
Abstract
Background:
Postoperative delirium is a common complication in older adults. Binary delirium outcomes may obscure clinically meaningful, sex-specific differences in delirium severity and burden. We sought to characterize these patterns in a surgical cohort.
Methods:
We prospectively studied older patients with repeated postoperative delirium assessments, obtaining daily Delirium Rating Scale (DRS) scores to measure severity, calculating area under the curve (AUC) across postoperative assessments as a measure of cumulative delirium burden (total symptom load over time). We used sex-stratified models and pooled models with sex interaction terms, adjusting for age, American Society of Anesthesiology (ASA) physical status, opioid exposure, and other physiologic covariates.
Results:
Risk factors for delirium severity and burden differed significantly by sex. Among women, higher ASA class was the primary predictor of increased delirium burden (AUC: β = 2.79 per class; peak DRS: β = 1.71). Among men, increasing age (AUC: β = 0.427 per year) and intraoperative opioid exposure were strongly associated with higher burden. The age-by-sex interaction was significant across all outcomes (p < 0.05), with age being a much stronger predictor of delirium severity in men than in women. At matched baseline risk, predicted delirium severity was consistently higher in men.
Conclusions:
Delirium risk factors are sex-differentiated. For men, age was the dominant predictor of delirium severity and burden, whereas for women, baseline physiologic status was more strongly associated with these outcomes. These findings highlight the importance of using severity-based outcomes to reveal sex-specific vulnerability patterns that are otherwise obscured by simple binary endpoints.
Keywords
Introduction
Delirium is a common and serious neuropsychiatric complication among older adults undergoing major surgery that is associated with longer hospital stays, functional decline, and mortality. While many studies focus on the presence or absence of delirium, emerging evidence supports a need to assess delirium’s severity and duration, constructs that may better capture patient-centered outcomes and long-term risk.1–3 Women, who make up a substantial proportion of the aging surgical population, appear disproportionately affected by delirium-related morbidity, although studies evaluating sex-specific vulnerability have yielded mixed findings.4,5
Biological and clinical sex differences may shape delirium risk through multiple mechanisms. Estrogen depletion has been linked to impaired cholinergic signaling and increased neuroinflammation, potentially lowering the threshold for postoperative neurocognitive disruption.6–8 Women are also more apt to show frailty and inflammatory vulnerability with age, both established risk factors for delirium.5,9 In addition, female patients often receive different perioperative care and exhibit distinct delirium phenotypes, and they are more likely to have hypoactive delirium than hyperactive delirium.6–8 Despite these differences, sex has rarely been examined as a modifier of delirium severity or burden across time.
Most studies of delirium define outcomes dichotomously, despite the existence of validated tools, for example, the Delirium Rating Scale-Revised-98 (DRS-R-98), which offers continuous assessment of symptoms. 10 Capturing delirium as a trajectory, rather than a binary event, can illuminate interindividual variation and enable modeling of cumulative burden, defined as the total symptom load experienced over time (e.g., area under the curve [AUC]).11,12 This is especially relevant for older women, in whom fluctuating symptoms and subtle presentations may be missed by binary case definitions.
Despite growing recognition of delirium as a dynamic and heterogeneous syndrome, sex has rarely been evaluated as a modifier of delirium severity trajectories or cumulative burden over time. Prior studies have largely relied on binary outcomes, which may obscure clinically meaningful differences in symptom expression and recovery patterns. Accordingly, the objective of the present study was to evaluate sex differences in postoperative delirium severity and cumulative burden using longitudinal DRS-R-98 assessments. We further sought to determine whether sex modifies the associations between key perioperative risk factors, including age, physiologic status, and opioid exposure, and delirium outcomes. We hypothesized that delirium burden would be differentially patterned by sex, reflecting distinct underlying vulnerability profiles.
Methods
Study design and participants
This study is a secondary analysis of a prospective, randomized controlled trial conducted at the
Study population
For this analysis, we examined sex differences in postoperative delirium severity and burden using data from trial participants who underwent surgery with at least 5 days of anticipated postoperative hospitalization (Supplemental Figure S1). We excluded individuals with severe baseline cognitive impairment, non-English speakers, or a history of a psychotic disorder. All participants or their proxies provided informed consent under IRB-approved protocols. Baseline demographic and clinical data were recorded, including age, sex, comorbidities, and preoperative American Society of Anesthesiologists (ASA) Physical Status classification. Surgical characteristics and anesthesia type were documented. Postoperative care followed standard protocols with no sex-specific interventions. Outcome assessors were blinded to the study hypotheses.
Delirium assessment
Delirium severity was assessed daily from postoperative day (POD) 0 through POD 4 using the DRS-R-98, a validated 16-item clinician-rated tool with scores ranging from 0 to 39.10,13 Higher scores indicate greater severity. Assessments were performed once daily by trained raters blinded to patient sex. Assessments occurred at a consistent time, typically in the morning. If the assessment was missed due to patient unavailability, a second attempt was made; otherwise, data were coded as missing.
We used the continuous DRS-R-98 severity score as the primary outcome, rather than a binary delirium diagnosis. Full-syndrome delirium is typically indicated by scores > 15; subsyndromal presentations range between 8 and 14. To quantify cumulative symptom burden, we calculated the AUC of DRS-R-98 scores over time (POD 0–4), using the trapezoidal rule. AUC scores represent cumulative delirium severity (“score-days”), with missing days scored as zero if it was due to early discharge.
Missing DRS-R-98 observations were infrequent and primarily attributable to early discharge or temporary patient unavailability. For AUC calculations, missing values due to early discharge were conservatively treated as zero, reflecting the absence of observed symptoms. In longitudinal models, missing observations were handled under a missing-at-random assumption using maximum likelihood estimation inherent to mixed-effects modeling. Sensitivity analyses restricting to complete cases yielded consistent results.
Covariates
The primary independent variable was patient sex (female vs. male). Additional covariates were selected a priori based on known delirium risk factors that included:
These covariates were included in all adjusted models to reduce confounding. No sex-specific treatment differences were introduced during the study.
Statistical analysis
Statistical analyses were conducted using R (Version 4.4.1; R Foundation for Statistical Computing; Vienna, Austria), using, dplyr, tidyr, sandwich, lmtest, clubSandwich, pracma, ggplot2, DiagrammeR, gtsummary, and broom packages. Descriptive statistics summarized cohort characteristics by sex. Continuous variables were compared using Student’s t-tests or Wilcoxon rank-sum tests, depending on distributional assumptions. Categorical variables were compared using chi-square tests. We also summarized postoperative delirium severity using the DRS-R-98, calculating the mean (±SD) daily scores by sex and the patient-level AUC as a measure of cumulative delirium burden.
For our primary analyses, we employed two complementary modeling approaches corresponding to the two primary outcomes: (1) delirium trajectory analysis and (2) cumulative delirium burden. The combined use of mixed-effects trajectory modeling and cumulative burden analysis was intended to capture both temporal dynamics and overall symptom load, providing complementary perspectives on delirium expression.
Delirium trajectory analysis
Linear mixed-effects models were used to assess sex differences in DRS-R-98 severity trajectories across postoperative days 0–4. Fixed effects included time (categorical POD 0–POD 4), sex, and their interaction (sex × time), along with covariates: age, ASA class, BMI, opioid exposure (MMEs), oxygen saturation, MAP, and other clinical factors. A random intercept was included for each subject to account for within-person correlation; a random slope for time was considered but did not improve model fit. DRS-R-98 scores were modeled on the original scale, with residual diagnostics evaluated to confirm model assumptions. From these models, we estimated adjusted daily delirium severity for each sex and tested for overall sex differences as well as differential rates of resolution. A sensitivity analysis stratified models by sex to evaluate whether specific covariates had sex-specific effects on delirium severity trajectories.
Cumulative delirium burden analysis
We used multivariable linear regression to examine differences in cumulative delirium burden (AUC of DRS-R-98 scores from POD 0–4) between sexes. Covariates were identical to those used in the mixed-effects models. Due to right-skewness of the AUC distribution, we assessed both log-transformed and untransformed models and verified robustness across specifications. Interaction terms (e.g., sex × age, sex × ASA, sex × opioid dose) were added individually to assess whether sex modified the association between clinical predictors and delirium burden. Exploratory interaction p-values were adjusted for multiple comparisons.
All statistical tests were two-tailed with α set at 0.05. We report β coefficients or adjusted mean differences with 95% confidence intervals. Model fit was assessed using R2 for linear models and marginal/conditional R2 for mixed models. Sensitivity analyses included sex-stratified models, restriction to patients with delirium (vs. full cohort), and comparison with alternative delirium indicators, such as Confusion Assessment Method (CAM)-based delirium day counts. Results were consistent across these approaches.
Results
Sample
The complete-case analytic sample for the sex-focused analyses included 206 participants (women, n = 106, men, n = 100) for burden models (AUC/peak) and 204 participants for longitudinal daily severity models (women, n = 105, men, n = 99).
Baseline differences by sex
Women and men were similar in age (median 72 years, in both sexes; p = 0.66) and BMI (median 28, in both sexes; p = 0.94). Men had higher intraoperative opioid exposure (median intraoperative MMEs, 45 vs. 35; p = 0.002) and higher postoperative nadir MAPs (median, 75.3 vs. 69.5; p < 0.001) (Table 1). DRS burden measures did not differ significantly by sex in unadjusted comparisons (AUC p = 0.32; peak p = 0.30) (Supplemental Figure S2). We therefore examined whether sex modified the relationships between clinical risk factors and delirium severity outcomes in adjusted models.
Baseline Characteristics of the Study Cohort by Sex
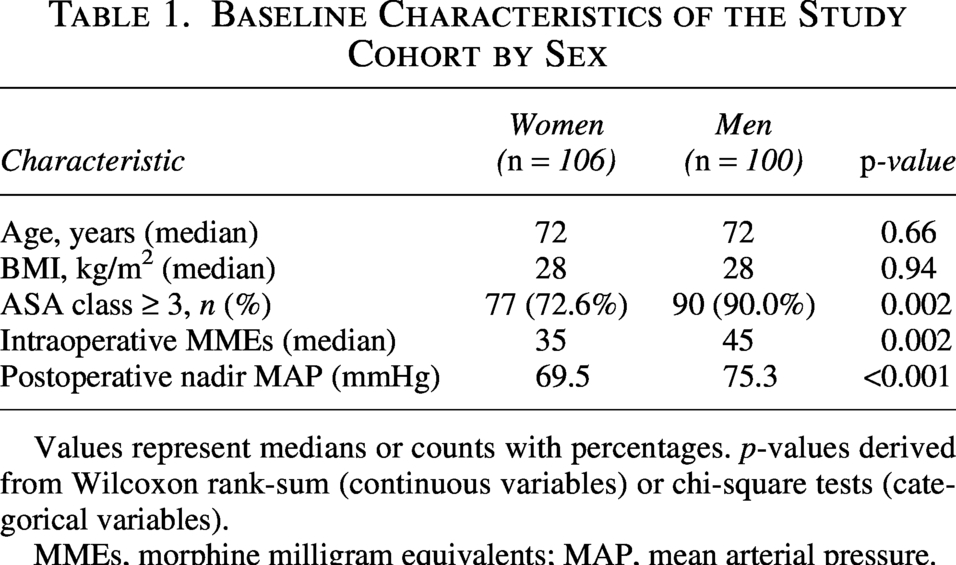
Values represent medians or counts with percentages. p-values derived from Wilcoxon rank-sum (continuous variables) or chi-square tests (categorical variables).
MMEs, morphine milligram equivalents; MAP, mean arterial pressure.
Sex-stratified longitudinal delirium severity
In women, age was not associated with daily DRS severity (β = 0.016 per year, 95% CI −0.062 to 0.094; p = 0.692). In men, age showed a strong positive association with daily severity (β = 0.164 per year, 95% CI 0.078 to 0.250; p = 0.00018). Associations with concurrent postoperative opioids (MMEs) and lagged opioids (MME_lag1) were not statistically significant in either sex (women: MMEs β = −0.004, p = 0.51; men: β = −0.014, p = 0.43). Oxygen saturation terms were directionally positive for lagged O2 (women β = 0.081, p = 0.13; men β = 0.098, p = 0.13) but were not statistically significant.
Sex-stratified delirium burden
For DRS AUC (0–4), ASA class was associated with higher burden in women (β = 2.79 per class, 95% CI 0.08 to 5.51; p = 0.044), while age was not (β = −0.010, p = 0.93). In men, age was strongly associated with a higher AUC (β = 0.427 per year, 95% CI 0.176 to 0.678; p = 0.00085), and intraoperative MMEs were also associated (β = 0.064 per mg, 95% CI 0.004 to 0.124; p = 0.0368). Postoperative opioid exposure (MMEs 0–3 days) was not associated with AUC in either sex (Table 2).
Sex-Stratified Associations with Delirium Burden (DRS AUC 0–4)

Multivariable linear regressions stratified by sex. Each model includes the listed predictor, adjusted for other covariates.
Β, change in AUC per unit increase in predictor; CI, confidence interval; MMEs, morphine milligram equivalents.
For peak DRS, women again showed an ASA association (β = 1.71, 95% CI 0.01 to 3.41; p = 0.049) without an age association (β = −0.013, p = 0.83). Men showed an age association (β = 0.219, 95% CI 0.065 to 0.373; p = 0.0054) and an intraoperative opioid association (β = 0.055, 95% CI 0.011 to 0.098; p = 0.013).
Effect modification by sex
In pooled interaction models, the age-by-sex interaction was significant for daily severity (β interaction = 0.146; p = 0.012), DRS AUC (β interaction = 0.420; p = 0.009), and peak DRS (β interaction = 0.216; p = 0.031), indicating a stronger association between age and delirium expression among men. Interactions between sex and ASA class or opioid exposure were not statistically significant (Table 3).
Sex Interaction Effects for Delirium Severity and Burden Outcomes
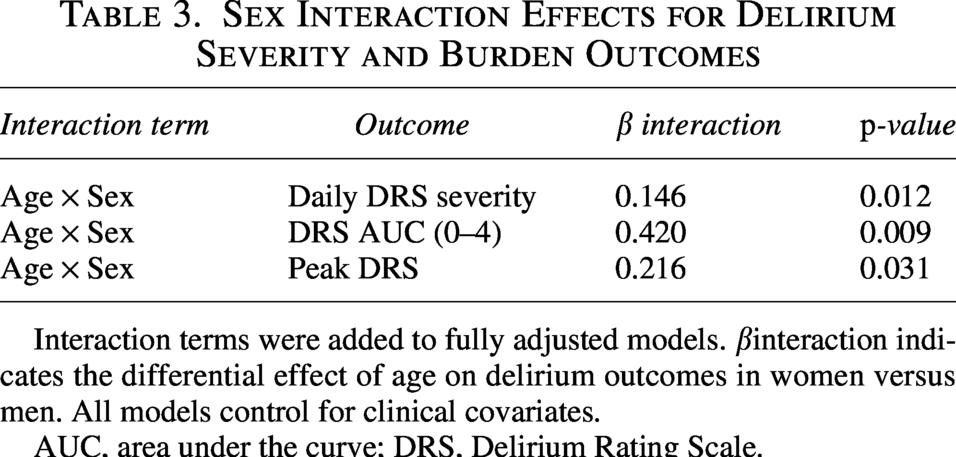
Interaction terms were added to fully adjusted models. βinteraction indicates the differential effect of age on delirium outcomes in women versus men. All models control for clinical covariates.
AUC, area under the curve; DRS, Delirium Rating Scale.
Predicted trajectories under matched baseline risk
At age 75 and ASA class 3 with covariates held at cohort medians, predicted delirium severity was higher for men across postoperative days 0–3 (Fig. 1; Supplemental Figure S3). Predicted mean DRS at day 0 was 3.01 (95% CI 2.15–3.86) for men versus 2.70 (1.88–3.51) for women; by day 3, predicted mean DRS was 1.97 (1.03–2.92) for men versus 1.66 (0.71–2.62) for women. These model-based findings are further illustrated in the sex-stratified forest plot of regression coefficients (Fig. 2).
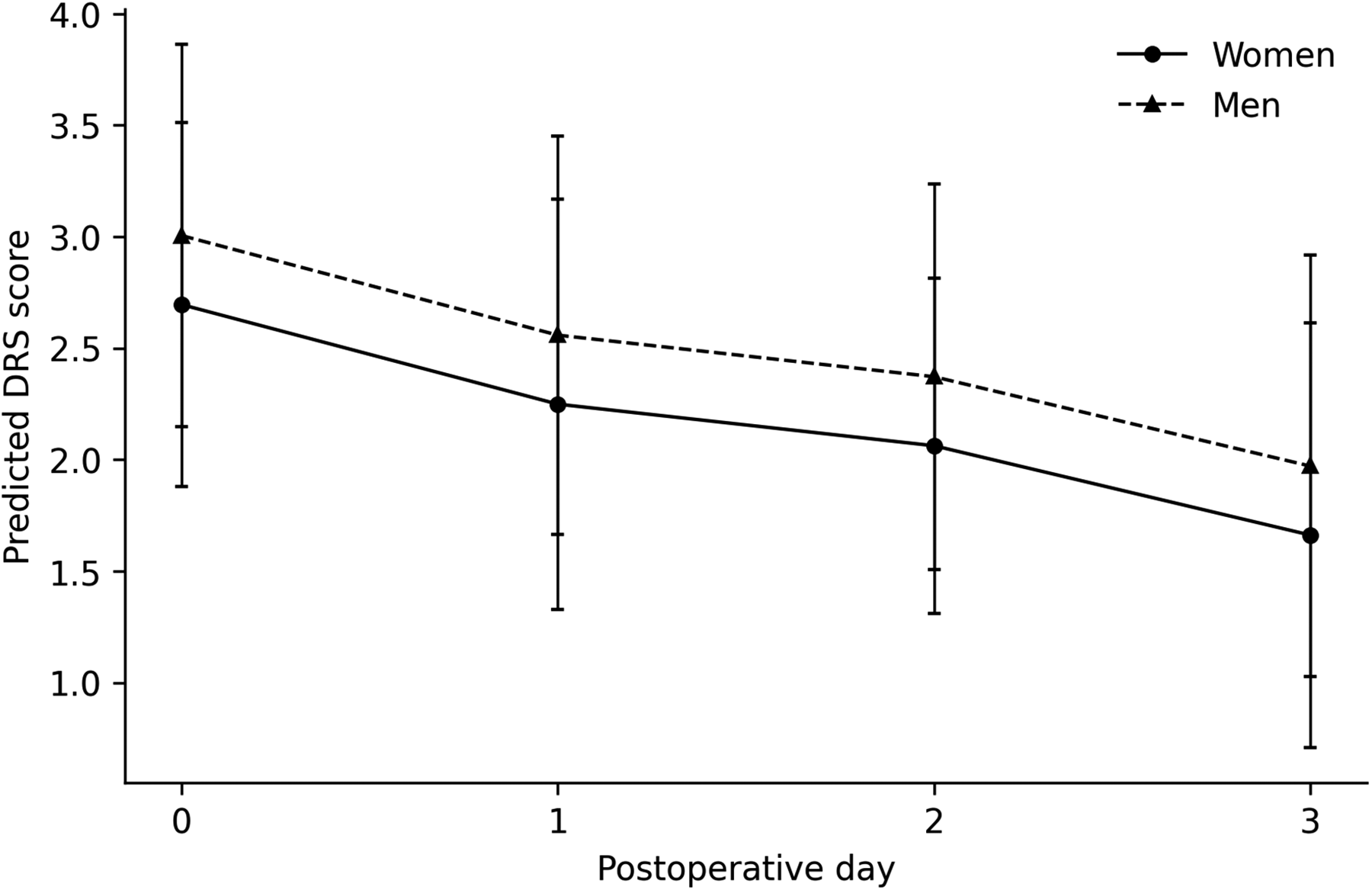
Predicted Postoperative Delirium Severity Trajectories by Sex at Matched Baseline Risk. Predicted Delirium Rating Scale (DRS) scores across postoperative days 0–3 are shown for women and men at age 75 and ASA class 3 using the adjusted longitudinal model. Other covariates were held at cohort medians. Error bars indicate 95% confidence intervals for the predicted mean.
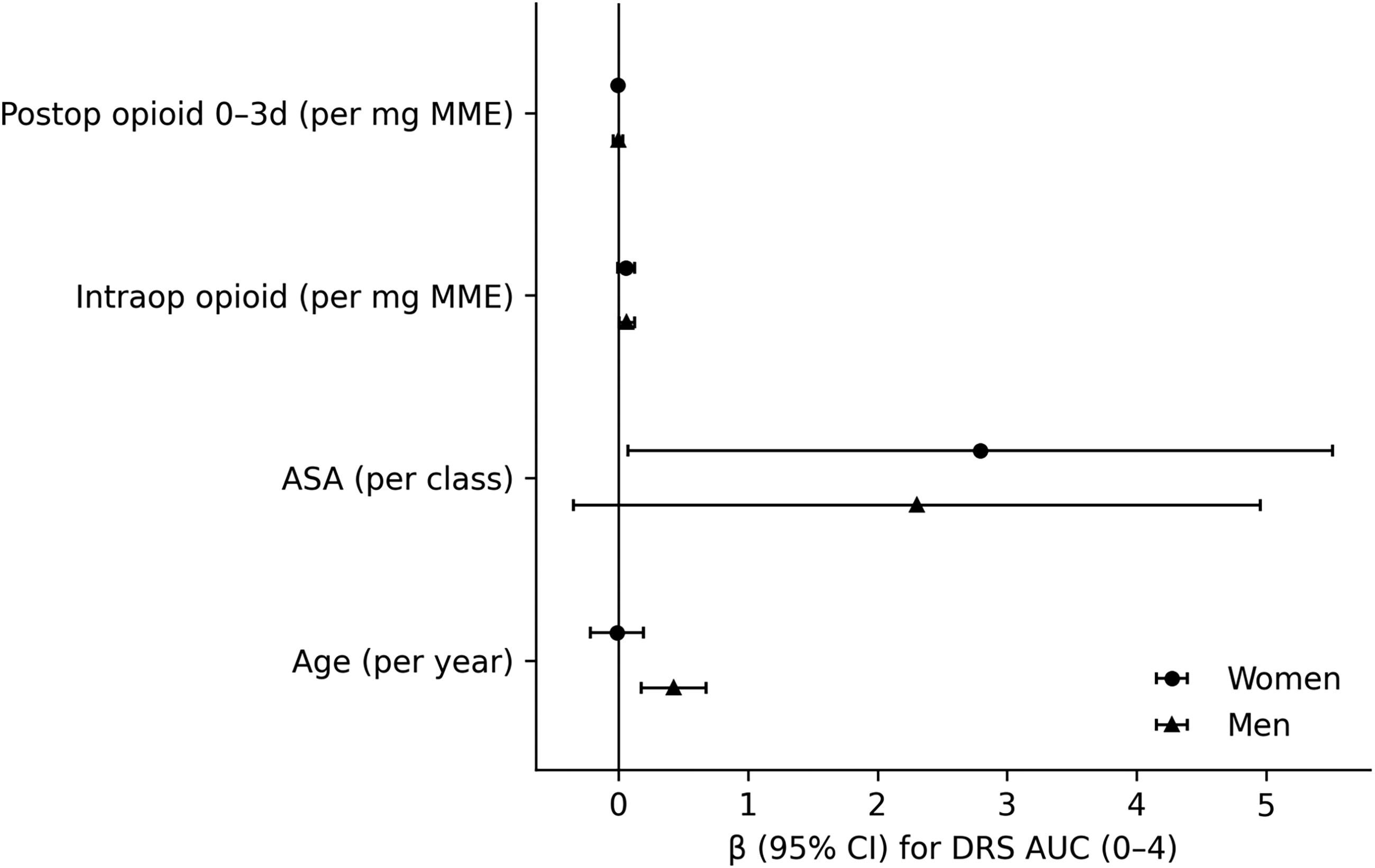
Sex-Stratified Associations with Delirium Burden (DRS AUC 0–4). Forest plot showing sex-stratified regression coefficients (β) and 95% confidence intervals for associations between baseline vulnerability (age, ASA class) and opioid exposure (intraoperative MME; postoperative MME 0–3 days) with delirium burden (DRS area under the curve, days 0–4). Coefficients are shown separately for women and men from adjusted models.
Discussion
In this cohort of older adults undergoing elective hip or knee replacement surgery, we found that postoperative delirium severity and burden were characterized by distinct sex-specific risk profiles rather than by overall differences in unadjusted burden between women and men. Adjusted analyses demonstrated that age was the dominant predictor of delirium severity and burden in men, whereas baseline physiologic vulnerability, reflected by ASA class, was more strongly associated with delirium burden in women (Table 2). In interaction models, the association between age and delirium outcomes was significantly stronger in men, supporting the concept that sex modifies vulnerability pathways underlying postoperative delirium expression.
Our results extend prior work documenting sex differences in delirium’s incidence and outcomes.4,14,15 While some studies have reported higher delirium rates in men, others suggest that women are more likely to experience persistent cognitive dysfunction and functional decline after a bout with delirium.5,16 The current study adds to this literature by modeling symptom severity rather than binary incidence and by capturing dynamic trajectories over time.
Potential mechanisms underlying the observed sex differences include estrogen-related modulation of neuroinflammation, cholinergic activity, and cerebral hypoperfusion.6,9 In animal models, estrogen protects against systemic inflammation-induced cognitive impairment, and its decline post-menopause may amplify susceptibility to delirium triggers.7,8 Frailty, more common among older women, may further lower functional reserve and impair recovery from acute insults. 5 Together, these biological and clinical factors provide a plausible basis for sex-specific vulnerability to delirium burden.
This study also underscores the value of severity-based metrics. Binary classification may underestimate delirium in women, particularly those with hypoactive or subsyndromal presentations.11,15 Continuous tools like the DRS-R-98 enable fine-grained tracking of symptom evolution and allow for the quantification of burden—metrics that correlate more closely with downstream outcomes, for example, discharge disposition and long-term cognition.17,18
These findings have practical implications for perioperative care. Risk stratification strategies may benefit from incorporating sex-specific predictors, with greater emphasis on age-related vulnerability in men and physiologic reserve in women. For example, older male patients may warrant intensified postoperative monitoring for delirium symptoms, whereas women with higher ASA classifications may benefit from proactive delirium prevention pathways, including optimization of physiologic status and minimization of perioperative stressors. More broadly, these results support a move toward individualized, sex-informed perioperative brain health strategies rather than uniform risk models.
This study does have several limitations that warrant consideration. First, this study was conducted at a single specialized orthopedic center, which may limit generalizability to other surgical populations or care settings. Second, although models adjusted for multiple clinical factors, residual confounding remains possible, particularly given potential sex differences in unmeasured perioperative exposures. Third, opioid exposure was quantified using aggregate MMEs and may not fully capture pharmacodynamic differences between individuals. Fourth, while the DRS-R-98 provides detailed severity assessment, it requires trained raters and may not be feasible in all clinical environments. Finally, the sample size, while sufficient for primary analyses, may limit the detection of smaller interaction effects.
Nonetheless, this study leverages rich longitudinal data and validated measures to provide new insights into sex-specific delirium vulnerability. The findings have implications for postoperative monitoring and risk stratification in both older women and men, particularly through sex-informed assessment of vulnerability profiles. Future research should explore mechanistic pathways and evaluate whether targeted perioperative strategies can mitigate delirium burden in this high-risk group.
Conclusions
Severity- and burden-based measures of postoperative delirium reveal distinct, sex-specific vulnerability patterns that are not apparent using binary outcomes alone. In this cohort, postoperative delirium outcomes demonstrated sex-specific patterns of association, with age emerging as the dominant predictor of delirium severity in men and baseline physiologic status more strongly associated with delirium burden in women. These findings support the importance of modeling delirium as a continuous and dynamic process and highlight the need to incorporate sex as a biological modifier in perioperative risk assessment. Future studies should evaluate whether sex-informed prevention and monitoring strategies can reduce delirium burden and improve patient-centered outcomes.
Authors’ Contributions
A.W.P.: Conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft, and approval of the final article. T.A.S.: Conceptualization, methodology, supervision, writing—review, and approval of the final article. K.A.L.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, supervision, writing—review, and approval of the final article.
Supplemental Material
sj-docx-1-jwh-10.1177_15409996261467347 — Supplemental material for Sex Differences in Postoperative Delirium Severity and Burden in Older Adults
Supplemental material, sj-docx-1-jwh-10.1177_15409996261467347 for Sex Differences in Postoperative Delirium Severity and Burden in Older Adults by Adam W. Potter, Theodore A. Stern, and Kenneth A. Larsen
Footnotes
Acknowledgments
The authors wish to express their sincere gratitude to Susan Kelly, MD, for her critical support in the main study. We are also truly grateful to the entire staff at New England Baptist Hospital who supported this effort, particularly for their contributions to patient recruitment, medical records review, and postoperative assessments. The high-quality patient care provided by the nursing staff, especially in the pre- and post-anesthesia care units, and the support from the administrative team were essential to our success.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
This study was supported by a grant from the
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.