
Abstract
Background:
Despite evidence that hookah poses similar risks to other tobacco products, it is often (mis)perceived as less harmful. Few studies have investigated the prevalence and correlates of hookah use during pregnancy. The present study sought to characterize the prevalence of and sociodemographic and psychosocial characteristics associated with hookah use during pregnancy and 3 months prior (i.e., preconception) in a large sample of pregnant women.
Materials and Methods:
Pregnant women (N = 900) from the Northeast United States completed a telephone screener assessing sociodemographics, mental health, and substance use during pregnancy and preconception. Women were categorized into three groups: any hookah use, cigarette and other tobacco (C&OT) use, and no tobacco use. Generalized linear models were used to calculate risk ratios.
Results:
Approximately 8.8% (n = 79) of the women in our sample reported hookah use during preconception and pregnancy, and the majority (n = 57) reported exclusive hookah use. Women who identified as Hispanic/Latinx were more than 2.5 times as likely to report hookah use than C&OT or no tobacco use. Women who drank alcohol during pregnancy were more than 1.5 times as likely to report hookah use than C&OT or no tobacco use.
Conclusions:
The prevalence of hookah during pregnancy and preconception in the present socioeconomically disadvantaged and ethnoracially varied sample is notably higher than in previous samples estimated using nationally representative data. Women who use hookah during pregnancy demonstrate a distinct sociodemographic and psychosocial profile, which suggests potential targets for intervention, such as alcohol use.
Prevalence and Problem
Waterpipe tobacco, or hookah, is a form of combustible tobacco traditionally used in the Middle East and India that has grown in popularity in the United States over the past two decades. 1,2 To use, hookah tobacco is heated with charcoal in the head (bowl) of the waterpipe. Smoke then passes through water in the base of the apparatus and is inhaled through a pipe-like mouthpiece. 3 Hookah tobacco is often sweetened and flavored, contributing to its appeal. 4 Despite evidence that hookah smoke contains numerous toxins, hookah is commonly (mis)perceived as less harmful than other forms of tobacco, which is possibly related to its flavoring and water “filtering.” 5,6 In fact, hookah use poses similar health risks to other tobacco products. 3,7 Perinatal cigarette use, the most common form of tobacco use in the perinatal period, 8 is causally associated with increased risk of maternal and infant morbidity and mortality. 9,10 Although under-researched, a small number of studies suggest similar impacts of prenatal hookah exposure on maternal and infant morbidity. 11 –14 The current study expands upon this limited literature by examining the prevalence and correlates of hookah use during pregnancy and in the 3 months before (referred to as “preconception”).
Prevalence of hookah use in the perinatal period
Despite suggestive evidence of adverse impacts of hookah use in pregnancy on maternal and offspring health, only a small number of studies to date have investigated prevalence of hookah use in pregnant people in the United States. Data from the 2013–2014 Population Assessment of Tobacco and Health (PATH) survey revealed that 6.5% of women of reproductive age (aged 15–44) reported current hookah use (i.e., “now using someday or everyday”). 15 The estimated prevalence of current (established or experimental) hookah use among pregnant women who completed the PATH survey in 2013–2014 was 2.5%, with rates of use at 12.4% among pregnant women who also reported use of combustible cigarettes. 8 Similarly, our group found rates of use of 11.0% in a New England pregnancy cohort oversampled for combustible cigarette use. 4 Finally, among postpartum women surveyed 2–6 months after delivery who were included in the 2016–2020 Centers for Disease Control and Prevention’s Pregnancy Risk Assessment Monitoring System (PRAMS), 4.1% reported hookah use in the past 2 years; although, it is unclear what proportion of these individuals used hookah during pregnancy and preconception versus postpartum. 16
Correlates of Hookah Use
Among women of reproductive age, current cigarette smoking and younger age (i.e., 15–24 years) were the strongest predictors of current hookah use. White race, higher education, and other substance use have also been associated with increased likelihood of hookah use in this population. 15 Interestingly, in a large sample of U.S. adults, younger adults and those with higher levels of education (i.e., a college degree) perceived hookah as less harmful, 5 suggesting that sociodemographic differences may be explained, at least in part, by differential perceptions of harm. However, in a smaller sample of pregnant women, perceptions of harm were not significantly associated with prenatal hookah use. 4 With regard to postpartum mental health, the odds of experiencing postpartum depression symptoms were 20% greater for mothers with past two-year hookah use compared with nonusers. 16
Kurti et al. 8 assessed correlates of hookah use during pregnancy and found that the odds of current hookah use were significantly greater among those who reported current cigarette or illicit substance use than those who reported former nonuse. They also found that the likelihood of hookah use significantly decreased with increased gestational age. No other significant sociodemographic predictors of hookah users were identified among this pregnant sample. 8 Accordingly, very little is known to date about the prevalence and correlates of hookah use in this specific population. Further research is warranted in this area to better inform tobacco screening and prevention efforts.
The Present Study
The current study expands on recent literature by using a large sample of pregnant women assessed between 2015 and 2018. Specifically, we measured hookah use in a sample of 900 pregnant women via a telephone screening survey that was part of two larger studies of tobacco use during pregnancy. Data were analyzed to answer the following questions: (1) What is the prevalence of hookah use in preconception and/or pregnancy? (2) Do sociodemographic characteristics predict prenatal/preconception hookah use versus cigarette and other tobacco (C&OT) use, and no tobacco use? (3) Do mental health conditions and use of other substances (e.g., alcohol, marijuana) predict prenatal/preconception hookah use versus C&OT use and no tobacco?
Methods
Participants
A total of 900 pregnant women completed a telephone survey between 2015 and 2018. Respondents were categorized into three groups: hookah use, C&OT use (no hookah), and no tobacco use.
Procedures
Participants were recruited for the telephone survey through active outreach at a single urban clinic serving low-income individuals in New England, as well as through flyers and advertisements in local obstetric offices and community centers. Participants provided verbal consent to take part in the telephone survey that assessed eligibility for two larger studies on the effects of maternal cigarette smoking on fetal and infant neurodevelopment. The survey was conducted prior to enrollment in the larger studies. During the telephone survey, participants answered a range of questions covering topics such as tobacco or nicotine use, substance and alcohol consumption, mental health, medications, and demographic information. The study was approved by the Women and Infants Hospital Institutional Review Board.
Measures
Demographic and health characteristics
We assessed demographic variables including maternal age (at the time of the survey), size of the household, number of children, income level, education level, and race/ethnicity. Income and education were analyzed as dichotomous variables: income (<$30,000 versus ≥$30,000) and education (<bachelor’s versus ≥bachelor’s). Obstetric factors were also assessed, including estimated gestational age at the time of the survey, which was determined based on the participant’s report of their last menstrual period or ultrasound.
During the survey, participants were asked to select the race and ethnicity with which they most closely identify, with the option to choose multiple categories. Responses were recoded as appropriate (e.g., if participants identified with two racial groups, they were assigned to the “multiracial” category). Race and ethnicity were analyzed as separate variables. Race variables were Black, White, Asian American/Pacific Islander, Native American/Alaska Native, another race, or multiple races. Ethnicity categories were Hispanic/Latinx versus non-Hispanic/Latinx. Participants who identified with more than one racial category or selected “multiracial” were classified as multiracial.
Prenatal/preconception hookah use
To assess hookah use before and during pregnancy, respondents were asked, “Are you currently using hookah or water pipe?” If participants responded no to current use, they were asked, “Did you use hookah or water pipe during this pregnancy or in the 3 months prior to pregnancy?” Participants were included in the “hookah” category if they responded yes to either question, that is, if they reported any hookah use in the 3 months before pregnancy and/or during pregnancy, regardless of whether they also used other tobacco products.
Prenatal/preconception C&OT/nicotine product use
To assess cigarette use, all participants were asked, “Do you smoke cigarettes?” If they responded no, they were then asked, “Did you smoke at all during this pregnancy or in the 3 months prior to the pregnancy?” To assess other tobacco/nicotine use, all participants were asked if they used any of the following currently, and if not currently, during this pregnancy or the 3 months prior: e-cigarettes, vaping, e-hookah or hookah pens, e-juice, vape pipes or pens, ENDS; bidis, cloves, or other herbal cigarettes; cigarillos or filtered cigars; cigars; pipes; chewing tobacco, snus, or snuff; nicotine lozenges, gum or patches; any other nicotine or tobacco products. Respondents were included in the C&OT use category if they reported any cigarette use and/or other tobacco product use from the list above during preconception and/or pregnancy, but did not use hookah. Participants were only included in the “no tobacco use” category if they did not use any tobacco products in preconception and/or pregnancy.
Mental health
All participants were asked both of the following questions: “During your pregnancy, did you ever feel depressed, down, sad, irritable, or lose interest in things you usually enjoy?” and “Did you feel like this most of the day, nearly every day, for 2 weeks or more?” Participants were considered to have experienced depressive symptoms if they responded “yes” to both questions. Information on depressive symptoms prior to pregnancy was not collected. In addition, participants were asked whether they had ever received a diagnosis of bipolar disorder, schizophrenia, schizoaffective disorder, or psychosis. Those who responded “yes” to any of these diagnoses were categorized as having a serious psychiatric diagnosis.
Alcohol, marijuana, and other substance use
Participants were asked about alcohol use during pregnancy and marijuana and other substance use in the 3 months prior to pregnancy. Participants who answered “yes” to the question, “Have you consumed any alcohol during this pregnancy, including the weeks before you knew you were pregnant?” were classified as having used alcohol in pregnancy. Participants were only asked about marijuana and other illicit substance use during the 3 months before pregnancy. If participants answered “yes” to the question, “In the 3 months prior to this pregnancy, did you use marijuana?” they were considered to have used marijuana. Following questions on alcohol, tobacco, and marijuana use, respondents were also asked, “In the 3 months prior to this pregnancy, did you use any other drugs?” Those who answered “yes” were categorized as having used other drugs in the preconception period.
Statistical analysis
Data were analyzed using Stata v. 15.1 to generate means and frequencies of all study variables and examine associations between hookah use and sociodemographic factors. Listwise deletion was applied to handle missing data. We conducted two sets of comparisons. First, we compared participants who reported using any hookah (n = 79) to participants who used no tobacco products (n = 680). Second, we compared participants who reported using any hookah (n = 79) to those who exclusively reported C&OT use (and no hookah; n = 141). We used generalized linear models with a binomial distribution and log link function (log-binomial model) and exponentiated results to estimate associations between the sociodemographic predictor variables and the likelihood of hookah use. Maternal age was modeled as a continuous variable centered at its mean (27.17 years). Log-binomial models allow for the direct estimation of risk ratios, which are more interpretable than the odds ratios generated by a logistic regression model when the outcome is not rare. 17 The reported coefficients can be interpreted as the relative risk (RR) of hookah use (compared with either other tobacco product use or no tobacco product use) associated with each sociodemographic, mental health, or substance use predictor variable.
Results
Prevalence of preconception/prenatal hookah use
In our sample, 8.8% (n = 79) of pregnant women reported prenatal/preconception hookah use, 15.7% (n = 141) reported C&OT use (no hookah), and 75.6% (n = 680) reported no tobacco use (see Table 1). Of the n = 79 women who reported hookah use, 72.2% (n = 57) reported sole hookah use with no other tobacco use, and 27.8% (n = 22) reported using hookah along with C&OT use. In the analyses reported below, the hookah group refers to the 8.8% (n = 79) of participants who reported hookah use regardless of other tobacco use.
Means and Frequencies of Sociodemographic and Psychosocial Characteristics
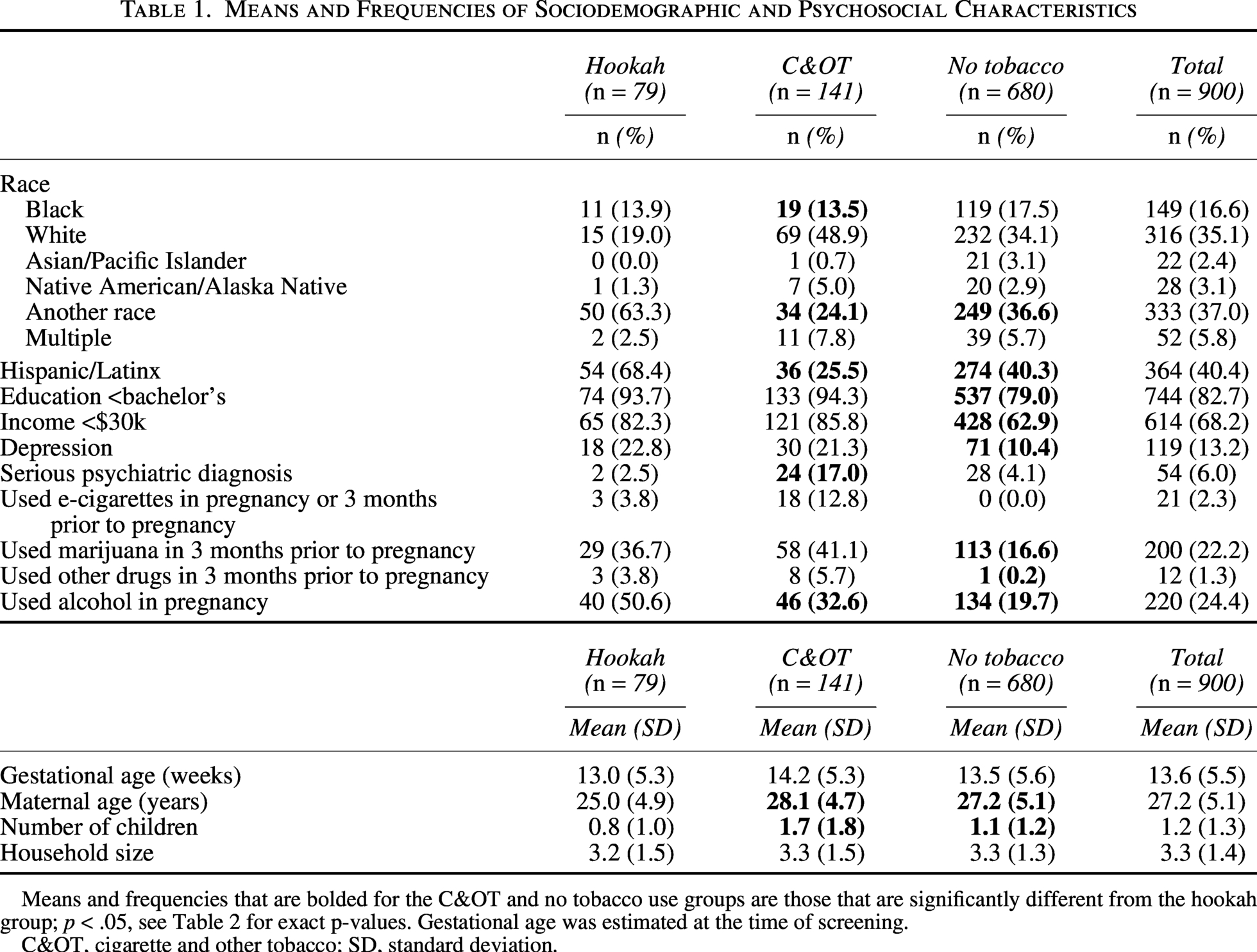
Means and frequencies that are bolded for the C&OT and no tobacco use groups are those that are significantly different from the hookah group; p < .05, see Table 2 for exact p-values. Gestational age was estimated at the time of screening.
C&OT, cigarette and other tobacco; SD, standard deviation.
Sociodemographic characteristics
The average maternal age in our sample was 27.2 years (SD = 5.1), and the average gestational age was 13.6 weeks (SD = 5.5). Approximately 35% of the sample identified as White, and 40.4% reported their ethnicity as Hispanic/Latinx. Thirty-seven percent of the sample identified as another race. Of those who identified as another race, approximately 70% identified their ethnicity as Hispanic/Latinx. The sample was predominantly of lower income (68.2%), and 82.7% had less than a bachelor’s education.
Sociodemographic correlates of preconception/prenatal hookah use
Hookah versus C&OT use only
Relative to White participants, Black participants were 2.05 times as likely to report using preconception/prenatal hookah compared with C&OT use (p = 0.032), and those who identified as another race were 3.33 times as likely to report hookah use (p < 0.001). Relative to those who did not report Hispanic/Latinx identity, participants who reported Hispanic/Latinx identity were 3.12 times as likely to report hookah use compared with C&OT use (p < 0.001). Each additional year of age over 27 was associated with an 8% decrease in the risk of hookah use compared with C&OT use (RR = 0.92, p < 0.001). Having more children was also associated with decreased risk of hookah use compared with C&OT use (RR = 0.72, p < 0.001; see Table 2).
Sociodemographic and Psychosocial Correlates of Hookah Use During Pregnancy (Unadjusted)
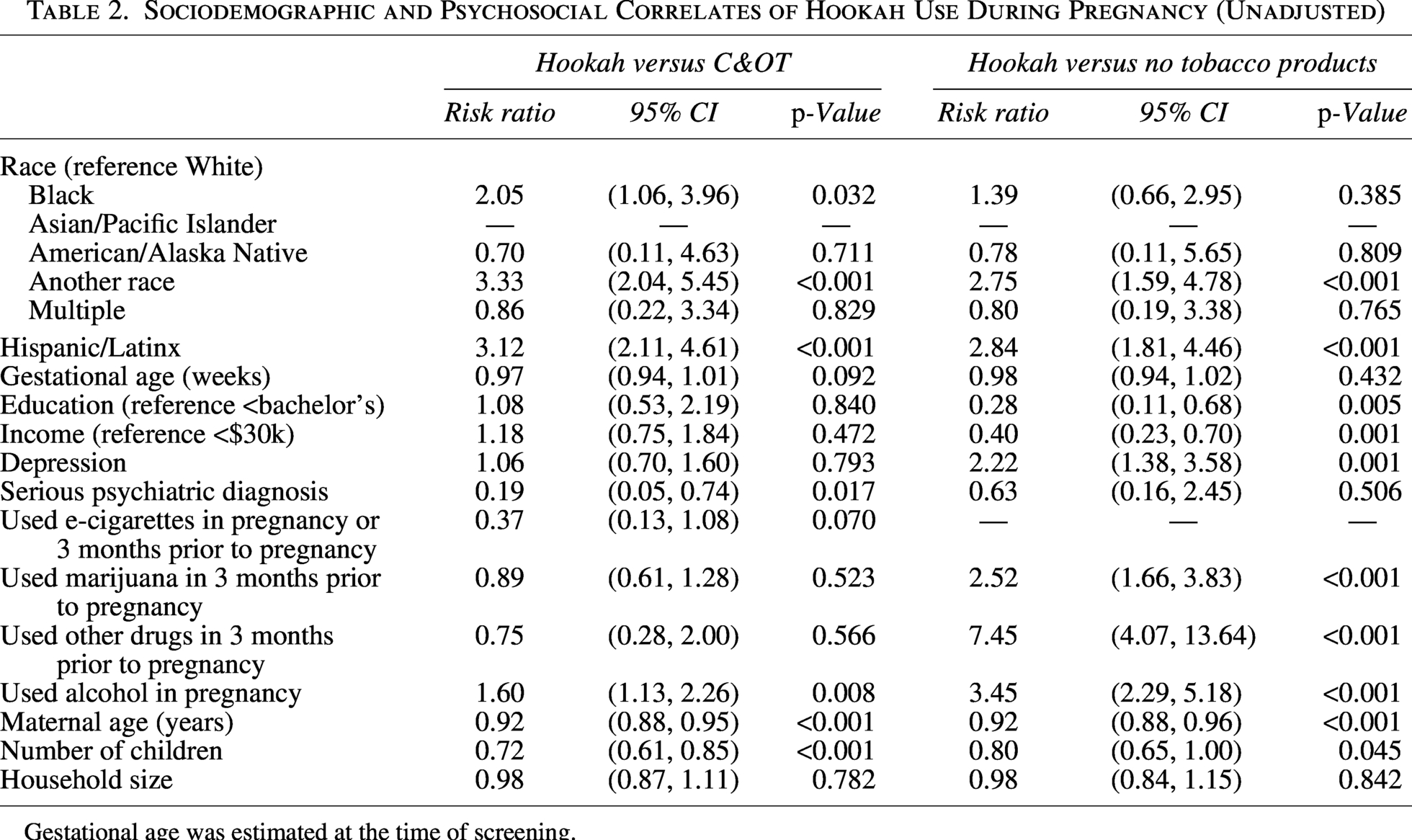
Gestational age was estimated at the time of screening.
Hookah versus no tobacco products
Relative to participants who identified as White, participants who identified with another race were 2.75 times as likely to report hookah use compared with no tobacco product use (p < 0.001), and relative to those who identified as non-Hispanic/Latinx, those who identified as Hispanic/Latinx were 2.84 times as likely to use hookah versus no tobacco products (p < 0.001). Relative to participants reporting annual income greater than or equal to $30,000, those reporting annual income less than $30,000 were 2.51 times as likely to report using hookah compared with no tobacco products (p = 0.001). Compared to those with a bachelor’s education or higher, participants with less than a bachelor’s education were 3.58 times as likely to report using hookah compared with no tobacco products (p = 0.005). Each additional year of age over 27 was associated with an 8% decrease in the risk of hookah use compared with no tobacco product use (RR = 0.92, p < 0.001). Having more children was also associated with decreased risk of hookah use compared with no tobacco product use (RR = 0.80, p = 0.045).
Concurrent mental health and substance use
Six percent of the sample reported serious psychiatric diagnoses, and 13% reported experiencing depression during pregnancy. Approximately one in five participants reported using marijuana in 3 months prior to pregnancy, and a quarter reported using alcohol during pregnancy. Less than 2% reported using other drugs in 3 months prior to pregnancy. Among those who smoked, participants reported smoking an average of seven cigarettes per day (SD = 5.2).
Mental health and substance use correlates of prenatal/preconception hookah use
Hookah versus C&OT use only
Participants with serious psychiatric diagnoses (e.g., bipolar disorder, psychosis) were 0.19 times as likely to use hookah compared with C&OT use than those without serious psychiatric diagnoses (p = 0.017). Participants who used alcohol during pregnancy were 1.6 times as likely to report also using hookah compared with C&OT than those who did not use alcohol during pregnancy (p = 0.008).
Hookah versus no tobacco products
Participants who reported depression during pregnancy were 2.22 times as likely to report hookah use compared with no tobacco product use than those who did not report depression during pregnancy (p = 0.001). Relative to participants who did not use, participants who used marijuana in the three months prior to pregnancy (RR = 2.52, p < 0.001), those who used drugs other than tobacco, alcohol and marijuana in 3 months prior to pregnancy (RR = 7.45, p < 0.001), and those who used alcohol during pregnancy (RR = 3.45, p < 0.001) were all more likely to use hookah compared with no tobacco products.
Discussion
Summary of present findings
In a large sample of pregnant women from New England, the prevalence of hookah use during pregnancy and preconception was 8.8%, notably higher than the current prevalence rates of hookah use in nationally representative samples of reproductive age 15 and pregnant women. 8 Of note, the majority of women in the present sample who reported hookah use were exclusively using hookah, that is, they did not report use of other tobacco products. Women who used hookah during pregnancy and preconception showed distinct psychosocial, mental health, and substance co-use characteristics. Relative to White women, Black women were more likely to report hookah use than C&OT use. Women who were younger (versus older) in age, identified as another race (versus White), and identified as Hispanic/Latinx (versus non-Hispanic/Latinx) were more likely to report hookah use than C&OT or no tobacco use. Our findings complement prior studies demonstrating that younger age and Hispanic/Latinx identity were associated with a greater likelihood of hookah use in U.S. adults and, more specifically, reproductive-age women. 5,15 In contrast to Lopez et al., 15 we did not find that the White race was significantly associated with increased likelihood of hookah use, a finding that likely reflects the unique composition of our sample.
Additionally, compared with those with higher income, pregnant individuals with lower income were more likely to report hookah use than no tobacco use during pregnancy and preconception. Prior studies of U.S. adults have similarly demonstrated greater risk of hookah use among individuals with low income, 18,19 albeit findings do vary. 20 It is possible that participants with lower income tend to live in neighborhoods where hookah is more readily accessible and that increased access leads to greater social acceptability and, thereby, greater use. Prior research has demonstrated that accessibility is positively associated with acceptability and use for other tobacco products. 21,22 With regard to substance use, rates of marijuana and alcohol use were substantially higher than rates of other drug use. Women who endorsed marijuana, alcohol, or other drugs were more likely to report hookah use than no tobacco use, a finding that is reflective of issues with polysubstance use in pregnancy. 23 Women who drank alcohol during pregnancy were also significantly more likely to report hookah use than C&OT. Overall, findings suggest a high comorbidity between hookah use and alcohol use during pregnancy, two substances which are often used socially. 24,25
The high prevalence rate of hookah use in the present study may be attributable to several factors. First, this may be a reflection of the sample’s young age (M age = 27.2 years); the mean age of the present sample is slightly younger than prior samples where the majority of participants were over 25 years old. 8,15 Prior studies have demonstrated that younger age is a correlate of hookah use 15 ; additionally, research in nonpregnant samples has found that younger individuals perceive hookah as less harmful, 5 perhaps accounting for their continued use during pregnancy. Second, the average gestational age of the present sample (13.6 weeks) is lower than in other samples (21 weeks), 8 which may contribute to higher prevalence rates given known decreases in tobacco and substance use over the course of pregnancy. 26 Greater substance use earlier in pregnancy may be attributable to lack of awareness of their pregnancy, misperceptions of substance use as less harmful at the start of pregnancy, lesser fear of public judgment, and/or difficulty quitting. Third, Kurti et al. 8 utilized data from 2013 to 2014 when estimating the prevalence rate of hookah use during pregnancy. Data for the present study were collected a few years later (2015–2018), during which time hookah increased in popularity. 2 Last, the current sample is not a nationally representative sample, and participants were oversampled for cigarette use during recruitment. Accordingly, it makes sense that the hookah prevalence rate in the current sample is approaching the hookah prevalence rate (12.4%) of pregnant women who also used combustible cigarettes. 8
Strengths and limitations
The present study has several notable strengths including assessing a novel and understudied health-risk behavior during pregnancy. First, it is one of three studies to date that assess the prevalence of hookah use during preconception and pregnancy. 4,8 In doing so, this study contributes to a small but growing literature on preferences, perceptions of risk, and reasons for hookah use during pregnancy and preconception. 4,8,27,28 Second, while not nationally representative, the present study recruited a variety of women from a range of racial, ethnic, and socioeconomic groups. In addition, the present sample of n = 900 is notably larger than samples in prior studies of n = 388 8 and n = 100. 4
Still, the present findings should be interpreted cautiously in light of several limitations. Given that tobacco co-use and polytobacco use are common, 8,23 and the present sample was oversampled for cigarette use, the prevalence of hookah use in the present sample may be overestimated. Participants were also asked if they used hookah and other substances during the “3 months prior to pregnancy OR during pregnancy,” which does not provide descriptive information about the specific timing or frequency of hookah use in the perinatal period. Last, the present study assessed substance use via self-report, which is subject to both recall and social desirability bias and may lead to underreporting.
Clinical implications and future directions
Findings from our study suggest that hookah use is more common in pregnant populations than previously reported, particularly among women reporting C&OT use and other substances, which directly impacts clinical care and routine screening for nicotine/tobacco use during preconception and pregnancy. Based on the prevalence rates in this sample, it is encouraged that tobacco/nicotine screenings should include hookah use, co-use, as well as addressing the belief that hookah is safer than combustible cigarettes. Clinicians should also consider assessing return to use in the postpartum period and discussing health implications for both mother and baby. Future directions should include assessing how and when hookah is used during pregnancy, studying return to hookah use in the postpartum, and developing interventions for hookah use cessation throughout the perinatal period.
Authors’ Contributions
L.E.L.: Conceptualization, methodology, validation, visualization, writing—original draft, and writing—review and editing. N.A.S.: Data curation, formal analysis, methodology, and writing—original draft. L.G.W. and G.E.G.: Writing—original draft and writing—review and editing. L.R.S.: Conceptualization, funding acquisition, methodology, investigation, supervision, and writing—review and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the