
Abstract
Objective:
The postpartum period represents an opportunity to increase human papillomavirus (HPV) vaccination rates for those not vaccinated previously. This study aimed to evaluate the health outcomes and cost-effectiveness of a postpartum HPV vaccination program.
Methods:
A Markov model was constructed to estimate the cost-effectiveness of a postpartum HPV vaccination program. A theoretical cohort of 400,000 vaccine-eligible postpartum individuals was simulated based on the U.S. birth rates and HPV vaccination data for those aged 18–26. Simulated health outcomes included diagnoses of cervical intraepithelial neoplasia grade 1 (CIN1), CIN2+ (CIN grade 2 or 3), and early-stage cervical cancer. Inputs were derived from the literature. Cost-effectiveness was assessed in terms of healthcare costs and patient time/quality of life. The cost of the program is represented as the cost of vaccination with staff support per person in 2024 U.S. dollars. We used an incremental cost-effectiveness ratio (ICER) threshold of $100,000 per quality-adjusted life year (QALY). Sensitivity analyses were conducted to assess the impact of varying model parameters.
Results:
Compared to no vaccination program, the postpartum HPV vaccination strategy resulted in 2,575 fewer CIN1 cases, 2,809 fewer CIN2+ cases, and 27 fewer cases of early-stage cervical cancer in our simulated population. The program yielded 3,476 additional QALYs at an incremental cost of $79.7 million. The ICER was $22,922/QALY and thus was cost-effective. The program remained cost-effective across 99% of probabilistic simulations.
Conclusions:
A postpartum HPV vaccination program is a cost-effective strategy to reduce cervical dysplasia and cancer, meeting standards for preventative care and intervention. These results highlight the postpartum period as an opportunity to complete the HPV vaccine series.
Introduction
Human papillomavirus (HPV) is the most prevalent sexually transmitted infection in the United States and causes nearly all cases of cervical cancer. The introduction of HPV vaccines in 2006 has significantly reduced the incidence of cervical intraepithelial neoplasia (CIN) and HPV-associated malignancies in vaccinated populations.1–3 Vaccine uptake remains below the national goal of 80% HPV vaccine series completion.4,5 In 2022, 57.2% of females aged 18–26 years had received one or more doses of the HPV vaccine, despite recommendations from the Advisory Committee on Immunization Practices for catch-up vaccination through age 26.6,7 Barriers to vaccine completion in this age group include limited utilization of medical care and missed clinical opportunities.8–10 Furthermore, the HPV vaccination landscape continues to evolve. In early 2026, the Centers for Disease Control and Prevention (CDC) revised the childhood and adolescent immunization schedule to recommend a single dose of HPV vaccine for all children, based in recent trial data demonstrating noninferiority of one dose compared with two. 11 However, this change does not address unvaccinated adults aged 19–26 for whom catch-up vaccination remains recommended, reflecting a continued need for targeted strategies to reach underimmunized populations.
Many individuals aged 18–26 interact with the health care system more frequently during and after pregnancy. 12 Low-income individuals qualify for Medicaid coverage during and after pregnancy, providing them access to health care services that may otherwise be unaffordable. As a result, the postpartum period is a window of opportunity to deliver preventive care services such as the HPV vaccine.12,13 Pilot studies have shown the acceptability and feasibility of postpartum HPV vaccine programs, particularly in safety-net hospital settings.14–18 Previously, we reported on the feasibility of our institution’s postpartum HPV vaccination program. 18 The long-term health outcomes and economic value of these programs have not been evaluated. Our goal with this study was to determine the cost-effectiveness of a postpartum HPV vaccination program.
Methods
Using TreeAge Pro 2024, a Markov model was built to evaluate the cost-effectiveness of a postpartum HPV vaccination program. Our model evaluates health outcomes in a cohort of 400,000 unvaccinated individuals who were offered the 9-valent HPV vaccine series in the postpartum period. This cohort was compared with an otherwise identical simulated cohort who were not offered HPV vaccination. Our cohort size was based on estimates of U.S. annual births and vaccination eligibility among those aged 18–26 (approximately 700,000 births in this age range with 52.6% being unvaccinated at the time of delivery).6,19 All model inputs were derived from the literature (see Table 1). This study was deemed exempt from institutional review board approval as there is no involvement of human subjects.
Model Inputs
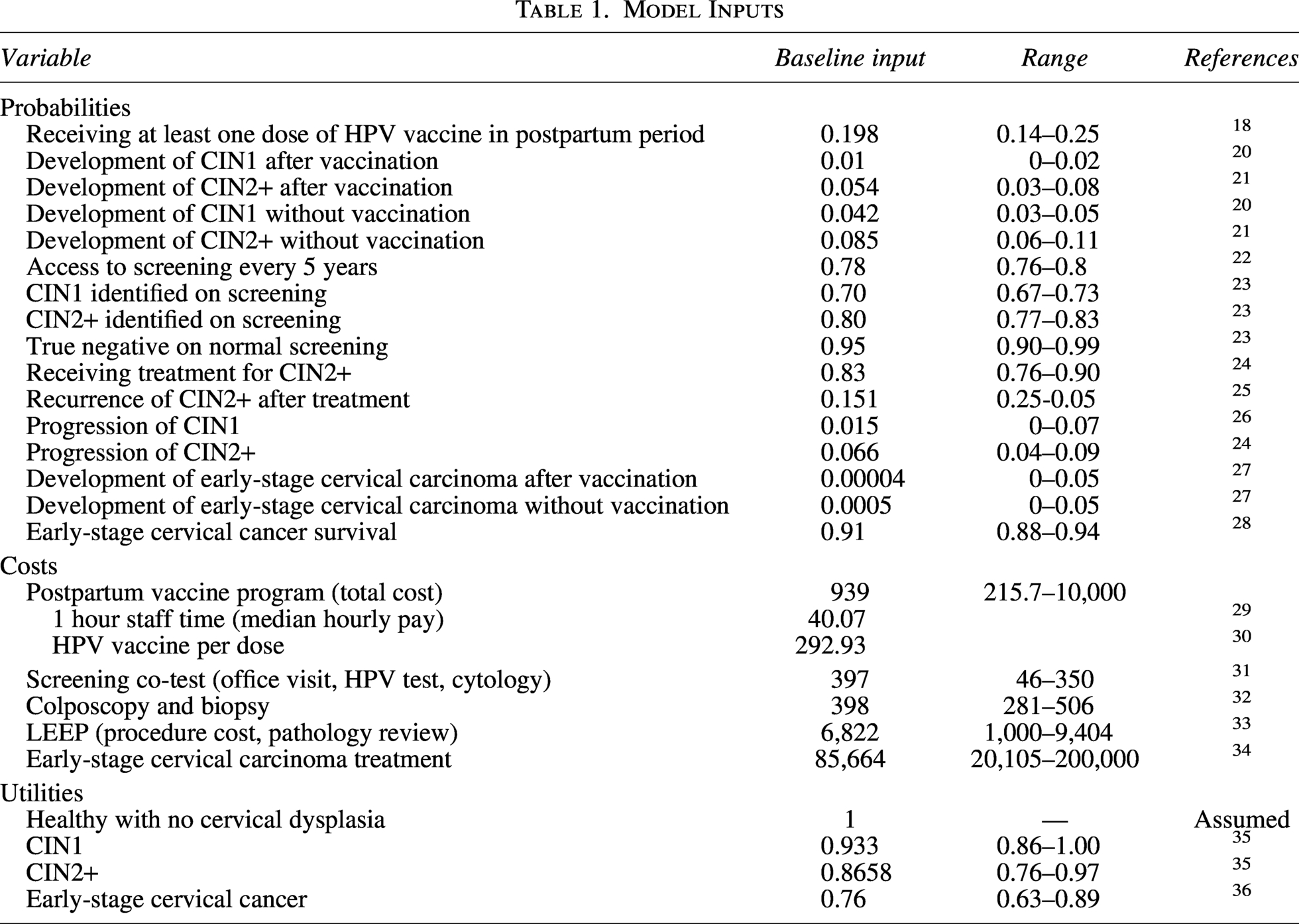
Our model structure is demonstrated in Figure 1. For the cohort that was offered HPV vaccination, we simulated the probability of an individual accepting HPV vaccination. If individuals accepted HPV vaccination, the model assumed they received at least one dose of the vaccine series. The rate of acceptance was based on our observational data from our institution’s low-resource postpartum program. 18 Next, we simulated the cohorts transitioning among three health states based on the natural history of developing cervical dysplasia. Our model’s health states included no dysplasia, CIN grade 1 (CIN1), and CIN2+, a health state representing high-grade cervical dysplasia (CIN2 and 3). The model then simulated successive rounds of screening, incorporating a probability of screening access at each interval so that not all individuals were assumed to undergo screening, and state transition probabilities were modified by vaccination status.20,21 Those individuals who were diagnosed with CIN2+ in the course of screening underwent loop electrosurgical excision procedure (LEEP) and entered a post-treatment surveillance arm, which incorporated recurrence probabilities and follow-up schedules recommended by the American Society for Colposcopy and Cervical Pathology (ASCCP). 37 Invasive cervical cancer was modeled as a separate downstream health state, with individuals in the CIN2+ state either undergoing treatment or progressing to early-stage invasive cancer based on the likelihood that treatment was successful. The model used 5-year cycles over a 20-year time horizon based on cervical cancer screening intervals recommended by the ASCCP.
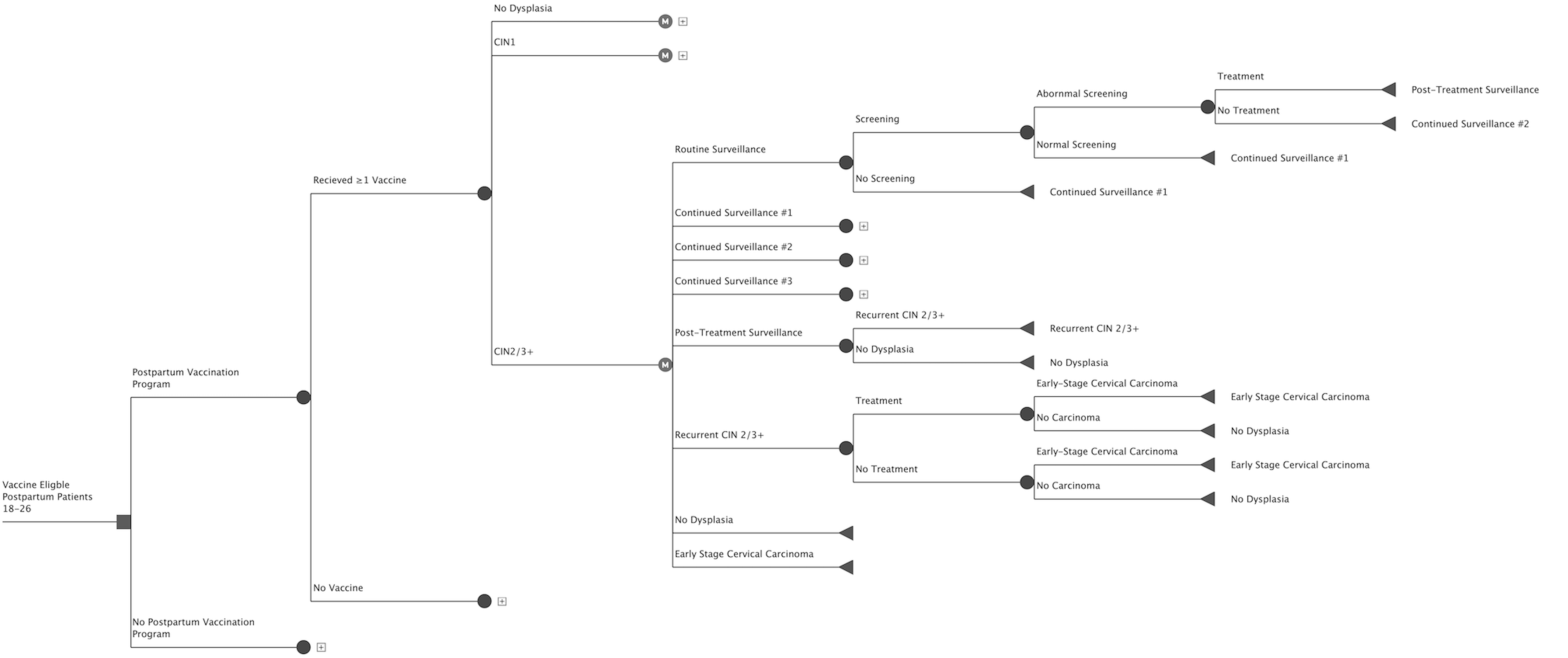
Markov model structure comparing the presence of postpartum vaccination program versus no available program. This figure only demonstrates the branching for those who developed CIN2+ following vaccination through the program for conciseness. The model is replicated for other cases where a plus sign is shown. Each green circle represents a branching node, the purple “M” represents a Markov node, and the red triangle represents a terminal node.
We made several assumptions to simplify model complexity. For individuals in the cohort who were not offered postpartum HPV vaccination, the model did not simulate HPV vaccination that might subsequently occur outside of the postpartum setting. We assumed that the HPV vaccine would be equally efficacious for all individuals offered the vaccine. Instead, vaccine effectiveness was modeled using lower probabilities of CIN1 and CIN2+ among vaccinated individuals based on published data, reflecting population-level outcomes without explicit stratification by prior HPV exposure. We simulated the possibility that individuals would start the vaccine series but receive fewer than three doses of the vaccine. The model accounted for how this would affect costs, but we did not simulate a difference in vaccine efficacy.
Costs were derived from the literature and adjusted to 2024 U.S. dollars using the medical care component of the Consumer Price Index. Costs were considered from a societal perspective. The baseline cost of a vaccination program was estimated based on a low-resource program design. The cost of the program was the cost of three doses of the HPV vaccine ($292.93 per dose) and the 1.5 hours of staff time to administer the vaccine ($40.07 per hour for three 30-minutes appointments). This low-resource model was based on existing postpartum HPV vaccination programs that were driven by the electronic medical record and did not require additional staffing or training to implement.17,18 These cost values were determined from the US Bureau of Labor Statistics Occupational Outlook Handbook. Costs for screening including the professional fee for the ambulatory visit and assumed that cotesting (cervical cytology and concurrent high risk HPV testing) was the screening method performed. 31 For individuals who had abnormal screening results, the model simulated the costs for colposcopy and colposcopic biopsies. For individuals diagnosed with cervical dysplasia that warranted treatment, the model simulated the costs to have a LEEP performed including the procedural cost and costs related to pathologic review.32,33 For those diagnosed with early-stage cervical cancer, we used the summation of per-person costs based on Medicare reimbursement claims. 34
Effectiveness was evaluated by using quality-adjusted life-years (QALY), a commonly used measure in economic analyses that reflects both quantity and quality of life. These were calculated by applying utilities to the length of time associated with a particular health state or scenario. Utilities range from 0 to 1, with 0 representing death, and 1 a state of ideal health. If individuals were diagnosed with CIN1 or CIN2+, utilities for these health states were applied for the subsequent 4 years based on prior literature, based on average time intervals for appropriate follow-up. 35 Baseline life expectancies were obtained from CDC data, while life expectancy for early-stage cervical carcinoma was based on SEER data. Cost effectiveness was then assessed using the incremental cost-effectiveness ratio (ICER), which is calculated by dividing the difference in cost by the difference in effectiveness between the two strategies. The willingness to pay threshold was set at a standard $100,000 per QALY. Future benefits and costs were discounted at 3% per year, a standard practice in cost-effectiveness analysis. 38
We performed multiple one-way sensitivity analyses that included all probabilities, costs, and utilities to determine which variables most affected the strength of our model. The range of values for each variable included three standard deviations above and below the baseline input. Inputs found to be the most influential were further investigated with additional one-way and two-way sensitivity analyses. Key sensitivity analyses examined the cost of the program and the probability that an individual would accept the vaccine series (e.g., vaccine uptake). To examine the robustness of the model, a Monte Carlo multivariable simulation, which varied inputs simultaneously over 10,000 simulations. Probabilities and utilities were sampled from beta distributions to approximate a normal distribution with a range of 0–1. Costs were sampled from gamma distributions to account for a lower limit of $0 and a right skew in the distribution. Life expectancies were varied according to triangular distributions to establish upper limits.
Results
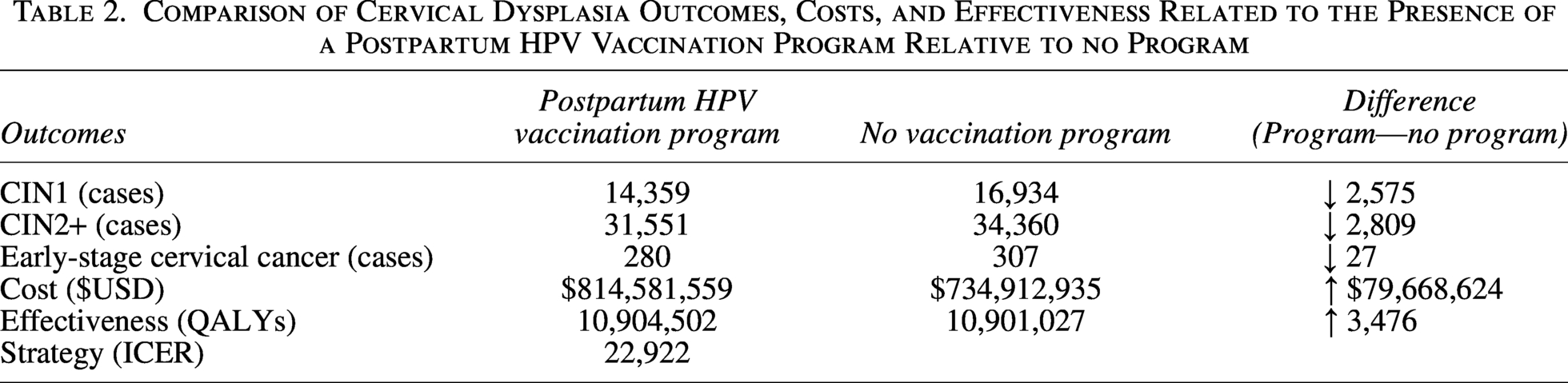
For individuals in the cohort where a postpartum HPV vaccination program was available, the model simulated that 19.8% (79,200/400,000) would accept the vaccine. In this cohort, there were 2,575 fewer cases of CIN1, 2,809 fewer cases of CIN2+, and 27 fewer cases of early-stage cervix cancer when compared with the cohort without a postpartum HPV vaccination program (Table 2). Health care costs were $79 million higher for the postpartum HPV vaccination program cohort. This cohort also gained 3,474 additional QALYs relative to the control arm. The ICER was $22,922 per QALY.
Comparison of Cervical Dysplasia Outcomes, Costs, and Effectiveness Related to the Presence of a Postpartum HPV Vaccination Program Relative to no Program
As shown in the tornado diagram, the cost of the program and the probability of developing CIN2+ following vaccination had the greatest impact on the ICER (Fig. 2). When varying the cost of the program in one-way sensitivity analysis, the HPV vaccination program was no longer cost-effective when the cost to vaccinate one individual exceeded $1,608 (Fig. 3). Similarly, two-way sensitivity analysis varying both program cost and vaccine uptake showed that ICER was maintained across nearly all uptake rates, but the ICER decreased with higher-cost programs (Fig. 4). Monte Carlo simulation demonstrated the program was cost-effective in 99% of simulations, confirming robustness despite parameter uncertainty (Fig. 5).
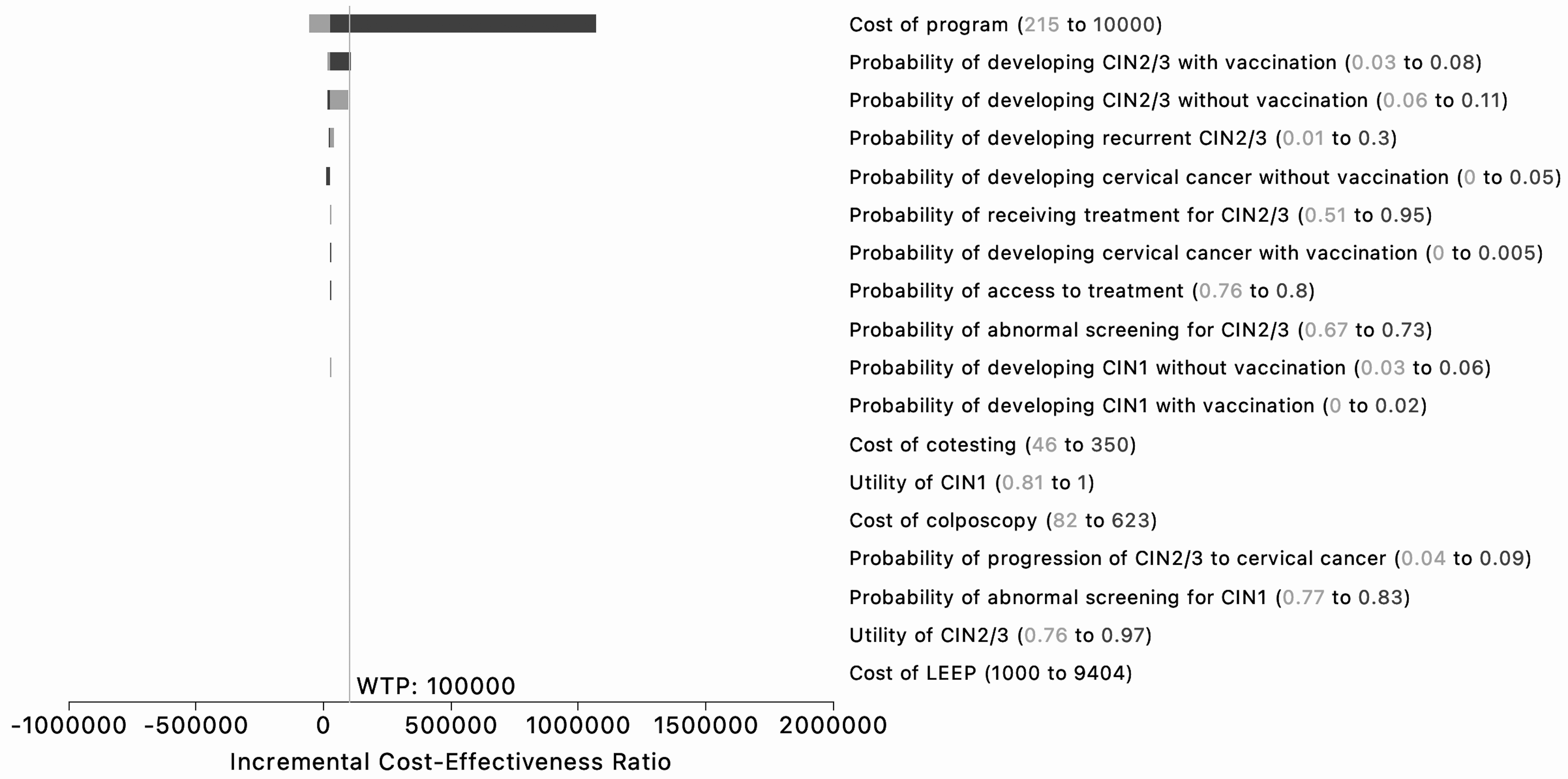
Tornado diagram representing the impact of inputs on the cost-effectiveness of the model. Each input ranged three standard deviations above and below the baseline input.
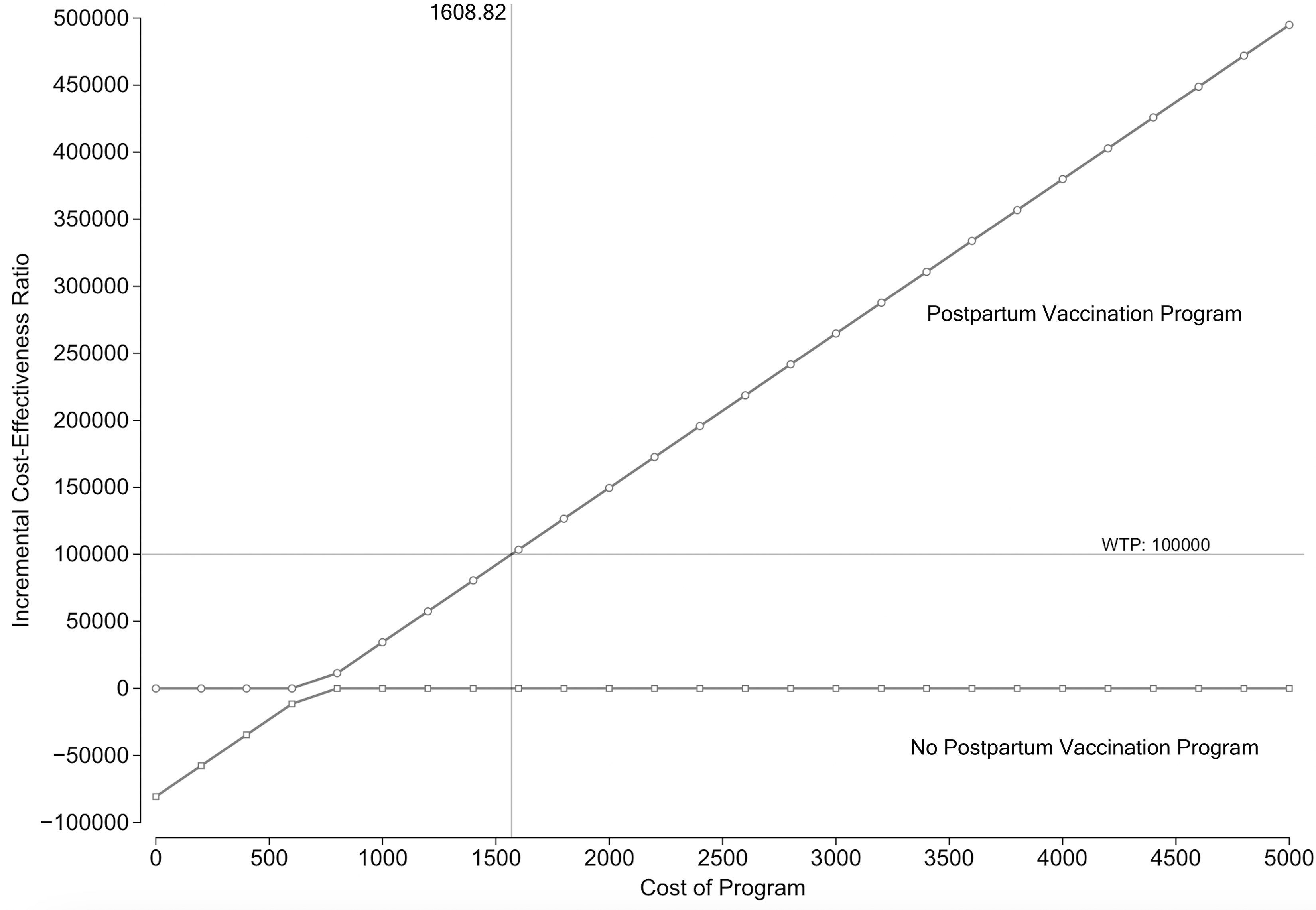
Univariate sensitivity analysis varying the cost of the program.
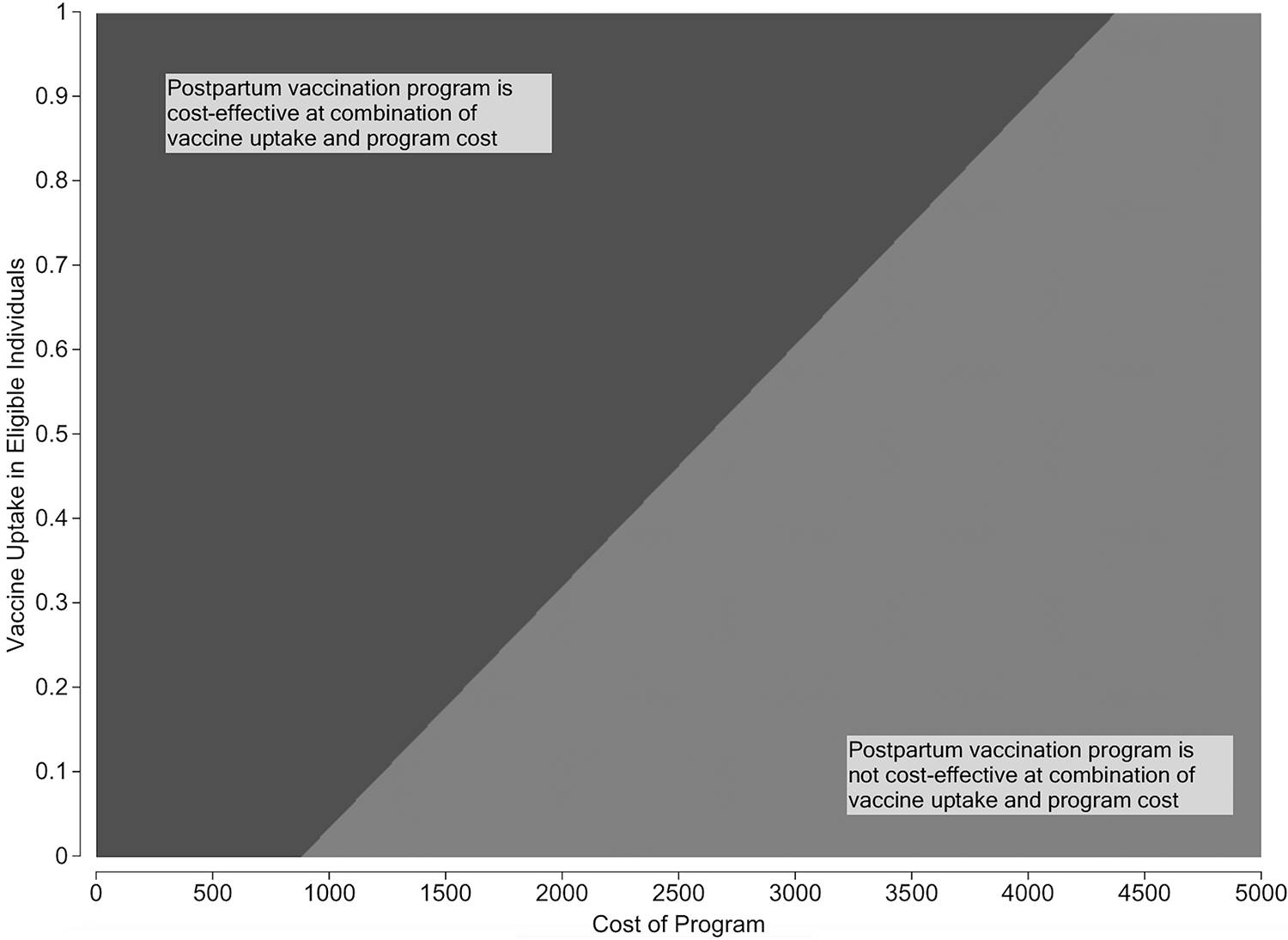
Two-way sensitivity analysis demonstrating the cost of the program by vaccine uptake.
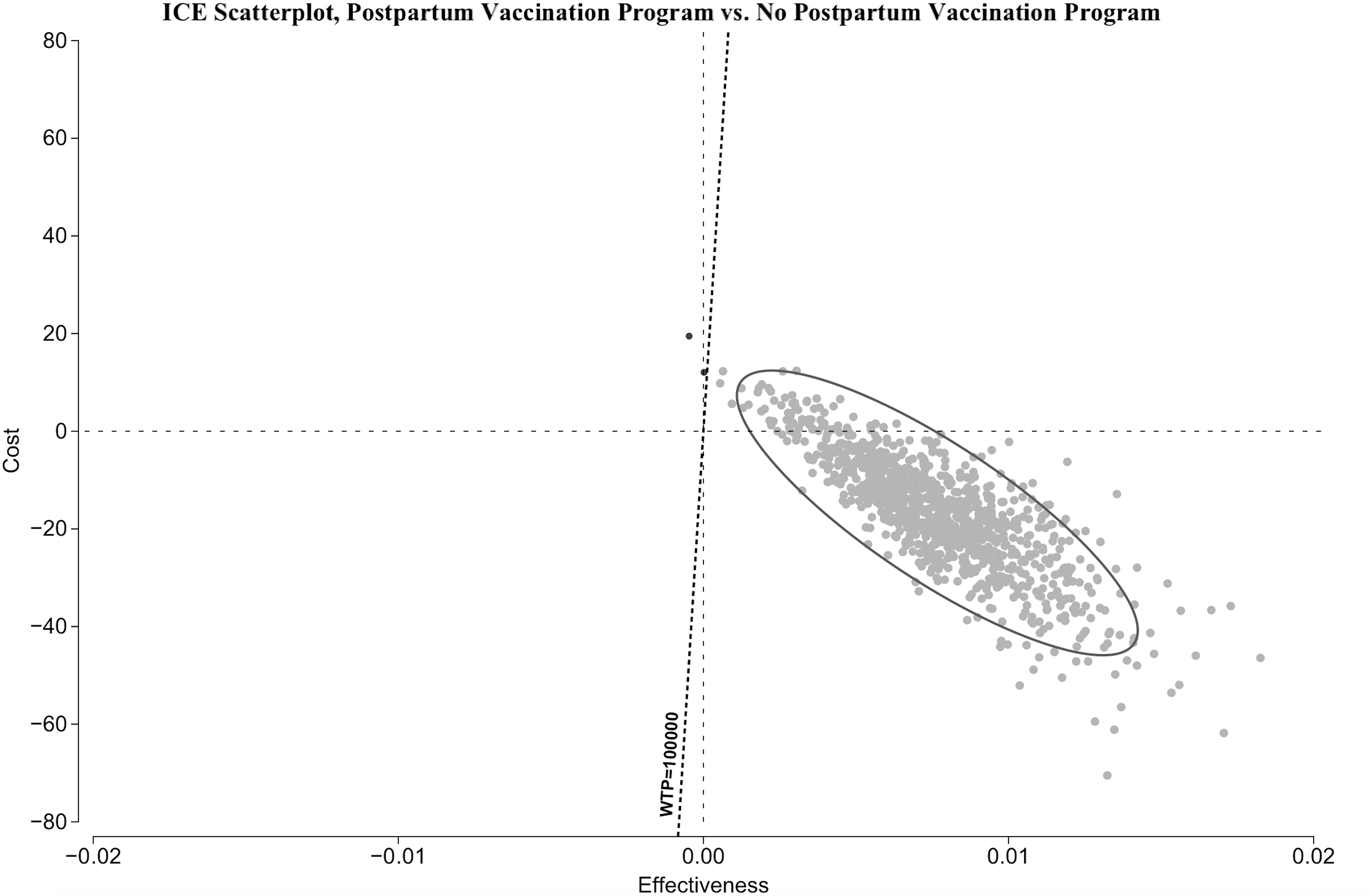
Monte Carlo sensitivity analysis of 10,000 trials, showing that when variation was incorporated into model inputs, the postpartum vaccination strategy was a cost-effective strategy 99% of the time.
Discussion
This study finds that a program offering the HPV vaccine during the postpartum period for individuals aged 18–26 is cost-effective. Using a Markov model, we found that integrating HPV vaccination into routine postpartum care can lead to substantial reductions in the need for invasive diagnostic and therapeutic procedures for HPV-related cervical disease. These results support offering HPV vaccination as standard postpartum care.
Our findings align with previous modeling studies showing that HPV vaccination in young adults can prevent substantial disease burden and remain cost-effective across a range of assumptions.39,40 Although HPV vaccination has been recommended through age 26 for over a decade, many individuals miss opportunities for vaccination during adolescence and young adulthood.4,5,7 The postpartum period presents a timely and actionable opportunity to reach individuals who may otherwise remain unvaccinated due to limited engagement with primary care. Implementation studies have shown that offering HPV vaccination during postpartum hospital stay is feasible and associated with uptake among eligible individuals.16,41,42 Our study adds to this literature by showing that such programs are also cost-effective.
A strength of our analysis is its focus on a low-resource implementation model. Our baseline cost estimates predicted an ICER substantially below the willingness-to-pay threshold of $100,000 per QALY, the standard benchmark for intervention in the United States. The model remained cost-effective and below the willingness-to-pay boundary even when we modeled costs 70% higher than our baseline estimates. This implies there is some flexibility in how a postpartum HPV vaccine program could be implemented, and health care organizations and policy makers would have the opportunity to consider modifications to the program to improve vaccine uptake and completion (eg, electronic reminders, patient education, or community health worker support) while maintaining cost-effectiveness. As demonstrated in Figure 4, lower resource programs remain cost-effective even if vaccine uptake is lower than what has been observed in the literature.14–16 These results align with earlier modeling work showing that catch-up vaccination among adults can be cost-effective when targeted to underimmunized populations, especially if programmatic costs are kept manageable.39,40
In addition to its clinical and economic advantages, postpartum HPV vaccination may be a strategy to mitigate health disparities in cervical cancer prevention. Individuals who qualify for health insurance through Medicaid often lose coverage after delivery, limiting access to ongoing preventive care. The same challenges in accessing preventative care also put these individuals at risk of delayed diagnosis and needing more invasive treatment. Vaccination does not require ongoing access to care to lower an individual’s risk for HPV-related disease. By incorporating vaccination into standard postpartum care, health care systems can promote the health of these individuals through primary prevention.
This study has several limitations. We made several simplifying assumptions that are described in the Methods. We believe these assumptions are reasonable and unlikely to substantially impact our finding that a postpartum HPV vaccine program is a cost-effective strategy. Importantly, several of these assumptions (e.g., not modeling vaccination outside the postpartum period, assuming uniform vaccine efficacy, and not differentiating by number of doses) would be expected to bias results toward underestimating the benefit of the intervention rather than overestimating it. Some modeling simplifications (e.g., assuming average probabilities across a heterogeneous population) prevent us from observing possible heterogeneity in the efficacy of the intervention. For example, demographic and socioeconomic characteristics influence both risk, the likelihood of vaccine acceptance, and access to secondary preventive care. Future work should incorporate more granular data to evaluate how postpartum vaccination programs can be tailored for specific populations or health care settings. Additionally, the focus of this model was on the benefit of HPV vaccine on a single disease process (i.e., cervical dysplasia and cancer). As the HPV vaccine prevents HPV-related disease beyond cervical dysplasia, including genital warts, HPV transmission to partners, and other HPV-associated malignancies such as anal and oropharyngeal cancers, we may underestimate of the cost-effectiveness of a postpartum HPV vaccination program by not including these health benefits in the model. Emerging evidence also suggests that fewer than three HPV vaccine doses may provide adequate protection, which would reduce program costs and make our estimates conservative. 11 Consistent with this, the model did not differentiate between one-, two-, and three-dose series in terms of efficacy, instead assuming that receipt of at least one dose conferred reduced risk of cervical dysplasia, as supported by the literature.43,44 Future models incorporating dose-specific uptake and real-world completion rates may provide a more nuanced estimate of cost-effectiveness.
In conclusion, postpartum HPV vaccination is a cost-effective intervention to reduce the burden of cervical dysplasia and cancer on individuals and the health care system. This strategy leverages a window of opportunity to reach unvaccinated individuals. Considering that the feasibility of postpartum HPV vaccination programs has been established and now with evidence of the cost-effectiveness of these programs, policymakers should advocate for HPV vaccination to become a standard part of postpartum care, particularly in health care settings that provide perinatal care to individuals who may not have health insurance coverage outside of pregnancy. Future studies should focus on implementation strategies to promote the uptake of this cost-effective strategy to prevent HPV-related disease.
Authors’ Contributions
A.M.: Conceptualization, methodology, model building, writing—original draft preparation, writing—review and editing; C.G.N.: Conceptualization, methodology, model building, writing—original draft preparation, writing—review and editing; R.F.H.: Conceptualization, methodology, model building, writing—original draft preparation, writing—review and editing; A.B.C.: Conceptualization, methodology, model building, writing—original draft preparation, writing—review and editing; A.S.B.: Conceptualization, methodology, writing—original draft preparation, writing—review and editing.
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal participants.
Data Availability
All data generated or analyzed during this study are included in this published article.
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.