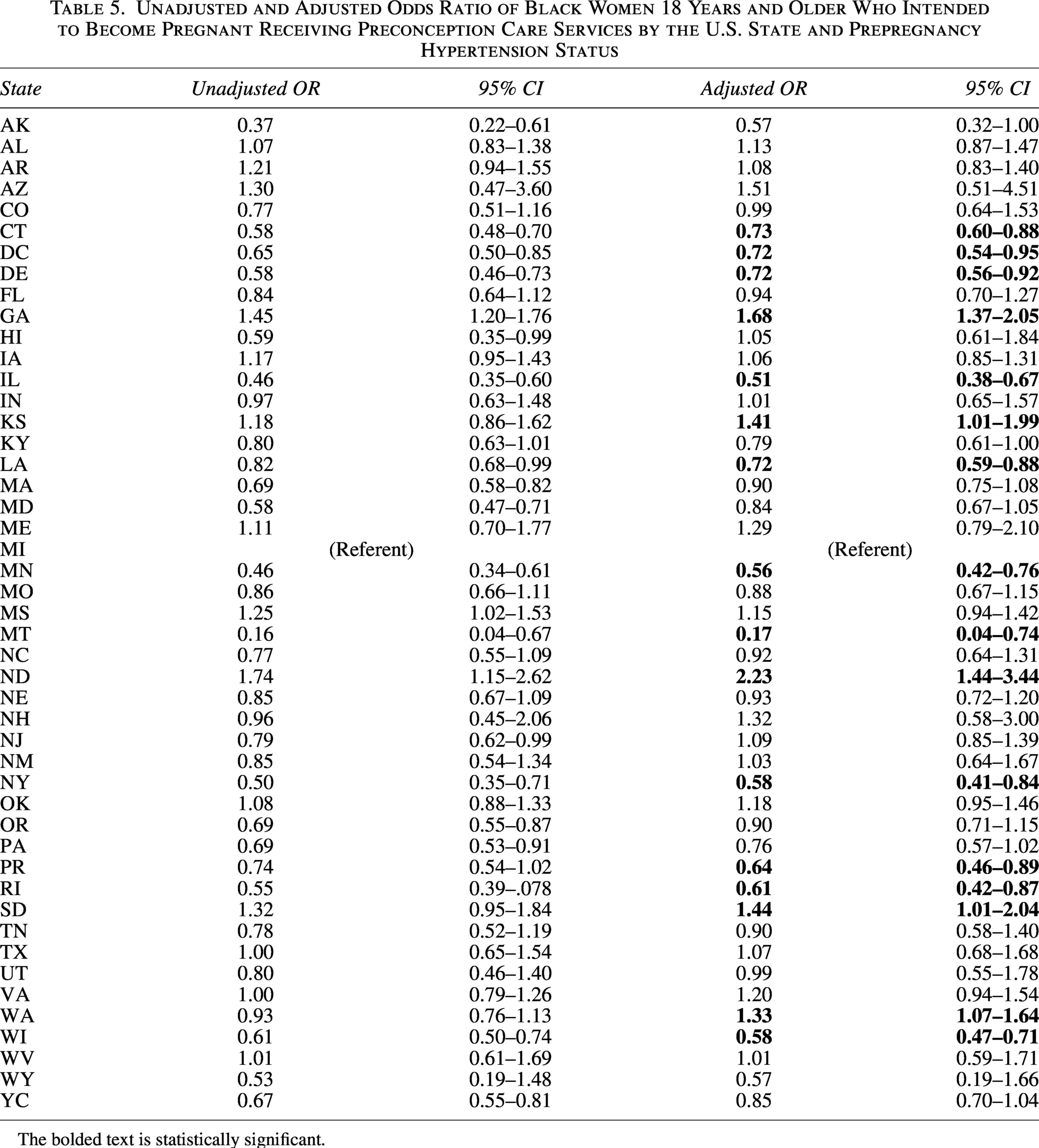
The bolded text is statistically significant.
Discussion
In 2019, Black women of reproductive age in the United States had the highest prevalence of hypertension (22.3%) among women diagnosed with hypertension. 44 In our study, approximately two-thirds of Black women received PCSs in the form of family doctor and OB-GYN office visits over the course of the research period in this study. Black women who began pregnancy with hypertension self-reported similar types of visitations. Of concern, the present study determined that Black women who intentionally began pregnancy and were previously diagnosed with hypertension had statistically significantly 21% lower odds of having received PCSs compared with Black women who did not begin pregnancy with hypertension, the opposite of the heightened attention one would expect for a known high-risk condition. Likewise, the findings that receipt of care prior to pregnancy decreased with higher education and income were worrisome. The results aligned with a growing literature that indicates that education and income do not provide Black women the same protective health benefits as they do for other race/ethnicities. 1,33
The findings related to specific PCS and provider interactions highlighted notable differences in the clinical experiences of Black women with hypertension prior to pregnancy. The frequency of reception of regular checkups with the family doctor, OB-GYN, and dentist was reported as the most received service prior to pregnancy and was similar in frequency to those without a diagnosis of hypertension. Black women in this study self-reported that questions related to modifiable risk behaviors, such as cigarette usage, STI detection, interpersonal violence, and types of occupation, were initiated by providers more than counseling related to improving overall health prior to pregnancy. Of concern, more than half of the women indicated that during these appointments, their providers initiated no discussions on controlling their chronic conditions, such as diabetes or high blood pressure. Likewise, providers were less often to counsel on folic acid intake and family planning. These findings complement the results of a recent 2023 qualitative study conducted to understand the preconception care experiences of Black and Latina women with type 2 diabetes, which highlighted the missed opportunity providers have in discussing the impact of diabetes on future pregnancies and overall reproductive health. 45 Women stated in this study that they preferred to learn about the effect of diabetes before pregnancy occurred and expected providers to “bring up” this valuable topic of conversation at their appointments.
Inconsistent care
The ways providers interact with Black women have been concerning when investigating maternal health outcomes. 46 Systemic implicit bias 47 –49 and obstetric racism 50,51 create an environment for providers to be led by feelings of discomfort when caring for Black women, which results in pertinent health care needs not being addressed by providers. ACOG, 52 American Academy of Family Physicians, 2 and the U.S. Preventive Service Task Force, 53,54 have provided Anticipatory Guidance 16 for rendering care for women in childbearing years; however, discomposure as well as time constraints and balancing other clinical priorities can affect how well this guidance is followed.
Surprisingly, women who reported having hypertension prior to pregnancy mostly reported not seeing their providers specifically regarding a chronic illness or planning for their upcoming pregnancy. Not seeking out a provider for management of a current chronic illness or to receive family planning counseling could be a matter of lack of access, lack of understanding of the importance of such care, or simply mistrust of the health care system. 56 –58 This disconnect merits further exploration, especially as this study’s findings suggest Black women may need to become better self-advocates to offset these gaps in care.
Furthermore, the results of this study identified that the majority of the women did not receive provider counseling regarding folic acid intake, controlling chronic conditions, steps to improve health prior to pregnancy, and family planning and contraception. The inability of providers to communicate reproductive health concerns and how to manage chronic illness prior to pregnancy with Black women is a noted theme in current research, which aligns with the findings of this study. A 2019 study 59 on the perspectives of clinicians related to maternal care and Black women highlighted how providers’ perceptions of Black women have influenced what counseling or recommendations are given about family planning options. In fact, clinicians acknowledge that the results of inequitable care stem from racism and directly impact the frequency and quality of care given. Additionally, communication failures and differential treatment toward Black women are a common manifestation of interpersonal, internalized, and institutional racism. 60
Five states in this study show increased odds for Black women to receive health care services 12 months prior to their pregnancy. Of import, these five states have implemented targeted statewide programs to improve pregnancy outcomes. Our findings suggest that those programs are working. The state of Georgia, which has 183 Title X-funded family planning network sites, 61 has implemented programs focused on their effort to improve PCSs among Black women and those who are at risk for poor maternal health outcomes. 62 –64 Our findings suggest that these efforts focused in the area of optimizing health prior to pregnancy are indeed working: Black women residing in Georgia, Kansas, 65 North Dakota, 66 and South Dakota 67,68 have implemented statewide plans to advance preconception care health, which is supported by our findings. In addition to the statewide program efforts, Medicaid expansion has also contributed to improvements in addressing preconception risks in some states 69 –71 ; but even with the expanded coverage, our findings show that Black women in those states have lower odds of receiving care in preparation for pregnancy.
Limitations and strengths
Although PRAMS is a reputable data source and has been used for surveillance since 1987, its use in this analysis has potential limitations. Only individuals who had a live birth were recruited to participate in the PRAMS questionnaire, which may have resulted in a coverage error where women who had also become pregnant but did not have a live birth were excluded. This bias might lead to the underreporting of factors related to poor birth outcomes. Due to the data being collected retrospectively, potential exists for recall bias on what health behaviors and services occurred and were experienced prior to pregnancy. Additionally, the diagnosis of hypertension prior to pregnancy was self-reported with no clinical confirmation. Therefore, it is not possible to confirm or time the diagnosis.
Given the sample size and sampling strategy, our findings from this national dataset are generalizable to Black women in childbearing age who reside in the United States, which is a strength for this study. Additionally, this analysis isolated women who intended to become pregnant, which provided a basis for assessing how women were preparing for pregnancy. Finally, PRAMS data include preconception care variables related to received services, health behaviors, and health status, which allows for the analysis of strength of association between received services and future maternal outcomes.
Implications and Conclusions
Health promotion tools are needed to encourage Black women to seek care prior to pregnancy to optimize their health. This knowledge will allow women to advocate for themselves by addressing health concerns prior to pregnancy. Health care providers should elucidate the risks and treatment plans associated with beginning pregnancy with hypertension, diabetes, sickle cell anemia, or any other chronic illness to Black women. State-level initiatives, such as Medicaid expansion, can be effective and have led to improvements in addressing preconception health indicators. 71 Our findings suggest targeted state-level programs can also be effective. Innovative mechanisms such as web-based conversational tools improve the knowledge of preconception risks and prompt health behavior changes among Black women in their reproductive years. 72,73 As Black women become aware of the need for individual health behavior changes, they work to make the changes to improve their health, 74 which highlights the imperative need for providers to conduct provider counseling to identify preconception risks and establish a protocol to address areas of concern.
Differences in provider interactions demonstrate that improved provider communications with Black women in clinical settings are needed. Our findings highlight the need for providers to prioritize delivering these services, which can inform the development of standard of care guidelines to improve the offering of provider counseling, the promotion of healthy behaviors, and the targeting of interventions that improve the likelihood of a healthy pregnancy.
Based on our knowledge, this is the first study to examine the association of Black women with prepregnancy hypertension with the intention of being pregnant and the reception of PCSs. The literature is limited on how Black women perceive the importance of preconception care, but it is clear that receiving care prior to pregnancy mitigates pregnancy complications due to chronic illness. 1,2,8 ,75 The results of our study should spur the development of initiatives to improve how Black women receive preconception care and how providers initiate that care. Guidelines already exist on how quality preventative care should be offered to women during their childbearing years; it simply has to be followed. 53,54 Moreover, a deeper understanding is needed on why providers are not initiating counseling and limiting discussion on treatments designed to optimize health for Black women in their reproductive years.
Future research should investigate the components of access to PCSs for Black women in the United States. Additionally, more research is needed on the offer, reception, and results of health promotion and health education on PCSs for Black women during childbearing years. Finally, research is also needed to understand how provider guidelines are operationalized in clinical settings with Black women.
Authors’ Contributions
S.J.B. contributed to the study conception and design, analyzed the data, interpreted the data, and drafted the article. M.E.T. contributed to the study conception and design, interpreted the data, and edited the article. L.N.H., S.E.W., S.Y.K., and J.B.L. all contributed to the conception and design of the article. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors thank the PRAMS Working Group, which includes the PRAMS Team, Division of Reproductive Health, CDC, and the following PRAMS sites for their role in conducting PRAMS surveillance and allowing the use of their data.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was not supported by any sponsor or funder.