
Abstract
Background:
Cervical cancer remains a significant health concern for women, with the U.S. Preventive Services Task Force (USPSTF) recommending routine screenings for women ages 21–65 years. This study aims to evaluate cervical cancer screening rates among active-duty servicewomen (ADSW) in the U.S. military and assess the proportion meeting USPSTF guidelines during fiscal year (FY) 2017–2022.
Methods:
We conducted a retrospective cohort study of ADSW ages 21–60 years screened for cervical cancer in FY 2017, who were then followed through FY 2022. Excluded from the study were reservists, National Guard, and Coast Guard personnel. Screening compliance was determined based on the USPSTF age-based guidelines. We performed descriptive statistics and logistic regression to examine screening rates and compliance likelihood.
Results:
We identified 212,081 ADSW during FY 2017 (62% were ages 21–29 years and 38% were ages 30–60 years). Overall, 76.5% of eligible ADSW received cervical cancer screenings. ADSW in the 30–60 years age group were less likely to undergo screening (odds ratio [OR]: 0.73, 95% confidence intervals [CI]: 0.71–0.74) compared with those aged 21–29 years. Similarly, senior officers showed lower screening rates compared with junior-enlisted personnel (OR: 0.78, 95% CI: 0.74–0.82). Compliance with USPSTF guidelines varied by age group, race, and military branch, with Black (OR: 0.88, 95% CI: 0.83–0.93), Asian American, and Pacific Islanders (OR: 0.85, 95% CI: 0.77–0.93), and those in the Air Force (OR: 0.64, 95% CI: 0.61–0.68) and Navy (OR: 0.84, 95% CI: 0.79–0.90) showing lower compliance rates compared with White and Army ADSW, respectively. Compliance rates were higher among ADSW opting for 5-year screening intervals (98%) compared with 3-year intervals (85%).
Conclusions:
Our results show that about three-fourths of the ADSW had a cervical cancer screening, and more than 90% of those screened were USPSTF compliant. Despite overall progress, disparities persist across military branches, rank, and racial groups, highlighting the need for targeted interventions to enhance screening rates among specific groups.
Background
Cervical cancer is a preventable cancer, and in the United States, an estimated 13,360 women will be diagnosed with cervical cancer in 2025. The U.S. Preventive Services Task Force (USPSTF) recommends cervical cancer screening in all women aged 21–65 years. The USPSTF recommends screening women aged 21–65 years every 3 years with cervical cytology alone, women aged 30–65 years every 5 years with high-risk human papillomavirus (hrHPV) testing alone, or every 5 years with hrHPV testing in combination with cytology. 1
Advancements in cervical screening have led to an over 50% decline in cervical cancer rates from the mid-1970s to the mid-2000s in the United States. However, rates have plateaued over the past decade, remaining at approximately 7.7/100,000 women. 2 Despite the overall decline in cervical cancer rates, disparities persist in screening rates and health outcomes among different demographic groups, even after controlling for insurance and site of care. 3 Across the United States, racial disparities in cervical cancer incidence and mortality exist, with Black women at a 30% greater likelihood of developing cervical cancer and a 60% increased risk of mortality from cervical cancer compared with non-Hispanic White women. 4
Active-duty servicewomen (ADSW) have cervical cancer rates like civilians, but research suggests there may be a higher rate of cervical dysplasia compared with their civilian counterparts. 5 Cervical cancer screening rates are noticeably lower among ADSW compared with the general population. A study by Pope et al. 6 found that only 50% of all servicewomen met USPSTF guidelines, whereas 87% of civilian women met the guidelines. 7 Despite low guidance adherence, Pope et al. 6 noted that racial disparities in cervical cancer screening were less pronounced among ADSW.
The Coronavirus Diseases 2019 (COVID-19) pandemic significantly impacted preventive health care measures, including cervical cancer screenings, with an 84% drop in cervical cancer screening rates during the pandemic. 8 Holder-Dixon et al. 9 found that marginalized groups experienced more discrimination and tended to delay obtaining health care during the COVID-19 pandemic compared with their counterparts, which likely impacted cervical cancer screening rates. Furthermore, screening rates have yet to return to pre-pandemic levels, with lower screening rates potentially increasing the risk of cervical cancer. 10 Models project that COVID-19 disruptions will lead to increased risk of cervical cancer cases by 2027 and may disproportionately affect those already at higher risk, such as Black women. 11 This study aims to evaluate cervical cancer screening rates among ADSW in the U.S. Military and assess the proportion meeting USPSTF guidelines during fiscal year (FY) 2017–2022.
Methods
We performed a retrospective cohort study of ADSW aged 21–60 years enrolled in FY 2017 and followed up over time till the end of FY 2022 for cervical cancer screening using Papanicolaou (PAP) smear and HPV testing. Data were obtained from the Comprehensive Ambulatory/Professional Encounter Record, Genesis and Comprehensive Ancillary Data Record Extract labs, and noninstitutional data stored in the Military Health System Data Repository (MDR). Cervical cancer diagnosis was identified using the International Classification of Disease 10 coding (Supplementary Table S1). Using the MDR, we also abstracted age (21–30 years/31–60 years), race, sponsor rank (Junior Enlisted, Junior Officer, Senior Enlisted, and Senior Officer), beneficiary category, branch of service affiliation (Army, Navy, Air Force, Marines, and other services), and health care service setting (direct or private sector). Race was recorded as documented in the MDR and based on individual self-report. Our racial categories consisted of White, Black, Asian/Pacific Islander, American Indian/Alaskan Native, Other (e.g., mixed race/multiple race), and missing. Each patient visit/encounter during the study period was taken as a unit of observation for this study. We also have regrouped the age categories to 21–30, 30–39, 40–49, and 50–60 years and performed a subset analysis to evaluate the granular trends by age group categories. Cervical screening rates were defined as the proportion who had 1 or more cervical cancer screening tests (PAP or HPV) during the study period (FY 2017–2022). Compliance for cervical cancer screening was determined using the USPSTF guidelines based on the age and the type of screening (PAP test versus HPV): (1) every 3 years for women aged 21–29 years who receive cervical cytology screening, (2) every 3 years for women aged 30–65 years who received cervical cytology, (3) every 5 years for women aged 30–65 years who receive hrHPV testing alone, or (4) every 5 years for women aged 30–65 years who receive hrHPV testing in combination with cytology. For evaluating compliance among ADSW who had cervical screening, in scenarios 1 and 2, evaluation for the second test was ∼3 years after the first test, whereas in scenarios 3 and 4, evaluation for the second test was ∼5 years after the first test. We have also applied a 30-day additional buffer time (3 years + 30 days and 5 years + 30 days) to account for patients not receiving screening exactly 3 or 5 years.
ADSW who were less than 21 years of age and older than 60 years at the time of enrollment and those who were reservists, National Guard, and Coast Guard were not included in this study. Women under 21 years of age were excluded as cervical cancer screening is not recommended for them and an age cut-off of 60 years at the time of enrollment in the system was used to have an adequate follow-up for screening. The TRICARE population has only been found to be representative of the U.S. population under the age of 64 years. After the age of 65 years, Medicare tends to be the primary insurance coverage, and TRICARE data may not capture the adequate information for them. Therefore, we had included women up to 60 years and excluded women >61 years of age to have adequate follow-up up to 5 years for cervical cancer screening after the initial enrollment in FY 2017.
Statistical analysis
Baseline characteristics of ADSW enrolled in the FY 2017 study period were reported using frequencies and proportions. We evaluated cervical cancer screening rates in the Military Health System (MHS) from FY 2017–2022 for each service branch (Army, Navy, Air Force, and Marines). Univariate logistic regression analyses were used to assess the impact of race, rank, and service on cervical cancer screening rates among ADSW. We evaluated the compliance for cervical cancer screening using the USPSTF guidelines based on the age and type of screening (PAP test versus HPV). We also compared the proportion of cervical cancers, pre-pandemic (September 1, 2017, to February 28, 2020), early pandemic (March 1, 2020, to September 30, 2020), and late pandemic (October 1, 2020, to September 30, 2022). Only new/incident cases of screening were reported on for each period; therefore, if a cohort member was not eligible for screening due to the timing of the last screen relative to the period, it was not included in the subsequent periods. All analyses were conducted using SAS 9.4 (SAS Inc., Cary, NC). Significance was set at p < 0.05.
This study was conducted as part of the Military Health System Response to COVID-19 (MIHREC19) project. This study was found exempt by the Institutional Review Board of the Uniformed Services University of the Health Sciences.
Results
Demographic characteristics
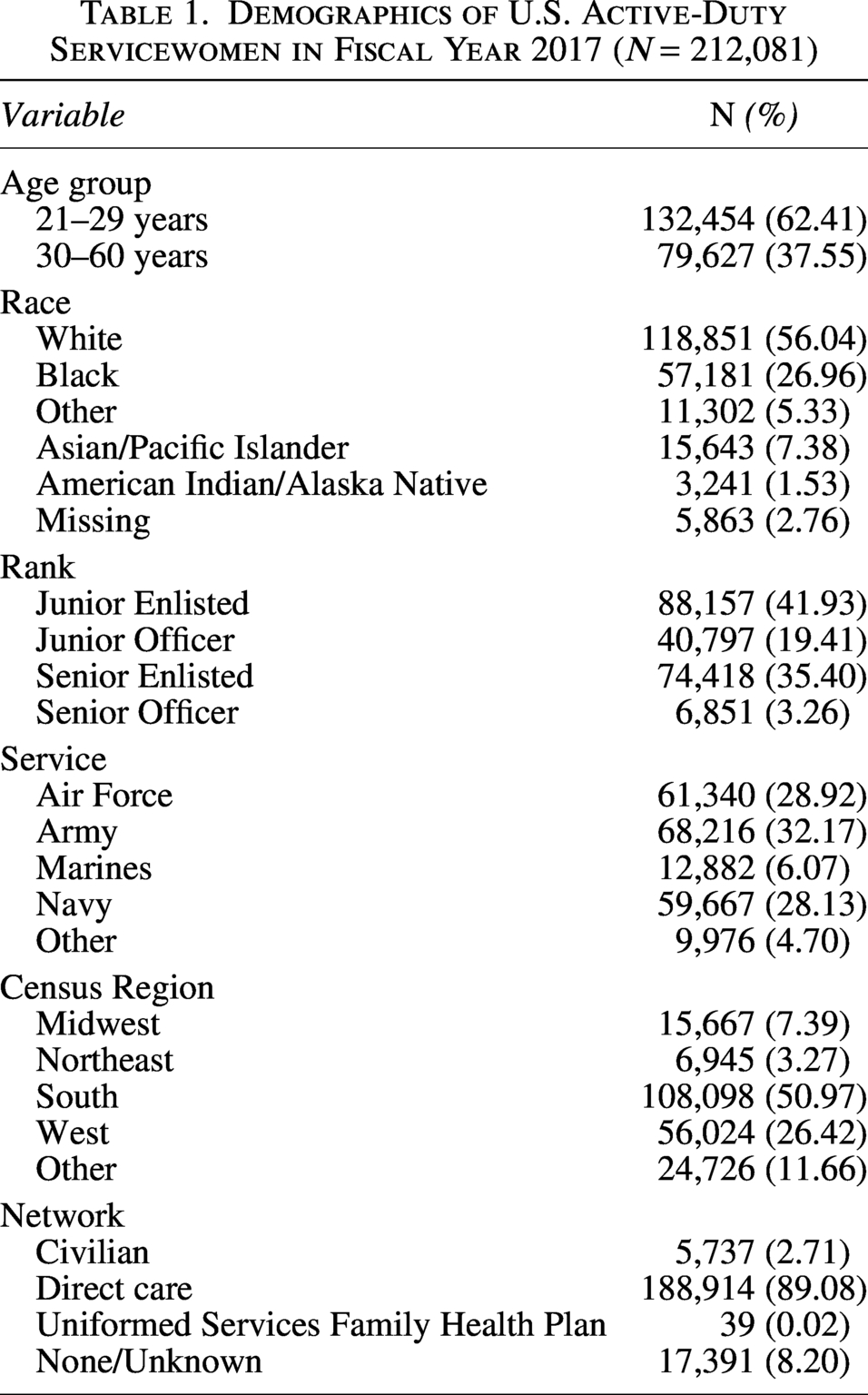
We identified 212,081 ADSW aged 21–60 years during FY 2017 who met our inclusion criteria. About 62% (n = 132,454) of ADSW were in the age group of 21–29 years, whereas 38% (79,627) were in the age group of 30–60 years. The majority of the ADSW were (56.04%, n = 118,851), followed by Black (26.96%), Asian/Pacific Islander (7.38%), and other races. About 42% of the ADSW (n = 88,157) were Junior Enlisted, and 32.2% (n = 68,216) were in the Army. ADSW within the MHS can use different health care services, such as direct care involving receiving medical services at military hospitals and clinics (Military Treatment Facilities or MTFs), purchased care provided by civilian health care providers who have contracted with the MHS, and the Uniformed Services Family Health Plan (USFHP), which provides comprehensive health care services to eligible uniformed service members and their families, retirees, and survivors in specific regions of the United States through community-based, not-for-profit health care systems or others. The majority of the ADSW received care through the direct care system (89.1%). Detailed demographic characteristics of ADSW are illustrated in Table 1.
Demographics of U.S. Active-Duty Servicewomen in Fiscal Year 2017 (N = 212,081)
Cervical cancer screening rates
In our cohort, 76.5% of eligible ADSW received cervical cancer screenings. Table 2 identifies the proportion and likelihood of cancer screening by age, rank, race, and service. Compared to women aged 21–29 years, those aged 30–60 years were less likely to be screened (odds ratio [OR]: 0.73, 95% confidence interval [CI]: 0.71–0.74). Black and Asian/Pacific Islander ADSW had an increased likelihood of screening compared with their White counterparts (OR: 1.04, 95% CI: 1.01–1.06; OR: 1.2, 95% CI: 1.15–1.25). This trend is further seen when examining rank, as senior officers were also less likely compared with junior enlisted to be screened (OR: 0.78, 95% CI: 0.74–0.82). ADSW in the Air Force (OR: 1.39, 95% CI: 1.35–1.42) and Navy (OR: 1.38, 95% CI: 1.35–1.42) were more likely to have been screened compared with those in the Army. In subset analysis, compared with women aged 21–29 years, those aged 30–39 years (OR: 0.94, 95% CI: 0.92–0.96 CI), 40–49 years (OR: 0.42, 95% CI: 0.41–0.44), and 50–60 years (OR: 0.28, 95% CI: 0.26–0.30) were less likely to be screened (Supplementary Table S1).
Cervical Cancer Screeninga Rates by Age, Race, and Rank
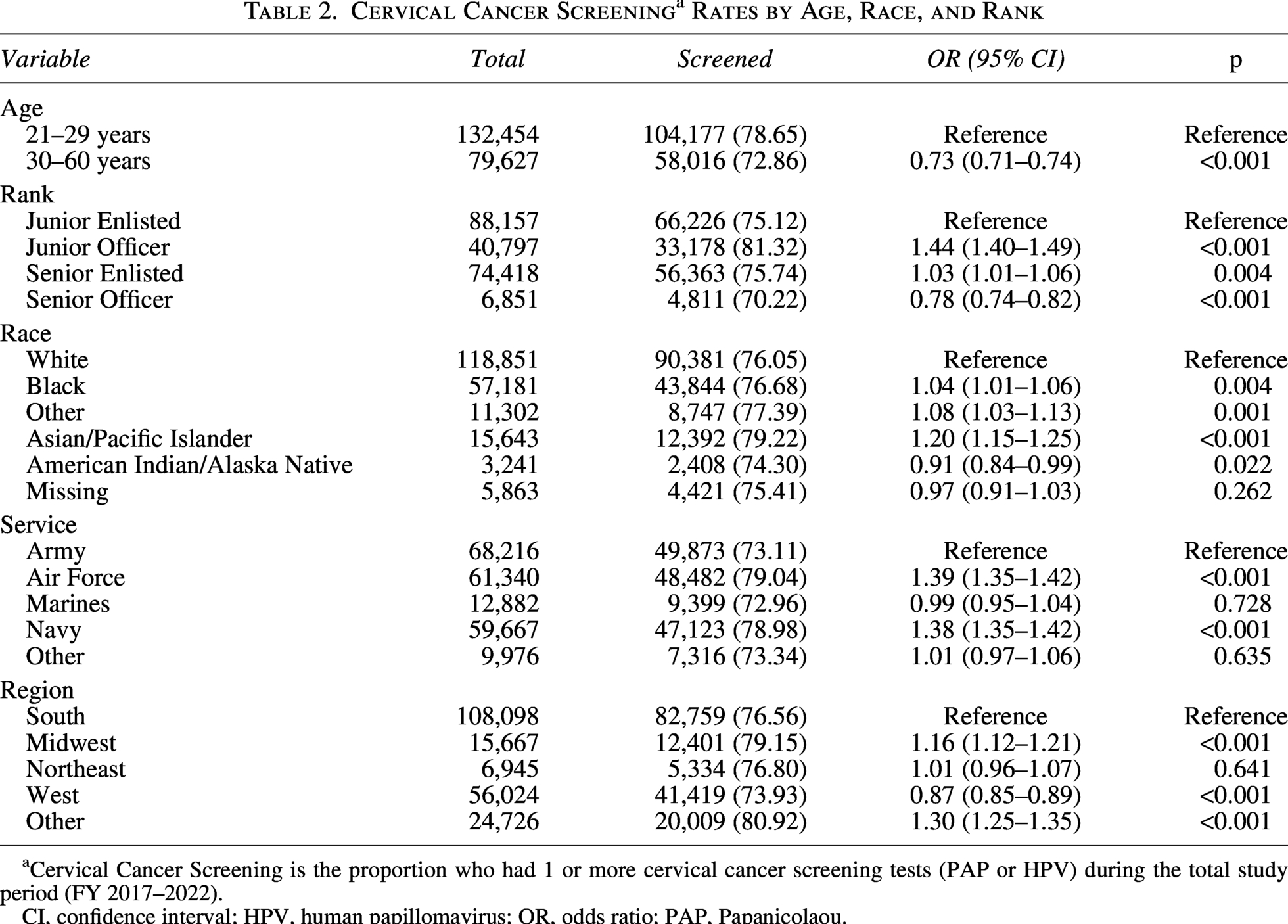
Cervical Cancer Screening is the proportion who had 1 or more cervical cancer screening tests (PAP or HPV) during the total study period (FY 2017–2022).
CI, confidence interval; HPV, human papillomavirus; OR, odds ratio; PAP, Papanicolaou.
Cervical cancer screening compliance
Out of 162,193 ADSW who got screening done for cervical cancer, 51,839 (32.0%) had a 3-year compliance and 94,277 (58.1%) had a 5-year compliance using the USPTF guidelines. Overall, 13,536 (8.4%) of the ADSW who got screening done were found to be noncompliant. We also evaluated the 3-year and 5-year cervical cancer screening compliance by race and service. The Air Force and Navy had significantly worse compliance compared with the Army (OR: 0.64, 95% CI: 0.61–0.68; OR: 0.84, 95% CI: 0.79–0.90). In contrast, the Marines had significantly better 3-year compliance (OR: 1.19, 95% CI: 1.00–1.41). On the 5-year screening group, compliance was relatively the same across all groups and races. However, notably, those of Native American/Alaskan Native race had significantly higher compliance (OR: 2.26, 95% CI: 1.07–4.78). Overall, among ADSW, those in the 3-year screening group had an average compliance of approximately 85%, whereas the 5-year stream was more compliant with an average compliance of approximately 98% (Tables 3 and 4).
Cervical Cancer Screening 3-Year Compliance for Active-Duty Servicewomen
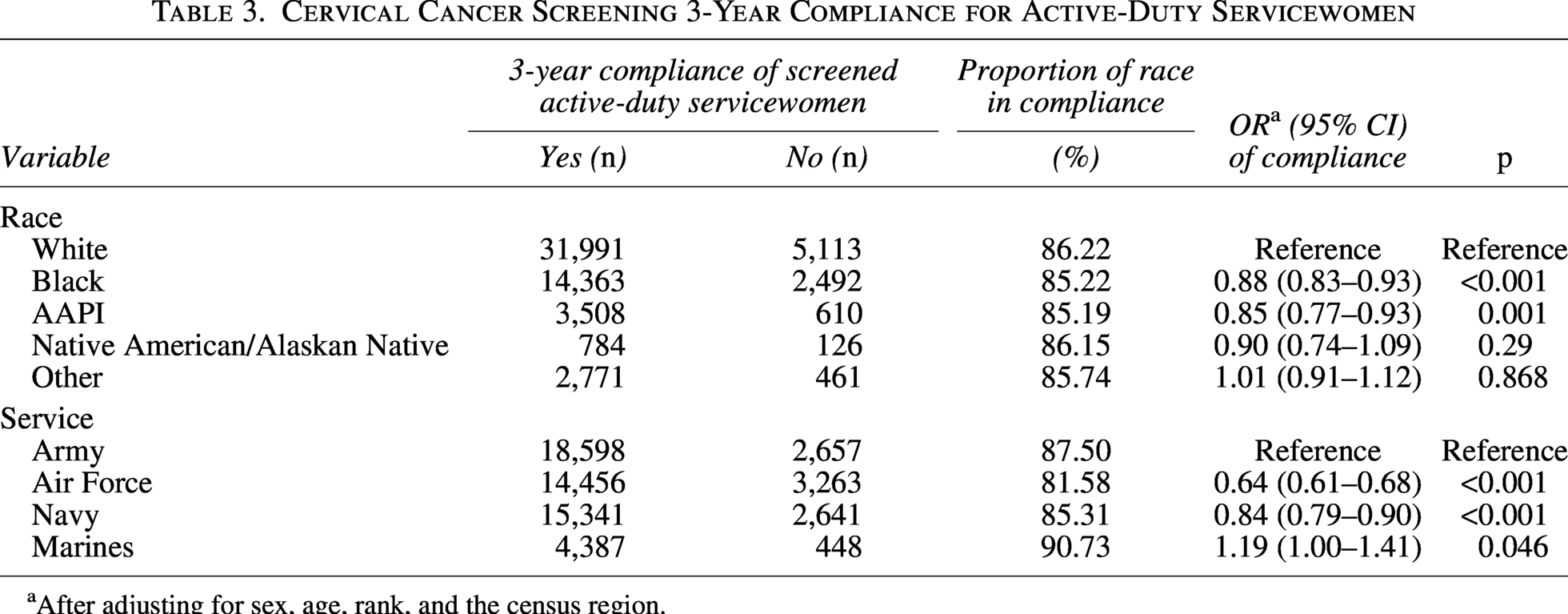
After adjusting for sex, age, rank, and the census region.
Cervical Cancer Screening 5-Year Compliance for Active-Duty Servicewomen
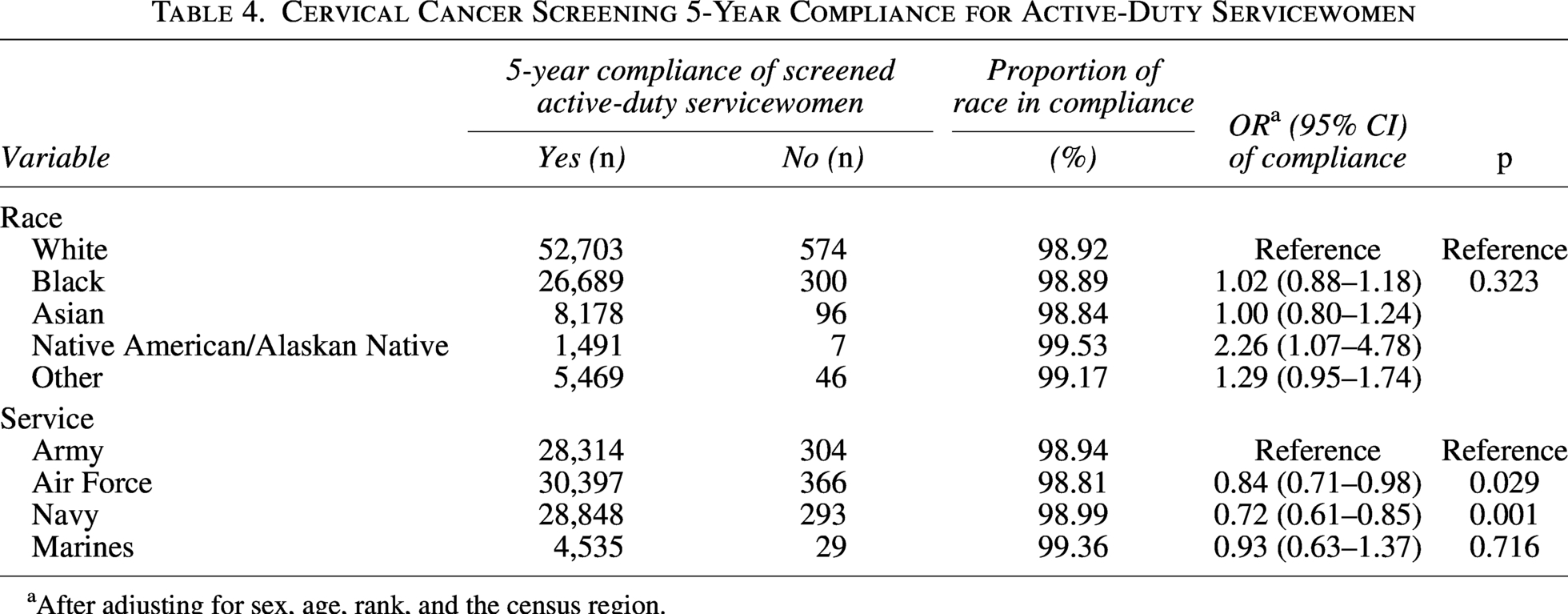
After adjusting for sex, age, rank, and the census region.
Cervical cancer screening rates by study period
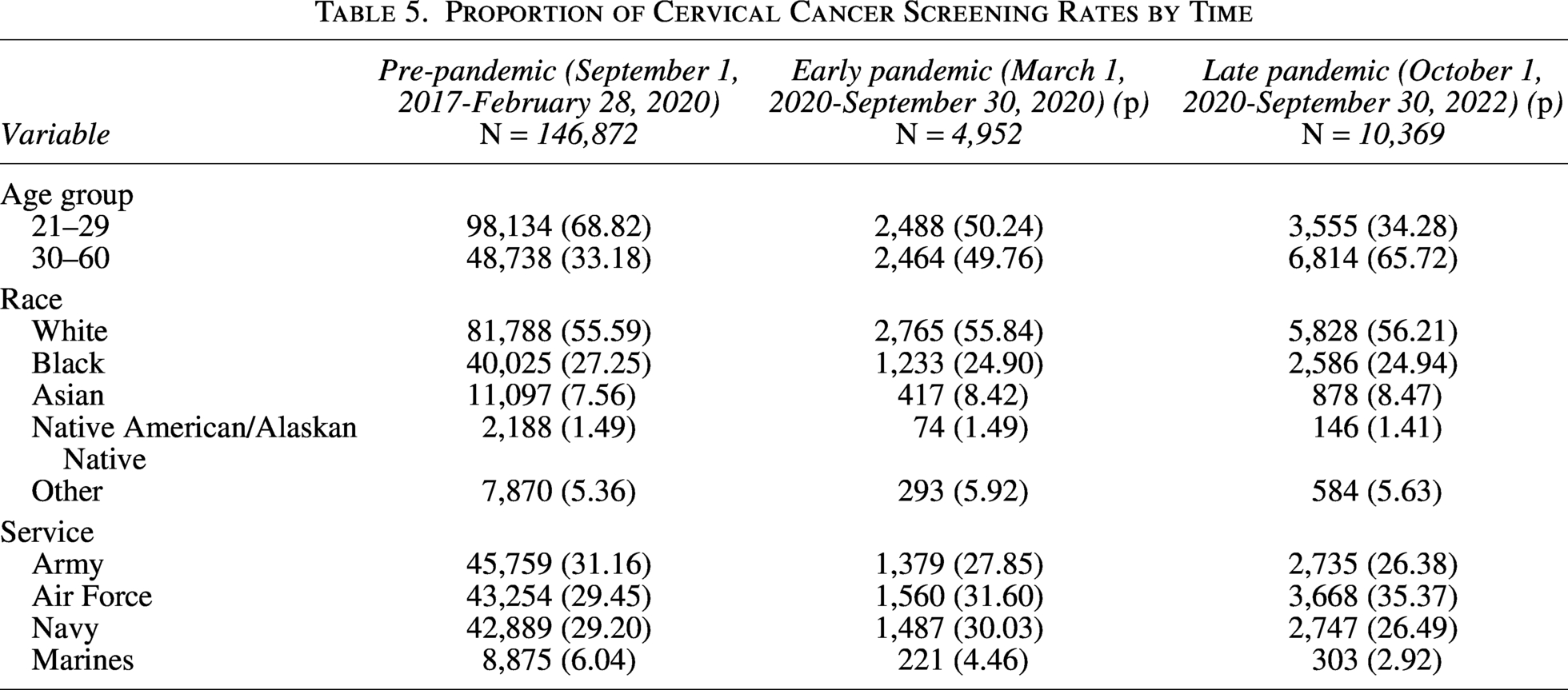
Analysis by age group revealed that women aged 21–29 years had lower screening rates during early pandemic and late pandemic periods compared with the pre-pandemic period, whereas those aged 30–60 years exhibited higher screening rates as the pandemic progressed (Table 5). Even in subset analysis, compared with women aged 21–29, those aged 30–39, 40–49, and 50–60 years were more likely to be screened during the early pandemic and late pandemic periods compared with the pre-pandemic period (Supplementary Table S2). Racial differences in screening rates did not vary significantly across these time periods. When examining screening rates by service branch, most services experienced a decline, except for the Air Force, which improved its screening rates (Table 5).
Proportion of Cervical Cancer Screening Rates by Time
Discussion
This study analyzed approximately 212,081 ADSW in FY 2017 who were eligible for a PAP smear. We found that overall, 76.48% of these eligible women received cervical cancer screening. This marks an improvement from the previous study by Pope et al., 6 which found that only 50% of ADSW received cervical cancer screenings during FY 2011–2016. Our findings also surpass the national U.S. population rate of 73.9% but fall slightly short of the Healthy People 2030 goal of 79.2%. 12 The improvement observed compared with Pope et al. 6 could be attributed to different demographics, with more women requiring cervical screening in 2017 than in 2011. Additionally, increased HPV vaccination may have raised awareness about the importance of cervical cancer screening, as suggested by Nakao et al., 13 who found that knowledge about HPV vaccination was associated with increased cervical cancer screening.
The increased adherence to cervical cancer screening, particularly in the 5-year screening category, could also be attributed to changes in cervical screening guidelines. The current USPSTF cervical screening guidelines 1 include hrHPV testing alone as a modality for screening, whereas the 2012 guidelines used in the previous study required cytology at all screening events. Many women indicate that fear of PAP smears is a barrier to cervical cancer screening due to embarrassment, vulnerability, and discomfort. 14 The introduction of hrHPV testing alone for women aged 30–65 years eliminates the need for a PAP smear, potentially reducing fear and increasing adherence to screening. Despite these improvements, senior officers had significantly lower cervical cancer screening rates compared with their counterparts, possibly because older women perceive their risk of cervical cancer and HPV to be lower. 15
Despite increased screening rates, there continue to be potential barriers to women receiving cervical cancer screening. One such barrier may be a provider’s influence on recommending cervical cancer screening, as studies show that provider and clinic factors influence cervical cancer screening in the civilian world. Women with good continuity or a female primary care provider had a 50% increased likelihood of being up to date with their cervical cancer screening. 16 Additionally, due to the nature of the military, individuals may be deployed or work in areas with limited access to cervical screening tests, potentially delaying their screening. Differences in screening rates were observed by geographic location as well, with the Midwest region having a higher screening rate and the western region having a lower screening rate compared with the southern region. Previous studies have shown that the availability of gynecological services within the MHS varies by region; size of the MTFs and ADSW are frequently referred to private practitioners when MTFs have limited staffing, lack female providers, or have high appointment wait times.17,18
Our study shows a vast improvement in compliance with cervical cancer screening compared with the study by Pope et al. 6 On average, between both 3-year and 5-year screening pathways, we observed an approximate 92% compliance rate. Despite these overall improvements, there are discrepancies, particularly for those in the 3-year cervical cancer surveillance cohort. Unlike Pope et al., we found significantly less compliance in the Air Force and Navy compared with the Army. This difference may be due to women in the Navy being posted to ships, limiting their access to cervical cancer screening.
Additionally, in the 3-year cohort, racial disparities were observed, with Black or Asian/Pacific Islander women having significantly lower screening rates than their White counterparts. This finding is concerning given the equitable access provided by the MHS, which should mitigate such disparities. Further research is needed to investigate why this occurred.
The trends observed in cervical cancer screening rates during this period provide valuable insights into the screening behaviors of ADSW in the context of the COVID-19 pandemic. The decrease in screening rates among women aged 21–29 years may be attributed to a perceived lower risk of cervical cancer, whereas the increase in screening among those aged 30–60 years likely reflects heightened health awareness prompted by the pandemic. This was much more evident in the subgroup analysis of age for 30–39, 40–49, and 50–60 years. This trend is unexpected, given that COVID-19 significantly disrupted preventive health care measures, including an 84% drop in cervical cancer screenings. 8 The increase in screening rates for older women might be due to improved health care awareness and a stronger desire to take control of their health during uncertain times.
This study has several limitations. As the Military Data Repository (MDR) is an administrative database, it is subject to coding or specificity errors and may fail to capture clinical nuances. For example, it cannot determine whether an individual received a cervical screen to follow guidelines or due to abnormal results. This limitation restricts our population demographic and may limit the generalizability of our findings to the U.S. military. We identified and included ADSW at the time of enrollment in FY 2017 and followed them over time for the next 5 years. Some of these women may have been discharged from the active duty over the course of the next 5 years; however, they were still followed even if they were discharged from the active duty. We do not have information on whether the ADSW was deployed overseas or on a ship. Irrespective of their overseas deployment, if they sought any medical service, all health care encounters (if any) are recorded in the MHS. Prior studies have shown that ADSW could schedule predeployment appointments at least 90 days prior to deployment.19,20 Lastly, we could not assess all correlates that may impact cervical screening due to limitations in our data source.
Overall, this study demonstrated a significant improvement in cervical cancer screening rates and compliance with USPSTF guidelines compared with previous findings. The screening rates observed in this study exceed those of the general population but fall slightly short of the Healthy People 2030 goals. Notably, the study identified differences in compliance adherence between military services and racial groups. Further investigation is warranted to understand the reasons behind these disparities.
Exploring the impact of service-specific guidelines on screening rates could be beneficial, with a view toward developing uniform, service-wide guidelines. Additionally, the recent Food and Drug Administration approval of self-swab HPV testing presents an opportunity to enhance screening rates and compliance, particularly for individuals in remote or austere locations.
Disclaimer
The contents of this publication are the sole responsibility of the authors and do not necessarily reflect the views, assertions, opinions, or policies of the Uniformed Services University of the Health Sciences, the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., the Department of Defense, or the Departments of the Army, Navy, or Air Force. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. government.
Authors’ Contributions
L.W. and T.P.K.: Study concept and design, interpretation of data, drafting of the article, critical revision of the article for important intellectual content, and approval of the final draft of the article. S.M.: Study concept and design, statistical analysis, interpretation of data, drafting of the article, critical revision of the article for important intellectual content; and approval of the final draft of the article. C.C.: Study concept and design, critical revision of the article for important intellectual content, and approval of the final draft of the article. A.B.: Critical revision of the article for important intellectual content and approval of the final draft of the article.
Ethics Approval and Consent to Participate
This study was found exempt by the Uniform Services University of the Health Sciences’ Institutional Review Board (IRB). The need for consent to participate was waived by the IRB.
Availability of Data and Material
Raw data used for this study is not publicly available. Any other data request regarding the analytical results will be shared upon reasonable request.
Conflict of Interest
The authors declare they have no conflicts of interest.
Funding Information
This study was funded through the MiHReC project by the
Footnotes
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.