
Abstract
Background:
Postpartum smoking adversely affects maternal and infant health outcomes. Although many women discontinue cigarette smoking during pregnancy, relapse patterns remain underexplored.
Objective:
To estimate the prevalence and identify demographic and behavioral correlates of postpartum smoking relapse among women who exclusively smoked cigarettes before pregnancy and discontinued smoking during pregnancy.
Methods:
We analyzed 2016–2022 Pregnancy Risk Assessment Monitoring System data to examine postpartum smoking relapse among 15,981 women (weighted population: 770,973) who reported exclusive prepregnancy cigarette smoking and discontinued smoking during pregnancy. Weighted frequency estimates and logistic regression were used to evaluate the prevalence of postpartum smoking relapse and its associated factors, with results reported as adjusted odds ratios (AORs) and 95% confidence intervals (CIs). Sensitivity analysis excluding postpartum covariates was also performed.
Results:
Postpartum smoking relapse occurred in 39.8% (95% CI:38.6–41.0) of women who quit smoking during pregnancy. Higher odds of relapse were observed among women aged below 20 years [AOR:1.7 (95% CI:1.3–2.4)], non-Hispanic Black women [AOR:1.6 (95% CI: 1.3–1.9)], and multiparous women [AOR: 1.6 (95% CI: 1.4–1.8)]. Mothers who never breastfed [AOR: 4.0 (95% CI: 3.3–4.8)] or discontinued breastfeeding [AOR: 3.1 (95% CI: 2.7–3.6)] had significantly greater relapse odds compared with those who continued breastfeeding. Sensitivity analysis excluding postpartum factors yielded similar associations with younger age, non-Hispanic Black race, and multiparity.
Conclusion:
Postpartum smoking relapse is common among women who were exclusive cigarette smokers before pregnancy and discontinued smoking during pregnancy and is associated with distinct demographic and behavioral factors. Postpartum cessation support targeting high-risk groups may improve maternal and infant health outcomes.
Keywords
Introduction
Smoking cigarettes during pregnancy is associated with impaired fetal growth and a higher risk of adverse perinatal outcomes.1,2 Pregnancy motivates women to quit smoking. 3 However, relapse after childbirth is common, with nearly half of women resuming smoking by the first six months postpartum. 4 Postpartum smoking exposes infants to secondhand smoke, which increases the risk of sudden infant death syndrome, respiratory infections, asthma, and neurodevelopmental and behavioral problems.5,6 It also negatively impacts maternal health by maintaining nicotine dependence.
Smoking is declining among pregnant women in the United States.7,8 Women who continue smoking during pregnancy and those who relapse after quitting account for most postpartum smokers.9,10 Quit rates and associated demographic and behavioral factors vary widely across different product types.3,11–13 Quitting is also influenced by the intensity of prepregnancy tobacco use, suggesting a dose–response relationship. Quit rates among exclusive cigarette users (50–55%) are higher than dual-users of cigarettes and electronic cigarettes (45–50%) but lower than exclusive electronic cigarette users (75–80%).3,11–13
Lower educational attainment, Medicaid coverage or participation in the Women, Infants, and Children (WIC) nutritional assistance program, unmarried status, multiparity, and a history of depression or abuse are each associated with reduced odds of quitting smoking during pregnancy.3,11,13 Conversely, Hispanic ethnicity is associated with higher odds of quitting cigarette use.
Studies based on Pregnancy Risk Assessment Monitoring System (PRAMS), a state-based surveillance system, indicate that postpartum smoking rates are lower than prepregnancy levels but remain higher than rates during pregnancy.8–10 Racial and ethnic differences are evident, with higher rates among non-Hispanic Black mothers.9,14,15 Longitudinal analyses integrating PRAMS data show higher relapse rates among women aged 18–24 years and among those with Medicaid coverage. 9 In addition, postpartum women receive less smoking cessation counseling from healthcare workers than women before and during pregnancy, 10 highlighting a gap in continuity of care.
PRAMS provides a unique opportunity to examine exclusive cigarette use before and during pregnancy, including quitting and postpartum smoking relapse behaviors. 16 We hypothesized that the correlates of women who relapse after discontinuing smoking during pregnancy differ from those who remain abstinent postpartum. Accordingly, this study uses PRAMS Phase 8 data to estimate the prevalence of postpartum smoking relapse and identify associated demographic and behavioral factors associated with relapse among pregnancy quitters. Understanding these patterns can inform targeted cessation strategies, support sustained abstinence, and reduce smoking in subsequent pregnancies.
Methods
Study design and dataset
This study is a secondary analysis of the cross-sectional PRAMS Phase 8 dataset covering the 2016–2022 cycles, obtained from the Centers for Disease Control and Prevention PRAMS portal. PRAMS is a population-based, state-specific surveillance system designed to monitor maternal behaviors before, during, and shortly after pregnancy among women with live births.16,17 The survey employs a mixed-mode data collection approach, comprising self-administered questionnaires and telephone interviews.
Each participating site samples between 1,000 and 3,000 women annually, selected from birth certificate records to ensure representativeness. Questionnaires are mailed to mothers 2–4 months after delivery, with telephone follow-ups for nonrespondents over the subsequent 2–4 weeks. Thus, PRAMS provides valuable information on maternal behavior during the extended postpartum period, up to ∼4 to 6 months. To improve precision for priority populations, PRAMS oversamples specific subgroups and employs stratified sampling by maternal age, race and ethnicity, infant birth weight, and geographic area. Only states that meet the minimum response-rate requirements are included in the public dataset (≥55% for 2015–2017 and ≥ 50% for 2018–2022).
The dataset is de-identified and also incorporates selected variables from birth certificates. The states included in this study, along with their years of participation, are listed in Supplementary Table S1.
Study population, outcome measures, and operational definitions
Of the 249,970 respondents (weighted count: 12,275,282) in PRAMS Phase 8, our study population comprised women who exclusively smoked cigarettes during the three months before pregnancy (weighted count: 1,418,454) and discontinued them in the last three months of pregnancy (weighted count: 770,973) and also provided information on smoking status at the time of the survey (Fig. 1).
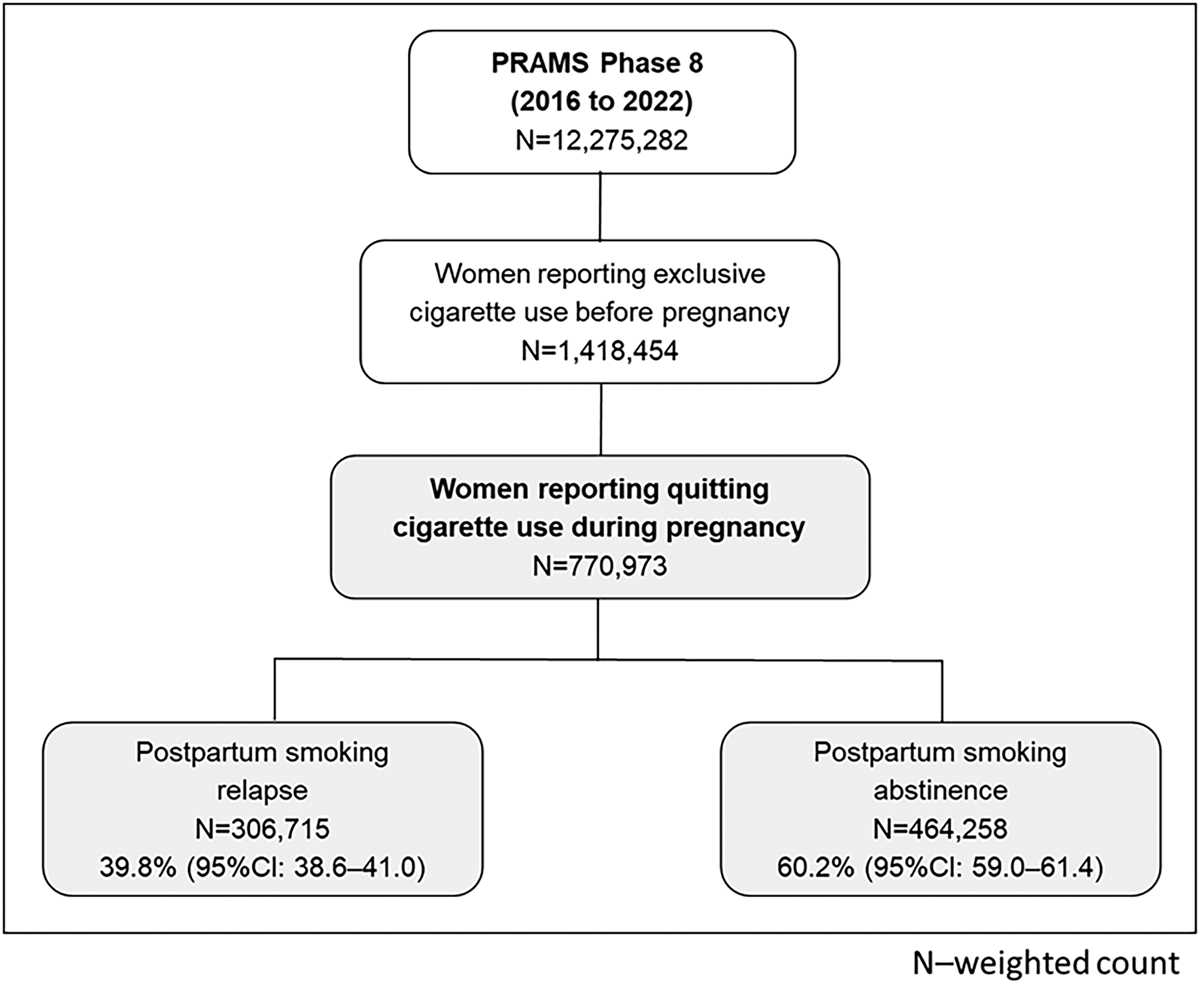
Study population selection (PRAMS Phase 8, 2016–2022). PRAMS, Pregnancy Risk Assessment Monitoring System.
Women with incomplete information on cigarette and/or electronic cigarette use before and during pregnancy, or incomplete information on cigarette smoking at the time of survey, were excluded. Smoking cessation during the last three months of pregnancy was used to define quitting behavior to align with the availability of electronic cigarette use data. Coding definitions used to create this variable are detailed in Supplementary Table S2.
Furthermore, among the study population, those who reported cigarette smoking at the time of the survey were classified as the risk group (postpartum smoking relapse), whereas those who did not were classified as the reference group (postpartum smoking abstinence).
Covariates
Covariates and their reference groups were selected based on existing literature on maternal smoking behaviors.9,14,15,18–20 These included age, race and ethnicity, education, Medicaid coverage during pregnancy, WIC participation, marital status, pregnancy intention, parity (primiparous or multiparous), plurality (single or multiple gestations), Kotelchuck Index (Adequacy of Prenatal Care Utilization or APNCU), infant maturity and birth weight, breastfeeding status, postpartum insurance coverage, and postpartum depression. Prepregnancy smoking intensity was also included as a covariate.
Sociodemographic variables, including age, education, ethnicity, and race, were recategorized into aggregated groups (Supplementary Table S2) to simplify analysis, reduce model overfitting, and improve statistical power. Ethnicity and race data were classified into four mutually exclusive categories: Hispanic, non-Hispanic White, non-Hispanic Black, and Other (including American Indian, Alaskan Native, Pacific Islander, Asian, or multiracial).
Income was excluded due to nonuniform PRAMS coding across states (46 categories), which limited comparability and resulted in approximately 8% missingness when collapsed. Instead, Medicaid coverage and WIC participation were used as standardized proxies, as they reliably capture low-income status, have lower missingness, and are more consistent across states. Marital status, pregnancy intention, parity, plurality, and the Kotelchuck Index affect maternal decisions to continue abstinence. However, postpartum smoking counseling by health care workers was excluded due to 13% missingness.
The postpartum period involves adjustment to a new maternal identity, which may heighten vulnerability to relapse as women navigate competing demands, stressors, and coping behaviors. 21 Postpartum covariates were chosen to reflect these influences on smoking relapse after childbirth. Reference groups were selected based on sample stability rather than solely on the lowest-risk status. The “less than high school” group comprised only 17.5% of the sample (Supplementary Table S3). In contrast, the “high school or equivalent” group provided a more stable (69.8%) and statistically robust reference category.
Statistical analysis
All analyses were performed using IBM SPSS Statistics version 20 with the survey-weighted package. All estimates incorporated survey weights, strata, and primary sampling units, following PRAMS analytic guidelines to produce population-representative results. Listwise deletion was applied to records with missing covariate data, as missingness was infrequent (Supplementary Table S3).
The period prevalence of postpartum smoking relapse among exclusive smokers who discontinued smoking during pregnancy was estimated using crosstabs. The associations between demographic and behavioral factors and postpartum smoking relapse compared with continued abstinence were analyzed using logistic regression models. Results were presented as odds ratios (ORs) and adjusted odds ratios (AORs) with 95% CIs. Statistical significance was set at p < 0.05.
Interaction terms were evaluated in a multiple logistic regression model to assess potential joint effects of predictors on the outcome. In weighted multiple logistic regression, statistical significance for categorical variables was assessed using overall Wald tests, whereas AORs with 95% CIs were used to interpret associations for individual categories. In cases of discordance between p-values and CIs, interpretation was guided primarily by the CIs.
Sensitivity analyses were conducted by reestimating models with and without postpartum covariates to assess the robustness of the findings. We chose sensitivity analyses over multiple imputation because the overall level of missingness in the covariates was <5%. In addition, multiple imputation is complex to implement in PRAMS due to its survey design, which incorporates weighting, stratification, and socially sensitive, trimester-specific responses.
Ethics approval
This study analyzed publicly available, de-identified PRAMS Phase 8 data. Because no identifiable private information was accessed, this analysis was deemed exempt from Institutional Review Board (IRB) review (Reference number: AUAIRBa25003, August 2025). As the dataset contained no direct subject identifiers, informed consent was not required.
Results
Among the 1,418,454 women who reported exclusive smoking before pregnancy, 770,973 [54.4% (95% CI: 53.4, 55.3)] reported quitting during pregnancy. Overall, postpartum smoking relapse was observed in 306,715 women, accounting for 39.8% (95% CI: 38.6–41.0) among those who discontinued smoking during pregnancy (Fig. 1).
The demographic and behavioral characteristics of women who quit smoking during pregnancy are shown in Supplementary Table S3. Compared with women who continued smoking during pregnancy, those who quit were more often younger (<25 years), Hispanic, and had higher educational attainment (bachelor’s degree or above). They were also more likely to be married, to have a planned pregnancy, to be primiparous, and to report adequate PNC utilization. In contrast, women with less than a high school education, WIC participation, and Medicaid coverage were more likely to be classified as persistent users.
Supplementary Table S4 presents the weighted prevalences and unadjusted ORs for demographic and behavioral characteristics associated with postpartum smoking relapse compared with continued abstinence among those who discontinued smoking during pregnancy. Most demographic and behavioral correlates, including young maternal age (<25 years), non-Hispanic race, less than high school education, unmarried status, unintended pregnancy, Medicaid coverage and WIC participation during pregnancy, multiparous status, and inadequate PNC utilization, showed statistically significant associations with relapse. Other postpartum correlates independently associated with smoking relapse included having a preterm or low birth weight infant, non-breastfeeding status, and experiencing depression after childbirth. However, multiple gestations and postpartum insurance were not significantly associated with smoking relapse. Relapse was also not associated with the number of cigarettes smoked before pregnancy.
In adjusted models (Table 1), several factors remained independently associated with postpartum smoking relapse. Non-Hispanic Black race [AOR: 1.6 (95% CI: 1.3–1.9)] compared with non-Hispanic White, multiparity [AOR: 1.6 (95% CI: 1.4–1.8)] compared with primiparity, and breastfeeding behavior were consistently associated with higher odds of relapse across discontinued product groups. Young maternal age was also significantly associated with smoking relapse, with women aged <20 years having 1.7-fold higher odds of relapse [AOR: 1.7 (95% CI: 1.3–2.6)] compared with women aged 25–34 years, whereas those aged 20–24 years also had 1.3-fold higher odds [AOR: 1.3 (95% CI: 1.1–1.5)]. Married status, planned pregnancy, and adequacy of PNC utilization did not influence smoking relapse.
Adjusted Associations of Demographic and Behavioral Correlates of Postpartum Smoking Relapse among Women Who Quit Cigarettes During Pregnancy, with Sensitivity Analysis Excluding Postpartum Correlates (PRAMS Phase 8, 2016–2022)
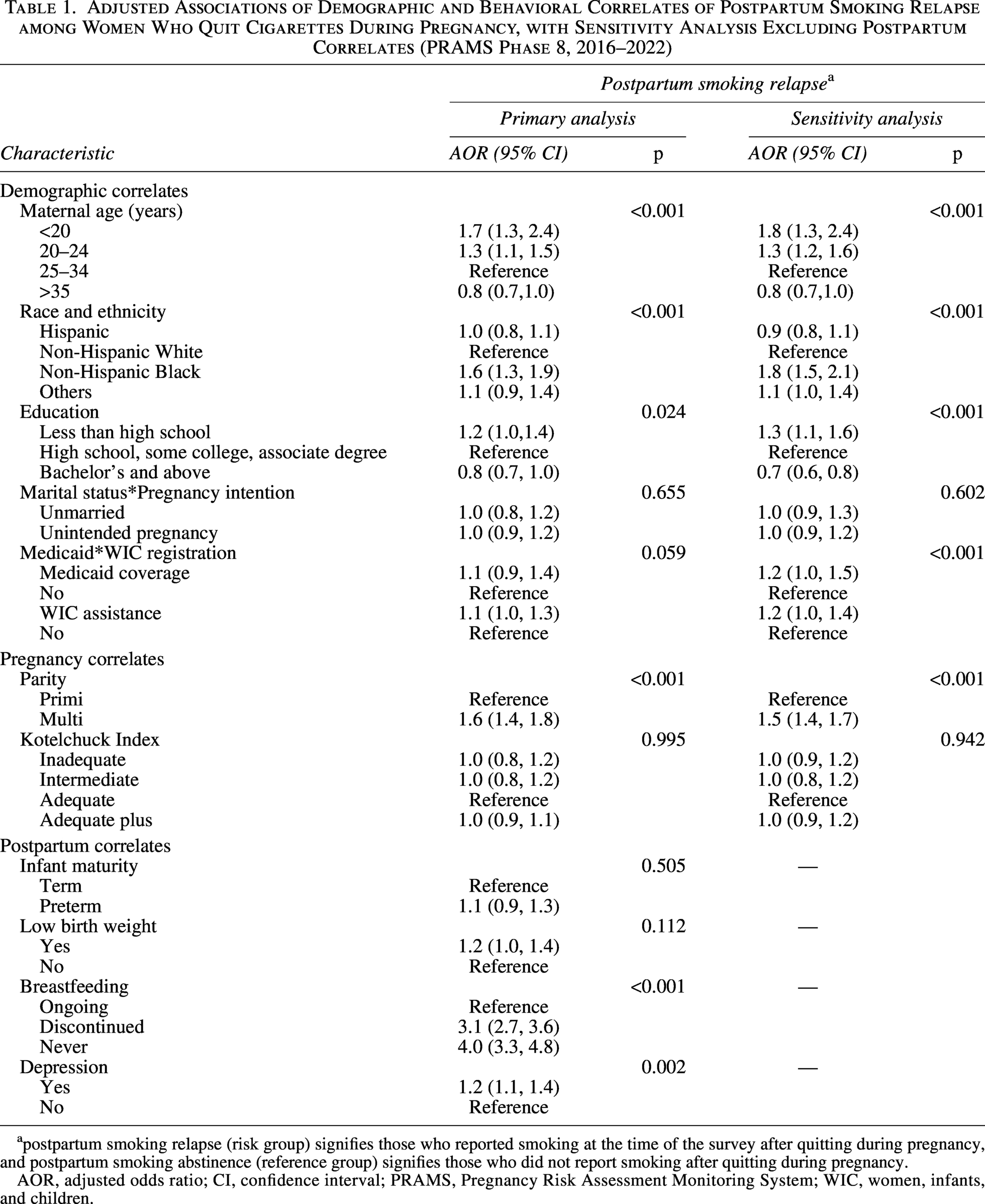
postpartum smoking relapse (risk group) signifies those who reported smoking at the time of the survey after quitting during pregnancy, and postpartum smoking abstinence (reference group) signifies those who did not report smoking after quitting during pregnancy.
AOR, adjusted odds ratio; CI, confidence interval; PRAMS, Pregnancy Risk Assessment Monitoring System; WIC, women, infants, and children.
Among postpartum correlates, breastfeeding demonstrated a graded association, with mothers who had never breastfed [AOR: 4.0 (95% CI: 3.3–4.8)] showing higher relapse risk than those who had discontinued early [AOR: 3.1 (95% CI: 2.7–3.6)], compared with mothers who were still breastfeeding at the time of the survey. Only 19.2% (95% CI: 17.7–20.8) of mothers who relapsed reported breastfeeding, compared with a 49.0% (95% CI: 47.4–50.6) among those who remained abstinent. Relapse was also associated with mothers reporting depression [AOR: 1.2 (95% CI: 1.1–1.4)]. Multiple gestations, prematurity, and low birth weight were not associated with smoking relapse.
Sensitivity analysis excluding postpartum behavioral covariates showed consistent and robust associations, particularly for non-Hispanic Black race [AOR: 1.8 (95% CI: 1.5–2.1)] and multiparity [AOR: 1.5 (95% CI: 1.4–1.7)]. Additional significant correlate included less than a high school education [AOR: 1.3 (95% CI: 1.1–1.6)] compared with those who completed high school education.
Discussion
In this population-based study using PRAMS Phase 8 data, we examined the associations of postpartum smoking relapse among women who exclusively smoked cigarettes before pregnancy and discontinued smoking during pregnancy. Approximately 4 in 10 women who quit resumed smoking within 6 months postpartum. Regression models indicated that younger age, non-Hispanic Black race, and multiparity notably increased the risk of relapse. Breastfeeding behavior showed graded associations among women who either discontinued or never breastfed.
Postpartum smoking prevalence is approximately 5.7% in recent national estimates and reflects the continued long-term decline in postpartum smoking from 18.9% to 8.8% between 2000 and 2020.8,9 However, relapse among pregnancy quitters remains substantial, with nearly 40% resuming smoking, consistent with prior reports of ∼40% to 45% relapse in the early postpartum period.14,15 This highlights a persistent gap between declining overall prevalence and sustained abstinence after pregnancy. Together, these findings underscore the need for continued postpartum cessation support, as reductions in smoking prevalence have not translated into meaningful declines in relapse.
The demographic and behavioral associations observed in our study are consistent with previous research on postpartum smoking relapse.14,15 Non-Hispanic Black women consistently report higher smoking prevalence than non-Hispanic White women. Smoking patterns in this group often start with comparatively lower use during adolescence but increase into young adulthood, along with lower cessation success than other racial and ethnic groups. 22 Although smoking has decreased since the early 2010s, the declines have been modest and mostly limited to the pregnancy period.8,23 Notably, the non-Hispanic Black demographic was the only group without a significant decrease in postpartum smoking between 2000 and 2020. 8 These ongoing disparities stem from structural barriers, chronic stressors, and unequal access to healthcare, highlighting the importance of culturally responsive, equity-focused cessation interventions.22,24
Young maternal age, multiparity, and depression after childbirth emerged as correlates of higher relapse risk, likely reflecting cumulative demands of caregiving, competing priorities, heightened stress, and limited time and opportunity for sustained cessation support. Younger age is a robust predictor of relapse,9,19 though they are among the largest quitters during pregnancy.7,9 Smoking is disproportionately concentrated among low-income adolescents, likely reflecting higher nicotine dependence, fewer resources for cessation, and multiple life stressors during early motherhood. Younger postpartum women also experience substantially higher insurance churn and fewer transitions into employer-sponsored insurance.18,25 A high school education or less, compared with college graduation, was also significantly associated with relapse in the sensitivity analysis, corroborating previously published literature.8,9
Breastfeeding demonstrated the strongest association with sustained postpartum abstinence in our study, with a clear gradient of increasing relapse among women who discontinued or never initiated breastfeeding compared with those who were currently breastfeeding. This aligns with prior cohort studies showing markedly lower relapse rates with longer breastfeeding duration.26–28 In their cohort of women who discontinued smoking during pregnancy, Issany et al. 26 observed reductions from nearly 60% among non-breastfeeding mothers to <25% among those breastfeeding for at least three months, with further declines at six months and beyond.
However, the temporality remains unclear. Given the cross-sectional design of PRAMS, it cannot be determined whether breastfeeding promotes abstinence or whether women committed to abstinence are more likely to breastfeed. The association is also likely influenced by shared sociodemographic and behavioral factors, including maternal age, race/ethnicity, education, parity, and breastfeeding intention. Multiparity and lower educational attainment, both linked to shorter breastfeeding duration, are also associated with higher relapse risk, whereas racial disparities in breastfeeding initiation and maintenance, particularly among non-Hispanic Black women, may further contribute to differences in smoking trajectories.29–31
Several biological and behavioral mechanisms may underlie this relationship, although they remain largely hypothetical. Nicotine concentrates in breast milk and has been linked with reduced milk production, shorter lactation duration, and impaired infant suckling. 32 Nicotine-related suppression of prolactin and altered feeding patterns may disrupt lactation, whereas changes in milk taste may decrease feeding time. Conversely, breastfeeding may support abstinence through oxytocin-mediated stress relief, maternal–infant bonding, and motivation to prevent infant nicotine exposure. These bidirectional influences suggest a complex relationship between smoking and breastfeeding. Since both behaviors are shaped by social factors, structural barriers, and caregiving demands, access to postpartum support is crucial. Interventions that combine breastfeeding support with smoking cessation among high-risk groups, such as multiparous and socioeconomically disadvantaged women, may provide dual advantages.
In contrast, socioeconomic disadvantage, reflected by unmarried status, unintended pregnancy, inadequate PNC utilization, Medicaid coverage, and WIC participation, is strongly associated with persistent smoking during pregnancy.3,8,11,23,25,33 Although these factors were associated with higher crude relapse prevalence among pregnancy quitters, their adjusted effects were attenuated, indicating they primarily characterize continued smoking during pregnancy rather than postpartum relapse. Medicaid beneficiaries have higher smoking rates before, during, and after pregnancy despite access to cessation services.9,34 Contrary to other studies,8,35 prepregnancy smoking intensity and PNC utilization adequacy did not independently predict postpartum relapse among women who quit during pregnancy, suggesting the need for continued counseling after childbirth.
Implications for practice and policy
These findings highlight the need to extend tobacco cessation support beyond pregnancy, with focused attention on younger mothers, non-Hispanic Black women, multiparous women, and those facing socioeconomic disadvantage. Postpartum care should strengthen smoking-cessation follow-up, integrate counseling into WIC, Medicaid postpartum services, and infant well-visits, promote breastfeeding as a dual-benefit strategy, and routinely assess partner or household smoking.
Digitally delivered contingency management interventions can substantially enhance smoking abstinence during pregnancy. These scalable, remote strategies are especially relevant for populations with limited access to in-person cessation services, including rural and socioeconomically disadvantaged women, emphasizing an important route for expanding postpartum relapse prevention efforts.36,37 Tailored approaches for e-cigarette and dual users are essential, along with policies that expand Medicaid cessation coverage, enhance postpartum home-visiting supports, and embed cessation modules in telehealth platforms.
Strengths and limitations
Strengths of this study include the use of a large, nationally representative dataset, the inclusion of 45 states and jurisdictions across seven years, standardized data collection, and population-weighted estimates. The analysis specifically focuses on women who quit cigarettes during pregnancy, a clinically relevant group with limited population-based evidence.
Limitations include the cross-sectional design, which restricts causal inference and limits understanding of temporal dynamics. PRAMS excludes women with pregnancy losses and does not follow participants longitudinally, which may underestimate relapse occurring after the survey window. All smoking measures are self-reported and subject to social desirability bias, particularly during pregnancy and postpartum. Because the study was restricted to women who exclusively smoked cigarettes before pregnancy and subsequently quit, cessation during the last three months of pregnancy was used to define quitting behavior to align with the availability of electronic cigarette use data. This approach may have overestimated quitting rates by not accounting for smoking earlier in pregnancy. 38 Importantly, PRAMS do not assess postpartum e-cigarette use or other nicotine products, potentially underestimating total relapse. Residual confounding from unmeasured factors, such as partner smoking20,35 and nicotine dependence severity, is possible. Sensitivity analysis that excludes postpartum correlates mitigates concerns about temporality and possible reverse causation.
Conclusion
Postpartum smoking relapse remains a significant public health issue, with one in two to three women who quit during pregnancy resuming smoking within six months after childbirth. Relapses are heavily influenced by demographic and behavioral factors, and disparities persist. Enhancing postpartum cessation support integrated with breastfeeding promotion is crucial for maintaining abstinence, decreasing infant secondhand smoke exposure, and improving maternal and infant health outcomes.
Authors’ Contributions
R.D.S., L.W., and J.M.A. conceived the study objectives. R.D.S. accessed the dataset. S.G.S. and D.D. organized and curated the data under the supervision of R.D.S., L.W., and J.M.A. The data analysis, tabulations, data interpretation, and article draft were collaborative efforts involving all authors: S.G.S., D.D., R.D.S., L.W., and J.M.A. Both S.G.S. and D.D. qualify as first authors. R.D.S. and L.W. will be the guarantors responsible for the data reported in the article. J.M.A. will be the senior author of the article. All authors have read the article, agree with the decision to submit it, and accept responsibility for its contents.
Footnotes
Acknowledgments
The authors thank the PRAMS Working Group, which includes the PRAMS Team, Division of Reproductive Health, CDC, and the following PRAMS sites for their role in conducting PRAMS surveillance and allowing the use of their data: PRAMS Alabama, PRAMS Alaska, PRAMS Arkansas, PRAMS Arizona, PRAMS Colorado, PRAMS Delaware, PRAMS District of Columbia, PRAMS Georgia, PRAMS Hawaii, PRAMS Illinois, PRAMS Indiana, PRAMS Kansas, PRAMS Kentucky, PRAMS Louisiana, PRAMS Maine, PRAMS Maryland, PRAMS Massachusetts, PRAMS Michigan, PRAMS Minnesota, PRAMS Mississippi, PRAMS Missouri, PRAMS Montana, PRAMS Nebraska, PRAMS New Hampshire, PRAMS New Jersey, PRAMS New Mexico, PRAMS New York City, PRAMS New York State, PRAMS North Dakota, PRAMS Northern Mariana Islands, PRAMS Oregon, PRAMS Pennsylvania, PRAMS Puerto Rico, PRAMS Rhode Island, PRAMS South Dakota, PRAMS Tennessee, PRAMS Utah, PRAMS Vermont, PRAMS Virginia, PRAMS Washington, PRAMS West Virginia, PRAMS Wisconsin, PRAMS Wyoming.
Ethical Approval
The study is a secondary analysis of de-identified data provided by the CDC and did not involve a consent process. The Institutional Review Board approved the study protocol.
Consent to Participate
Not applicable; secondary analysis of de-identified data provided by the CDC.
Consent for Publication
Article copy is being submitted to PRAMS-CDC before submission to journal as per data download agreement.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.