
Abstract
Background:
Despite significant medical and scientific advances, gaps remain in women’s health research across the lifespan. We explore the use of the All of Us Research Program Data set to help close the research gaps for women.
Methods:
This paper describes the utility of the All of Us Research Program—a large, longitudinal U.S. cohort of over 800,000 individuals (63% women) representing all 50 states—to advance research in women’s health. Three use cases explore conditions that affect women: (1) disproportionality (hyperthyroidism and osteoporosis), (2) differently (health care access), and (3) uniquely (postpartum hemorrhage). Each use case utilized electronic health records, survey responses, and clinical measurements, and was analyzed with R on the secure cloud-based workbench.
Results:
Hyperthyroidism was strongly associated with the development of osteoporosis, suggesting opportunities for additional screening and treatment. Examining access to care, women described barriers including cost, transportation, and caregiving responsibilities. In postpartum hemorrhage of the over 10,000 pregnancies we analyzed, the multivariable linear regression showed that anemia, preeclampsia, obesity, placental abruption, and placenta previa were all significant risk factors. These use cases demonstrate the size and depth of the data and the usefulness for testing hypotheses and identifying areas for screening and prevention for women’s health.
Conclusions:
All of Us enables comprehensive, inclusive research into sex-specific health issues. Our analyses show how this dataset fills long-standing gaps by supporting stratified analyses enabling research into women’s health across the lifespan. Researchers can readily access these tools to accelerate science and medical advances for women.
Keywords
Introduction
The United States continues to face significant challenges in the design and conduct of women’s health research. Historically, women have been underrepresented in clinical trials, resulting in a lack of data reflecting conditions affecting women differently, disproportionately, and uniquely, and across the lifespan. 1 The 1993 U.S. National Institutes of Health (NIH) Revitalization Act mandated inclusion of women in NIH-funded clinical research, leading to additional reporting by sex 2 however, deficiencies remain. Particularly in the 1970s and 1980s, women were excluded from clinical research, due to concerns about potential harm in reproductive health and assumptions that findings in men could be generalized to women. 3 –5 This exclusion led to inadequate sex-specific data and the inability to account for differences in drug metabolism, efficacy, and adverse effects. Indeed, women experience adverse drug reactions nearly twice as often as men, partly because dosing recommendations were based predominantly on trials of male participants. 6,7 Further, there has been a paucity of studies that address biological differences—such as hormonal influences, immune response differences, perimenopause, and pharmacokinetics—making inclusion of women critical to understanding disease processes, progressions and outcomes. 7 While policies have pushed for more balanced representation, few large cohort studies are designed specifically for women in recruitment, enrollment, and retention. The two largest and best-known studies are the Nurses’ Health Study (NHS) and the Women’s Health Initiative (WHI). Starting in 1976, the NHS is now in its third generation with NHS 3 (enrolling male and female nurses www.hus3.org) with over 275,000 participants. The unique strengths of NHS include regular follow-up and repeated assessment of health and lifestyle factors. Notably, NHS has helped to shape public health recommendations.
The WHI began in 1991 and is sponsored by the National Heart, Lung, and Blood Institute (NHLBI). WHI has enrolled 161,000 women at 40 centers. The initial focus was on preventing heart disease, breast and colorectal cancer, and osteoporosis in postmenopausal women. Although the initial study was completed in 2005, the WHI continues to contribute to the science of women’s health through extension and ancillary studies.
While the strengths of these studies are clear, no large-scale effort has combined medical records, biospecimens, physical measurements, genetics, and self-reported surveys on a national scale. Furthermore, no study allowing us to compare men and women has been specifically enriched for women as the dominant group. We describe how this dataset can accelerate women’s health research, defined by the NIH as “diseases that affect women uniquely, differently, and disproportionately.” At inception, it was envisioned as a “first of its kind’ resource modeled on innovations in women’s health and large-scale genomic efforts such as the U.K. Biobank. The vision was to enable precision medicine and individualized clinical care, guided by the nation’s scientific priorities and evolving health needs.
Launched in 2018, All of Us is a disease-agnostic, cloud-based research platform designed to accelerate scientific discovery. This longitudinal study aims to enroll one million or more participants, providing a resource for the collection and analysis of biomedical data to inform prevention, precision medicine, and overall health. All of Us contains survey data in English and Spanish, electronic health records, physical measurements, biospecimens, mobile/wearable devices, assays, “omics” data (including long, reads short reads, and Single Nucleotide Polymorphisms), phenotype, and genotype data) in an All-by-All Directory. Participants are recruited through medical centers, Federally Qualified Health Centers, mobile bus units, and self-enrollment kits. The program is digital-first, with enrollment beginning electronically, followed by an in-person visit for physical measurements, when possible.
All of Us recruitment targets populations that have not had access to large-scale research participation, including rural communities, women, children, and older adults, thereby better reflecting our nation’s population and enabling more relevant research efforts. In 2019, All of Us Investigators published the operational protocol for launching national enrollment and baseline data collection. 8 Since then, the cohort has grown to over 800,000 individuals from across the United States, 63% women. Its operational protocol has expanded, and its repository of clinical, behavioral, and genetic data has launched 20,000+ research projects as of September 2025. All of Us provides a unique opportunity to study women’s health across the United States.
To demonstrate the breadth and depth of this dataset, we provide three use cases along with analytics to serve as models for women’s health research using All of Us. Each use case illustrates one of three categories: conditions affecting women differently, disproportionately, and uniquely. We also explored access and utilization in the care women seek and receive, as well as the reasons for delayed or incomplete care for women.
We describe the use of the data to examine hyperthyroidism (HT) and osteoporosis (OP), which affect women both disproportionately and differently, and barriers to care, which affect women differently. Lastly, we examine postpartum hemorrhage, a condition affecting women uniquely. Our use cases illustrate these differences by demonstrating how certain health conditions develop in women compared with men. These findings underscore the need to move beyond simply adjusting for sex as a covariate in pooled analyses, as this is insufficient when the effects of risk factors are not homogeneous across genders. Instead, exploring interactions between sex and risk factors, conducting sex-stratified analyses, and applying factor cluster analysis uncovers sex-specific mechanisms in health outcomes.
Use Case 1: A Condition That Affects Women Disproportionately and Differently–HT and OP
HT is a condition in which the thyroid gland generates and secretes excessive amounts of thyroid hormone. 9 Several studies have shown that HT is more common in women than men, 10,11 specifically, the Whickham Survey 12 revealed that the prevalence of HT in women was nearly 12 times higher than in men (2.7% versus. 0.23%). HT exhibits a broad range of clinical symptoms and manifestations that are linked to substantial physical 12 –14 and mental effects. 15 One significant consequence of elevated thyroid hormone levels is their impact on bone metabolism, often leading to a drastic reduction in bone mineral density. This can lead to OP, which increases the risk of fragility fractures and is associated with higher mortality rates. 16,17 We examined HT as a use case in the All of Us Workbench, as an example of a condition that affects women disproportionately, and how conditions can be studied in tandem in this dataset. In this use case we analyze HT and the effect on OP.
Methods
Exposure: HT
A binary variable indicating HT was synthesized from available electronic health records (EHR), retrieved via the All of Us workbench search function for the terms “hyperthyroidism,” “Graves’ disease,” and “thyrotoxicosis.” We confirmed the diagnosis of HT for each participant by comparing the earliest and latest dates of HT, Graves’ disease, and thyrotoxicosis; for confirmed diagnoses, the second earliest distinct diagnosis date became the confirmed diagnosis date. This critical step helped to eliminate any medical records, which were coded as “rule-out” HT and left us with only those who “ruled-in.” Participants treated for HT with commonly prescribed medications were marked as diagnosed, including methimazole, propylthiouracil, thyrotropin alfa, iodine (131I) compounds, and antithyroid preparations.
Outcome: OP
We created a binary variable indicating diagnosis of OP from data retrieved via a Workbench search for “osteoporosis.” As with HT, the second-earliest distinct diagnosis date became the confirmed date of diagnosis. Participants with confirmed OP diagnosis were included for analysis only where the OP diagnosis followed HT diagnosis. Participants prescribed medication for OP such as romosozumab, raloxifene, teriparatide, abaloparatide, bisphosphonates, combinations, denosumab, and bazedoxifene were marked as diagnosed. Records for prescribed supplements, such as cholecalciferol, were not considered an indication of diagnosis.
Data analysis
Data were analyzed within Jupyter notebooks using R version 4.4.0 and stored within the virtual environment of the All of Us Workbench. All data were derived from Controlled Tier Dataset V8. The ATHENA-OHDSI database was used to obtain Observational Health and Medicines Outcomes Partnership codes, Systemized Nomenclature of Medicine codes, and equivalent diagnosis terms.
We assessed differences in participant demographics and Body Mass Index (BMI) stratified by OP diagnosis. We reported summary statistics as means and standard deviations for continuous variables, and frequencies (percentages) for categorical variables. Group comparisons were evaluated using two-sided t-tests and Chi-squared tests.
As death records were not available for every participant, participant data were included for analysis only if their latest available EHR date was recorded within 5 years preceding the enrollment survey response. Throughout these analyses, a two-sided p-value < 0.05 was considered statistically significant.
We employed univariable logistic regression models, followed by a multivariable model including an interaction term between sex and HT in predicting OP. Since the interaction was statistically significant, we then used sex-stratified analyses, adjusting for age, race/ethnicity, education, income, relationship status, insurance status, and categorical BMI.
Result
The demographic characteristics for the cohort appear in Table 1. In total, data from 269,790 individuals were assessed, with women constituting 60.8% of those analyzed (n = 164,032). EHR indicated 264,222 (97.9%) had no confirmed HT diagnosis, whereas 5,568 (2.1%) were found to have a confirmed diagnosis of HT. Of those diagnosed with HT, 81.3% were women and 18.7% were men; by sex, 2.8% of women and 1.0% of men were diagnosed with HT. In women, HT diagnosis occurred regularly across most age categories, with 1.8% diagnosed at ages 18–44, 3.3% at ages 45–54, 3.2% at ages 55–64, 3.5% at ages 65–74, and 3.1% at age 75 or older. For men, HT prevalence remained low across age categories, with 0.5% diagnosed at ages 18–44, 0.8% at ages 45–54, and 0.1% at ages 55–64, 65–74, and ages 75 or older. Figure 1 illustrates the differences in OP prevalence by age and HT, stratified by sex.
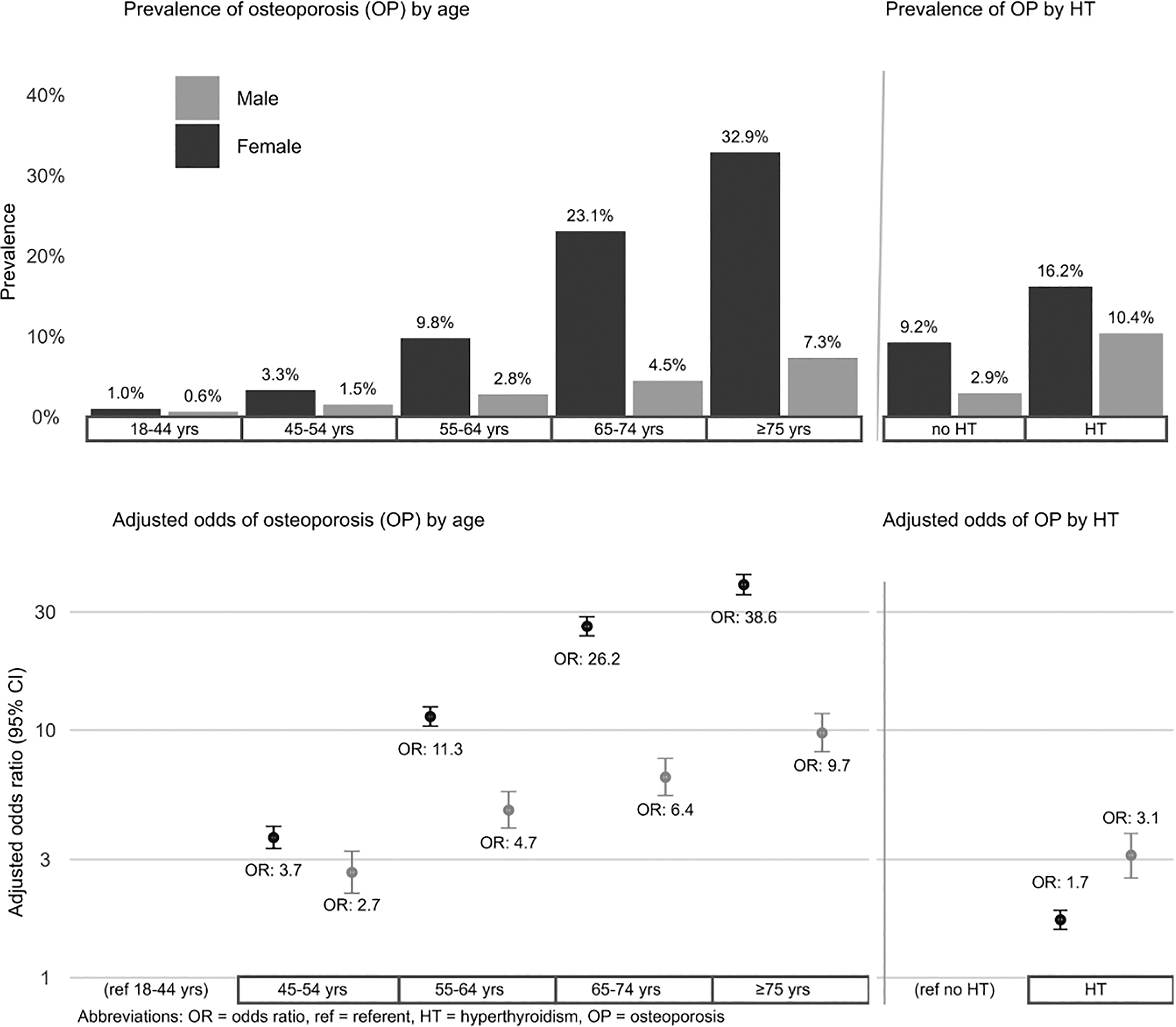
Prevalence and adjusted odds of osteoporosis by age and HT diagnosis.
Hyperthyroidism: sample Characteristics, Percent by Column
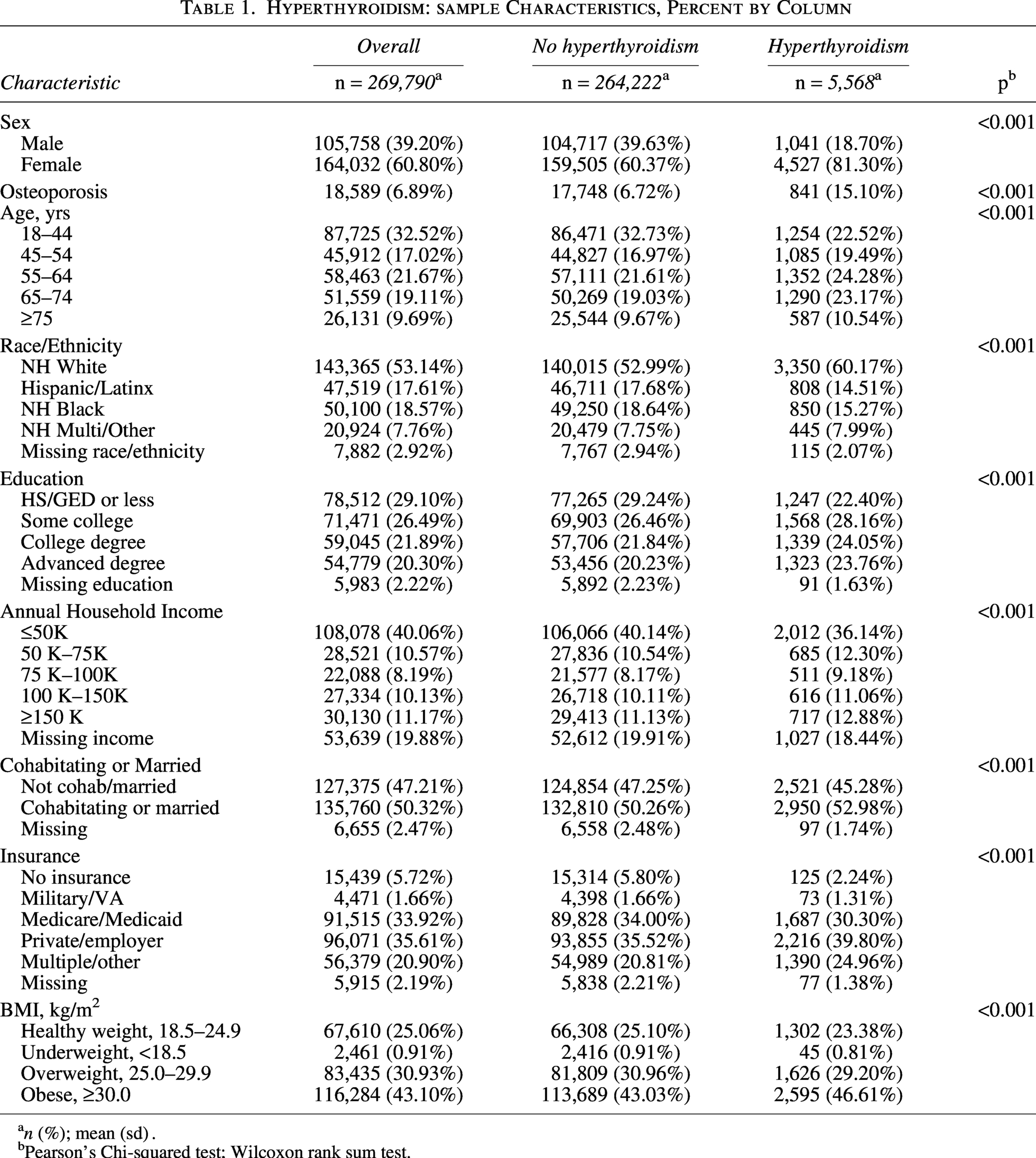
n (%); mean (sd) .
Pearson’s Chi-squared test; Wilcoxon rank sum test.
In univariable models (Supplementary Table S1), individuals diagnosed with HT had more than twice the odds of being diagnosed with OP compared with those without HT (unadjusted Odds ratio [OR] 2.47, 95% CI: 2.29–2.66, p < 0.001), and women had over 3 times the odds of developing OP compared with men (unadjusted OR = 3.35, 95% CI: 3.23–3.49, p < 0.001). When stratified by sex and adjusted for covariates, women with HT had 1.71 times the odds of developing OP than women without HT (OR 1.71, 95% CI: 1.57–1.87, p < 0.001), whereas men had 3.12 times the odds of developing OP than men without HT (OR 3.12, 95% CI: 2.52–3.82, p < 0.001). Odds of developing OP rose with older age for both sexes, though the magnitude of increase differed in multivariable models. Women had over 11 times the odds of OP at ages 55–64 compared with women 18–44 (OR 11.3, 95% CI: 10.4–12.4, p < 0.001), whereas men 55–64 years of age had nearly 5 times the odds of developing OP compared with men 18–44 years of age (OR 4.75, 95%CI: 4.02–5.64, p < 0.001). Women aged 65–74 years had 26 times the odds of OP at ages 65–74 compared with women 18–44 (OR = 38.6, 95% CI: 35.2–42.5, p < 0.001), whereas men at ages 65–74 had over 6 times the odds of OP compared with men 18–44 (OR = 6.45, 95% CI: 5.44–7.68, p < 0.001). Women at 75 years or older had 38 times the odds of OP compared with women at ages 18–44 (OR = 38.6, 95%CI: 35.2–42.5, p < 0.001), whereas men 75 years or older had nearly 10 times the odds of OP than men 18–44 (OR 9.74, 95% CI: 8.18–11.7, p < 0.001) (see Fig. 1).
Discussion
This analysis showed that although the adjusted effect of HT on OP was lower overall, as expected, the odds of OP increased significantly across all age groups. However, the impact of HT on OP appears greater in men, likely due to their lower baseline OP rate. In women, the likelihood of developing OP rises dramatically with age, regardless of HT status. In contrast, in men, the increased risk for OP may be due to biological susceptibility in HT to bone loss from excess thyroid hormone. Historically, research has often failed to adequately reflect women across the lifespan, leading to gaps in understanding various conditions affecting women, such as OP. These results highlight opportunities for further investigation using the All of Us dataset.
Use Case 2: A Condition That Affects Women Differently–Health Care Access and Utilization
According to the McKinsey Blueprint for Closing the Gap in Women’s Health, although women live longer than men, they live those extended years in poorer health. 18 In part, this may be due to women facing significant barriers to accessing and utilizing health care services. Financial constraints remain a major obstacle, with women spending an average of 20% more on out-of-pocket health care costs than men—even when excluding maternity-related expenses. 18 This disparity is further exacerbated by the ongoing gender wage gap, making health care even less affordable for women. 19 Additionally, systemic issues such as limited appointment availability, transportation challenges, and difficulties finding providers who accept their insurance have led to delays or avoidance of necessary medical care. In 2022, approximately 22% of U.S. adults reported delaying or not receiving medical care due to nonfinancial access barriers. 20 We selected this use case to demonstrate a condition that affects women differently.
Methods
We used the All of Us dataset to explore Health Care Access and Utilization via a survey that examines factors associated with barriers in accessing medical care. Participants reported reasons for postponing health care and avoiding certain types of care in the past year due to cost concerns. Responses collected within 2 years following the enrollment survey were analyzed. Responses of “Yes” (1), “No” (0), or “Don’t know” (0) were coded to identify barriers in five domains: Transportation Access, Everyday Responsibilities, and cost of General Health care, Medication, and Mental Health care, as shown in Table 2.
Healthcare Access and Utilization: sample Characteristics, Percent by Column
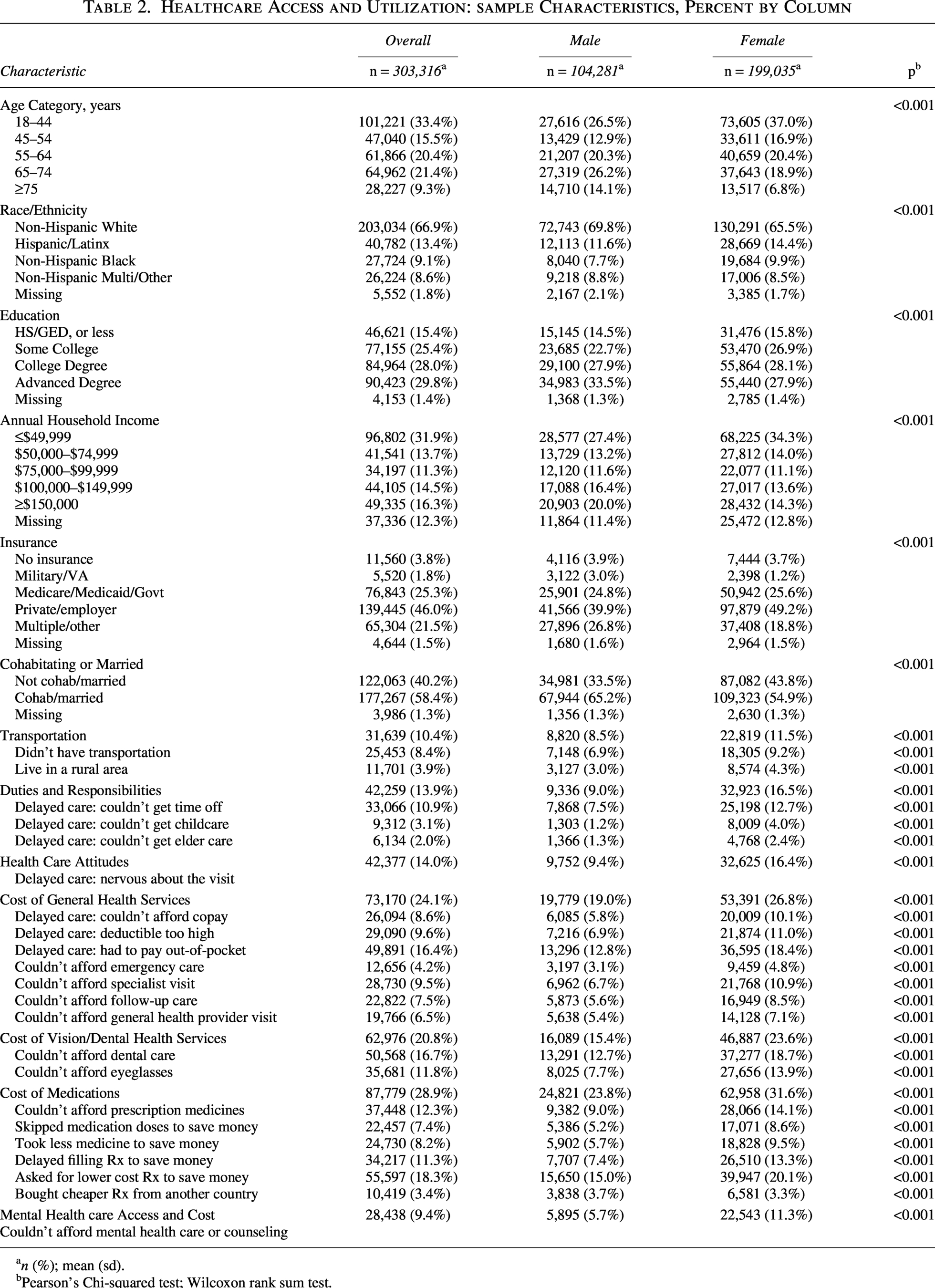
n (%); mean (sd).
Pearson’s Chi-squared test; Wilcoxon rank sum test.
Data analysis
Table 2 displays proportional differences among men and women across domains and demographic characteristics, evaluated via Chi-squared tests. Those missing sexes were omitted. Of 250,640 responses analyzed, 85,726 were male and 164,914 female. Odds ratios were derived from multivariable binary logistic regression models stratified by sex for each domain. Results are shown in Supplementary Tables S2A and S2B.
Results
ORs for each sex are shown in Figure 2 with significant differences marked by asterisks. Compared with those with a high school education or less, females with some college, a college degree, or an advanced degree had significantly greater odds of barriers than males at the same education level in responsibilities (OR 1.18, 95% CI: 1.08–1.29, p < 0.001; OR 1.22, 95% CI: 1.11–1.34, p < 0.011; OR 1.15, 95% CI: 1.05–1.27, p = 0.004, respectively), general health care costs (OR 1.15, 95% CI: 1.01–1.23, p < 0.001; OR 1.12, 95% CI: 1.04–1.20, p = 0.002; OR 1.14, 95% CI: 1.06–1.23, p < 0.001), medication costs (OR 1.2, 95% CI: 1.13–1.28, p < 0.001; OR 1.11, 95% CI: 1.04–1.18, p = 0.002; OR 1.09, 95% CI: 1.02–1.17, p = 0.011), and mental health care costs (OR 1.3, 95% CI: 1.17–1.43, p < 0.001; OR 1.37, 95% CI: 1.23–1.52, p < 0.001; OR 1.47, 95% CI: 1.30–1.65, p < 0.001). Compared with respondents without insurance, females with military/VA, Medicare/Medicaid, and private insurance reported barriers in responsibilities—the inability to secure time off, childcare, or elder care—more often than males with equivalent insurance types (OR 1.33, 95% CI: 1.08–1.64, p = 0.006; OR 1.31, 95% CI: 1.15–1.49, p < 0.001; OR 1.26, 95% CI: 1.11–1.43, p < 0.001, respectively).
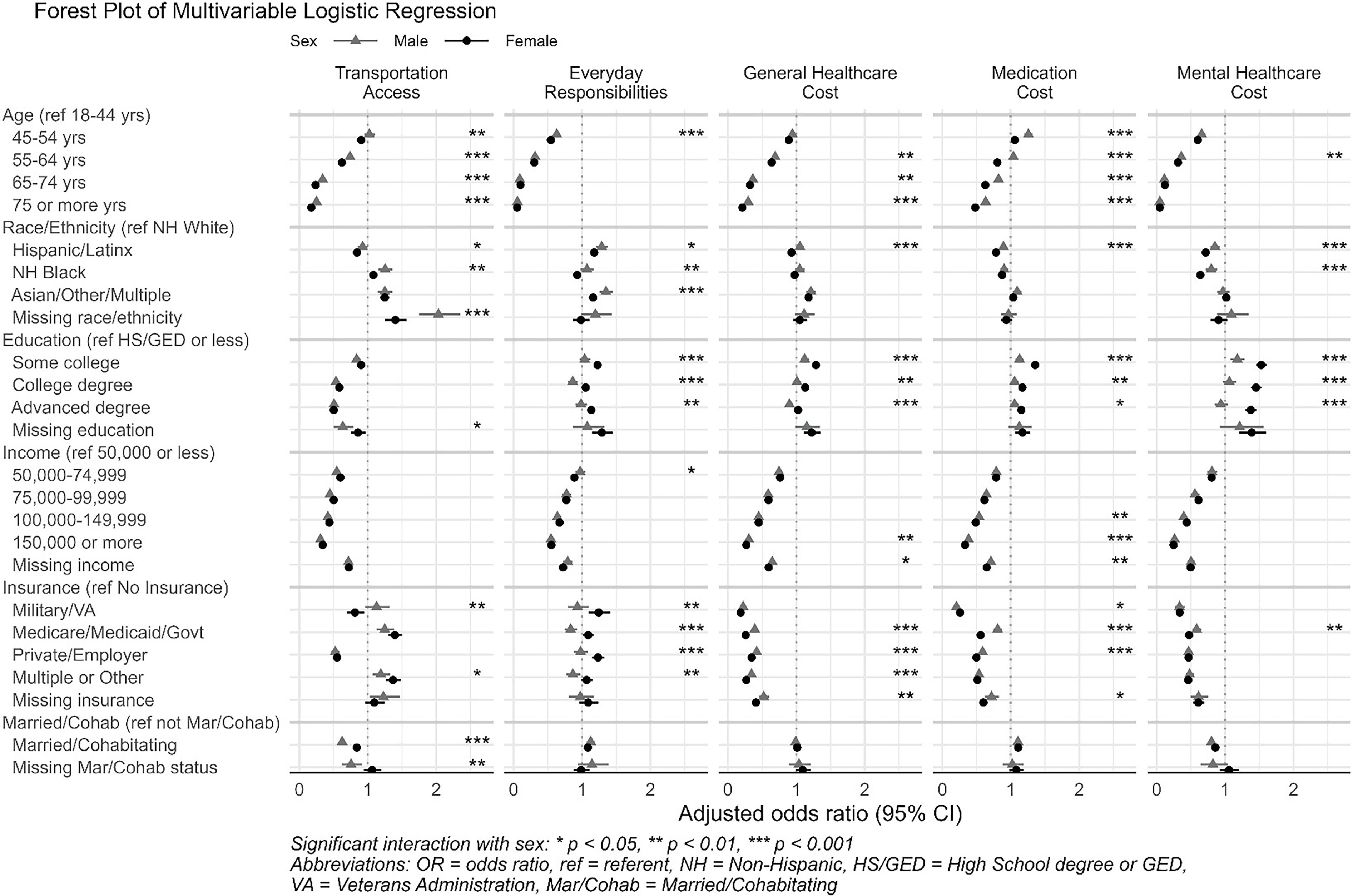
Health care access and utilization among men and women by domain.
Discussion
Our analysis suggests that barriers to seeking care differ between men and women, and thus, efforts and studies to improve access should consider addressing these specific barriers. The Health Care Access and Utilization survey provides survey responses available for analysis. This is supported by the work of Huang et al., 21 which demonstrated similar barriers in a socioecological model for vulnerable women including transportation, medical benefits and coverage, and management of multiple conditions. A finding from Bataineh, Devlin and Barham in Unmet health care and health care utilization in Canada 22 found that men under the care of doctors had fewer unmet medical needs but, in the women-only group, increasing visits to physicians did not result in meeting more health care needs. Even after increased visits to providers, women continued to report that their health care needs were not met. So, it is not access alone accounting for the difference, and the exploration of this gap remains. 22
Use Case 3: A Condition That Affects Women Uniquely–Postpartum Hemorrhage
Postpartum hemorrhage (PPH) occurs in approximately 1%–3% of hospital deliveries globally and is the leading cause of obstetric morbidity and mortality, 23 accounting for 12.1% of maternal deaths in the United States. 24,25 Although prevalence varies greatly across patient populations, studies have shown incidence is increasing. Risk factors include advanced maternal age, diabetes or gestational diabetes, hypertension, preeclampsia, multiple gestation, a history of leiomyoma, and placental disorders such as placenta previa or placental abruption. Studies indicate moderate or severe anemia at the time of delivery to be an additional risk factor. Though these indicators are widely acknowledged, the rates and incidence remain concerning if not critical worldwide.
Methods
We began by first retrieving records of delivery and available records of gestation week or trimester. Delivery records were omitted where gestation week did not align with delivery date, or where a miscarriage was recorded within 270 days preceding each delivery date. We then calculated time elapsed between each consecutive delivery date after sorting chronologically. Because EHR includes billing records, EHR encounters, diagnoses, and other recorded data, we used a stepwise approach, keeping the first record among those within 30 days, then 60, 90, 180, and 270 days, recalculating elapsed days between records and assessing the distribution of elapsed days among all participants after each step. After the final step, 97% of consecutive delivery dates were separated by 365 days or more.
We then divided the 270 days preceding each participant’s delivery date into 39 date variables representing 7-day chronological thresholds for each week of pregnancy. After querying metrics for hemoglobin (Hb) and hematocrit (HCT) from available lab results, we omitted outliers using Tukey’s method by unit of measure, then converted values where units of measure differed. We designated 39 separate variables for each lab value by week and created an algorithm to sort lab results by date into their respective slots according to our 39 date thresholds. If Hb was not available, we calculated Hb from HCT (Hb = HCT/3). We calculated a median for time slots if multiple values were encountered. Among those participants with multiple pregnancies, we analyzed those with the greatest frequency of Hb or HCT lab results. Those with Hb < 11 g/dL within 4 weeks of delivery were marked as evidence of anemia.
We derived a binary variable indicating postpartum hemorrhage from EHR with a recorded date within 12 weeks of each participant’s delivery date.
Other risk factors and conditions
From available EHR within 270 days of delivery, we created binary variables to identify: (1) those with multiple gestation, (2) those with a record of preeclampsia, (3) those with a record of gestational diabetes, (4) those with a record of placenta previa, and (5) those with a record of placental abruption. We created a binary variable indicating obesity during pregnancy from available BMI within 635 days preceding delivery and recorded observations or conditions within 270 days preceding the delivery date. A binary variable indicating cesarean delivery and a variable identifying those with a history of leiomyoma (uterine fibroids) were also derived from available EHR.
We limited our analysis to participants with at least 2 years of available EHR and were 18–44 years of age at the time of pregnancy.
Results
Characteristics of those analyzed are shown in Table 3. Of the 10,852 pregnancies we analyzed, 5.7% included instances of PPH. The majority, 59.9%, were 25–34 years of age, and 46.7% identified as Hispanic/Latina. Those with less than $75,000 annual household income comprised 47.0% of the sample, and 52.7% were insured by Medicaid, Medicare, or other public insurance. Of those analyzed, 18.9% were considered anemic within 4 weeks of delivery, 20.8% were identified as obese during pregnancy, and 16.0% of deliveries were cesarean. Multiple gestations characterized 2.6% of pregnancies, and 4.6% of those analyzed had instances of preeclampsia.
Postpartum Hemorrhage: Sample Characteristics, Percent by Column
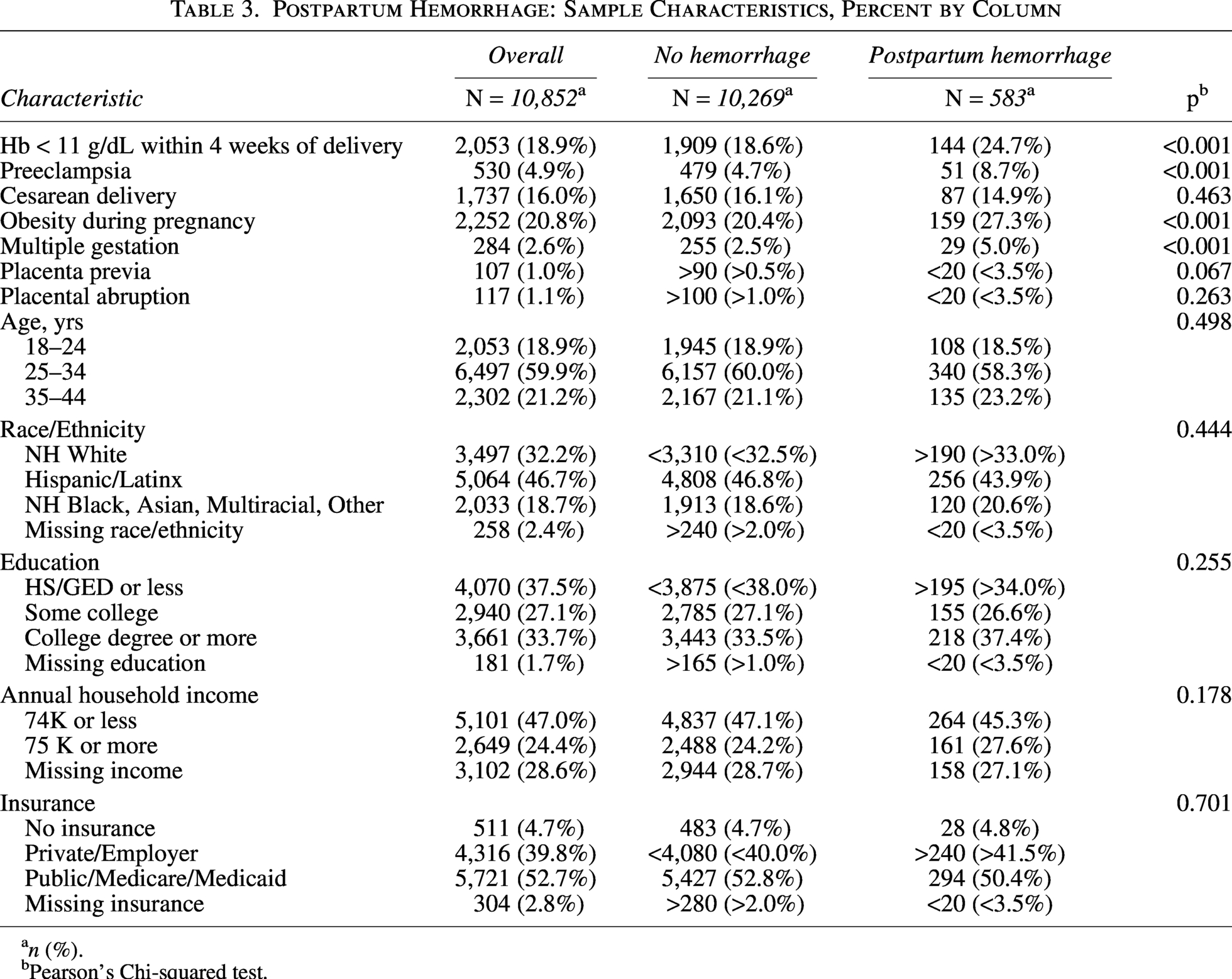
n (%).
Pearson’s Chi-squared test.
Univariable and multivariable model results are shown in Supplementary Table S3. Univariable models indicated twice the odds of PPH for multiple gestations (unadjusted OR 2.06, 95% CI: 1.36–2.99, p < 0.001) when compared with singleton pregnancies, and twice the odds of PPH for those with preeclampsia (unadjusted OR 1.96, 95% CI: 1.43–2.62, p < 0.001). Evidence of anemia in the last 4 weeks of gestation (Hb < 11) was associated with significantly higher odds of PPH (unadjusted OR 1.44, 95% CI: 1.18–1.71, p < 0.001). Compared to those with other BMI during gestation, those who were obese had greater odds of PPH (unadjusted OR 1.46, 95% CI: 1.21–1.76, p < 0.001).
The multivariable model identified a significant association of anemia with higher odds of PPH (OR 1.45, 95% CI: 1.18–1.77, p < 0.001) after adjusting for covariates. Obesity was also linked with higher odds of PPH (OR 1.51, 95% CI: 1.24–1.83, p < 0.001). Other risk factors significantly associated with PPH in the multivariable model were preeclampsia (OR 1.76, 95% CI: 1.28–2.38, p < 0.001), multiple gestation (OR 1.74, 95% CI: 1.14–2.55, p < 0.001), and placenta previa (OR 1.80, 95% CI: 0.87–3.33, p = 0.080). A forest plot of multivariable logistic regression is shown in Figure 3.
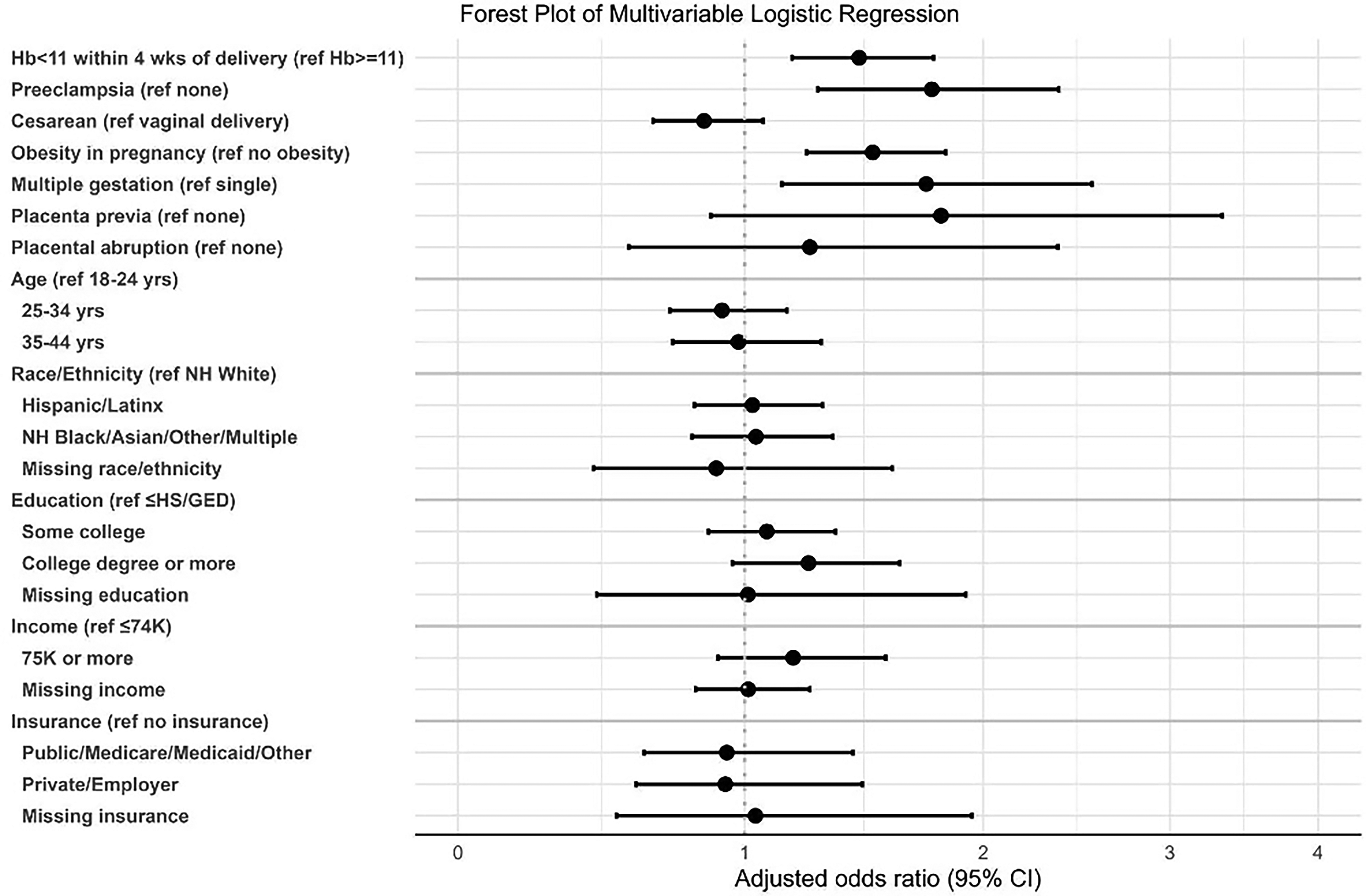
Model results, postpartum hemorrhage.
Discussion
In this cohort of more than 10,000 pregnancies, PPH occurred in 5.7% of deliveries. We identified several independent risk factors, including anemia within 4 weeks of delivery, obesity, preeclampsia, and multiple gestation. These conditions were associated with 45%–76% higher odds of PPH after adjustment, underscoring their clinical importance. Our findings are consistent with prior studies demonstrating that anemia and obesity increase vulnerability to obstetric complications. 23,24 The alignment of our results with existing evidence strengthens the biological plausibility of these risk factors and highlights areas where clinical interventions may have the greatest impact.
This study adds value by analyzing a large, socioeconomically diverse cohort, including populations disproportionately affected by maternal morbidity. While these factors are well understood, the issue and sequela from PPH remain critical factors today, especially in minority populations. These findings suggest that systematic screening and management of anemia, weight, and hypertensive disorders, along with tailored delivery planning for multiple gestations, may reduce the burden of PPH and advance maternal health.
Conclusion
In this article, we demonstrate the use of the All of Us dataset for conditions that affect women differently, disproportionately, and uniquely, and describe three use cases, their analysis, and findings. We anticipate that rigorous use of this dataset can provide a structured roadmap for advancing women’s health research, particularly in the current context of resources and funding. Accelerating research in this area represents a critical scientific priority, and leveraging an existing, freely accessible dataset offers a cost-effective approach to conserving time and resources while generating evidence with the potential to improve health outcomes and save lives.
Limitations
While researchers may only access the dataset if their institution has a signed Data Use and Registration Agreement (DURA) in place, requesting a DURA is straightforward and free. Currently, nearly 1,200 DURAs are in place. Registering as a Researcher requires identity verification and a set of ethical training modules. Using the dataset requires knowledge of Python, SAS, or R; however, tutorials and educational resources are available for help with programming. Users are allocated $300 in initial credits per registered Workbench Researcher. The program is digital and cloud-based—a potential limitation for participants in areas without internet or computer access. Information on this dataset can be found at www.researchallofus.org.
Authors’ Contributions
E.C., S.S.J., C.C., E.J.O., and N.P. contributed to conceptualizing and supervising this program. J.F., A.Z., S.T.M., K.C., H.J., Y.Z., E.W.K., and H.A.C., provided input and revisions. All authors have reviewed this research article and approved this version for publication.
Footnotes
Acknowledgments
The authors would like to thank the All of Us Research Program, participants who contributed their data, and Next Generation Partners Council for Women’s Health. Northwell Health’s Katz Institute for Women’s Health advances women’s health through specialized clinical care and robust, sex-specific research throughout every stage of life.
Funding Information
This work was supported by the Katz Institute for Women’s Health Foundation at Northwell and the Next Generation Partners Council for Women’s Health. Dr. Cohn, Nakisa Pourkey, S. Scott Jones are supported by National Institutes of Health Grant Number OT2OD038104-1S1.
Author Disclosure Statements
The authors have no conflicts of interest.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.