
Abstract
Background:
Polycystic ovary syndrome (PCOS) has been associated with adverse pregnancy outcomes, although reported risks vary across studies. Metabolic heterogeneity within PCOS may contribute to this variability. Dysglycemia during pregnancy may identify a subgroup at increased obstetric risk. The study aims to evaluate whether dysglycemia is associated with preeclampsia and other adverse pregnancy outcomes among individuals with PCOS.
Methods:
We performed a secondary analysis of the prospective Fatty Liver in Pregnancy (FLIP) cohort (n = 1,321). PCOS was defined by chart review of the electronic health record. Dysglycemia was defined as current or prior gestational diabetes, abnormal glucose tolerance testing, hemoglobin A1c > 5.7% during pregnancy, or pregestational diabetes. Participants were categorized as PCOS with dysglycemia (n = 36), PCOS without dysglycemia (n = 44), or non-PCOS controls (n = 1,238). The primary outcome was preeclampsia. Secondary outcomes included gestational hypertension, preterm birth, abnormal neonatal weight, and neonatal hypoglycemia. Multivariable logistic regression adjusted for maternal age and body mass index.
Results:
Among 80 individuals with PCOS, 45% had evidence of dysglycemia. Preeclampsia occurred in 33% of those with PCOS and dysglycemia, 7% of those with PCOS without dysglycemia, and 12% of controls (p = 0.005 for PCOS with dysglycemia versus controls). In adjusted analyses, PCOS with dysglycemia was associated with preeclampsia (odds ratio [OR] 2.9; 95% confidence interval [CI]: 1.4–6.1), whereas PCOS without dysglycemia was not (adjusted odds ratio [aOR] 0.53; 95% CI: 0.16–1.73). PCOS with dysglycemia was also associated with increased preterm birth (OR: 2.3; 95% CI: 1.04–5.14), abnormal neonatal weight (OR: 2.87; 95% CI: 1.36–6.10), neonatal hypoglycemia (OR: 2.8; 95% CI: 1.38–5.77), and any adverse pregnancy outcome (aOR: 4.49; 95% CI: 1.94–10.40).
Conclusions:
In this prospective cohort, dysglycemia was associated with higher rates of hypertensive and metabolic pregnancy complications among individuals with PCOS. These findings suggest that coexisting dysglycemia may contribute to heterogeneity in obstetric risk among individuals with PCOS and warrant confirmation in larger studies.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder among reproductive-aged women and has been associated with a range of adverse pregnancy outcomes, including gestational diabetes, hypertensive disorders of pregnancy, and preterm birth.1–3 Meta-analyses have reported increased odds of preeclampsia and gestational diabetes among individuals with PCOS, though substantial heterogeneity exists across studies.1,3–6 Some large population-based cohorts demonstrate modest increases in hypertensive morbidity, whereas others have found attenuated or nonsignificant associations after adjustment for body mass index (BMI) and other confounders.2,7
One potential explanation for this variability is the phenotypic heterogeneity of PCOS. PCOS encompasses a spectrum of reproductive and metabolic abnormalities, including hyperandrogenism, obesity, insulin resistance, and impaired glucose metabolism.8–10 Metabolic dysfunction has been proposed as a key modifier of obstetric risk within PCOS.6,11–13 Dysglycemia, defined broadly as impaired glucose metabolism, is common among individuals with PCOS and may serve as a clinically measurable marker of metabolic vulnerability.14,15
Pregnancy represents a physiological state of increased insulin resistance, potentially unmasking underlying metabolic dysfunction. 16 Because routine prenatal care includes glucose screening, dysglycemia during pregnancy offers a pragmatic opportunity to examine whether metabolic abnormalities are associated with obstetric risk among individuals with PCOS. We therefore evaluated whether dysglycemia was associated with preeclampsia and other adverse pregnancy outcomes among individuals with PCOS in a prospective cohort.
Materials and Methods
Study design and population
We conducted a secondary analysis of the Fatty Liver in Pregnancy (FLIP) cohort, a prospective study of 1,321 pregnant individuals recruited between 2019 and 2024 at a single urban academic medical center to evaluate predictors and outcomes of steatotic liver disease in pregnancy. The study protocol was approved by the Program for the Protection of Human Subjects at the Icahn School of Medicine at Mount Sinai (STUDY-20-02146).
Exposure definitions
PCOS was identified by chart review of the electronic health record for documentation of PCOS in problem lists, past medical history, or clinical encounter notes. Dysglycemia was defined by documentation of any of the following during the index pregnancy or historically: current gestational diabetes mellitus, a history of gestational diabetes in a prior pregnancy, a positive 1-hour 50-g glucose challenge test, a positive 3-hour 100-g glucose tolerance test, hemoglobin A1c ≥ 5.7% during pregnancy, or pregestational diabetes. 17
Participants were categorized into three groups: (1) PCOS with dysglycemia, (2) PCOS without dysglycemia, and (3) non-PCOS controls.
Outcomes
The primary outcome was preeclampsia, defined according to American College of Obstetricians and Gynecologists (ACOG) criteria. 18 Secondary outcomes included gestational hypertension, 18 preterm birth (<37 weeks gestation), abnormal neonatal weight (large for gestational age [LGA] or small for gestational age [SGA], defined as birthweight >90th or <10th percentile for gestational age using the Fenton growth chart reference 19 ) and neonatal hypoglycemia documented in the neonatal record. We additionally examined a composite of any adverse pregnancy outcome, defined as the occurrence of any of the above five outcomes.
Statistical analysis
Baseline characteristics were compared using Fisher’s exact test for categorical variables and t-tests for continuous variables. Multivariable logistic regression models were used to evaluate associations between exposure groups and each outcome. Models were adjusted for maternal age and BMI at the first prenatal visit. Aspirin use during pregnancy and parity was evaluated in sensitivity analyses. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported. We additionally tested for an interaction between PCOS and dysglycemia on preeclampsia risk. All tests were two-sided with p < 0.05 considered statistically significant. Statistical analyses were performed using Stata version 19 (StataCorp, College Station, TX).
Results
Cohort characteristics
Among 1,321 participants, 80 (6%) had a documented diagnosis of PCOS. Of these, 36 (45%) had evidence of dysglycemia and 44 (55%) did not. The remaining 1,238 individuals comprised the non-PCOS control group. Compared with non-PCOS controls, individuals with PCOS were older and more likely to use metformin prior to pregnancy. Aspirin use during pregnancy was more common among those with PCOS. Race, ethnicity, and insurance status did not significantly differ across exposure groups (Table 1). Parity differed across groups (p = 0.012); nulliparity was more common among PCOS patients than non-PCOS controls (54% versus 36%), particularly in the PCOS-without-dysglycemia subgroup (61%).
Baseline Characteristics by Exposure Group
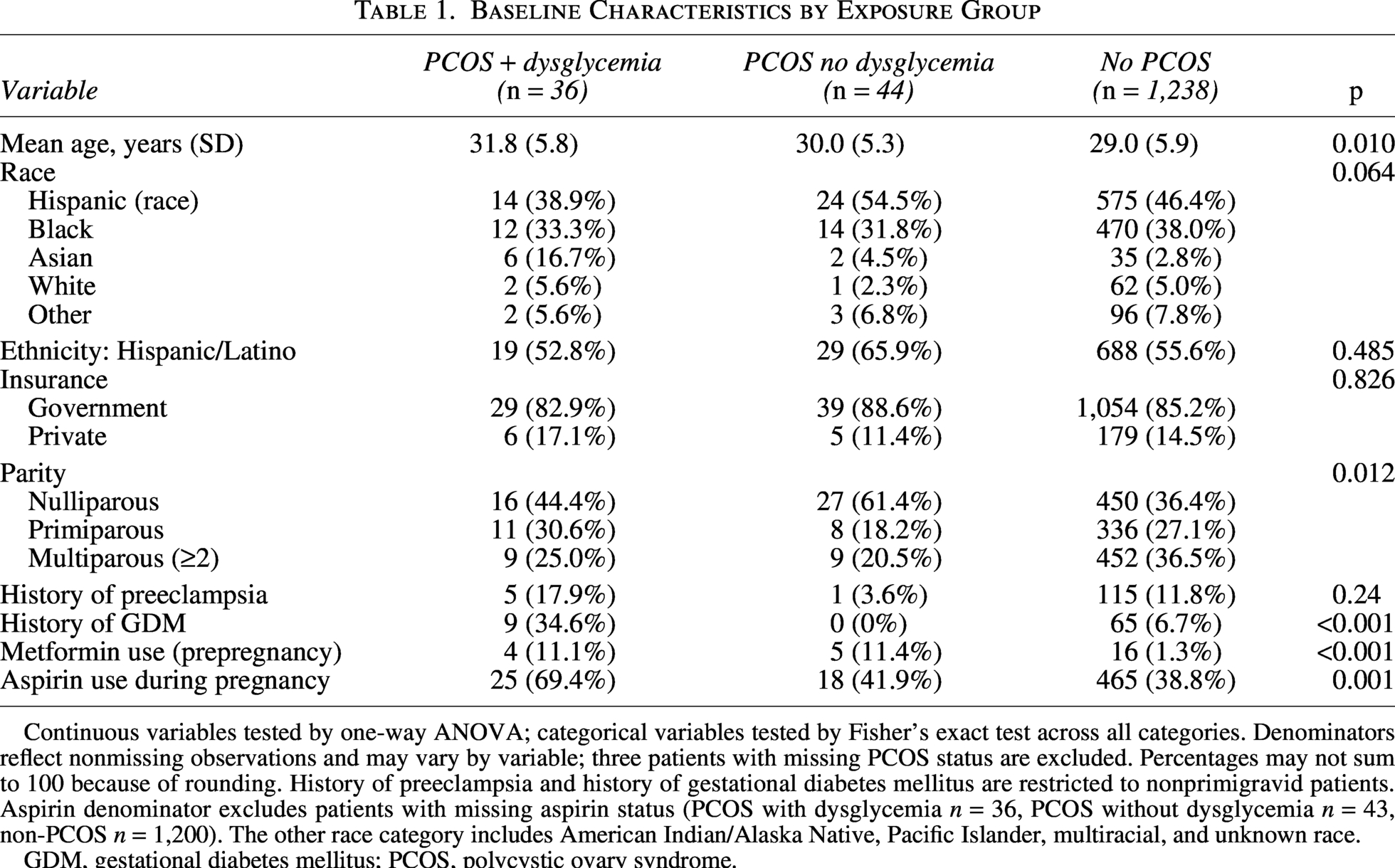
Continuous variables tested by one-way ANOVA; categorical variables tested by Fisher’s exact test across all categories. Denominators reflect nonmissing observations and may vary by variable; three patients with missing PCOS status are excluded. Percentages may not sum to 100 because of rounding. History of preeclampsia and history of gestational diabetes mellitus are restricted to nonprimigravid patients. Aspirin denominator excludes patients with missing aspirin status (PCOS with dysglycemia n = 36, PCOS without dysglycemia n = 43, non-PCOS n = 1,200). The other race category includes American Indian/Alaska Native, Pacific Islander, multiracial, and unknown race.
GDM, gestational diabetes mellitus; PCOS, polycystic ovary syndrome.
Among the 36 patients in the PCOS with dysglycemia group, the dysglycemia composite was driven by current gestational diabetes (n = 13, 36%), positive 1-hour glucose challenge test (n = 21, 58%), HbA1c ≥ 5.7% during pregnancy (n = 13, 36%), historical gestational diabetes (n = 9, 25%), pregestational diabetes (n = 7, 19%), and positive 3-hour glucose tolerance test (n = 7, 19%), with patients potentially meeting more than one criterion. Prepregnancy metformin use was documented in 4 of 36 (11%) patients in the PCOS with dysglycemia group.
Preeclampsia
Preeclampsia occurred in 12 of 36 individuals (33%) with PCOS and dysglycemia, 3 of 44 (7%) with PCOS without dysglycemia, and 144 of 1,173 (12%) controls (p = 0.005 for PCOS with dysglycemia versus controls). In adjusted analyses, PCOS with dysglycemia was associated with increased odds of preeclampsia (OR: 2.9; 95% CI: 1.4–6.1). PCOS without dysglycemia was not significantly associated with preeclampsia (aOR: 0.53; 95% CI: 0.16–1.73; p = 0.29; Table 2). A significant PCOS and dysglycemia interaction on preeclampsia risk was observed (p = 0.027).
Adjusted Odds Ratios for Adverse Pregnancy Outcomes
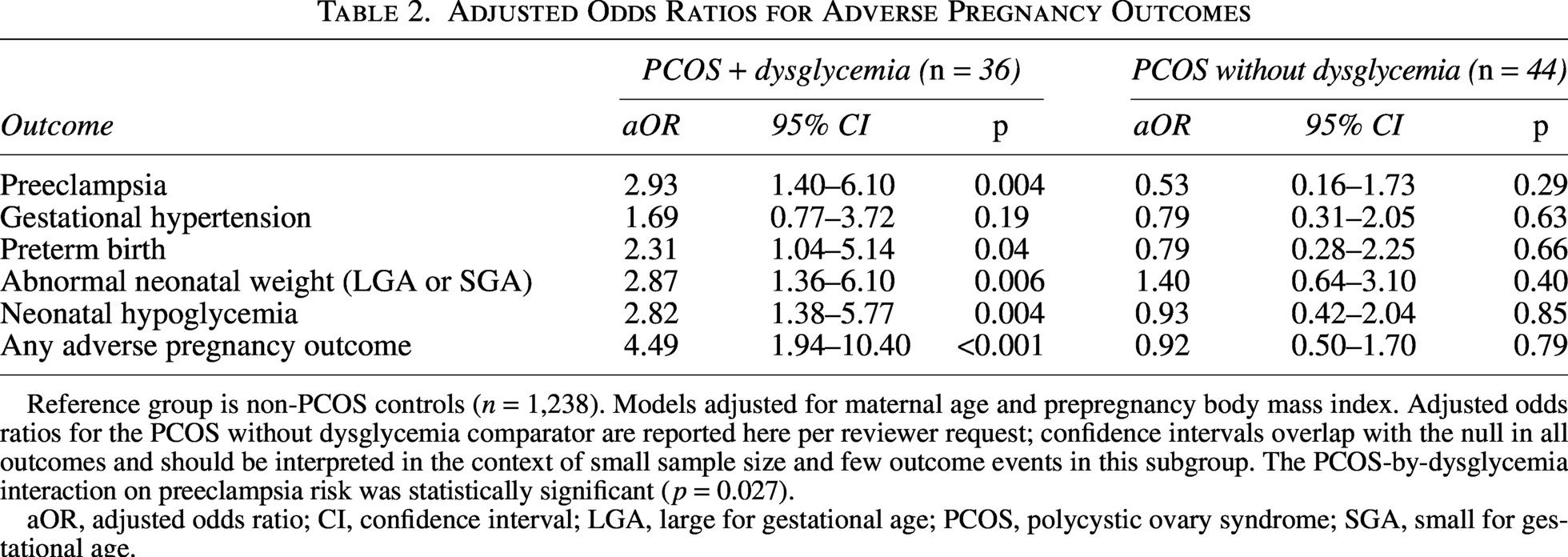
Reference group is non-PCOS controls (n = 1,238). Models adjusted for maternal age and prepregnancy body mass index. Adjusted odds ratios for the PCOS without dysglycemia comparator are reported here per reviewer request; confidence intervals overlap with the null in all outcomes and should be interpreted in the context of small sample size and few outcome events in this subgroup. The PCOS-by-dysglycemia interaction on preeclampsia risk was statistically significant (p = 0.027).
aOR, adjusted odds ratio; CI, confidence interval; LGA, large for gestational age; PCOS, polycystic ovary syndrome; SGA, small for gestational age.
Other adverse pregnancy outcomes
PCOS with dysglycemia was associated with increased odds of preterm birth (OR: 2.3; 95% CI: 1.04–5.14), abnormal neonatal weight (OR: 2.87; 95% CI: 1.36–6.10), neonatal hypoglycemia (OR: 2.8; 95% CI: 1.38–5.77), and any adverse pregnancy outcome (aOR: 4.49; 95% CI: 1.94–10.40). PCOS without dysglycemia was not consistently associated with these outcomes (preterm aOR: 0.79, 95% CI: 0.28–2.25; abnormal neonatal weight aOR: 1.40, 95% CI: 0.64–3.10; neonatal hypoglycemia aOR: 0.93, 95% CI: 0.42–2.04; any adverse pregnancy outcome aOR: 0.92, 95% CI: 0.50–1.70; Table 2).
Sensitivity analyses
Effect estimates were robust across specifications. After additional adjustment for aspirin use during pregnancy, the association between PCOS with dysglycemia and preeclampsia remained significant (aOR: 2.67, 95% CI: 1.27–5.61, p = 0.009). After additional adjustment for nulliparity, the association also remained significant (aOR: 2.53, 95% CI: 1.19–5.36); associations with preterm birth (aOR: 2.39), abnormal neonatal weight (aOR: 2.97), neonatal hypoglycemia (aOR: 2.87), and any adverse pregnancy outcome (aOR: 4.23) were essentially unchanged, and the PCOS-by-dysglycemia interaction remained significant (p = 0.030). Within the PCOS subgroup, the presence of dysglycemia was strongly associated with preeclampsia (aOR: 5.78, 95% CI: 1.40–23.9, p = 0.015), supporting the interpretation that metabolic dysfunction, rather than PCOS itself, drives obstetric risk in this population.
Discussion
In this prospective cohort, dysglycemia was associated with increased odds of preeclampsia and other adverse pregnancy outcomes among individuals with PCOS. In contrast, PCOS without dysglycemia was not independently associated with preeclampsia after adjustment for maternal age and BMI. These findings suggest that metabolic abnormalities may contribute to heterogeneity in obstetric risk among individuals with PCOS and may partially explain the variability observed across prior studies.
Meta-analyses have consistently reported elevated risks of gestational diabetes and hypertensive disorders among individuals with PCOS, with pooled ORs for preeclampsia generally ranging from approximately 1.5 to 3.01,3–6 However, substantial heterogeneity has been noted, including variation in diagnostic criteria for PCOS and inconsistent adjustment for metabolic confounders. Large population-based studies have demonstrated modest increases in hypertensive morbidity after controlling for BMI,2,4 whereas other analyses have found attenuation of risk after accounting for metabolic factors. 7 Our findings align with the hypothesis that metabolic dysfunction may be a key modifier of pregnancy risk within PCOS rather than PCOS itself uniformly conferring elevated risk.
Dysglycemia may reflect underlying insulin resistance, endothelial dysfunction, and chronic low-grade inflammation: pathophysiologic processes implicated in both PCOS and hypertensive disorders of pregnancy.8–10,12,20 Pregnancy is characterized by progressive insulin resistance, which may unmask preexisting metabolic vulnerability. 16 Individuals with PCOS who develop dysglycemia during pregnancy may represent a subgroup with greater underlying cardiometabolic burden, potentially predisposing them to placental dysfunction and hypertensive complications. While our study was not designed to evaluate mechanistic pathways, the observed clustering of hypertensive and metabolic neonatal outcomes among those with both PCOS and dysglycemia is biologically plausible.
Our findings also contribute to the growing literature emphasizing metabolic heterogeneity within PCOS. Clinical phenotypes of PCOS vary widely with respect to obesity, hyperandrogenism, and glucose metabolism.8–10,13 Prior work has suggested that hyperandrogenic or metabolically abnormal phenotypes may be associated with greater obstetric morbidity.6,11,12,21 By focusing on dysglycemia, a clinically measurable marker routinely assessed in pregnancy, we examined one dimension of metabolic variation within PCOS that is readily captured in obstetric care. Importantly, we do not suggest that dysglycemia fully explains obstetric risk in PCOS, but rather that it may identify a subgroup with heightened vulnerability.
These findings should be interpreted cautiously. The dysglycemia composite spans a clinical spectrum from positive antenatal screening tests to overt pregestational diabetes, with corresponding heterogeneity in pharmacologic treatment. Glycemic derangement in pregnancy exists on a metabolic continuum, and our composite reflects this. Although we adjusted for key confounders including BMI, residual confounding is possible. Dysglycemia and preeclampsia share overlapping risk factors, and the observational design precludes causal inference. The PCOS-without-dysglycemia group was modest in size, with few preeclampsia events; null findings in this subgroup should be interpreted with caution, as the small sample size precludes definitive conclusions regarding obstetric risk in this group. Additionally, PCOS was defined by chart documentation rather than systematic application of standardized diagnostic criteria; we could not verify which framework (e.g., Rotterdam, NIH, or AE-PCOS Society) the documenting clinician applied at the patient level, and some misclassification is possible.22,23 However, this approach reflects real-world clinical practice and enhances pragmatic relevance.
The cohort was drawn from a single urban academic center with a predominantly Hispanic and government-insured population. While this enhances representation of populations often underrepresented in clinical research, findings may not be generalizable to all settings. Future studies in larger, multi-center cohorts with standardized PCOS phenotyping are needed to validate these associations and to further disentangle the relative contributions of obesity, insulin resistance, and dysglycemia to hypertensive risk in pregnancy.
Despite these limitations, this study has several strengths. We leveraged prospectively collected data with standardized obstetric outcome definitions in a racially and ethnically diverse population. The analysis focused on clinically meaningful outcomes and adjusted for important confounders. By examining dysglycemia as it is encountered in routine prenatal care, the study provides clinically interpretable data regarding metabolic risk in PCOS pregnancies.
Taken together, our findings suggest that obstetric risk in PCOS may not be uniform and may be influenced by coexisting metabolic abnormalities. Larger studies with detailed metabolic phenotyping are needed to confirm these observations and to clarify whether metabolic optimization before or during pregnancy modifies hypertensive risk in this population.
Conclusions
In this prospective cohort, dysglycemia was associated with increased odds of hypertensive and metabolic pregnancy complications among individuals with PCOS. These findings support the concept that obstetric risk in PCOS may be influenced by coexisting metabolic abnormalities. Larger studies are needed to confirm these associations and clarify mechanisms underlying metabolic heterogeneity in PCOS pregnancies.
Authors’ Contributions
Conception and design of the study were initiated by C.K. Acquisition of data was completed by C.K., N.R., J.R., and M.L. Analysis of data was completed by C.K. Interpretation of data was completed by C.K., R.S., K.S., N.T., and T.K. C.K. drafted the article, and revisions and edits were provided by all. All authors provided final approval of the article and agree to be accountable for all aspects of the work.
Consent to Participate
Written informed consent was obtained from all participants at the time of enrollment in the FLIP cohort.
Consent for Publication
This article does not contain data from any individual person in a form that permits identification.
Data Availability
Study data were collected and managed using REDCap electronic data capture tools hosted at the Icahn School of Medicine at Mount Sinai. Deidentified data may be made available upon reasonable request to the corresponding author, subject to institutional and ethical approval.
Footnotes
Acknowledgments
The authors used a large language model to assist with article organization, statistical code debugging, and editing. The authors reviewed and verified all analyses and content and take full responsibility for the integrity and accuracy of the work.
Author Disclosure Statement
T.K. has research support from Gilead and Mirum and has served on advisory boards for Gilead, AbbVie, Mirum, GSK, Madrigal, and Ipsen. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
T.K. is supported by the National Institutes of Health (NIH) K23 award (1K23 HL163486-01A1), the Irma T. Hirschl/Monique Weill-Caulier Trust Research Award, and an NIH R01 grant (1R01 DK139189). The funding sources had no role in study design, data analysis, article preparation, or the decision to submit for publication.