
Abstract
Objective:
The primary objective of this study was to estimate the specificity of cytology and high-risk human papillomavirus (hrHPV) testing to predict the presence of cervical intraepithelial neoplasia 2 (CIN2+) among transmasculine patients. The exploratory objective compared the specificity of cytology and hrHPV tests among three populations: transmasculine patients using testosterone, premenopausal cisgender, and postmenopausal cisgender patients.
Design:
This multicenter retrospective cohort study included individuals aged 18–65 undergoing cervical cancer screening from 2015 to 2024. Transmasculine patients were included if using ≥30 mg daily transdermal or ≥30 mg weekly subcutaneous testosterone for at least 6 months with no estrogen supplementation. Patients with co-tests followed by colposcopy or hysterectomy were included in the sensitivity and specificity analysis. McNemar’s test was used to examine differences in specificity between cytology and hrHPV tests within each cohort.
Results:
Of 2,437 records screened, 149 (70 transmasculine, 30 postmenopausal, and 49 premenopausal) met the inclusion criteria with co-tests followed by histologic confirmation via colposcopy or hysterectomy. In the transmasculine cohort, the specificity of screening to predict CIN2+ was comparable between cytology (68.9% [95% CI: 55.7 − 80.1%]) and hrHPV tests (63.9% [95% CI: 50.6 − 75.8%]) with a p-value of 0.26. Sensitivity was equivalent in the transmasculine cohort. In the postmenopausal cohort, specificity was significantly lower for hrHPV screening compared to cytology (24.1% vs. 69.0%).
Conclusions:
The ability of cytology and hrHPV screening to predict the presence of CIN2 + was not different in the transmasculine population. With high insufficient cytology rates, transitioning to primary hrHPV screening can limit unwanted pelvic exams and unnecessary diagnostic testing in transmasculine patients.
Introduction
Nearly all cervical cancers are associated with high-risk human papillomavirus (hrHPV) infection. 1 Cervical cancer can be both prevented and intervened upon at early stages with the use of regular cervical cancer screening with Pap smears and hrHPV testing. The U.S. Preventive Services Task Force has three grade A recommendations for cervical cancer screening between ages 30 and 65: cytology every 3 years, primary hrHPV testing every 5 years, or co-testing, a combination of both cytology and hrHPV testing, every 5 years. 2 Between ages 21 and 29, cytology alone every 3 years is recommended. 2
Multiple challenges exist when using conventional cervical cancer screening methods in the transmasculine population. The gynecology visit experience, the pelvic exam required for Pap smear completion, and the increased risk of insufficient cytology samples requiring repeated exams may all contribute to the lower lifetime odds of transmasculine patients having up-to-date cervical cancer screening.3,4 The presentation of transmasculine patients to the gynecology office puts patients at risk of misgendering and discrimination. Among transgender individuals, trans men and nonbinary individuals assigned female at birth (AFAB) report the highest rates of avoiding health care in the last 12 months out of concern for being disrespected as a trans person (32% and 24%, respectively). 5 Among those that received health care, AFAB nonbinary individuals and trans men also reported the highest rates of negative experiences with health care providers in the last year (55% and 53%). The pelvic exam also has both psychological and physical risks. While some patients desire physical examination at the time of presentation to the gynecologist, this can risk destabilization of one’s gender identity for others.6,7 Furthermore, this exam is often uncomfortable due to high rates of vaginal atrophy with testosterone use, comparable to atrophy found in the postmenopausal population.3,8–10 The cervical squamous epithelium also undergoes atrophy in transmasculine patients, contributing to a higher likelihood of misdiagnosis of atrophic changes as high-grade lesions.11,12 Transmasculine patients are more likely to have an atypical squamous cells of unknown significance (ASCUS) Pap smear result than their cisgender counterparts, and the rate of ASCUS in transmasculine individuals varies widely in the literature from 5.9% to 13.0%.8,11,13,14 Elevated rates of ASCUS results have also been documented in the postmenopausal population and are predominantly due to atrophy, with low positive predictive value (PPV) for dysplasia. 15 ASCUS results can increase the screening interval frequency and ultimately require more visits and pelvic exams for transmasculine patients. Research in the postmenopausal population has found that cytology has a lower specificity to predict the presence of cervical intraepithelial neoplasia (CIN) 2+ compared to primary hrHPV testing, with equivalent sensitivity. 16 Due to the similar hypoestrogenic environment caused by testosterone use, it has been questioned whether these results translate to the transmasculine population.
This project aims to explore the clinical utility of cervical cancer screening tests in the transmasculine population. The primary objective of this study is to estimate the specificity of cytology and hrHPV tests to predict the presence of CIN2+ among the transmasculine population. Our exploratory objective aims to compare the specificity of cytology and hrHPV tests to predict the presence of CIN2+ among three populations: transmasculine patients, premenopausal cisgender patients, and postmenopausal cisgender patients. Our hypothesis is that the ASCUS results in the transmasculine population are due to atrophy rather than dysplasia and are therefore false positive (FP) results that decrease the specificity of cytology compared to hrHPV testing. We also expect the performance of cytology to be similar to that in the postmenopausal group, due to atrophic changes in both populations.
Materials and Methods
This study is a multicenter retrospective cohort analysis to explore Pap smear cytology and hrHPV performance for cervical cancer screening in the transmasculine population. The Oregon Health and Science University Institutional Review Board (IRB#27056) and Kaiser Northwest Institutional Review Board (IRB#2193171-5) both approved via expedited review and provided oversight for this study.
Records were collected by querying the electronic health record (EHR) for individuals AFAB and over the age of 18 with a documented Pap smear completed between January 1, 2015, and December 31, 2024. Inclusion criteria for the transmasculine cohort were a gender identity of “nonbinary,” “male,” or “transgender male” and testosterone use. Gender identity was found among demographic data within the medical record, and if not explicitly denoted, patients with pronouns including “she/they,” “they/them,” or “he/they” were included. To capture individuals with a clinically meaningful testosterone effect, individuals were included if they had used ≥30 mg subcutaneous testosterone (e.g., testosterone cypionate) weekly or ≥30 mg transdermal testosterone (e.g., testosterone 1% gel) daily for at least 6 months. 3 The inclusion criteria for the postmenopausal cohort were age over 52 years or provider documentation of menopause in the medical record. Patients were included in the premenopausal cohort if they were aged 18–50, had no documented testosterone use, and had no documentation of menopause or documentation of menses within 12 months of a Pap smear. Patients were excluded if they had a history of hysterectomy prior to the screening test of interest, gynecologic malignancy, radiation therapy with fields including the uterine cervix or vagina, pregnancy during Pap smear collection, or were unable to be categorized as pre- or postmenopausal. Postmenopausal or transmasculine patients were excluded if they had prescriptions for any formulation of estrogen.
To fulfill the primary and exploratory aims of this study, demographic and clinical information were extracted from the medical record. For each Pap test during the study period (2015–2024), we collected data including the test type (cytology only, hrHPV only, or co-test), date of test, and cytology and hrHPV results. For any colposcopy or hysterectomy for benign indications performed during the study period, we documented the procedure date and pathology results. We collected additional demographic information, including age (at the time of the first Pap smear documented within the time frame of the study).
For all Pap test results during the study period, we calculated the proportion of ASCUS, insufficient cytology samples, low-grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion (HSIL), and hrHPV positivity results among all the Pap tests in our sample during the study period, reported at the test level. At the patient level, we assessed the prevalence of insufficient cytology results among each of the patient populations by assessing the proportion of patients in each group that ever had an insufficient cytology result during the study period.
For our primary analysis, sensitivity and specificity were calculated using data from all patients with histological confirmation in the form of colposcopy or hysterectomy during the study period, following a co-test. 17 For each patient, the histologic result was considered the gold standard, with colposcopy favored over hysterectomy if both were available. The patient’s most recent Pap test was then compared to the histologic confirmation. We generated 2 × 2 tables comparing true negatives, true positives, false negatives (FN), and FP results for cytology testing and hrHPV separately. Positive cytology tests were defined as results of ASCUS or worse (e.g., LSIL, HSIL, atypical glandular cells). Histology results of CIN2 or worse were considered positive gold standard tests. We calculated and reported sensitivity, specificity, PPV, negative predictive value (NPV), and associated 95% confidence intervals for each.
Due to the paired nature of the data (patients with co-testing having both cytology and hrHPV test results), we used McNemar’s test to determine whether there was a significant difference in the specificity of the two tests within each of our population groups. We obtained a sufficient sample size of disease-free patients who received a co-test prior to histologic confirmation in our transmasculine cohort to detect a 15% difference in the probability of a negative result between the cytology and hrHPV test among the same participants with greater than 80% power (>50 patients). 16 Although we included an equal number of patients from each group, due to a differential rate of referral and completion of the gold standard testing between groups, we were underpowered for this comparison in the cisgender premenopausal and cisgender postmenopausal groups. Data were extracted from the chart records into the REDCap electronic study database and analyzed using Stata 18 (StataCorp, College Station, TX, USA). A two-tailed p-value was used for all analyses with an alpha level of 0.05 to indicate statistical significance.
Results
A total of 2,437 records were screened, with 1,377 meeting the inclusion criteria and 149 included for the primary analysis. There were 456 patients in the transmasculine cohort, 457 in the cisgender postmenopausal cohort, and 464 in the cisgender premenopausal cohort (Table 1). Included in our primary analysis, 149 patients underwent further evaluation with histologic confirmation in the form of colposcopy or hysterectomy after a co-test (70 transmasculine, 30 postmenopausal, and 49 premenopausal patients), as exhibited in Table 2. The transmasculine cohort included a larger proportion of patients with hysterectomy (42.9%) than either of the two groups, for whom the vast majority of gold standard tests used for calculating sensitivity and specificity were colposcopies. The cohort selection diagram is shown in Figure 1.
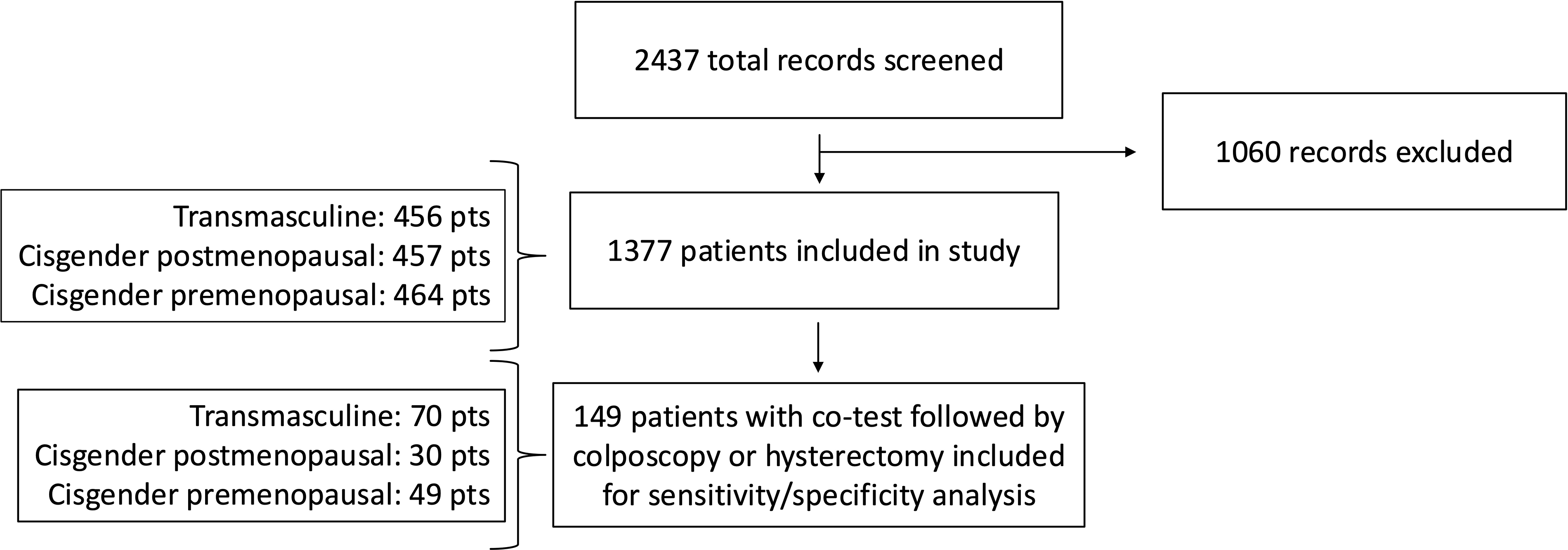
Cohort Selection Diagram. Figure 1 illustrates the number of records screened and included for analysis among each cohort.
Cohort Characteristics of All Cervical Cancer Screening Among All Populations
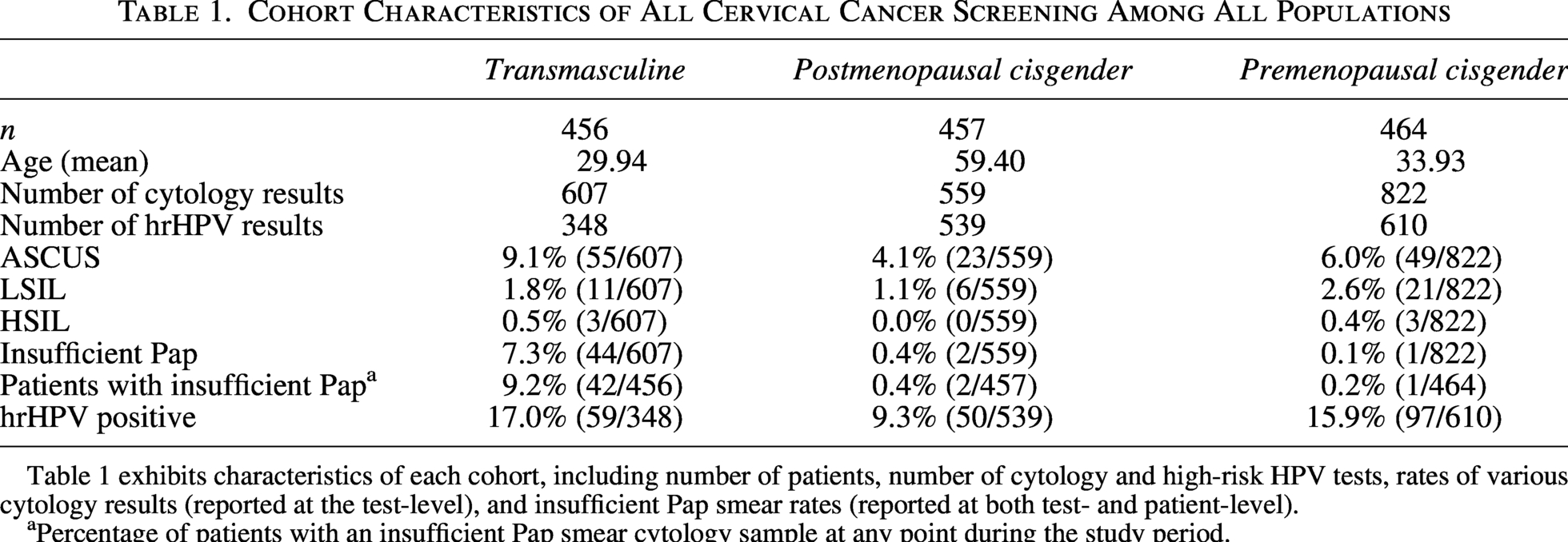
Table 1 exhibits characteristics of each cohort, including number of patients, number of cytology and high-risk HPV tests, rates of various cytology results (reported at the test-level), and insufficient Pap smear rates (reported at both test- and patient-level).
Percentage of patients with an insufficient Pap smear cytology sample at any point during the study period.
Primary Analysis Cohort Characteristics
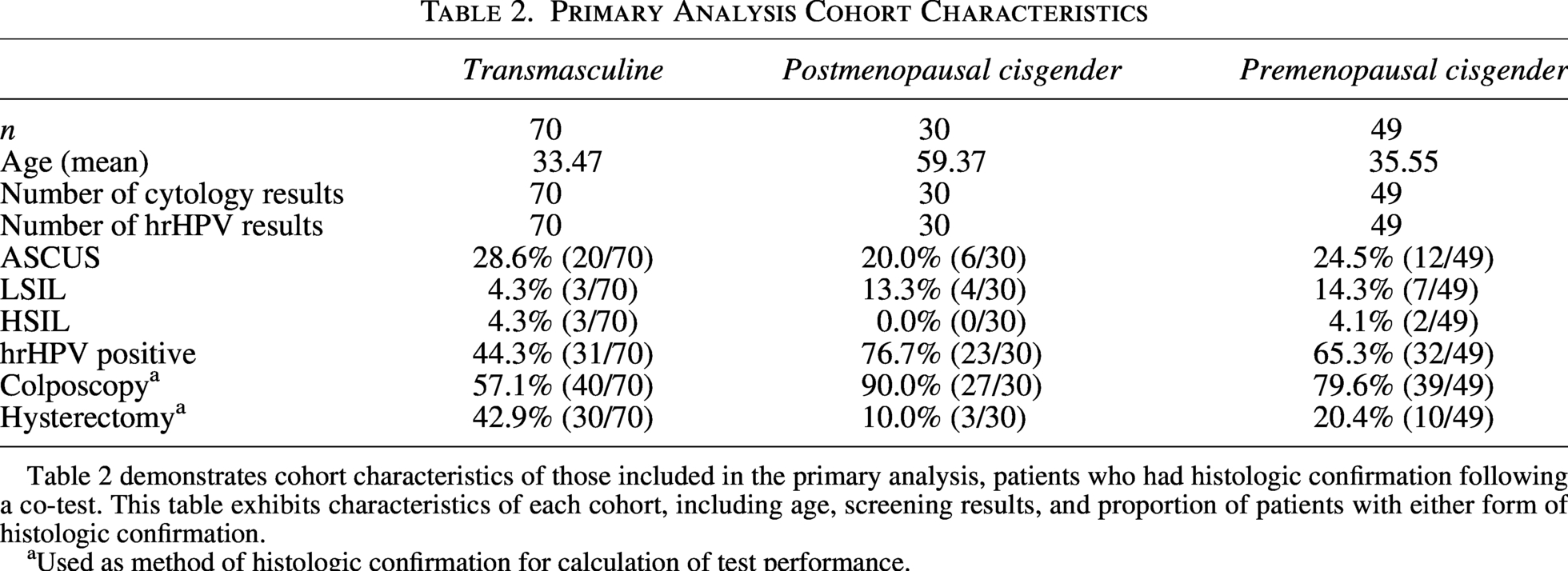
Table 2 demonstrates cohort characteristics of those included in the primary analysis, patients who had histologic confirmation following a co-test. This table exhibits characteristics of each cohort, including age, screening results, and proportion of patients with either form of histologic confirmation.
Used as method of histologic confirmation for calculation of test performance.
The average age was lowest in the transmasculine cohort (29.9) compared to cisgender cohorts (59.4 and 33.9). The rate of ASCUS out of all cytological tests was highest in the transmasculine cohort (9.1%), compared to cisgender populations (4.1% in the postmenopausal and 6.0% in the premenopausal cohort). Of all cytology results, 7.3% were insufficient in the transmasculine cohort, compared to 0.04% and 0.1% in the postmenopausal and premenopausal cohorts, respectively. This translates to 9.2% of all transmasculine patients having an insufficient Pap smear at least once during the study period. The positivity of hrHPV was comparable between the transmasculine and premenopausal cohorts (17.0% and 15.9% of all tests, respectively), compared to 9.3% of all tests in the postmenopausal cohort. A higher proportion of tests in the transmasculine cohort (19.7%) were followed by a colposcopy procedure, compared to 6.6% of tests in the postmenopausal cohort and 9.1% in the premenopausal cohort (data not shown).
Test performance to predict the presence of CIN2+ among all cohorts is displayed in Table 3. In the transmasculine cohort, the specificity of screening to predict the presence of CIN2+ was comparable between cytology and hrHPV tests (68.9% compared to 63.9%). The sensitivity of cytology and hrHPV testing was high in both the transmasculine cohort and postmenopausal cohorts. The specificity of abnormal cytology to predict the presence of CIN2+ (68.9%) was not statistically significantly different from the specificity of hrHPV testing (63.9%) in the transmasculine cohort (p = 0.26). The difference in specificity between cytology and hrHPV testing was more notable in both postmenopausal and premenopausal cohorts (69.0% vs. 24.1% and 59.0% vs. 41.0%, respectively). Although underpowered due to small numbers, the difference reached statistical significance (p = 0.002) in the postmenopausal cohort and approached but did not reach statistical significance in the premenopausal cohort (p = 0.09). Figure 2 demonstrates the specificity of abnormal cytology and hrHPV positivity to predict CIN2+ across the three cohorts. The PPV of cytology and hrHPV screening was similar in the transmasculine cohort (32.1% and 29.0%, respectively) and comparable to that in the premenopausal cisgender cohort (30.4% and 28.1%, respectively). The transmasculine PPV for both tests was higher than that in the postmenopausal cohort (10.0% and 4.4%, respectively).
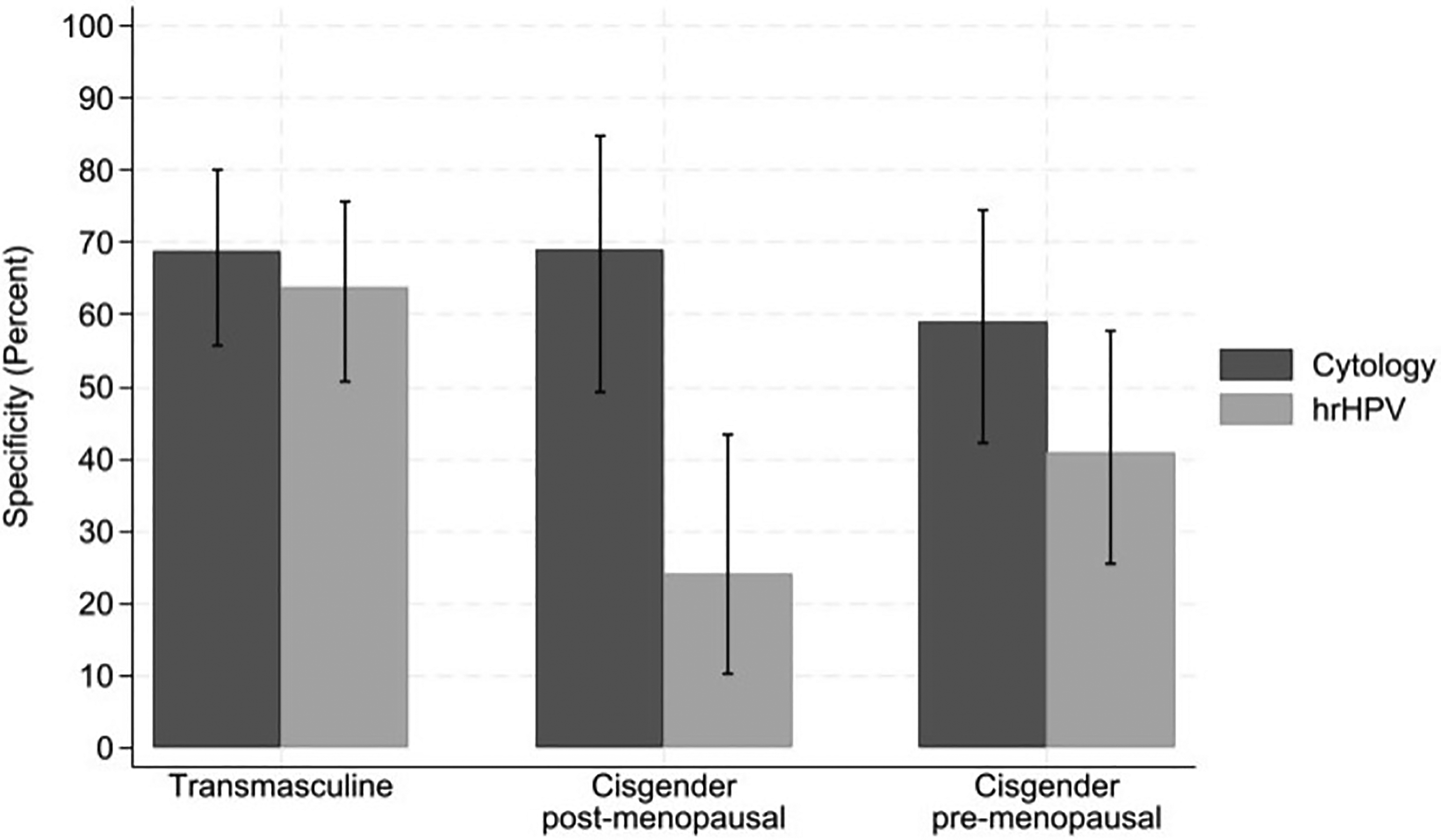
Specificity of Cervical Cancer Screening to Predict CIN2 or Worse Across Cohorts . Figure 2 illustrates the specificity of cytology and hrHPV screening tests to predict the presence of CIN2+ among each cohort, with positive cytology test defined as ASCUS or worse.
Cervical Cancer Screening Performance to Predict Presence of CIN2 or Worse
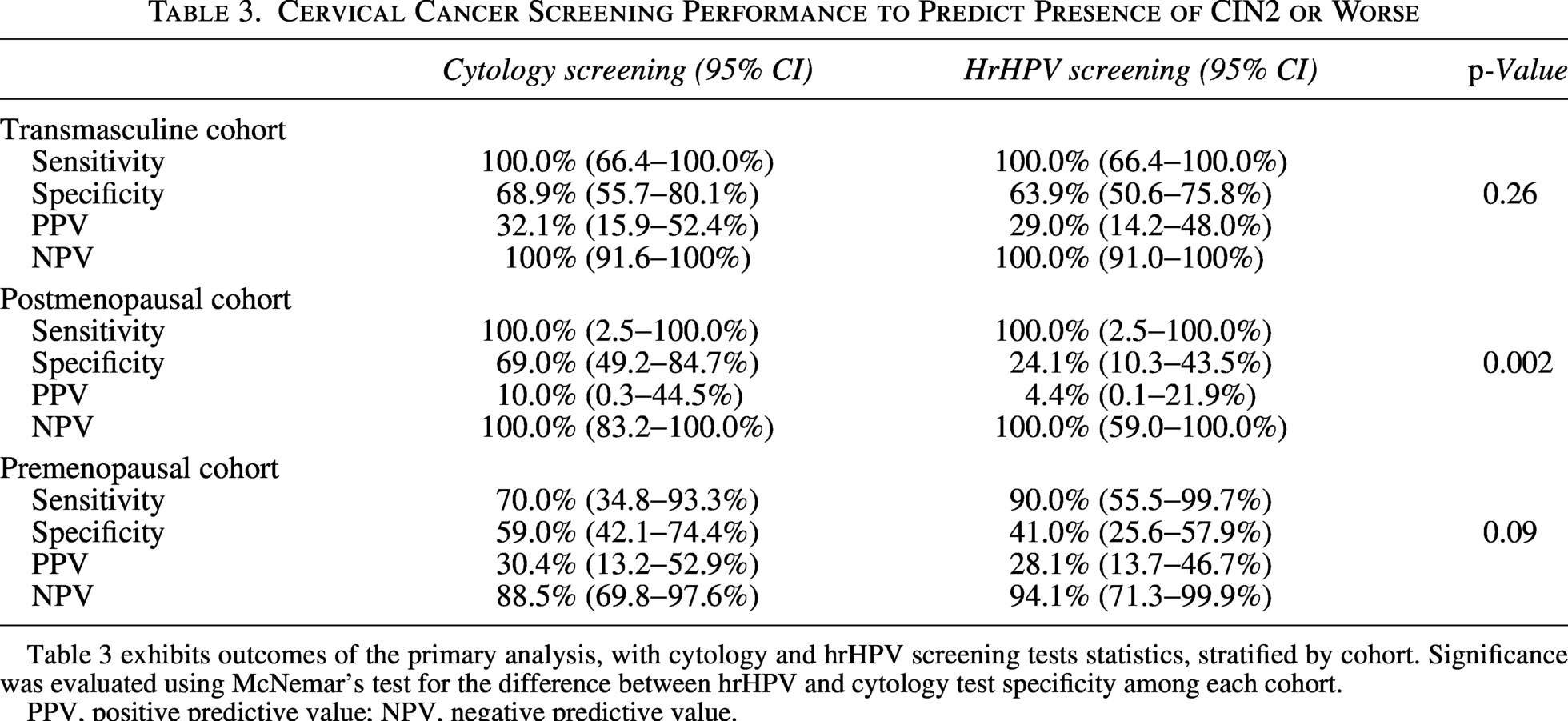
Table 3 exhibits outcomes of the primary analysis, with cytology and hrHPV screening tests statistics, stratified by cohort. Significance was evaluated using McNemar’s test for the difference between hrHPV and cytology test specificity among each cohort.
PPV, positive predictive value; NPV, negative predictive value.
Discussion
Principle findings
Our results demonstrate that there is no statistically significant difference between the specificity of cytology and hrHPV screening tests to predict the presence of CIN2+ in transmasculine patients. In other words, cytology screening is not better than hrHPV screening in reducing false positive results. Notably, 9.2% of transmasculine patients received at least one cytology test with an insufficient sample during the study duration. Sensitivity for both tests was high in all cohorts. PPV of screening tests is comparable between the two tests in the transmasculine cohort and comparable to the PPV for both tests in their premenopausal cisgender counterparts. The PPV for the hrHPV and cytology tests were higher in the transmasculine cohort than the postmenopausal cohort, which may be explained by disease prevalence and its effect on PPV. These results suggest that the likelihood of a positive screening result to predict the presence of dysplasia is fairly equal in both cytology and hrHPV screening.
Strengths and weaknesses of the study
Primary strengths of this study include its novel design in comparing cervical cancer screening test performance among multiple cohorts, most notably the transmasculine cohort, a population that until recently has been absent from cervical cancer research. The comparison of the transmasculine cohort to the postmenopausal population, also known to have vaginal atrophy, strengthens our analysis. Further, the multicenter design allowed for the collection of data from large numbers of transmasculine patients.
Due to this study’s retrospective nature, fewer patients with negative screening underwent diagnostic testing, limiting a representative capture of FN results and therefore reducing the validity of sensitivity and NPV results. Additionally, this study included two measures of the gold standard diagnostic testing, both colposcopy and hysterectomy specimens. Each cohort had a different proportion of colposcopy and hysterectomy specimens (see Table 2) used to generate test performance statistics, limiting the ability to compare across cohorts. Further, colposcopy may underestimate the prevalence of dysplasia due to its reliance upon provider interpretation and biopsy choice.
Comparison to current literature
The specificity of cytology and hrHPV testing to predict CIN2+ in the transmasculine cohort, 68.9% and 63.9%, respectively, is lower than what is reported in randomized controlled trials, which estimate the cytology and hrHPV specificity to be 97.3% and 94.3%, respectively. 18 Randomized trials also estimate the sensitivity of cytology in allcomers (55%) is lower than with hrHPV screening (95%). This study’s results of cytology and hrHPV sensitivity of 100% in atrophic populations are comparable to the sensitivity found by Kiff et al in the postmenopausal population when comparing incident Pap smears to CIN2+ incidence at 5 years, which is likely attributed to the retrospective nature of both studies. 16 Currently published prospective clinical trials, like Mayrand et al., have investigated a largely cisgender, premenopausal cohort, while our study analyzes three unique cervical environments. 18
Our finding of a significantly different specificity to predict CIN2+ with cytology and hrHPV testing was not demonstrated by Kiff et al, who found a significantly lower specificity in cytology specimens compared to hrHPV specimens. The ASCUS rate in the postmenopausal population in our study was lower than reported in the literature and in Kiff et al, which may have contributed to the conflicting results. This lower ASCUS rate may be accounted for by increasing documentation of menopausal status in Pap smear order sets in the EHR to provide clinical context to cytopathologists.
Studies have documented an 8 times higher inadequate Pap smear prevalence in the transmasculine population compared to cisgender counterparts.3,19 Our analysis supports these findings with 9.2% of transmasculine patients with insufficient cytology samples, compared to 0.4% of the cisgender premenopausal cohort. Peitzmeier et al found that the majority of insufficient Pap smears were attributed to scant cellularity and that the risk of insufficient Pap increases after 6 months of testosterone use. 3
Meaning of the study
To account for cytologic differences in the transmasculine population, clinicians should prioritize primary hrHPV testing, in accordance with the American Cancer Society screening guidelines. Our results reveal that while sensitivity and specificity of cytology and hrHPV screening for cervical dysplasia are not different in the transmasculine cohort, the increased insufficient and ASCUS Pap results in the transmasculine population make primary hrHPV testing ideal. With primary hrHPV testing, clinicians may minimize unnecessary repeated pelvic examinations and reduce unnecessary diagnostic testing in transmasculine patients. Gottschilch et al. found that the employment of primary hrHPV screening results in lower colposcopy referral rates, particularly when triaged with cytology following a positive result. 20 Adopting primary hrHPV self-swab screening may further improve the experience of cervical screening in this population.
Unanswered questions and future research
More research is needed to explore the use of primary hrHPV self-collection in a variety of practice settings, including clinic-testing and home kit-based testing. Prospective data are needed to understand long-term outcomes in colposcopy referral and screening performance with the use of primary hrHPV testing in transmasculine patients. Qualitative research could incorporate the patient perspective in the optimization of best practices. Alongside the use of self-collection should be made to ensure that the clinic-performed Pap smear and colposcopy environment is inclusive, as screening test performance only holds true when patients complete the necessary follow-up testing. Future studies may explore transmasculine patient acceptability of the colposcopy experience and alternative environments to the clinic for completion of confirmation of histology.
Conclusions
While rates of insufficient Pap smear results were high, the ability of cytology and hrHPV screening to predict the presence of CIN2+ was not different in the transmasculine population. Transition toward primary hrHPV screening may limit unwanted pelvic exams and unnecessary diagnostic testing in the transmasculine population.
Authors’ Contributions
K.B.—guarantor of article; substantial contribution to the conception or design of the work; substantial contribution the acquisition, analysis and interpretation of data for the work; substantial contribution to drafting the work or revising it critically for important intellectual content; and final approval of the version to be published. H.B.—substantial contribution to the conception or design of the work; substantial contribution the acquisition, analysis and interpretation of data for the work; substantial contribution to drafting the work or revising it critically for important intellectual content; and final approval of the version to be published. C.S.—substantial contribution to the conception or design of the work; substantial contribution to drafting the work or revising it critically for important intellectual content, final approval of the version to be published. K.S.—substantial contribution the acquisition, analysis and interpretation of data for the work; final approval of the version to be published. A.M.—substantial contribution the acquisition, analysis and interpretation of data for the work; final approval of the version to be published. G.D.H.—substantial contribution to the conception or design of the work; substantial contribution to drafting the work or revising it critically for important intellectual content, final approval of the version to be published. J.J.—substantial contribution to drafting the work or revising it critically for important intellectual content, final approval of the version to be published. A.B.—substantial contribution to the conception or design of the work; substantial contribution the acquisition, analysis and interpretation of data for the work; substantial contribution to drafting the work or revising it critically for important intellectual content; and final approval of the version to be published. All authors contributed to the interpretation of the results and reviewed and approved the final article. The corresponding author is the guarantor.
Footnotes
Acknowledgments
A poster presentation at the Society of Gynecologic Oncology Annual Meeting, March 2025, and an oral presentation at the Western Association of Gynecologic Oncology Annual Meeting, June 2025, were completed based on this research.
Author Disclosure Statement
All authors declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years, no other relationships or activities that could appear to have influenced the submitted work. A.B. is a consultant for AbbVie without relevant conflicts of interest to this subject matter. All other authors report no conflicts of interest.
Funding Information
This research was funded by the Robert Wood Johnson Foundation Grant #77148.