
Abstract
Objective:
Across the lifespan, more women than men report abdominal bloating. However, little is known about bloating during the menopause transition (MT). The purpose of this study was to assess patterns of bloating severity during the MT in relation to age, reproductive aging stage, reproductive- and stress-related biomarkers, and stress-related perceptions in a longitudinal cohort study.
Methods:
This analysis included 291 women from the Seattle Midlife Women’s Health Study who provided health diary data and could be classified into reproductive aging stages. A subset of 131 women also provided urine samples, which were assayed for estrone glucuronide, follicle-stimulating hormone, testosterone, cortisol, norepinephrine, and epinephrine levels. Mixed-effects multilevel modeling was used to examine the relationship between bloating severity and age, reproductive aging stages, reproductive- and stress-related biomarkers, and stress-related perceptions.
Results:
In the univariate model, the early MT stage, tension, and anxiety were associated with increased bloating severity, whereas the early postmenopausal stage and testosterone levels were associated with decreased bloating severity. In the multivariate model, both the early and late MT stages were related to an increase in bloating severity. Age and testosterone levels were associated with decreased bloating severity. Tension was related to increased bloating severity.
Conclusions:
Tension and anxiety may play a role in increased bloating severity, whereas testosterone levels and age are associated with decreased bloating severity. The MT stage may contribute to bloating through several mechanisms. More research is needed to fully elucidate these relationships.
Introduction
Bloating—the sensation of distention or stretching in the abdomen—is more common among women than men. 1 In a study of 88,795 Americans, 14% reported bloating during the past 7 days, with women reporting greater bloating severity. 2 Furthermore, the odds of bloating were higher among individuals younger than 60 years. 2 The increased prevalence of bloating among younger women leads to the hypothesis that sex steroid hormones, such as estrone, progesterone, and testosterone, may be related to the prevalence of bloating and/or its severity. However, knowledge about bloating is primarily derived from studies of women with conditions such as irritable bowel syndrome, endometriosis, and dysmenorrhea, which have a higher prevalence in younger women. Little is known about bloating severity and the factors associated with it across menopause transition (MT) stages in the general population.
Bloating is a complex symptom as an expansion of abdominal girth or distention does not always occur with reports of bloating.3,4 Potential physiological mechanisms of bloating may include delays in gastric emptying leading to postprandial fullness, foods such as certain carbohydrates (e.g., beans and dairy) that promote gas production, delays in colonic transit time leading to constipation, small intestinal bacterial overgrowth, the presence of dysbiotic gut bacteria associated with increased intraluminal gas production, inadequate expulsion of gas, and abdominal wall hypersensitivity. 5 Psychological factors have also been associated with bloating. Compared with women without bloating, women across the age spectrum with bloating report higher levels of anxiety and depression, lower global mental and physical health, increased somatization, greater abdominal pain severity, and higher levels of stress.4–6
Although sex steroid hormones and stress impact pain perception and may have similar influences on bloating reports, most studies of bloating have not used biological markers to ascertain reproductive or menopausal stage or physiological stress. Animal studies have demonstrated a relationship between sex and indices of chronic stress, such as cortisol. 7 Few studies have specifically targeted bloating during the MT, a period when sex steroid hormone levels are changing and self-reported stress levels may be increasing. The Seattle Midlife Women’s Health Study (SMWHS) collected longitudinal data on over 300 women to interrogate factors that could be related to symptoms during the transition from the late reproductive stage to postmenopausal stage. 8 Using these data, we previously examined both abdominal pain severity and bowel pattern characteristics, i.e., constipation and diarrhea, during the MT.9,10 Using multivariate model testing, both estrone and stress-related characteristics were positively associated with abdominal pain reports, whereas tension and cortisol were significant predictors of constipation severity. Building on these findings, we examined whether estrone, testosterone, reported stress level, and stress-related biomarkers were associated with the symptom of bloating, which we propose is distinct from abdominal pain and constipation. Given the limited literature on bloating across the MT, the aim of our study was to test bloating severity during the MT in relation to chronological age, reproductive aging stage, reproductive- and stress-related hormones, and perceptions of anxiety, tension, and stress.
Methods
Design and sampling
The data used in this study were gathered as part of the SMWHS, a prospective repeated-measures study conducted from 1990 to 2013 in the greater Seattle area. The SMWHS primarily focused on symptoms, reproductive-related and stress-related hormones, and perceived stress associated with natural MT, which is further elaborated elsewhere. 8 To summarize, participants were recruited from a population-based sample between 1990 and 1992. Inclusion criteria were women who were between 35 and 55 years of age, had experienced a menstrual period within the previous 12 months, were not pregnant or lactating, had at least one ovary and an intact uterus, and could read and speak English. Women who were interested in participating provided informed consent.
Details regarding study procedures can be found elsewhere. 8 Briefly, women completed a daily menstrual calendar each year to report occurrences of bleeding or spotting, as well as amount of bleeding. They also completed a health questionnaire each year that included questions such as reproductive aging, stress, and symptoms. A health diary was used as an additional data collection tool, but it was not a required for entering the longitudinal component of the study, and only a subset of the women agreed to complete it. The health diary was collected on days 5 through 7 of the menstrual cycle for those who were still cycling, for each month from the beginning of the study until the end of the year 2000, and quarterly from 2001 to 2013. Questions in the health diary included a symptom checklist with a severity scale, indicators of health behaviors, and stress-related perceptions. In 1996, a subset of women (N = 170) agreed to provide a monthly first-void urine specimen for biomarker analysis. This occurred on day 6 of the menstrual cycle, coinciding with health diary completion, until the end of 2005.
A total of 820 individuals were eligible, 508 provided initial cross-sectional data, and 390 began the longitudinal component of the study, which included annual data collection through daily menstrual calendars and annual health questionnaires. Participants remained in the study for up to 5 years post menopause. This current analysis includes a subset of 291 participants from the original cohort of 508 women. These women had complete diary entries and calendar data and had not used hormone therapy, undergone a hysterectomy, or received chemotherapy or radiation therapy. In addition, this subset of participants could be classified into one of the reproductive aging stages (see below). Of the 291 women meeting the above criteria, 131 also provided urine samples to be assayed for reproductive-related and stress-related biomarkers.
Measures
We analyzed the following measures: MT stages, urinary assays (reproductive-related and stress-related biomarkers), health diary data (anxiety, tension, and perceived stress), and the outcome measure of bloating severity.
Women were classified into reproductive aging stages based on menstrual calendar data, including late reproductive stage (LRS; STRAW −3), early menopausal transition (early MT; STRAW −2), late menopausal transition (late MT; STRAW −1), and postmenopause (PM; STRAW +1). These stages were defined using criteria developed for the SMWHS by Mitchell, Woods, and Mariella11,12 and validated by the ReSTAGE collaboration.13,14 The LRS was defined as the time during midlife when menstrual cycles were regularly occurring, with fewer than 7 days of variation between two consecutive cycles documented by calendar data, along with at least one menstrual cycle change during the past year compared with the previous year (longer or shorter cycle length, more or fewer number of days of flow, and/or greater or lesser amount of flow), as documented in the yearly questionnaire.12,14 Early MT was defined as persistent irregularity of more than 6 days of absolute difference between any two consecutive menstrual cycles within a calendar year, with no skipped periods. Late MT was defined as the persistent skipping of one or more menstrual periods. Amenorrhea for 60 or more days within a calendar year constituted a skipped period. Persistence was defined as a skipped period, irregular cycle, or event occurring one or more times during the 12 months following the initial occurrence of any one of these events. Early PM was defined as the 5 years after the final menstrual period (FMP). The FMP was retrospectively identified after 1 year of unexplained amenorrhea and was considered synonymous with the onset of menopause.
Health diary data
Primary outcome variable: Symptom severity
The severity of bloating was evaluated in the health diary by asking women to report the severity of bloating within the past 24 hours on a scale from 0 (“absent”) to 4 (“extreme”).
Stress-related perceptions
Stress-related perceptions were evaluated using items in the health diary. Participants responded to a list of symptoms that included anxiety, tension, and perceived stress. Anxiety and tension were assessed (separately) by asking women whether they had felt “anxious” or “tense,” respectively, during the past 24 hours. Women responded on a scale of 0–4, where 0 was “absent” and 4 was “extreme.” Perceived stress was assessed by the question: “How stressful was your day?” Reponses ranged from 1 and 6, where 1 was “not at all” and 6 was “extremely, a lot.”
Urine sample collection and biomarker analysis
Women collected first-void morning urine specimens at home. For those with a menstrual period, samples were collected on day 6 of the menstrual cycle. For those with menstrual periods that were unidentifiable or erratic, or for those whose menstrual periods had completely ceased, urine specimens were collected on a consistent monthly date.
8
Women abstained from smoking, exercise, and caffeine use before urine collection. Sodium metabisulfite and sodium ethylenediaminetetraacectic acid were used to preserve the urine samples. The samples were then collected and immediately frozen in the home freezer. They were later transported on ice to the research laboratory by research personnel and subsequently frozen at −70
Analysis
A mixed-effects model (using the R library) was used to investigate whether urinary reproductive and stress biomarkers, age, MT stage, and reported levels of anxiety, stress, and tension were significant predictors of bloating severity. Multilevel modeling was selected as data were collected at multiple time points over several years for each woman. To enhance the interpretability of the results, the sample mean age (47.6 years) was used in the analysis. A brief description of these models is presented below, and prior papers include a more extensive description.8,15
To determine the best-fitting model for analyzing the data, two models were tested. In the first model, we assumed that bloating severity varied between subjects but that it would consistently change according to age; this model used a random intercept and a fixed slope. In the second model, there was one variation from the previous assumptions: for each subject, the fixed slope was interchanged with a random slope. From this point on, age was replaced with MT stage as the predictor, and the previously described models were retested to determine if bloating severity differed between women but changed in a consistent (fixed slope) or random (random slope) manner according to MT stage. The two models were then tested using a likelihood ratio test and the Akaike information criterion.
Using the best-fitting model, individual covariate effects on bloating severity were independently inserted into the model. To analyze the data, the outcome observation (bloating) was paired with each predictor variable. These pairings were not consistent across covariates because the number of observations (n = 3,325–6,977) and the number of women (n = 130–291) varied for each covariate. Covariates with statistical significance (set at a p value of 0.05) upon independent insertion, that revealed an improved model fit to the data, were then inserted into the final model altogether.
Results
Demographics and clinical characteristics of the population have been published in full previously.9,10 In summary, participants at baseline had a mean age of 41.5 years (standard deviation: 4.3 years), and the majority were White (82%).
Age versus menopausal transition stage
Results showed that the best fit for the data (p < 0.001) was the random-effects model (Table 1). Chronological age, itself, was not a statistically significant predictor of bloating; however, MT stage itself showed two stages that were statistically significant: early MT (p < 0.02) and early PM (p < 0.002). Bloating increased in severity during early MT but decreased during early PM.
Age-Adjusted Associations With Bloating Severity
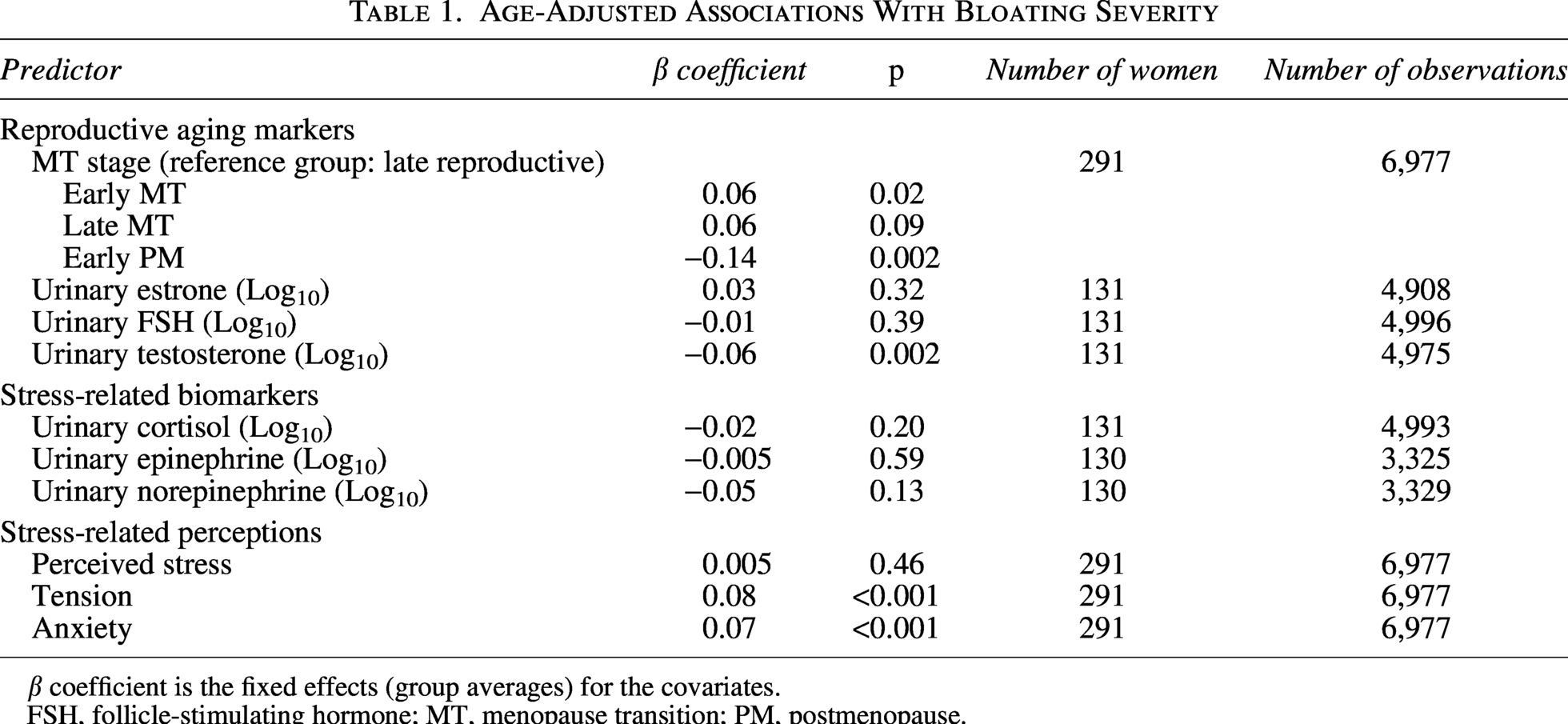
β coefficient is the fixed effects (group averages) for the covariates.
FSH, follicle-stimulating hormone; MT, menopause transition; PM, postmenopause.
Univariate analysis
Among the urinary reproductive biomarkers, only testosterone levels had a significant effect, showing a decrease in bloating severity (β = −0.06, p < 0.002). Among the stress-related perceptions, both tension and anxiety each showed statistically significant effects. Tension showed an increase in bloating severity (β = 0.08, p < 0.001), and anxiety an increase in bloating severity (β = 0.07, p < 0.001).
Multivariate analysis
All covariates that were statistically significant were then simultaneously entered into a multivariate random-effects model (Table 2). This model decreased the tested data to 131 women and 4,890 observations. While chronological age did not have statistically significant effects in the univariate analysis, in this model, age was related to a decrease in bloating severity of 0.04 (p < 0.001). Early MT stage remained statistically significant and was joined by late MT stage, with both associated with increases in bloating severity of 0.09 and 0.12, respectively (p < 0.02 and p < 0.01). Testosterone levels also remained statistically significant and were associated with a decrease in bloating severity of −0.06 (p < 0.002). Tension was associated with an increase in bloating severity of 0.05 (p < 0.003).
Multivariable Mixed-Effects Model Predicting Daily Bloating Severity (N = 131; Observations = 4,975)
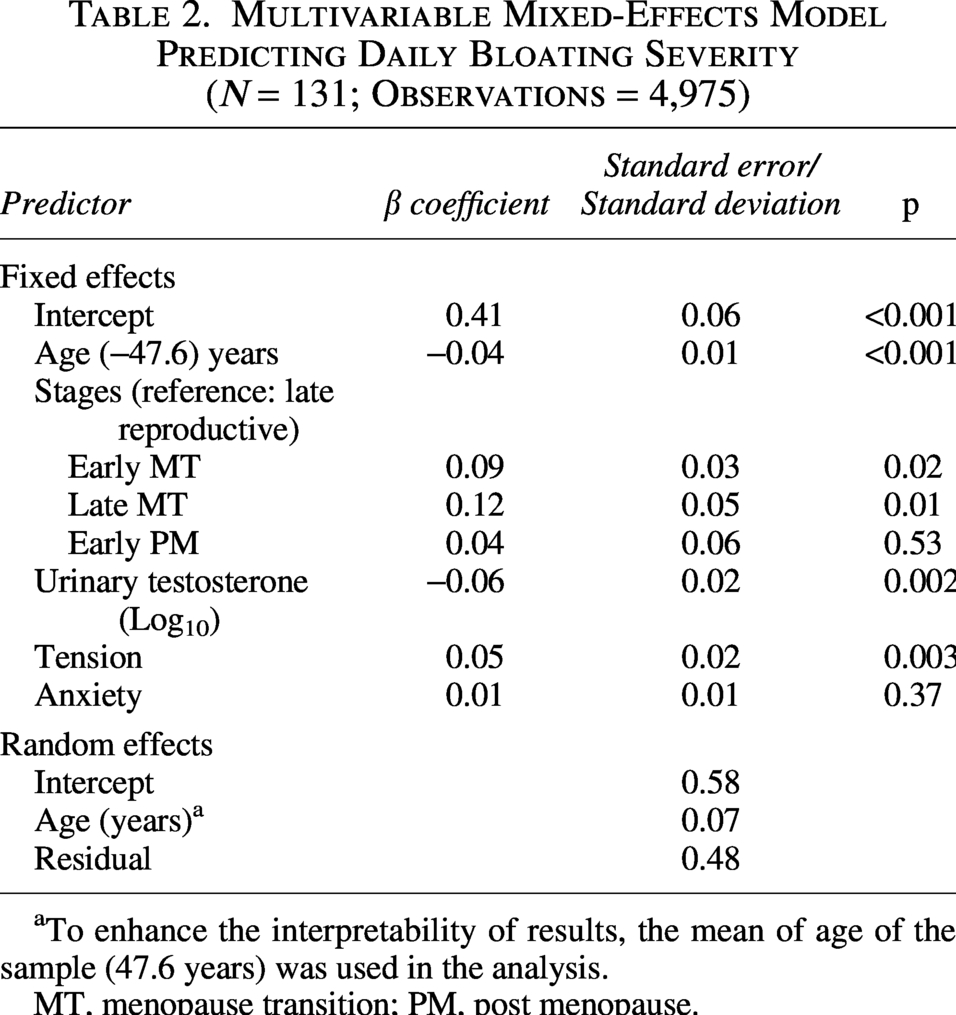
To enhance the interpretability of results, the mean of age of the sample (47.6 years) was used in the analysis.
MT, menopause transition; PM, post menopause.
Discussion
Although many women experience bloating, it is an understudied symptom that adversely impacts daily activities and quality of life.16,17 Our team sought to test physiological and psychological factors, in concert with chronological age and MT stage, and their relationships with women’s reports of bloating. Using a well-characterized cohort of women from the SMWHS and multivariate model testing, we found that, overall, early and late MT stages were associated with higher bloating severity. Urinary testosterone levels were associated with decreased bloating severity regardless of MT stage. Reports of tension were associated with increased bloating severity.
We found that higher urinary testosterone levels, but not estrogen or cortisol levels, were associated with lower bloating severity regardless of MT stage. Although there is some literature to support a role for testosterone in somatic pain sensitivity in animal models, human data are inconsistent.18,19 In a prior analysis done with this sample, we found no significant relationship between urinary testosterone levels and abdominal pain severity during the MT. 10 This suggests that testosterone’s relationship to the cause or perception of abdominal distension and/or fullness may be distinct from its effect on abdominal pain sensitivity. One possible mechanism is its effect on motility and intestinal transit. However, data regarding testosterone and motility may be animal-model specific. An early study in rats found no effect of testosterone on motility and gastric emptying rate. 20 In contrast, in mice, orchiectomy (i.e., the removal of testicles) results in both disorganized motility contraction patterns and decreased colonic transit time, supporting a link with gastrointestinal (GI) motor activity. 21 There are other potential mechanisms that may also explain our findings; thus, additional research is needed to further delineate the potential physiological relationship between testosterone and bloating.
In cross-sectional studies of gut–brain interaction, bloating often occurs with perceived abdominal distention, but not always.3,22 For example, an international survey of over 3,000 respondents (mean age 43 years) found that 26.5% of females, compared with 14.9% of men, reported the simultaneous occurrence of bloating and distention. 3 Using a latent class analysis approach, they identified six subgroups of individuals with bloating. 3 Some clusters included both bloating and distention, whereas others included predominantly bloating or predominantly distension. Future research is needed to distinguish among bloating, distention, gas, and pain, particularly among women throughout the MT stages.
Of the psychological factors tested in the multivariate modeling, reports of tension, but not anxiety or perceived stress, were found to be positively associated with bloating. While the link between psychological/emotional distress, including anxiety, and abdominal pain has been well established, the relationship between the physical sensation of tension and abdominal pain-related symptoms is less clear. 23 It is possible that feelings of tension represents a disturbance in the bidirectional gut–brain axis through a predominately peripheral mechanism. For example, few studies have examined whether bloating is due to abdominal wall tension or related to specific brain networks. To date, studies have either shown microstructural or network changes in women with bloating or found no differences.24,25 At the same time, the sensation of bloating, abdominal distention, or gas also brings psychological distress leading to feelings of tension. The Rome Foundation Global Epidemiology Study of 51,425 individuals across 26 countries reported that individuals with bloating were more likely to have symptoms of anxiety, as well as poor global mental and physical health. 5 Surprisingly, in our results, we did not find anxiety or perceived stress to be associated with bloating severity. However, we did find that tension was associated with an increase in bloating severity. In our previous work identifying symptom clusters during the MT, tension has been grouped together with depressed mood. 26 Interventions focused on methods to reduce tension, such as abdominal breathing, may also have the benefit of reducing bloating severity.
Bloating represents an important yet understudied symptom among women during the MT. Because bloating can be one of the first signs of ovarian cancer, women presenting with bloating should be evaluated for other red flags. 27 The American Gastroenterological Association Clinical Practice Guidelines for bloating recommend assessment for alarm symptoms (vomiting, weight loss, and GI bleeding), constipation, and food intolerances. 28 Whether a relationship exists between food intolerances and bloating among women in the MT represents an important area for future research. As bloating may be more closely associated with abdominal pain rather than bowel patterns, neuromodulators may be helpful for some women.22,28
A strength of our study is the robust characterization of MT phases and the use of biomarkers. A limitation is that we did not measure comorbid conditions, such as irritable bowel syndrome and functional dyspepsia, which commonly co-occur with bloating, or diet, which is often a trigger for bloating. At the start of the study, definitions for such comorbid conditions were still being developed. The primary purpose of the SMWHS was to examine symptoms, reproductive and stress-related hormones, and perceived stress associated with natural MT. 8 Since the primary purpose was not specific to GI symptoms, there are several GI symptom-specific confounders that were not collected. Future studies on GI symptoms, particularly bloating, should incorporate confounders including diet and food triggers, food intolerances, medications, stool form, and comorbid GI conditions. 29 Additionally, future studies should incorporate multiple GI symptoms, such as constipation and diarrhea, in the model to examine whether bowel habits mediate the relationship between the menopause transition and bloating. We found that tension was associated with bloating severity. Because participants self-reported this symptom, it is unclear how participants interpreted tension, such as muscle tension, stress-related tension, or something else. Additional research is needed to further examine the impact of tension and better understand its meaning among women during the MT.
Conclusions
Bloating, a symptom more common in women than in men, is typically studied during the menstrual cycle. We examined bloating among women during the MT and found that increasing age and higher urinary testosterone levels were associated with decreased bloating severity. In contrast, early and late MT stages, as well as tension, were associated with increased bloating severity.
Authors’ Contributions
K.J.K.: Writing—original draft (equal). N.G.L.C.: Writing—original draft (equal) and conceptualization. E.S.M.: Review and editing (equal); conceptualization; formal data analysis; and methodology. M.M.H.: Review and editing (equal). N.F.W.: Review and editing (equal); conceptualization; and funding acquisition.
Footnotes
Acknowledgments
The authors thank the participants of the SMWHS, whose contributions of time and attention made this study possible.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Institutes of Health (NIH), National Institute for Nursing Research (Grant Nos.: R01NR004141 and P30NR04001). The salary/stipend for N.G.L.C. was provided by the Department of Health and Human Services, Public Health Service, Ruth L. Kirchstein National Research Service Award (PHS Grant No. 5T90AT008544-03). K.J.K. was supported by the National Institutes of Health (Grant No.: K23NR020044).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.