
Abstract
Some Arabic-speaking Muslim family members of children requiring bone marrow transplantation receive medical care for their children in the United States. Muslim family members’ use of Islam in the course of their child’s bone marrow transplantation was studied using grounded theory, a qualitative research method. Eighteen members of Middle Eastern Muslim families with a total of 13 children receiving bone marrow transplantation were interviewed by an Arabic-speaking healthcare provider. Interviews were coded by an interdisciplinary team. Seven key themes were identified.
Introduction
A significant number of Arabic-speaking Muslim children requiring bone marrow transplantation (BMT) receive medical care in the USA. These children and their families spend an extended period of time in the USA. Adherents of Islam are a minority population in the USA. Healthcare workers and recipients of care may both have trepidation based on perceived or real lack of education about the faith by some providers. Some US healthcare providers, including chaplains, may not understand the impact of Muslim family members’ religious beliefs and practices on their healthcare experience (Abu-Ras, 2011). Just as importantly, some providers may have an understanding of Islam and assume that all Muslim families will use their religion in a similar way. Religious believers make meaning in multiple ways. While the formal study of Islam is important because it is a rapidly growing religion, the goal of this study was to see how Arabic-speaking Muslim families actually used their religion in the hospital during their child’s BMT.
The research about the use of Islamic beliefs and practices in the context of healthcare is growing. In his chapter on Islam in The Soul of Medicine, El-Jawahri (2011), a physician, notes that seeking healthcare when ill is required by Muslim beliefs. While all suffering is understood to be the will of God, Muslims will make meaning of suffering differently based on their culture, values, and education. Lazenby and Khatib (2012) state that the few studies that exist indicate that Muslims do gain comfort and support from their religious practices. In 2015, Abu-Raiya, Hamama and Folkra (2015) found that Israeli Muslim members of families with children with cancer evidenced positive religious coping defined as “activities reflect[ing] a secure relationship with God, a belief that there is a greater meaning to be found, and a sense of spiritual connectedness with others” (Abu-Raiya et al., 2015, p. e84); however, their study did not explore how family members accessed and used their religious beliefs. Muslim believers who are committed to Islam may express their commitment in differing ways: “… just like any cultural group, Muslims around the world can be conservatives, traditionalists or liberals. They may share commonalities and differences in beliefs, practices, values and norms” (Al-Mutair, Plummer, Clerehan, & O’Brien, 2014, p. 254). A team of European researchers found that Muslim patients had spiritual needs informed by a theological world view that differed significantly from religious beliefs and practices informed by western values: “Thus, in addition to their physical healthcare needs, Muslim patients bring their specific cultural, religious and spiritual needs” (Baeke, Wils, & Broeckaert, 2012, p. 2).
In 2012 this medical center received a significant increase in patients from the Middle East who needed bone marrow transplants. This Midwest medical center had limited experience caring for Arabic-speaking Muslim families and many healthcare providers had never previously interacted with Muslim patients. Members of this research team had done a previous study of the use of religion in the course of BMT by adolescents and young adults in 2012 (Ragsdale, Hegner, Mueller, & Davies, 2014). Those who agreed to participate in that study were Christian; only one patient from a different faith tradition fit the inclusion criteria and that patient declined to participate. Seeing a need to better understand the use of Islam by Middle Eastern Muslim patients and families, this research team decided to use the same methodology to explore how Arabic-speaking Muslim members of families with BMT patients used their religion in the context of the treatment process. This medical center’s institutional review board approved this qualitative study.
This study refers to transliterated Arabic words that may not be familiar to some readers. A glossary of terms is provided in Appendix 1.
Method
The inductive research method grounded theory guided both data collection and analysis. Qualitative interviews provided data about the use of Islam in the context of pediatric BMT. Refusal to have the interview audiotaped was understood to be declining consent to participate in this research study. Interdisciplinary members of the research team analyzed the transcribed, translated texts to identify core themes (Charmaz, 2006; Glaser & Strauss, 1967). The open-ended interview questions provide a guide for the interviewer to prompt research participants to describe their use of faith and how their religious practices and beliefs impacted their experience of their child’s BMT. In situations with both parents in the room, and when one grandparent was present, the interview was conducted as a dyad or triad with all participants related to the patient. The semi-structured interview guide is in Appendix 2.
A male, Arabic-speaking PhD researcher serving as an intensive care nurse interviewed 18 members of the families of 13 children from three Middle Eastern countries receiving BMT in this pediatric medical center. Another Arabic-speaking PhD nurse researcher transcribed the audio recorded interviews and translated them into English. An Arabic-speaking physician corroborated his translation by listening to the audiotapes and reviewing the text for accuracy. A research team of eight interdisciplinary healthcare providers including three physicians, three nurses, and two chaplains coded the interviews in three coding phases: open coding, in which the participants’ own words are used; focused coding, in which emerging themes among the open codes are identified and placed in larger categories; and axial coding, in which focused codes were combined to create core themes. Core themes were agreed upon along with explanatory sub-themes. The sub-themes were also identified in the process of analysis; they served to describe key aspects of core themes. In addition to coding, the research team wrote memos, which are notes about ideas and questions generated by research team members in the analysis process. Memos are ideas contributing to the generation of a proposed theory about the question under review (Charmaz, 2006, 2014). An emerging theory was developed describing how Arabic-speaking Muslim families from the Middle East use Islam in the process of their child receiving BMT in the USA.
Results
Demographics.
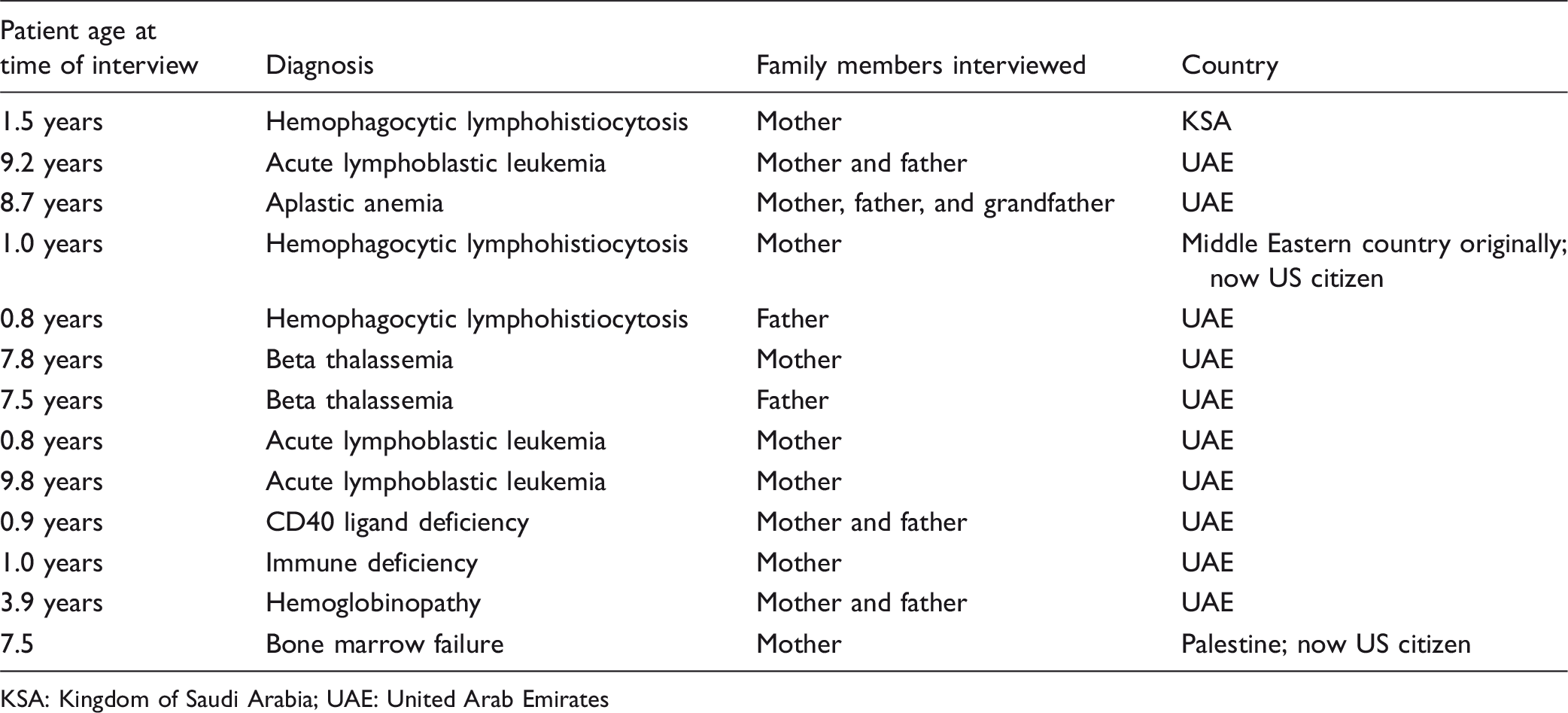
KSA: Kingdom of Saudi Arabia; UAE: United Arab Emirates
Only one potential participant’s family declined to participate in this study due to discomfort with the interview being audiotaped; the patient was a 12-year-old male with immune deficiency from the United Arab Emirates.
Results.
These seven elements impact and inform each other. The emerging theory is that for Middle Eastern Muslim families, their religion is an integral component in understanding and responding to their children’s illness and treatment. Every aspect of the treatment is seen through the lens of their religion. One of the fathers being interviewed commented on the pointlessness of the questions the interviewer asked due to what he considered to be obvious answers. The essential element of his Muslim religion was such a given to him that to ask its level of importance struck this father as “kind of weird.” Nevertheless, he and each family member serving as research participants were willing to answer questions to help healthcare providers in the USA understand better how important Islam was in their experience of their child’s illness and treatment.
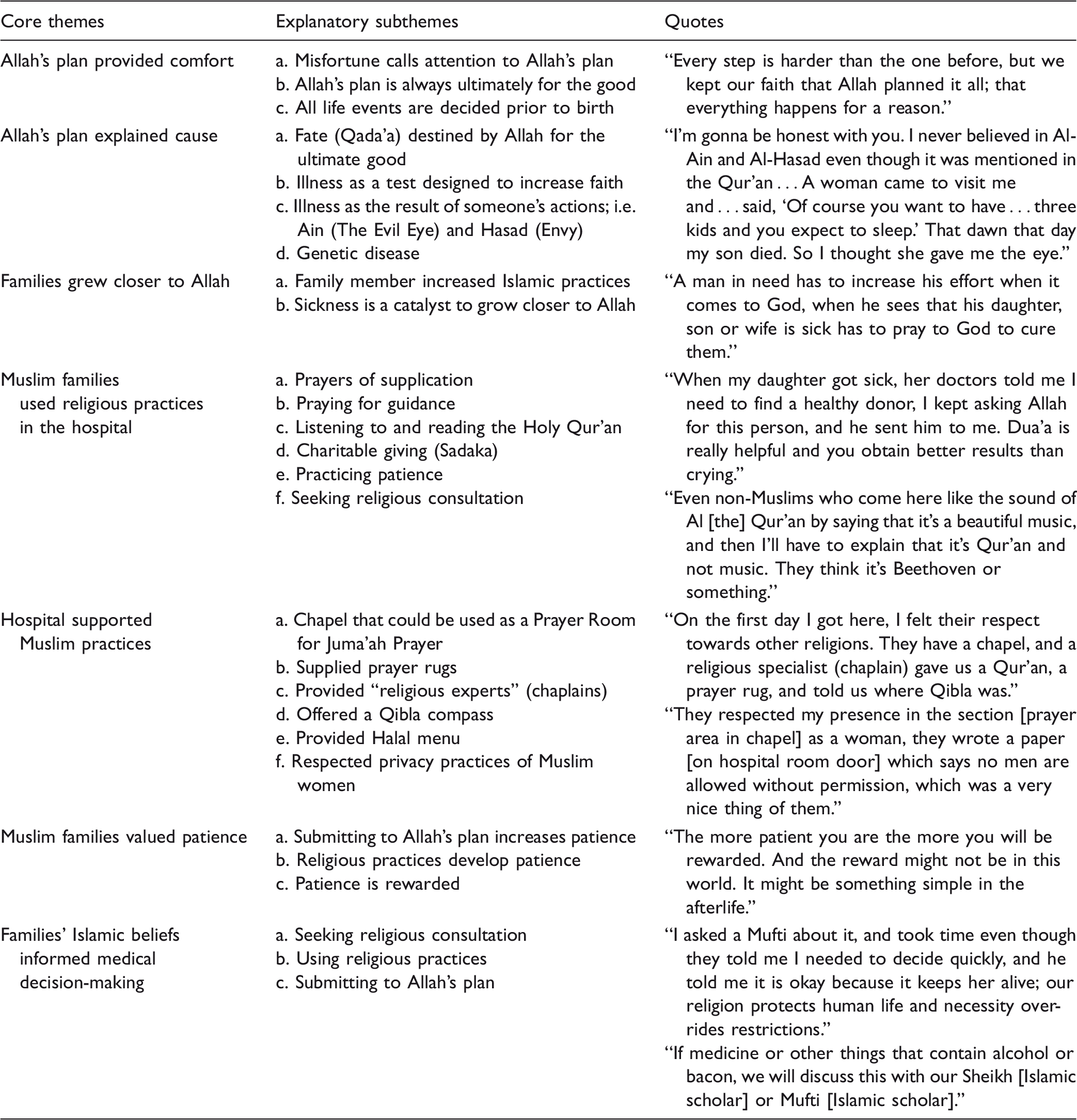
The following seven themes emerged from analysis of the interviews.
Allah’s Plan Provided Comfort
Central to each participant was the theme of Allah’s plan; first and foremost, participants identified Allah’s plan as their primary source of comfort. This is the first core theme. Participants described a sense of trust drawn from their Islamic belief in Allah’s plan. Allah’s plan was understood to be ultimately always for the good. Families did not deny the difficulty of having a very sick child, but definitely took comfort from the knowledge that Allah had planned this situation. They believed Allah knew before their child was born that she or he would be sick, and the outcome of the transplant was part of the plan from before the child was born. Allah’s plan also included knowledge that Islamic practices of the family members would increase as a response to the child’s illness. The families also viewed the medical team, especially the doctors, as part of Allah’s plan in providing treatment for their child. The doctors were seen as instrumental in carrying out the plan of Allah for these children. The fact that Allah had a plan did not decrease the need for religious practices of family members; rather, increased religious practice was part of Allah’s expectation and understood to be part of Allah’s plan.
Allah’s Plan Explained Cause
The second core theme was that the Muslim belief that Allah has a life plan for each person explained why the child had a disease requiring BMT. Participants described various ways they understood the cause of their children’s illnesses. Several family members describe the illness of their children as an affliction. “There is a verse in the Qur’an: ‘But you may hate a thing although it is good for you, and you may love a thing although it is evil for you. Allah knows and you do not.’ So good will come out of an affliction.” Affliction was considered an inescapable part of life, and a part planned by Allah. One mother said: Praise be to Allah that we are Muslims and we know that everything is Qada’a [fate] and Qadar [destiny] and Allah has planned it all; everything is written with Allah. I mean that no man was born without his life being planned including when you’re born, what afflicts you, and when you die.
Family Member Grew Closer To Allah
The third core theme was identified by each participant: every family member acknowledged spending more time thinking about her/his Muslim religion. Most said they had been committed before, but this experience of significant illness and difficult treatment led to an increase in religious practices. Participants highlighted an increase in various forms of prayer, relying on the Holy Qur’an, and charitable giving. “When anyone is affected by an adversity it makes them closer to Allah, in many aspects such as praying, [and] reading the Qur’an.”
Muslims Used Religious Practices in the Hospital
The fourth core theme defined which practices Muslim families used most while their children were being treated. The prayers family members most often referenced were Dua’a, which are prayers asking Allah for something specific knowing He will respond, and Estekhara, which are prayers seeking guidance. Another practice often noted as very helpful was Sadaka (charitable giving): “In our religion, Sadaka is what relieves patients more than anything else. God might provide a cure from Sadaka and Dua’a. That’s what we hear from the Muslim scholars.” Another extremely important practice for Muslim families was listening to or reading the Holy Qur’an. One particularly important portion of the Holy Qur’an was Surat Al-Baqara, a chapter in the Holy Qur’an; one mother said it brought her great comfort: “It fades away all the griefs inside my heart, and it makes the demons go away.”
Hospital Supported Muslim Practices
The fifth core theme demonstrated what the medical center provided that these Muslim family members found especially useful during their children’s hospitalizations. One father gave voice to a concern his family felt coming to the USA: “They might think I was from ISIS or something … I was worried about how people in the West perceive Muslims.” On the contrary, participants reported that the religious expert (chaplain) offering religious resources created a sense of support and respect: “On the first day I got here, I felt their respect towards other religions. They have a chapel, and a religious specialist [chaplain] gave us a Qur’an, a prayer rug and told us where Qibla [direction that should be faced when a Muslim prays] was.” Participants verbalized that the hospital’s provision of space for both men and women (with culturally sensitive partitions) to pray in the multi-faith chapel made them feel respected.
Muslim Family Members Valued Patience
Each research participant affirmed patience as a core value and practice used to both understand and cope with the child’s BMT. The sixth core theme is closely related both to submission to Allah’s plan and to committed practice of Islam. Patience is both a religious practice and the result of committed practice in Islam. “Allah afflicts you to test your patience, how you deal with it, and how much faith you have in God. The more patient someone is and the more he trusts in God, all these afflictions will go away. When you handle these things better, you will receive better results.” Another participant said, “Allah is testing us not only by disease, other people have other disasters, what I know is patience makes you closer to Allah.”
Families’ Islamic Beliefs Informed Medical Decision-Making
The seventh core theme revealed that the highest authority for medical decision-making for these research participants was their Islamic religion. Study results showed that while family members very much respected the doctors, they also consistently consulted an authority in their faith, whether it was an Imam or an Islam scholar such as a Mufti or a Sheikh. Several research participants stated that they would under no circumstances accept a medical treatment at odds with Islam. BMT is acceptable for Muslims. Life-saving treatments are generally accepted by Islam; this study did not identify any life-saving treatments not acceptable to these research participants.
The theory emerging from this study is that Muslim families from the Middle East use their religion consistently in the hospital in ways that impact their experience and guide their decision-making; this theoretical model is shown in Figure 1.
Model for emerging theory: Arabic Muslim religious practices and beliefs are integral in US pediatric bone marrow transplantation.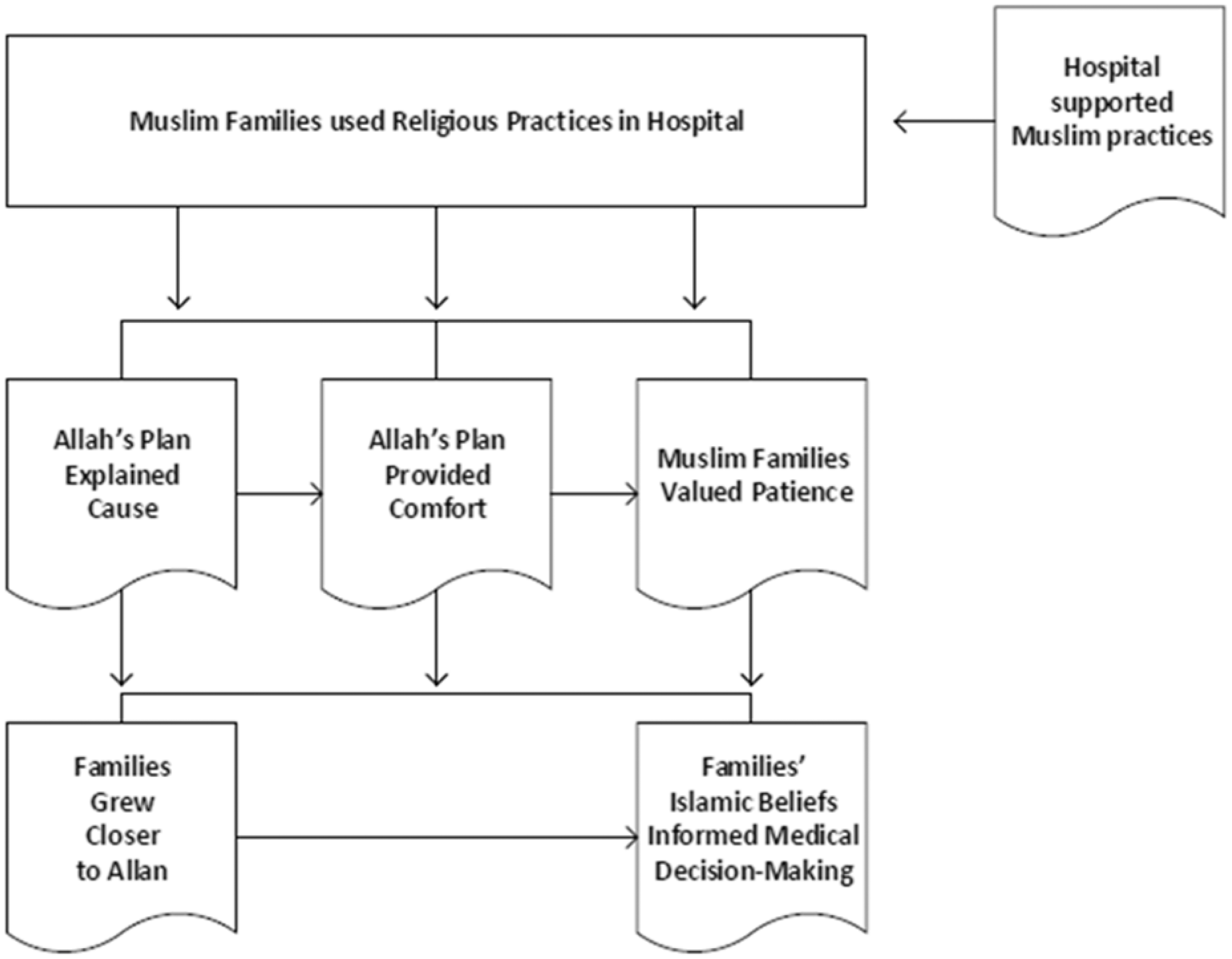
Arabic Muslim religious practices and beliefs proved to be integral to the experience of families seeking BMT for their children in the USA. This model shows the relationship of the core themes to each other. Of particular note is the relationship between religious practices in the hospital core theme with each other core theme. The belief that Allah’s plan explains the cause of illness led directly to Allah’s plan providing comfort. Both of these elements led to and were impacted by religious practices in the hospital. Hospital support for Muslim practices was not causal; certainly these families would have practiced their religion independently of religious support provided by the hospital. However, the hospital’s support for Muslim religious practices led families to feel respected and supported by the hospital in a way that enhanced their BMT experience. Results also showed that the hospital could provide increased support, for example by providing better opportunities for Wudu (cleansing practices before prayer) in the toilet areas. Valuing patience was related to and a result of submitting to Allah’s plan, which provided comfort. Living with patience was both an expression of and resulted from practicing Islam. Intentionally using patience reflected acceptance of Allah’s will. Religious practices resulted in increased patience, which also led families to feel closer to Allah. Engaging in religious practices and feeling closer to Allah impacted decision-making because families were able to receive guidance from prayer, from the Holy Qur’an, and from consulting Islam scholars such as Muftis. Muslim families using religious practices while in the hospital impacts each of the other core elements in this study; religious practices are central to the Middle Eastern Arabic Muslims’ experience of pediatric BMT.
Discussion
This paper reports a study of how practicing Arabic Muslims from the Middle East used their religion in the context of their child’s BMT. The purpose is not to explain Islamic beliefs, but rather to explore how Arabic Muslim families either currently or originally from the Middle East used their religion while their children were hospitalized in the USA either receiving or recovering from BMT. Practitioners of various religions make sense of religious practices based on their own understanding and use their religion as a way of understanding and responding to the situations in which they find themselves (McSherry, Cash, & Ross, 2004; VandeCreek & Burton, 2001).
The literature supports these research participants’ perspective that Allah’s plan both explains and provides comfort; a study of three Muslim women with breast cancer found that: For all three women interviewed, their advanced illness became a spiritual awakening as they came to understand that their experience of cancer ultimately brought them to the deep realization that everything and everyone is under the dominion of Allah. The women discovered that the burden of their breast cancer became more bearable as they realized how the disease brought them closer to Allah. Illness, therefore, was regarded as a sign of God’s love and grace, not punishment.(Ahmad, binti Muhammad, & Abdullah, 2011, p. 40).
The participants interviewed for this study each reported relying on their Islam to understand and to cope with their child’s illness and to make medical decisions. A Canadian study of Muslim spiritual caregivers included the finding that “Muslim scholars are one of the important sources of effective Islamic spiritual care”(Isgandarova, 2012, p. 1). All participants interviewed expressed some version of “I will not do anything Islam does not allow.” Those who addressed the subject agreed that Islam allowed anything that would save a child’s life, and that Islam made allowances for a change in religious practice to accommodate hospitalization. For instance, a participant indicated that prayer requirements could be changed to accommodate families in the hospital. Four of the five required prayers could be combined so that two prayers were said at one time. Prayers could also be shortened.
Given the distinct differences with which religious practitioners understand their faith traditions, one surprising finding in this study is how similarly Muslim participants understood and practiced their faith. The participants themselves, however, noticed significant differences among Muslim Arabic Middle Easterners in the practice of their religion while at the hospital; one participant said: Some people forget Islam as soon as they get out of their country. I told them that that’s what we do, we wear a head veil. A woman in Islam is like a diamond and needs to be covered. So they told me there are some [Arabic Middle Eastern Muslims] here who took off their head covers. This is wrong … They keep saying this is freedom and I said this is not what it means to be free.
One finding that was markedly different from the earlier study was the emphasis on patience. Research participants for this study acknowledged difficulties, but uniformly reported that Islam provided and strengthened patience. Allah desires patience and rewards patience with cure in this life, and/or with reunion in the afterlife. One image offered from Islam was that when a child dies before his or her parents, when the parents die, the child will guide them by the hand into heaven. This finding is supported by a study of Muslim elderly women in Belgium who had immigrated from Morocco or Turkey; a key finding was that “patiently enduring illness and suffering is of utmost importance, as it gives evidence of gratitude to God. Complaining about illness is altogether wrong” (Baeke et al., 2012, p. 3). El-Jawahri noted that “patience, perseverance, and gratitude … open the door for spiritual and physical well-being” (El-Jawahri, 2011, p. 81).
One goal of this study was to learn how to better understand how Arabic Muslim families from the Middle East use their religion so that families’ religion/spirituality could be incorporated into the treatment plan, including incorporating religiously-informed chaplaincy care. An article reviewing literature addressing the psychology of Islam focusing on mental health issues provided information about the integration of Islam in treatment: First, given the centrality of Islam to many Muslims, mental health professionals should invite Muslim clients into a “religious conversation” by explicitly inquiring about the place of religion in their lives. Second, because Islam is a multidimensional religion and can mean different things to different people, it is important to ask Muslim clients “what does Islam mean for you?” Third, given the demonstrated links between positive religious coping and well-being, therapists can encourage their clients to identify and draw on their religious coping resources (e.g. considering stressors as a test from Allah, seeking Allah’s love, care and forgiveness, reading the Holy Qur’an to find consolation). Finally, given the potential negative impacts of religious doubts and struggles, therapists should thoroughly assess for the presence of religious struggle and doubts, normalize them and avoid passing judgment on clients who are struggling. In the process of normalizing spiritual struggles, it might be helpful to refer to individuals from the Islamic tradition (e.g. Muhammad, Moses, Abraham) as models of esteemed figures who experienced such struggles (Abu-Raiya & Pargament, 2011, p. 104).
While it was not a goal of this study to seek feedback about the care Cincinnati Children’s Hospital offered Muslim families, results indicated that families very much appreciated the way their religion was approached in this context. Participants reported appreciation of the religious experts, which is the term interpreters have agreed on for chaplains because the word “chaplain” does not translate into Arabic. Isgandarova (2018) notes that the word “chaplain” is counterproductive when working with Muslim patients. Participants noted that the religious experts provided them with prayer rugs, with copies of the Holy Qur’an, and with Qibla compasses. One parent commented that the religious expert did not know she should not directly touch the Holy Qur’an but that only a Muslim should touch the Holy Qur’an. This perspective was new learning for the non-Muslim members of our research team. It seems that this practice, like so many religious practices, is open to interpretation; Muslim members of our research team did not agree with aspects of this participant’s comment. However, following our goal to gain greater understanding of perceptions of Muslim patients and families, this perspective broadened our understanding.
The results from this study suggest several implications for chaplains in the USA providing care for Middle Eastern Muslim families. First, chaplains have the important role of helping the medical team understand the Muslim families’ patience not as lack of understanding the severity of their child’s situation; rather, a calm demeanor is a sign of using patience as a way of demonstrating trust in Allah’s plan. Second, the chaplain’s understanding the use of specific prayers beyond the five prayers a day, especially the Dua’a (prayer asking Allah for something specific knowing He will respond) and the Estekhara (prayer for guidance), may be experienced by Muslim family members as very supportive. Third, the chaplain can explain to staff the healing and protective components of playing the Holy Qur’an in the room; since most staff do not understand Arabic, it can cause anxiety if they have no understanding of what is being played and how it supports the family. Hearing the Holy Qur’an audibly can also be a sign to the chaplain that the family is more concerned about the child’s condition since families tended to pray the Holy Qur’an more often when a child’s illness was at its most serious. Fourth, the title “chaplain” does not translate easily into Arabic. Some interpreters at this medical center at first used the word “missionary” for chaplain; this was not helpful in establishing rapport. Working in collaboration with the chaplains, the interpreters began the practice of calling chaplains “religious experts,” which allowed families to receive the support of chaplains. Fifth, understanding that many Muslim families turn to Muftis, Imams, or Sheikhs for help in making medical decisions, the chaplain can be proactive in building relationships in her or his community so that if this need arises, the chaplain can act as an important liaison between the family and the Muslim leader. Sixth, while it is always useful for the chaplain to provide a spiritual assessment of the way a family’s religion/spirituality impacts healthcare, when working with patients whose faith traditions are less common in the dominant culture, the spiritual assessment is even more important. The chaplain’s spiritual assessment would be most helpful to the patient, family, and staff if it is offered as early as possible in the patient’s course of treatment. Seventh, education for chaplains in Clinical Pastoral Education (CPE) could equip chaplaincy students to understand the many ways Muslim beliefs and practices impact patients, families, and staff members in the healthcare context. Isgandarova (2018) notes that CPE for Muslim spiritual care providers includes Islamic theology and interfaith dialogue and relations; these elements could be incorporated into CPE curricula for all CPE programs focused on preparing hospital, hospice, and military chaplains. Abu-Ras and Laird (2011) agree that Western-trained chaplains must be educated in the illness and death practice of Islam because it is essential for Muslim patients to receive healthcare that incorporates spirituality. CPE students with knowledge of Islam may be encouraged to spiritually assess how individual Muslim patients and hospital staff members use Islam to make meaning, cope, and make medical decisions.
Limitations
This study is limited by the specific demographic of Arabic-speaking Muslim families from the Gulf region of the Middle East; results cannot be transferred to all Muslim patients receiving BMT in the USA. As in many qualitative studies, this one is limited by sample size. The convenience sample of Arabic-speaking Muslim families receiving care at this medical center limited diversity of potential participants. Because of the level of illness of the pediatric patients requiring BMT, it was determined that this study not ask participants to elaborate on disparities in the results such as how praying might impact Allah if the child’s life is already planned. This question could be studied with Muslim families in a less vulnerable context.
Conclusion
The practice of their Muslim religion is integral to the pediatric BMT experience of Arabic-speaking Muslim families. Knowledge of how Muslim family members use their religion could equip hospital staff members and administrators to understand and support these religious practices. This perspective mirrors the comments of a Muslim chaplain that “a grounded understanding of general Islamic beliefs on the definition of life, the use of palliative care, etc … offers caregivers the potential to greatly improve patient experience and satisfaction” (Zaidi, 2015, p. 173). Supporting Muslim religious beliefs in the context of hospitalization is not only a sign of respect but, based on results from this study, is key to assisting Muslim families in their medical decision-making. The healthcare experience of Arabic-speaking Muslim patients and families is improved when hospital staff members better understand the impact of Muslim beliefs on the hospital experience. Chaplains provide helpful support for patients and families, and provide understanding of faith practices and perspectives to members of the medical team.