
Abstract
Background:
Myotonic dystrophy type 1 (DM1) impacts women’s health in several ways, causing gynecological and obstetrical issues, among others. Documenting the frequency and severity of these clinical issues is crucial for improving the care and health-related quality of life of women with DM1. This scoping review aimed to map and describe existing research on gynecological and obstetrical issues in women with DM1 and identify research gaps.
Methods:
Comprehensive searches were conducted across multiple databases, including PubMed, CINAHL, ProQuest Central, and Google Scholar, from inception to December 2023. Studies examining gynecological and obstetrical issues in women with DM1 using quantitative, qualitative, and mixed methods were included. Two authors independently screened studies and extracted data using standardized forms.
Results:
A total of 36 studies were included. Gynecological problems in women with DM1 included fertility issues, genital malignancies, and pelvic floor disorders, while obstetrical complications entailed miscarriage, ectopic pregnancy, preeclampsia, hypertensive disease, polyhydramnios, preterm labor, and nonvertex presentation.
Conclusion:
This scoping review demonstrates that few articles document gynecological and obstetrical issues in women with DM1. Future studies should address this important knowledge gap and enhance management and outcomes for these women.
Keywords
Introduction
Myotonic dystrophy type 1 (DM1) is a rare disease, but it is the most common neuromuscular disorder in adulthood. A recent study reported a pooled estimate of 9.27 cases (95% CI: 4.73–15.21) per 100,000, ranging from 0.37 to 36.29 cases per 100,000. 1 The highest prevalence of DM1 is observed in the region of the Saguenay–Lac-St-Jean, Quebec, Canada, where 158 out of 100,000 individuals are affected. 2 The disease results from a mutation in the dystrophic myotonic protein kinase (DMPK) gene located on chromosome 19q13.3, which involves the expansion of a cytosine–thymine–guanine (CTG) trinucleotide repeat. 3 The disease’s pathogenic mechanism revolves around the RNA transcribed from the expanded allele, which contains extended sequences of (CUG)n. This RNA exerts a toxic effect through two RNA-binding proteins: muscleblind-like 1 (MBNL1) and CUG-binding protein 1 (CUGBP1). In DM1, MBNL1 becomes sequestered on CUG repeat-containing RNA, leading to its loss-of-function, while CUGBP1 undergoes an up-regulation via a signaling pathway. The downstream consequences include disrupted regulation of alternative splicing, mRNA translation, and mRNA stability, contributing to the diverse features of DM1. These atypical RNAs, with an elongated CUG sequence, exert profound effects on cellular function by influencing the biogenesis of other cellular RNAs. A prominently altered aspect of RNA metabolism is the regulation of alternative splicing. Through this mechanism, the consequences of myotonic dystrophy repeat expansions affect numerous pathways, instigating an intricate array of signs and symptoms.4–8
DM1 is categorized into five clinical phenotypes by age of onset: congenital, childhood, juvenile, adult, and late-onset. 9 The disorder is characterized by muscle weakness, delayed muscle relaxation (myotonia), and early cataract development. It also affects other organ systems, including the endocrine and reproductive systems, which can have multifaceted implications on women’s health. Among them, a negative impact on fertility has been documented. 10 Furthermore, the impact of DM1 on smooth muscles 11 can increase the risk of abnormal pregnancy and delivery, such as spontaneous abortion, preeclampsia, polyhydramnios, and preterm labor.12,13 It has been suggested that women carrying a fetus with the congenital form of the disease are far more at risk of multiple complications during pregnancy and delivery. Therefore, their condition should be identified early in the pregnancy. 14 A case report also showed an increased risk of benign and malignant neoplasms in DM1 patients, such as gynecological cancers. 15 There are currently no reviews of reproductive health in women with DM1, which greatly hinders adequate clinical screening and management. This scoping review aimed to map and synthesize previous research on gynecological problems and obstetrical complications in women with DM1, to identify areas where further research is required.
Methods
The scoping review was conducted following the Joanna Briggs Institute methodology. 16 This approach was selected to facilitate a comprehensive examination of a wide range of scientific literature, thereby providing an optimal methodological framework for achieving the study objectives. The first aim was to answer the question “What are the gynecological problems and obstetrical complications experienced by women diagnosed with DM1?”. We formulated this question using the Population, Context, and Concept framework. 16 Bibliographic databases, including PubMed, CINAHL, ProQuest Central, and Google Scholar, were searched from inception to the end of December 2023. Articles had to be written in French or English, with full-text accessibility. We used specific keywords to identify potentially relevant studies (see Supplementary Appendix S1 for the complete search strategy).
Results of the search were organized in the EndNote reference management software. After duplicates were excluded, articles were screened for inclusion following two rounds of iterative screening. First, two reviewers (I.F.P. and C.G.) independently screened all titles and abstracts based on the eligibility criteria. Following the initial screening, the selected full-text articles were thoroughly reviewed and evaluated by two independent reviewers based on the same criteria and confirmed by a third reviewer. Any disagreements were resolved through discussion or consultation with a third author (M.M.). The inclusion criteria were as follows:
Women diagnosed with DM1, Studies reporting on gynecological problems and obstetrical complications.
The exclusion criteria included:
Studies examining gynecological problems and obstetrical complications among women with DM1 and coexisting comorbidities impacting the issues under investigation, such as type 2 diabetes or hypertension, Studies primarily focusing on fetal outcomes instead of pregnancy outcomes, Review articles.
We also conducted hand searches in the bibliographies of the articles found in the database search to identify additional relevant studies. This involved reviewing the reference lists of relevant scoping reviews, systematic reviews, and meta-analyses, as well as the reference lists of all publications included in the study.
We extracted data from the selected studies using a predesigned data extraction form that captured key information such as first author’s name, publication year, country of origin, study type, sample size, research objective, data collection method, and study findings. This form was created and approved by all team members prior to the data extraction process. Two authors (A.Tremblay and M.L.) performed an independent data extraction, and the extracted data were compiled into Table 1. A third author with a background in gynecology performed an independent data extraction validation (A.Tamizi). To collect, synthesize, and report the results, we analyzed the data using a descriptive summary and categorized them based on general characteristics such as author’s name, publication year, country of origin, study type, sample size, and research objectives. Additionally, specific characteristics such as study aims and outcomes were classified into two groups: gynecological problems and obstetrical complications.
Data Extraction Grid
CTG, cytosine–thymine–guanine; DM1, myotonic dystrophy type 1.
Results
The search yielded a total of 559 studies. After excluding duplicates, 524 records were screened for eligibility, and 36 studies were finally included in the present review (see Fig. 1 for the detailed PRISMA diagram).
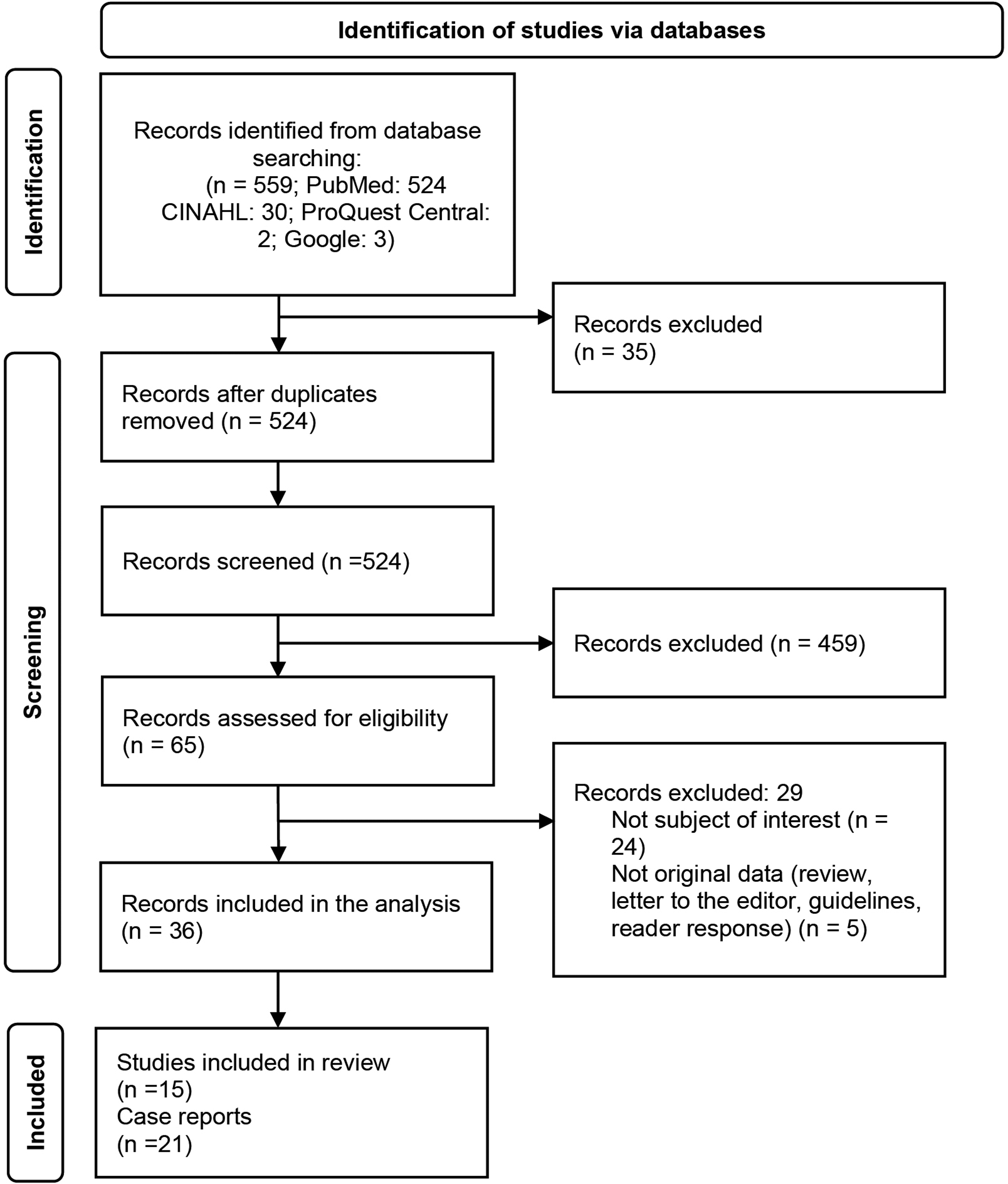
Prisma flow diagram for identified, included, and excluded records.
Characteristics of included articles
A summary of study characteristics is presented in Tables 2 and 3, where Table 2 includes studies related to gynecological problems and Table 3 contains studies about obstetrical complications. Out of the 36 selected articles, three were prospective cohorts, 9 were retrospective cohorts, 3 studies were cross-sectional, and 21 were case reports. Supplementary Table S1 provides a summary of all selected case reports addressing gynecological problems and Supplementary Table S2 the case reports addressing obstetrical complications. The studies were conducted in various countries, and their publication dates ranged from 1958 to 2023. While most studies were based on a single case report, the largest cohort study had a sample size of 472 women participants. As most articles were case reports, excluding them could have significantly limited the body of knowledge that could support further research. However, when a finding was only supported by case reports, the code CR was added next to the sentence in the following paragraphs of the Results section.
Summary of Studies Reporting on Gynecological Problems in DM1 Patients
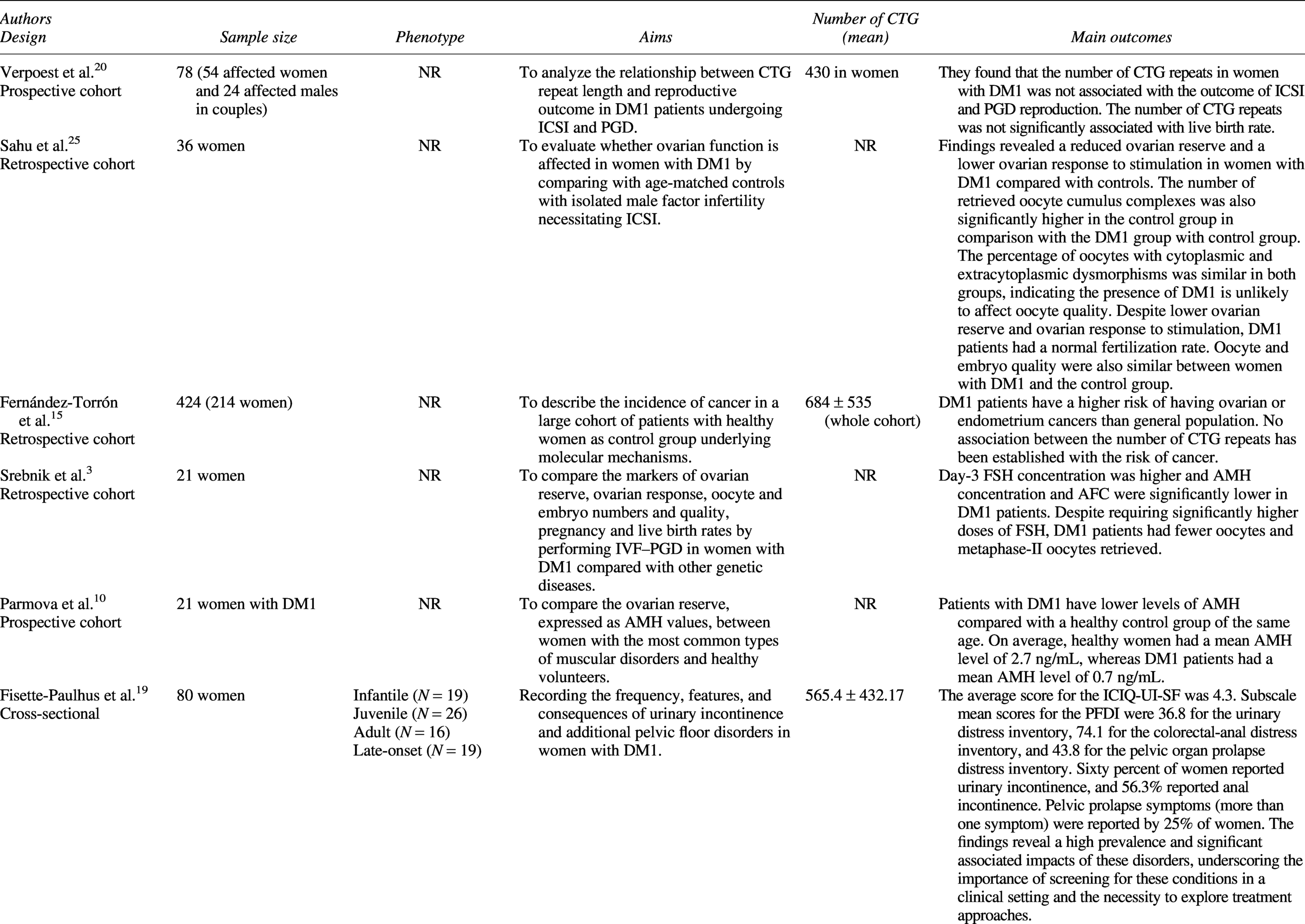
AMH, anti-Müllerian hormone; IVF, in vitro fertilization; PGD, preimplantation genetic diagnosis; ICSI, intracytoplasmic sperm injection; NR, not reported; ICIQ-UI-SF, the International Consultation Incontinence Questionnaire–Urinary Incontinence short form; PFDI, the Pelvic Floor Disorder Inventory; PFIQ-SF, the Pelvic Floor Impact Questionnaire short form.
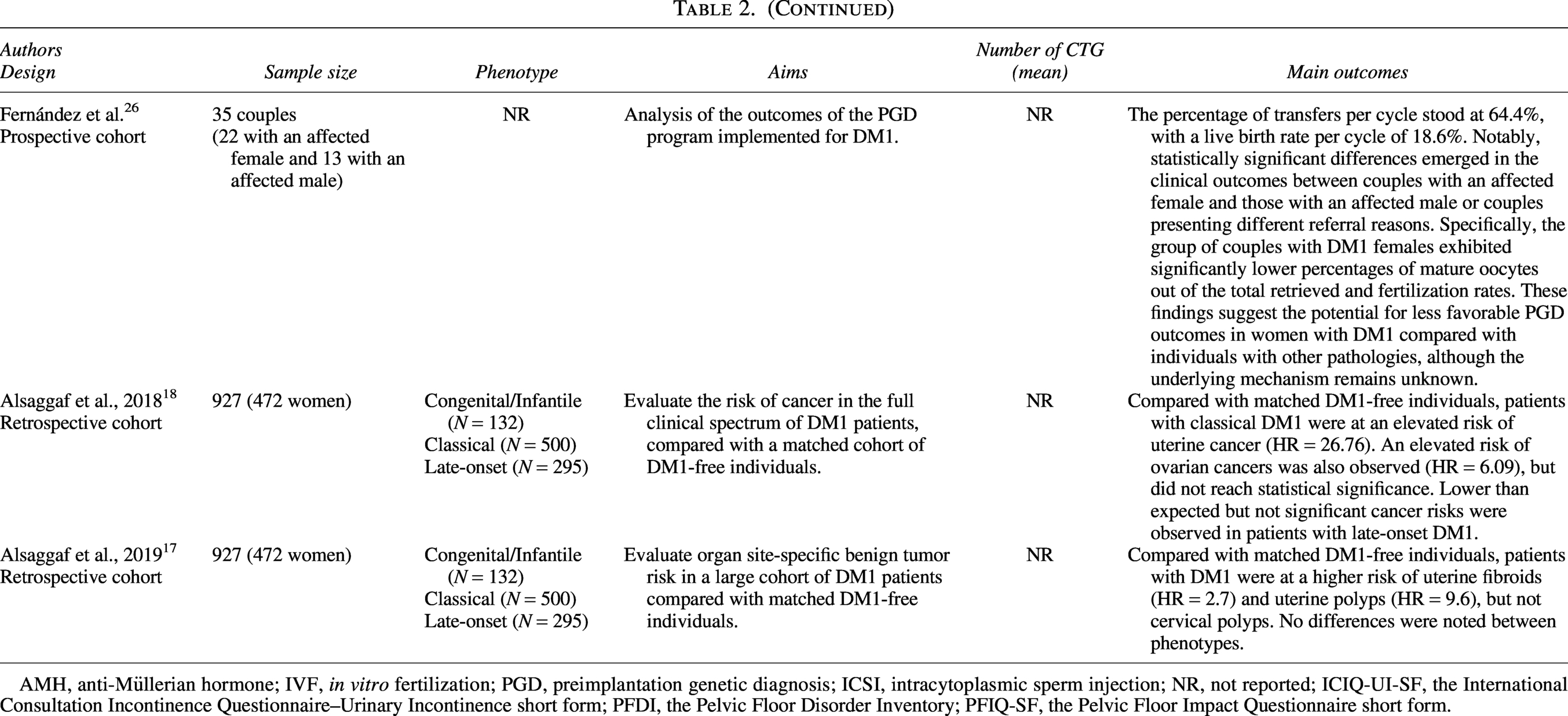
continued
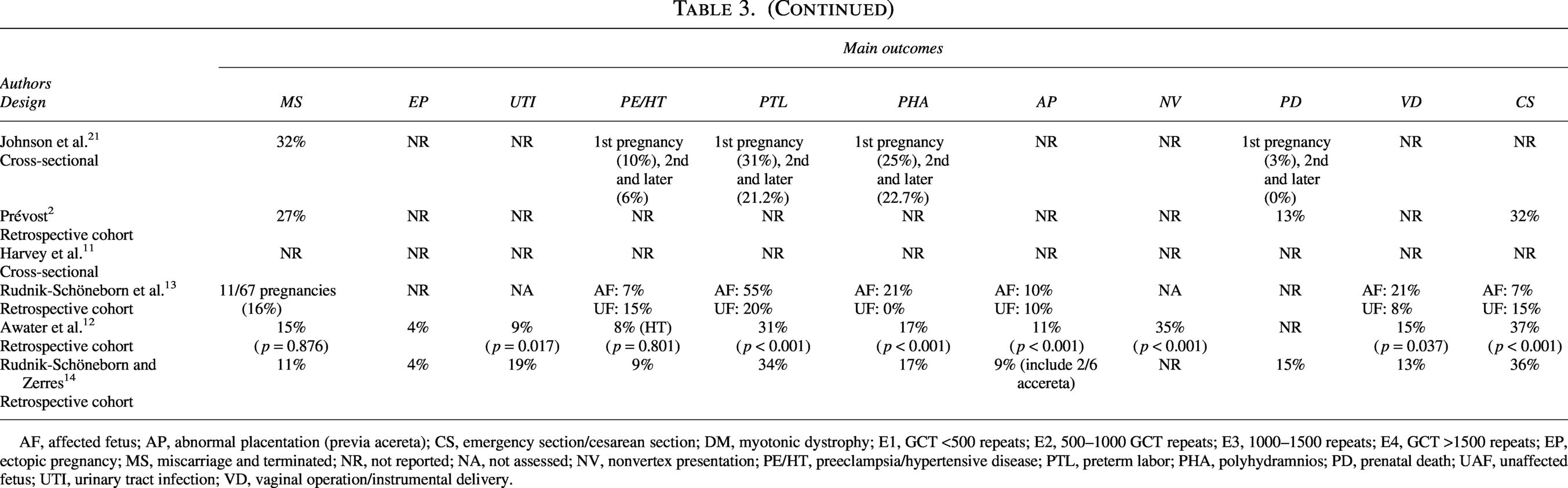
Summary of Studies Reporting on Obstetrical Complications in DM1 Patients
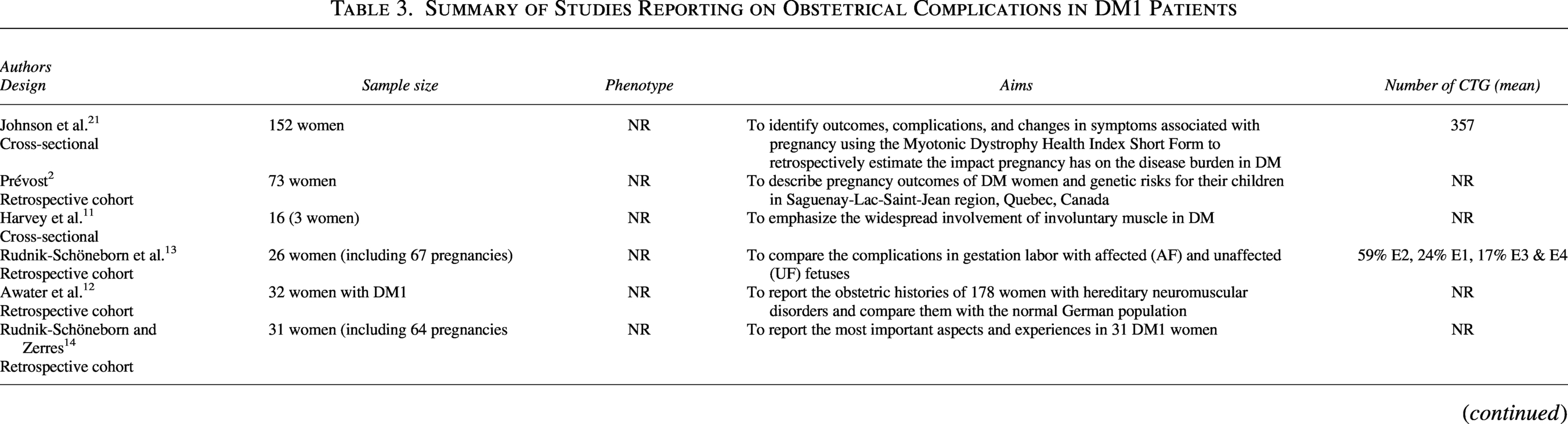
AF, affected fetus; AP, abnormal placentation (previa acereta); CS, emergency section/cesarean section; DM, myotonic dystrophy; E1, GCT <500 repeats; E2, 500–1000 GCT repeats; E3, 1000–1500 repeats; E4, GCT >1500 repeats; EP, ectopic pregnancy; MS, miscarriage and terminated; NR, not reported; NA, not assessed; NV, nonvertex presentation; PE/HT, preeclampsia/hypertensive disease; PTL, preterm labor; PHA, polyhydramnios; PD, prenatal death; UAF, unaffected fetus; UTI, urinary tract infection; VD, vaginal operation/instrumental delivery.
continued
The phenotype was not reported in the majority of studies (n = 33), but two studies, involving the same cohort, included all phenotypes, with the majority being adult-onset.17,18 Also, one cross-sectional study included all phenotypes except the congenital phenotype. 19 Additionally, the number of CTG repeats was not reported in most studies (n = 28), but one prospective cohort study, 20 two retrospective cohort studies,13,15 two cross-sectional studies,19,21 and three case reports22–24 reported the number of CTG repeats.
Gynecological problems
Eight cohort articles3,10,15,17,18,20,25,26 (involving between 21 and 472 patients) and five case23,27,39,40 reports focused on two gynecological problems: either fertility issues or gynecological cancers. A single study examined pelvic floor disorders. 19 Table 2 provides a summary of findings for these nine studies, while Supplementary Table S1 presents case report results.
According to Parmova et al., 10 women with DM1 had lower levels of anti-Mullerian Hormone (AMH) compared with a healthy age-matched group; healthy participants had a mean AMH level of 2.7 ng/mL, whereas women with DM1 had a mean AMH level of 0.7 ng/mL.
Another study by Srebnik et al. 3 found that women with DM1 had higher concentrations of day-3 follicle-stimulating hormone (FSH) and significantly lower concentrations of AMH and Antral follicle count (AFC). Despite requiring higher doses of FSH, women with DM1 had fewer oocytes, and metaphase-II oocytes were retrieved. Sahu et al. 25 documented that women with DM1 have a reduced ovarian reserve and lower ovarian response to stimulation. The number of retrieved oocyte cumulus complexes was also significantly higher in the control group. However, oocytes quality was similar in both groups. Despite lower ovarian reserve and ovarian response to stimulation, DM1 patients had a normal fertilization rate, and oocyte and embryo quality were also comparable to the control group. On the other hand, Fernández et al. 26 observed that both the percentage of mature oocytes out of the total oocytes retrieved and the percentage of fertilization were considerably lower in the group of DM1 females. Their finding suggests the possibility of achieving less favorable preimplantation genetic diagnosis outcomes in women with DM1 in comparison with other pathologies, although the underlying mechanism remains unknown. 26 Verpoest et al. 20 demonstrated that the number of CTG repeats in women with DM1 did not affect the outcome of intracytoplasmic sperm injection, preimplantation genetic diagnosis reproduction or live birth rate.
In addition, gonadal failure with distinct characteristics was found in four patients with DM1, of whom only one was female. The woman was presenting with a childhood-onset DM1 with intellectual disability and had presumed hypothalamic amenorrhea [CR]. 27 These findings suggest that there are varying expressions of hypogonadism associated with the same inherited muscle disease. Indeed, two of the three males were her brothers, one with cryptorchidism, childhood onset intellectual disability and hypogonadotropic hypogonadism, and the second with disease onset in his teenage years, who had seminiferous tubular failure and elevated gonadotropins.
As mentioned, there is limited research on gynecological cancer. Fernández-Torrón et al. 15 reported that women with DM1 have a higher risk of ovarian or uterine cancer than healthy women, but no link has been established between the number of CTG repeats and cancer development risk. However, the authors stated that this result could be biased since the number of CTG repeats was measured years before cancer onset, and the somatic instability of the expansion might be an underlying mechanism in tumoral tissue. Alsaggaf et al. also reported a higher risk of uterine cancer 18 and benign tumors, 17 such as uterine fibroids and polyps. In a case report, Kinoshita et al. [CR] 28 examined the unstable nature of (CTG)n expansions in tissues obtained from ovarian cancer and ovarian cyst of a DM1 woman. The findings indicated that the (CTG)n expansion in the ovarian cancer was longer than in the ovarian cyst, suggesting that elongation may occur during acquired cell proliferation.
As mentioned earlier, DM1 can impact both smooth and striated muscles, including pelvic floor muscles. Consequently, these changes in pelvic floor muscle function can trigger a range of pelvic floor disorders in women, such as issues related to urinary, anorectal, and vaginal conditions. Fisette-Paulhus et al. 19 observed no statistically significant difference in the prevalence of urinary incontinence between women who underwent cesarean sections and those who had vaginal deliveries, although time since delivery was not reported. Higher scores on the International Consultation Incontinence Questionnaire—Urinary Incontinence short form (ICIQ-UI-SF) were associated with infantile, juvenile, and adult phenotypes, as well as multiparity, compared with the late adult phenotype and nulliparity, respectively. Regarding the pelvic floor disorder inventory, the juvenile phenotype exhibited elevated scores on the urinary distress inventory (UDI) (irritative subscale), colorectal–anal distress inventory (CRADI) (obstructive and pain/irritation subscales), and pelvic organ prolapse distress inventory (posterior subscale). The infantile phenotype also showed a higher score, specifically in the pain/irritation subscale of the CRADI. 19 In addition, 60% of women reported urinary incontinence, 56.3% reported anal incontinence, and 25% reported symptoms of pelvic prolapse (more than one symptom). 19
Obstetrical complications
Six studies2,11–14,21 (involving 16–152 patients) and 16 case reports22,24,30–32,42–51 have documented different obstetrical complications in women with DM1. Table 3 provides a summary of findings for these six studies, while Supplementary Table S2 presents case report results.
The majority of studies (n = 5) reported cases of miscarriage.2,12–14,21 The other reported complications included ectopic pregnancy,12,14 preeclampsia, hypertensive disease,12–14,21 polyhydramnios, preterm labor, nonvertex presentation, 12 and prenatal death.2,14,21 Prévost et al. 2 also reported neonatal death associated with low birth weight, premature delivery, and hydramnios during the pregnancy of women with DM1. Increased risk of urinary tract infections has also been reported during pregnancy in women with DM1 compared with a control group.12,14 Vaginal delivery with or without instrumentation was investigated in three studies,12–14 while emergency cesarean section to terminate the pregnancy was reported in four studies.2,12–14 The percentage of instrumented vaginal delivery is the same or slightly above the general population (13–15% for DM1 women12,14) and Rudnik-Schöneborn et al. 13 suggest that the frequency is higher with DM fetuses compared with nonaffected fetuses (21% compared with 5%). Rudnik-Schöneborn et al. 13 also found that 14% of pregnancies with affected fetuses (congenital phenotype) and 40% of pregnancies with unaffected fetuses did not experience any complications. However, obstetrical complications and congenitally affected fetuses occurred in all maternal phenotypes and CTG repetition classes (Supplementary Table S2). The frequency of cesarean sections ranges from 24% to 36.7%,12–14 compared with 24.5% for primary cesarean delivery in Canada in 2002. 29
Two studies have reported on the prolongation of the stage of labor, especially in the first stage, and suggested that it may be due to the involvement of the uterine muscle and maternal weakness.11,14 Harvey et al. 11 demonstrated that early in the first stage of labor, the uterine contractions were mild in intensity and had prolonged duration, with a typical “myotonic” response and prolonged relaxation phase observed on tocodynamometer tracings. More recently, Awater et al. 12 found that the incidence of prolonged labor was not significantly increased in gestations with any neuromuscular disease.
Rudnik-Schöneborn and Zerres 14 reported postpartum hemorrhage due to uterine inertia in two deliveries (3%). It was found in another study that 17.2% of pregnancies in DM1 patients had a peripartum hemorrhage. 21
Among other complications reported, three articles12–14 have demonstrated abnormal placentation, such as previa and accreta. In one case report by Dorcier et al. [CR], 30 researchers indicated placenta increta in the primary gravid patient without any risk factors other than myotonic dystrophy. Also, although cardiomyopathy and arterial dissection are both uncommon complications of pregnancy, Besant [CR] 22 reported it in one case report with DM1. In addition, 31% of patients experienced a worsening of their general symptoms during pregnancy, with three cases reporting a temporary weight-related deterioration. However, most mothers were able to care for their families and newborns without help during the postpartum period. Johnson et al. 21 also reported that symptoms generally worsened in the postpartum period, particularly mobility, fatigue, and pain.
Finally, anesthesia procedures were discussed in two case reports. Indeed, given the risks associated with general anesthesia in DM1, it is of utmost importance to identify women with DM1 before possible surgery or pregnancy [CR].31,32
Discussion
This scoping review provides an overview of gynecological problems and obstetrical complications documented in women with DM1. Several important aspects were absent from the literature, including abnormal bleeding, dysmenorrhea, fibroma, hysterectomy, family planning and contraception.
Cancer is the third most prevalent cause of mortality in individuals with DM1. 14 Adult-onset DM1 women may face a higher risk of uterine fibroids and uterine cancer, 15 highlighting the need for further research in this area. Understanding these tumor-related complications can have significant clinical implications for the management and treatment of DM1 patients, but only two studies included in this scoping review discussed the potential pathways.15,18 However, D’Ambrosio et al. suggest that the exact mechanism that accounts for certain cancers increase in DM1 is not well-understood, but the upregulation of the Wnt/B-catenin pathway and/or alterations of the mRNA transcripts encoding tumor suppressor genes or oncogenes have been postulated. 33 A better understanding of the molecular mechanisms involved in gynecological problems and tumor development in DM1 patients is crucial. 34
Fertility problems in DM1
DM1 patients often experience reduced fertility due to lower concentrations of AFC and AMH, leading to diminished embryo quality and lower pregnancy rates. 9 Higher rates of infertility have also been reported in nondystrophic myotonias, as highlighted in a recent review on maternal health and obstetric complications in neuromuscular disorders. 35 Moreover, although previous epidemiological studies indicate that women with DM1 do have children, they also show that affected women tend to have fewer children than affected men.36,37 However, these studies did not assess fertility parameters directly and further studies are thus needed to better understand fertility in women with DM1.
Preimplantation genetic diagnosis in DM1 is established as a workable option to prevent transmission of the disorder and result in healthy live births, but outcomes, particularly ovarian response and reproductive success, show variability across studies and potentially less favorable outcomes in DM1.3,38 There remain important unanswered questions regarding the physiological effects of DM1 on fertility, optimal stimulation protocols, and long-term outcomes for families using preimplantation genetic diagnosis, underscoring the need for further research.
Obstetrical complications in DM1
Pregnant individuals with DM1 are at higher risk of complications such as prematurity, polyhydramnios, malpresentation, cesarean section, hemorrhage, and placenta previa. 11 In their review, Ahmed et al. also found prolonged labor and breech presentation, leading to more cesarean deliveries, as intrapartum complications in myotonic dystrophy. 35 These complications, specifically the increased rate of cesarean sections, are also found in other neuromuscular diseases, such as congenital myotonic dystrophy, limb–girdle muscular dystrophy, facioscapulohumeral muscular dystrophy, spinal muscular atrophy, and Pompe disease, mainly due to breech presentation or fetal distress. 35 In these neuromuscular diseases, postpartum hemorrhage and prolonged recovery have also been identified as frequent postpartum complications. Women with DM1 could also face cardiovascular risks, including spontaneous coronary artery dissection and other cardiac abnormalities during pregnancy. 22
Several limitations exist in this research area, including the limited number of studies available. The scarcity of research restricts the available evidence and limits the ability to draw firm conclusions. Additionally, many of the studies included in this scoping review have small sample sizes, which impacts the generalizability of findings to the broader population of DM1 patients. In addition, most studies do not present results by phenotype, limiting the potential to adjust the recommendations. One of the principal caveats highlighted by this review is the absence of standardized questionnaires/clinical interviews that specifically address gynecological problems and obstetrical complications in DM1. This is a key aspect to better describe symptom severity and estimate accurate prevalence.
Furthermore, the lack of comprehensive research in this field is another limitation. Existing studies often lack suitable experimental designs and fail to address the broader implications of DM1 on gynecological problems and obstetrical complications. Additional gaps to address include the effects of DM1 on gynecological problems such as abnormal uterine bleeding, menstruation, endometriosis, sexual dysfunction, and global sexual health. Research on menopause and associated symptoms in DM1 patients is also needed. Developing a comprehensive guideline for gynecological problems, particularly obstetrical complications, specifically designed for DM1 patients would be a significant step forward in the future.
Area for future research
The findings from this scoping review, along with other evidence, yield important interpretations concerning gynecological problems and obstetrical complications in patients with DM1. Gene dysregulation and expression pathways, particularly abnormal RNA splicing and changes in gene expression, emerge as potential key factors contributing to the development of gynecological problems and tumors in DM1 patients. 15 This underscores the relevance of understanding the molecular mechanisms at play in order to advance knowledge in this field. 34 DM1 impact on fertility constitutes another important topic. The deleterious effects of expanded RNA on the ovaries, coupled with alterations in the hypothalamic–pituitary–gonadal axis, are targeted as a potential contributing factor to diminished fertility in DM1 patients. 10 Further research is imperative to elucidate the precise mechanisms involved and pave the way for developing effective strategies to manage fertility problems in this population. In addition, as individuals with DM1 represent a complex population, it is crucial to evaluate the association between symptoms and other contributing factors such as phenotype, genotype, obstetrical history, age, and muscular impairment.
Furthermore, obstetric management considerations are of paramount importance for DM1 patients. Muscle weakness and cardiovascular risks may require diligent monitoring and tailored management during pregnancy and delivery. It is crucial to have proficient health care teams to manage those high-risk pregnancies and ensure optimal outcomes for both the mother and the baby. In addition, some studies suggest the need to address the increase in symptoms during pregnancy and the postpartum phase, which may require additional planning of services to support the family.
Additionally, addressing research gaps pertaining to other gynecological problems mentioned earlier and developing guidelines can contribute to better manage DM1-related complications. By expanding the scope of research and establishing comprehensive guidelines, health care professionals will improve their understanding and management of gynecological problems and obstetrical complications in DM1 patients, ultimately enhancing the quality of care provided to this population. Finally, our review highlighted a critical lack of evidence on treatment options for these issues.
Conclusion
Further research is needed to advance our understanding of gynecological problems and obstetrical complications in women with DM1. Studies with longitudinal design could provide valuable insights into the long-term impact, progression, recurrence, and preventive measures for these complications. Mechanistic investigations are necessary to explore the underlying mechanisms and pathophysiology, and to identify specific targets and pathways for potential therapeutic interventions.
Conducting interventional studies to evaluate the efficacy and safety of different treatment options to better manage gynecological problems and obstetrical complications in women with DM1 is also required. This may involve assessing the impact of lifestyle modifications, medication regimens, and specialized interventions aimed at reducing the burden of these complications.
Collaborative efforts should be made to develop comprehensive guidelines tailored specifically to health care providers to better manage gynecological problems and obstetrical complications in women with DM1. These guidelines should be evidence-based, incorporating the latest research findings, and providing clear recommendations for diagnosis, management, and follow-up care. By addressing these practical and research recommendations, health care providers can improve the care and quality of life for women with DM1, while expanding our understanding of these complex complications.
Authors’ Contributions
C.G. and M.M. contributed to the study design, project supervision, analysis and interpretation of the reviewed publications, and the review and editing of the article. C.S. and I.F.P. contributed to the scientific evaluation and article revision. A.Tamizi wrote the initial draft, revised it with input from all authors, and validated the initial data extraction. A.Tremblay and M.L. conducted the initial data extraction.
Footnotes
Ethics Approval
Ethics approval was not required for this scoping review.
Author Disclosure Statement
C.G. acts as a consultant for Vertex, Arthrex, Seelos, and Biogen. She also conducts academic work for Biogen, Ionis and Seelos, all unrelated to the present article. All other authors report no conflicts of interest.
Funding Information
This study was funded by the
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.